
Abstract
Background:
The calf muscle pump is an understudied contributor to venous return from the lower extremity. This study aimed to determine if calf pump function (CPF) is independently associated with the severity of chronic venous disease classified by CEAP (Clinical-Etiology-Anatomy-Pathophysiology).
Methods:
The Mayo Clinic Vascular Laboratory database was analyzed from January 2015 through September 2023. Ambulatory adults who underwent venous air plethysmography were included. Venous plethysmography assessed the severity of venous incompetence, and CPF was measured as ejection fraction (EF) per leg. The clinical component (C0 through C6) of the CEAP score was evaluated for each extremity at the time of the study.
Results:
A total of 7760 limbs from 3733 patients were analyzed. The mean age was 62 years, with 62% women. Venous obstruction was detected in 3.2% of limbs. Venous incompetence severity was categorized as normal (44%), mild (26%), moderate (19%), and severe (10%). A significant trend of reduced CPF was observed with higher CEAP scores (p < 0.001). Multivariable logistic regression, adjusted for age, sex, degree of venous incompetence, and obstruction showed reduced CPF was a significant predictor (odds ratio 1.84, CI: 1.5–2.2) of active/prior ulcer (C5 or C6). In contrast to more severely reduced CPF, mildly reduced CPF (EF 40–49%) was not associated with active/prior ulcers.
Conclusion:
This large contemporary study demonstrates that decreased CPF is associated with worse chronic venous disease. Importantly, we demonstrate for the first time that CPF is independently associated with active/prior venous ulcers after accounting for other venous physiologic parameters and demographics.
Background
Chronic venous disease (CVD) is common in the general population, with prevalence estimates varying widely based on geographic region, study population, and disease classification systems. Reported rates range from 30% in the Edinburgh Vein Study to as high as 60% in global epidemiological studies.1–3 Most cases are mild, but the disease can range from telangiectasias and reticular veins (50–66%) to more advanced disease, causing swelling, skin changes, and ulcerations. Venous ulceration has a prevalence of 1–5% in Western countries, and women are more affected than men, although men may experience more severe disease.2,3 Valvular competence, venous patency, and calf pump function (CPF) are critical in determining ambulatory venous pressure. Dysfunction in any of these elements can lead to varying severities of CVD, though an effective calf muscle pump (CMP) can help compensate for valvular dysfunction or obstruction. 4
The CMP is an understudied contributor to venous return from the lower extremities but plays a crucial role in preventing venous stasis and promoting efficient blood flow back to the heart. A reduced CPF is an independent risk factor for mortality,5,6 and is associated with an elevated risk of venous thromboembolism.7,8 Despite its importance, no large contemporary study has examined CPF and its independent link to CVD and ulcers. Previous small studies have suggested a connection between CPF and the progression of CVD, but comprehensive, large-scale research is lacking. This study aimed to investigate the association between CPF and the severity of CVD classified by CEAP (which evaluates the severity of venous insufficiency based on clinical presentation, etiology, anatomy, and pathophysiology) and to determine if reduced CPF was independently associated with active/prior venous ulcers.
Methods
Study population
Patients 18 years of age or older referred for venous air plethysmography to the Mayo Clinic Gonda Vascular Laboratory between March 2015 and September 2023 were eligible for inclusion. Common reasons for referral include leg pain or swelling, varicose veins, and lower-extremity ulcerations. Clinically, venous hemodynamic testing is only performed on ambulatory patients, and equipment precludes testing on patients weighing > 300 pounds (136 kg). The Vascular Laboratory database was queried for eligible subject inclusion, and demographic and comorbidity data (International Classification of Diseases, 9th and 10th Revision codes) were collected from a centralized system containing complete records of all patients treated and followed at Mayo Clinic. The Mayo Clinic Institutional Review Board approved the study and waived the requirement for informed consent.
Venous plethysmography
Standard venous air plethysmography techniques (Supplement) were employed to evaluate venous physiology as previously described.7,8 Testing includes three phases: venous outflow, passive drainage and refilling, and ankle flexes, followed by postexercise refilling, assessing venous obstruction, valvular incompetence, and CPF evaluated on both lower limbs. Per limb, the presence or absence of obstruction is noted, and the degree of venous incompetence is graded as normal, mild, moderate, or severe based on established laboratory criteria. Obstruction by venous plethysmography can indicate acute or chronic deep vein thrombosis (DVT) or other anatomical flow abnormalities (e.g., pelvic mass, May-Thurner). The calf ejection fraction (EF) is calculated by dividing the volume of blood returned after exercise by the volume returned after passive refilling and multiplying by 100. Reduced CPF (rCPF) was defined as an EF of less than 45%. Limbs were categorized into two groups: those with normal CPF levels and those with rCPF. The clinical component (C0 through C6) of the CEAP score was performed/supervised on each extremity at the time of the study by Registered Vascular Technologists.
