
Abstract
It has been posited that the inflammatory process seen in atherosclerosis is underpinned by gut dysbiosis. Dysbiosis refers to alterations in the function, composition, and diversity of the human gut microbiota, all of which are influenced by endogenous and exogenous stimuli. Currently there is limited literature describing the association between gut microbiota and peripheral artery disease (PAD). This review summarizes the evidence surrounding the role of gut microbiota in the initiation of atherosclerosis (through direct infection of atherosclerotic plaque or systemic immune response to bacterial products and metabolites) and how dysbiosis may influence the various treatment modalities for PAD, including medical therapy (pharmacotherapy, lifestyle changes, and supervised exercise training) and surgery (endovascular and open revascularization). In particular, the role of short chain fatty acids (SCFAs), the effects of exercise on SCFA-producing and lactic acid bacteria (LAB) and, consequently, the lack of targeted research into dietary interventions and supplementation are highlighted in this review. This review highlights the potential for gut microbiota as not only a therapeutic target in patients with PAD, but also as a diagnostic and screening tool. It is imperative that the focus of future research is on the potential for personalized treatment which targets the gut microbiota (such as synbiotics, postbiotics, nicotinamide adenine dinucleotide (NAD) supplementation, selective antibiotics, resistance exercise, senolytics, and fecal microbial transplantation [FMT]) to be utilized as adjuncts to already existing treatment options for PAD. This review also highlights the potential role of biobanks and analysis of atherosclerotic plaques in further advancing knowledge and research in this area.
Introduction
The human gut microbiome is extremely diverse, comprising at least 10 trillion cells and 5 million distinct genes. 1 Most bacterial species in the adult human gut belong to the phyla Firmicutes and Bacteroidetes, along with less abundant phyla such as Actinobacteria, Proteobacteria, Fusobacteria, and Verrucomicrobia. 2 Dysbiosis refers to alterations in the function, composition, and diversity of the human gut microbiota, all of which are influenced by endogenous and exogenous stimuli2,3 (Figure 1). In turn, gut dysbiosis has been implicated in various disease states, with studies demonstrating the role of gut microbe-derived factors in many chronic inflammatory diseases such as inflammatory bowel disease and atherosclerosis.2,4
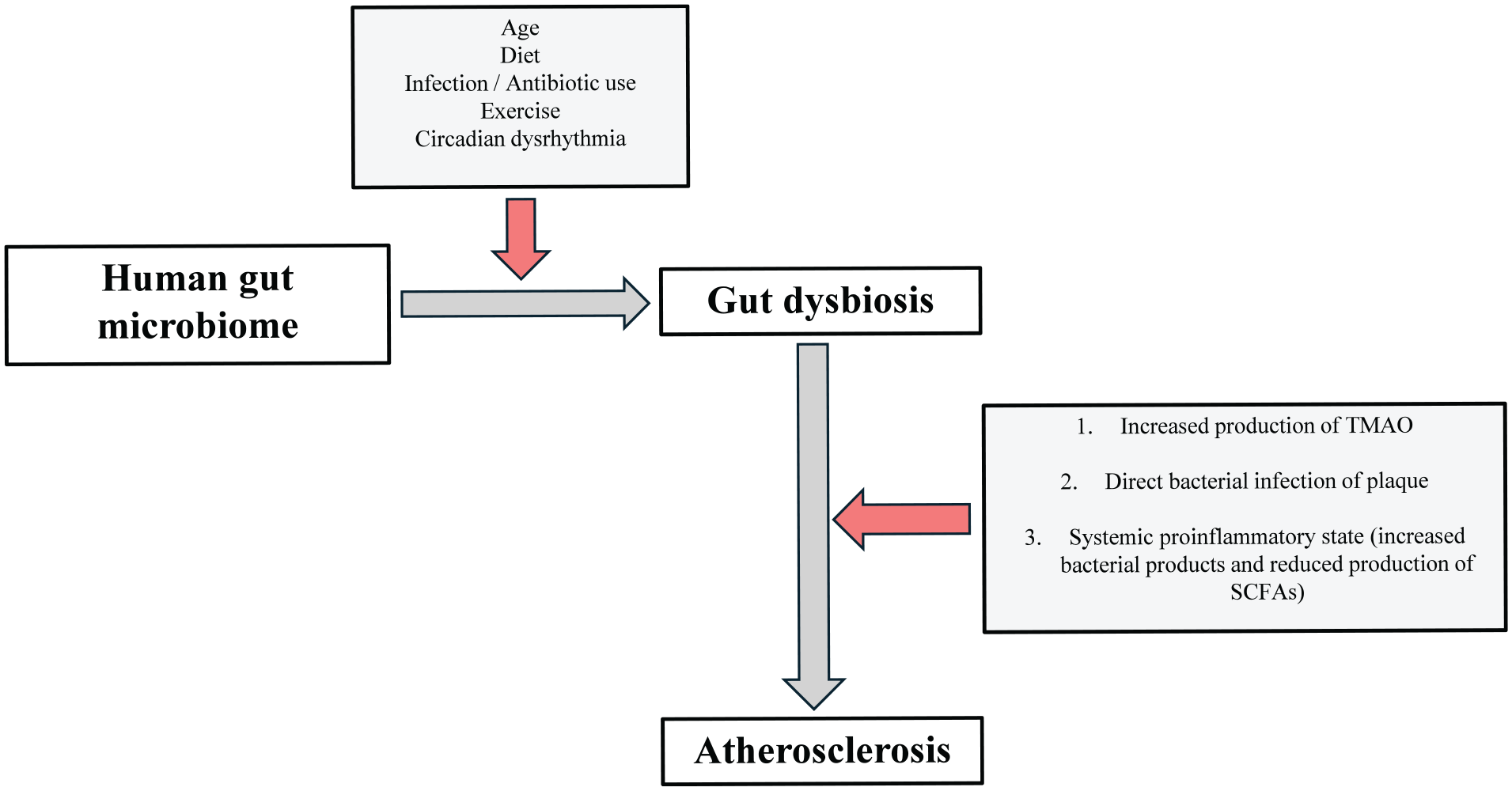
Proposed mechanisms by which the gut microbiota could contribute to the development and progression of atherosclerosis in peripheral artery disease.
Peripheral artery disease (PAD) is an occlusive disorder that reduces blood flow to the extremities. It affects over 200 million people worldwide, and its prevalence increases with age. 5 PAD presents as a spectrum of disease, ranging from claudication to chronic limb-threatening ischemia (CLTI). 6 Treatment of PAD encompasses a range of different strategies – best medical therapy (pharmacotherapy, dietary and lifestyle modifications) is implemented for all patients with PAD including those with asymptomatic disease, supervised exercise training (SET) is recommended for patients with claudication, and endovascular intervention or open revascularization is often necessary for those presenting with CLTI in the form of rest pain or tissue loss. 6
PAD is a local manifestation of atherosclerosis and, thus, this review provides a general overview on the role of gut microbiota in the development of this systemic disease state. More specific to PAD, one recent study reported interesting results suggesting that certain bacteria may be protective against the development of PAD, though the presence of others may be a risk factor. 7 Currently, there is limited literature addressing the role of gut microbiota in the management of lower-extremity PAD specifically, as opposed to other forms of atherosclerosis such as coronary or carotid artery disease. There have been significant advances in the surgical management of lower-extremity PAD, but there is a relative lack of progress in the medical management of those with less severe forms of PAD (asymptomatic or claudication). In order to provide an overview of the role gut microbiota plays in the initiation and progression of atherosclerosis and PAD, as well as in the various treatment options that are implemented for patients with lower-extremity PAD, a comprehensive literature search was conducted through electronic databases (PubMed, Cochrane, and Embase) using key words including “atherosclerosis”, “peripheral artery disease”, “endothelial dysfunction”, “gut microbiota”, and “dysbiosis”. Reference lists were scoped to further identify relevant studies for the review. Ultimately, this review will provide a framework from which future studies could be designed to test the utility of gut microbiome modulation as an adjunct to currently available treatment modalities, and as a novel therapeutic target for the prevention and treatment of PAD.