Analysis
As each limb contains independent measures of CPF, incompetence, obstruction, and CEAP score, the analysis was performed per limb. The primary outcome of interest was the presence of C5 or C6 disease, indicating a healed or active venous ulcer at the time of the study. Descriptive characteristics were presented as mean and SD for continuous variables, and numbers and percentages were used for categorical variables. To analyze differences between groups in numerical and categorical variables, t-tests and chi-squared (χ2) tests were utilized, respectively. The Wilcoxon rank-sum test was used when continuous data were not normally distributed. Fisher’s exact test was used for categorical comparisons when categories had less than 10. The Charlson Comorbidity Index (CCI) was calculated per patient at the time of the study using the following comorbidities: myocardial infarction, congestive heart failure, peripheral vascular disease, stroke or TIA, dementia, chronic obstructive pulmonary disease, connective tissue diseases, peptic ulcer disease, liver diseases, renal diseases, diabetes mellitus, hemiplegia, chronic kidney disease, cancers, and HIV/AIDS. 9
Univariable and multivariable logistic regression analyses were performed to identify independent predictors of active/prior ulcers. First, we examined each result of the plethysmography study (obstruction, incompetence, CPF) through univariate analysis to assess its association with active/healed ulcers. Next, we used two multivariable logistic regression models to explore the relationship between CPF categorized as a dichotomous variable (reduced vs normal CPF) or by groups of abnormal CPF (EF 0–9, 10–19, 20–29, 30–39, 40–49, > 50) with additional clinical variables (age, sex) and venous variables (obstruction, incompetence). The model results are reported using odds ratios (OR) and their corresponding 95% CIs. All statistical tests were two-sided, with significance defined as p < 0.05. Data were visualized and analyzed using Python 3.0 and BlueSky (version 7.4, BlueSky Statistics LLC, Chicago, IL, USA).
Results
A total of 7760 limbs from 3733 unique patients underwent venous plethysmography at the Mayo Clinic Gonda Vascular Laboratory and were included in the analysis. Most patients had only one (n = 3588) or two studies (n = 126). Eight patients had CPF assessed only unilaterally due to various factors (e.g., fused ankle, below knee amputation). The mean age was 62 years (SD ±14.83), and 62% were women. Among the 7760 limbs, 251 (3.2%) had obstruction. The severity of venous hemodynamic incompetence was categorized per limb as follows: 3422 (44%) normal, 2048 (26%) mild, 1485 (19%) moderate, and 805 (10%) severe. An active/prior ulcer was present in 611 (7.9%) limbs. The CEAP classification was distributed as follows: 327 in class 0 (4.2%), 1020 in class 1 (13.1%), 1009 in class 2 (13.0%), 3139 in class 3 (40.5%), 1654 in class 4 (21.3%), 251 in class 5 (3.2%), and 360 in class 6 (4.6%). Reduced CPF was common overall and was seen in 3692 limbs (47.6%) studied.
Significant demographic differences were observed between patients with rCPF and those with normal CPF (Table 1). Patients with rCPF were older, with a mean age of 64.3 years compared to 59.7 years in the normal CPF group (p < 0.001). CPF was less often reduced among men compared to women (p < 0.001) and was more often reduced on the left compared to the right limb (55.4% vs 44.6%, p < 0.001). Limbs with rCPF exhibited a higher frequency of moderate (22.9% vs 15.7%) and severe (16.5% vs 4.8%) incompetence and were more likely to have outflow obstruction (5.0% vs 1.6%, p < 0.001) compared to limbs with normal CPF.
Comparing characteristics of normal and reduced calf muscle pump function groups.

T-test; bchi-squared test; cWilcoxon rank-sum test; dFisher’s exact test.
BMI, body mass index; CCI, Charlson Comorbidity Index; CEAP, Clinical-Etiology-Anatomy-Pathophysiology; CPF, calf pump function.
The clinical staging of venous disease, as assessed by the CEAP classification, showed significant differences between the two groups. A higher percentage of limbs in the rCPF group (37.4%) were classified as CEAP class 4 or higher, compared to only 21.7% in the normal CPF group (p < 0.001). Visually, we observed a trend of increasing CEAP scores with decreasing EF categories (Figure 1). Active/healed venous ulcers were present in 11.5% (n = 425) of limbs with rCPF versus 4.6% (n = 186) of limbs with normal CPF (p < 0.001).
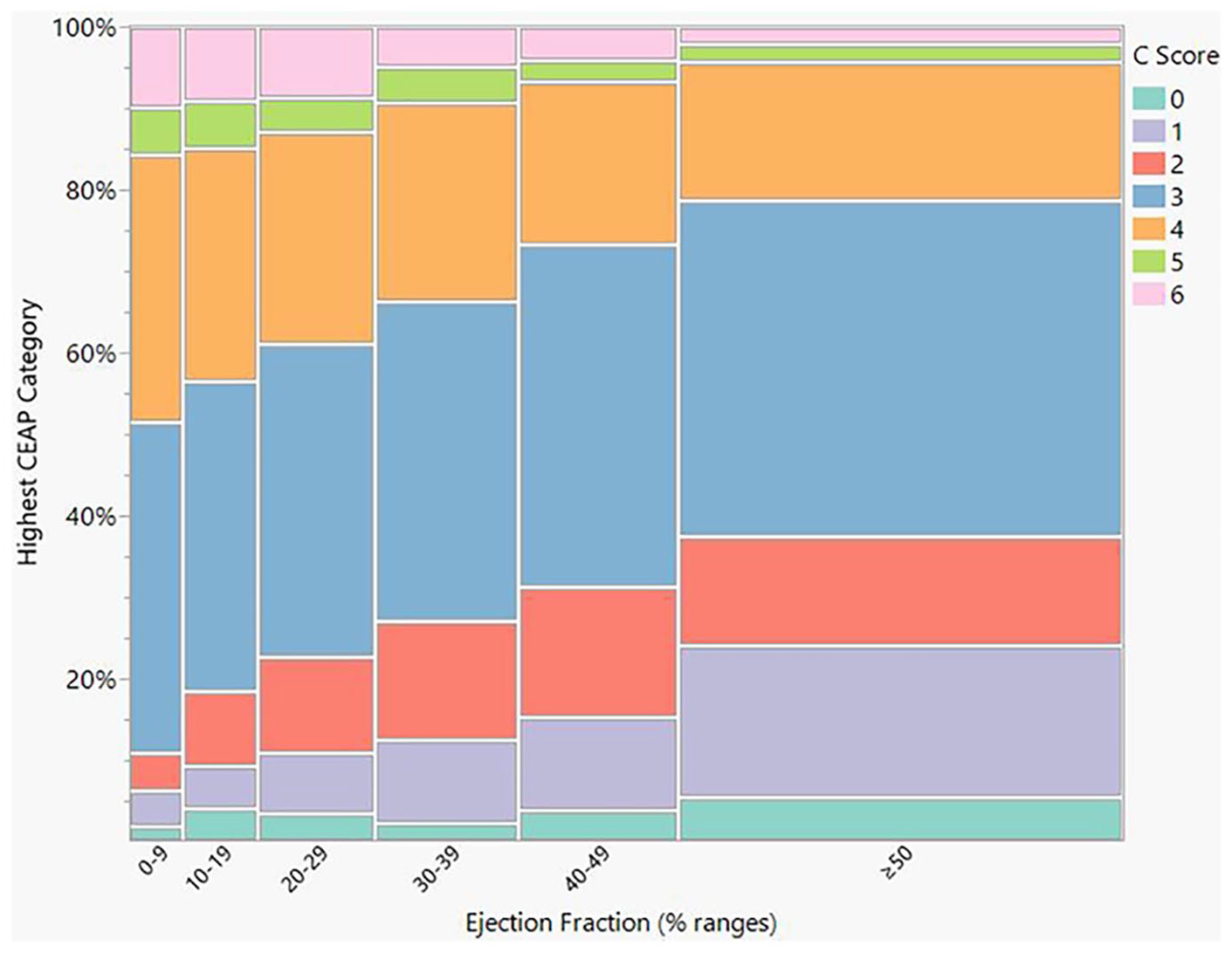
Relationship between CEAP and calf pump function ejection fraction.
Univariate logistic regression analysis revealed several factors associated with active/prior ulcers (Table 2), including age (OR 1.02 95% CI: 1.02–1.03), male sex (OR 1.64, 95% CI: 1.39–1.94), all categories of venous incompetence severity, presence of venous obstruction (OR 1.92, 95% CI: 1.32–2.78), and rCPF (OR 2.72, 95% CI: 2.27–3.25). Lower EF categories showed a higher association with active/prior ulcers: EF 0–9% (OR 4.07), EF 10–19% (OR 3.88), EF 20–29% (OR 3.27), EF 30–39% (OR 2.25), and EF 40–49% (OR 1.58). After adjustment using a multivariable logistic regression model (including age, sex, and degree of venous incompetence and obstruction, Model 1), rCPF was independently associated with active/prior ulcers, with an OR of 1.84 (95% CI: 1.52–2.22). Next, we performed another analysis (Model 2) with the same covariates but using CPF categorized based on EF categories, providing more detailed insights. Compared to limbs with normal EF (⩾ 50), those with an EF ranging from 0 to 9% exhibited the highest OR of 2.43 (95% CI: 1.75–3.37), followed by limbs with an EF of 10–19% with an OR of 2.37 (95% CI: 1.76–3.19). Similarly, limbs with an EF of 20–29% had an OR of 2.16 (95% CI: 1.66–2.81), and those with an EF of 30–39% showed an OR of 1.54 (95% CI: 1.18–2.03). However, CPF ranging from 40% to 49% was not significantly associated with active/healed ulcers (OR 1.28, 95% CI: 0.97–1.70). In a multivariable sensitivity analysis, we excluded any patients who had CPF measured in only one extremity and any patient who had a study performed more than once and found that rCPF was similarly associated with active/prior ulcers (OR 1.96, 95% CI: 1.61–2.38).
Logistic regression analysis for active/prior ulcers.

CPF, calf pump function; EF, ejection fraction; OR, odds ratio; Ref, reference.
Next, extended multivariable models were created to control for comorbidities using the Charlson Comorbidity Index (CCI), without age because this was already included in the model. Though CCI was associated with ulcers in the univariate analysis (OR 1.04, 95% CI: 1.01–1.08), in the multivariable model, CCI was not an independent predictor of ulcers (OR 0.91, 95% CI: 0.48–1.72) and did not significantly change the effect estimate for CPF. Similarly, body mass index (BMI) (continuous scale) was associated with ulcers in univariate analyses (OR 1.02, 95% CI: 1.01–1.04) but was not significantly associated in the multivariable model and did not change the effect estimate for CPF. To investigate CPF findings further within other plethysmographic findings, we performed additional sensitivity analyses to determine if the CPF findings were similar across groups. Additional multivariable logistic regression models added an interaction term between CPF and either obstruction or incompetence (performed separately). The p-value for interaction was 0.7 when examining CPF by obstruction category, indicating that CPF was similarly associated with ulcers across both groups. The interaction term between CPF and incompetence was also not significant (p = 0.4). There was no clear trend across categories (OR for normal: 1.82, mild: 1.43, moderate: 1.79, severe: 2.67), although the effect estimate was numerically highest in patients with severe incompetence, possibly suggesting an enhanced effect in this group. To explore this finding, we recategorized the severity of incompetence into severe versus not severe. We added this as an interaction term in the model, which did not change the conclusion (p = 0.1). Similarly, the extremity side had no statistically significant interaction with CPF on the ulcer outcome (p > 0.99).
Discussion
This large contemporary study of 7,760 limbs evaluated by air plethysmography provides compelling evidence for the significant role of CPF in CVD, particularly its association with venous ulcers. Reduced CPF was common in limbs examined in this study and, importantly, was independently associated with active/prior venous ulcers after adjusting for established risk factors such as age, sex, valvular incompetence, and venous obstruction.
Our result aligns with and extends previous research in this field. Santos et al. 10 evaluated 99 women using the CEAP clinical classification and assessed the strength of the CMP by measuring total work and peak torque. Their analysis, which adjusted for age, BMI, and physical activity, revealed that patients with higher clinical severity of CVD demonstrated reduced CMP strength. Similarly, Panny et al. 11 found that in 84 limbs from 44 patients, higher clinical severity of CVD was related to poorer strength of calf muscles, as measured by dynamometry. They observed that the strength of the dorsiflexor was significantly reduced in patients with the most severe CVD (C6 classification) compared to healthy controls. Interestingly, markers of muscle strength, such as hand grip strength, correlate poorly with CPF. 12 Another study 13 used air plethysmography to examine CPF in 59 limbs of patients with venous leg ulcers. The findings revealed that patients with rCPF were older and had larger and more longstanding ulcers with longer healing times. This was consistent with our observations and reinforces the clinical significance of CPF in ulcer development and healing.
The CMP is crucial for returning venous blood from the lower extremities to the heart. Its failure can cause sustained venous hypertension, contributing to venous leg ulcers. 14
Araki et al. 15 studied 69 limbs in 55 patients with CVD, categorized by the SVS/ISCVS 16 classification into three groups: no ulcer history (19 limbs), healed ulcers (20 limbs), and active ulcers (30 limbs). Using air plethysmography, they found that limbs with active ulcers had significantly lower CPF and EF compared to nonulcerated or healed limbs. Notably, the degree of venous insufficiency did not differ significantly among the groups. Our study provides new insights into the relationship between CPF and provides supporting evidence for efforts to enhance the CMP to aid in the healing of venous ulcers. 17
We observed a graded association between CPF and active/prior ulcer, with severely reduced CPF (characterized by ejection fractions of 0–9%) showing the strongest association. This finding highlights the importance of rCPF at a specific cut-off and the overall severity in the context of the EF. Of note, limbs with CPF in the 40–49% range did not show a statistically significant association with active/prior ulcers compared to those with higher EF values. The observed threshold effect aligns with a systematic review proposing an EF range of 42–62% as the boundary between functional and dysfunctional CMPs. 18 Back et al. 19 assessed 32 limbs of 26 adult men and determined CPF using air plethysmography measurements of EF and residual volume fraction (RVF). They reported significantly reduced EF in patients with CVD, particularly those with active ulceration. This suggests a potential ‘safe zone’ for CPF, above which the risk of ulceration does not substantially increase. These threshold-based insights provide valuable clinical markers for risk stratification and potential intervention targets in managing CVD.
Though lower thresholds may be associated with a higher likelihood of venous ulcers, we also demonstrate a graded effect as it relates to other CEAP scores, suggesting that a single cut-off value to define normal and abnormal may obscure a more meaningful interpretation. We believe that a system more akin to venous incompetence grading of mild, moderate, and severe would be more appropriate and propose that CPF < 20% is severe, 20–29% is moderate, 30–39% is mild, and ⩾ 40% is normal based on the prevalence of ulcers and worsening CEAP scores overall. Of note, the ~20% threshold has been observed in prior studies as the threshold where rCPF is most associated with prospective DVT risk. 8
Compared to prior small studies, this study’s significantly large sample size allowed for a robust statistical evaluation that had not previously been possible. Whether or not reduced CPF is independently associated with worse CVD or active/healed venous ulcers has not previously been reported, but it is an important detail to understand, especially in patients with concurrent obstruction and valvular incompetence. A strength of our study was the assessment of CEAP in each extremity at the time of the study, preventing mischaracterization of CVD in relation to plethysmography assessment. A limitation of this analysis is the exclusion of patients at particularly elevated body weights as they exceeded the weight limit for the study chair; however, among patients included, BMI did not differ between categories of CPF. Owing to the nature of the referral for testing, our population has a referral bias that increases the prevalence of venous disease and, therefore, does not reflect the prevalence of venous disease more generally in the population. Our study was also limited in that we could only assess the presence of CVD at the time of the study due to the cross-sectional nature of the database. Future studies should be performed to understand if CPF predicts the subsequent occurrence of new or recurrent venous ulcerations in a prospective study.
Conclusion
Plethysmography is endorsed for the assessment of venous disease by multiple societal organizations.20–22 Yet, it has been abandoned entirely for ultrasound at many medical systems, partly due to better reimbursement with ultrasound. Our findings demonstrate the ongoing utility of plethysmography and highlight one potential advantage over ultrasound. This study provides strong evidence that CPF is independently associated with active/prior venous ulcers and contributes to the severity of CVD. The observed threshold effect and EF gradient offer valuable insights for clinical practice and future research, and demonstrate the added value of plethysmography compared to ultrasound in the global assessment of CVD.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241311254 – Supplemental material for Relationship between calf muscle pump function and severity of chronic venous disease
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241311254 for Relationship between calf muscle pump function and severity of chronic venous disease by Atefeh Ghorbanzadeh, David Liedl, Hossam Elbenawi, Thom Rooke, Paul Wennberg, Robert D McBane and Damon E Houghton in Vascular Medicine
Footnotes
Acknowledgements
An editorial by Melvin et al. accompanies this article. 23
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.