Gut microbiome in the development and progression of PAD
Several potential mechanisms have been identified by which the gut microbiota could contribute to the development and progression of atherosclerosis (Figure 1). Development of atherosclerotic plaques can be influenced by systemic or direct bacterial infection of cells within the vessel wall.2,8 –10 Indeed, Koren et al. detected bacterial DNA in atherosclerotic plaque that identified several bacterial phyla common to plaque, oral cavity, and fecal samples from the same individual. 8 Studies have also demonstrated that certain bacteria are more abundant in the oral cavity of symptomatic patients than in those of patients with asymptomatic disease. 10 It would be interesting to correlate atherosclerotic plaque morphology with bacterial content of the plaque and gut of asymptomatic patients to determine whether patients with ‘vulnerable plaques’ demonstrate a unique microbial profile. This highlights the potential role of biobanks in advancing our knowledge on the specific organisms involved and could also provide valuable insight into the utility of gut microbiota as a screening tool to determine which asymptomatic patients would benefit from early arterial intervention.
Other potential mechanisms include activation of the innate immune system by bacterial products such as lipopolysaccharides, the processing of dietary constituents, and production of metabolites that enter the circulation. 2 The main products of the bacterial fermentation of carbohydrates and proteins are short chain fatty acids (SCFAs) such as acetate, propionate, and butyrate, and it has been proposed that a reduction in SCFA-producing bacteria (including Veillonellaceae and Akkermansia) may impair intestinal permeability leading to bacterial translocation and low-grade endotoxemia. 11 This in turn leads to the systemic pro-inflammatory state that is pivotal in the pathophysiology of atherosclerosis.
Trimethylamine N-oxide (TMAO) is a derivative of TMA, which in turn is generated from multiple nutritional precursors including choline,
Gut microbiome in the management of PAD – medical therapy
Management of PAD is guided by the severity of disease. In patients with asymptomatic disease or claudication, treatment strategies focus on risk profile modification aimed at preventing progression of disease and reducing the risk of major adverse cardiovascular events. 6 Best medical therapy for PAD involves smoking cessation, exercise, as well as the use of pharmacotherapy and dietary strategies to improve glycemic control, optimize blood pressure management, and improve lipid profile. 6 The dynamic nature of the gut microbiome means that many of these interventions have the capacity to augment it.
Pharmacotherapy
Some of the more commonly prescribed medications in patients with PAD include antiplatelets and anticoagulants, antihypertensives, oral hypoglycemics, and statins. Studies have reported on the complex bi-directional interaction that exists between commonly used medications and the human gut microbiome. 21 For instance, certain medications may induce gut dysbiosis by disturbing the gut epithelial barrier (e.g., proton-pump inhibitors reducing the acidity barrier of the stomach), and others may directly promote or inhibit the growth of specific bacteria within the intestines. 21 The gut microbiome in turn may metabolize and enzymatically transform the structure of certain drugs, thereby altering the drugs’ absorption, distribution, excretion, and consequently, their efficacy and therapeutic outcomes.22,23
Statins or 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors are an integral part of pharmacotherapy in patients with cardiovascular disease. 23 There is strong evidence supporting the use of statins in patients with PAD. 6 The use of statins is associated with a reduction in cardiovascular-related mortality, mainly through their lipid-lowering effects, as well as through reduction of systemic inflammation and stabilization of atherosclerotic plaque. 23 However, the response to statin therapy varies greatly between individuals, and one interesting proposal is that the gut microbiome can directly modify statin activity and, thus, differences in microbial composition can lead in turn to changes in statin efficacy. 24 Dias et al. found that the lipid-lowering effect of statins were attenuated in the presence of intestinal dysbiosis. 25 On the other hand, Dias et al. also reported that in almost all studies there were significant variations in gut microbiota diversity after statin intake. 25 Other studies have shown that individuals who had a more satisfactory response to statin therapy had higher levels of microorganisms belonging to the Firmicutes phylum and increased proportions of Lactobacillus and Bifidobacterium genera. 24 One study investigated the role of statins in modulating the gut microbial composition. This study showed that in patients with hypercholesterolemia, those treated with statins had increased proportions of antiinflammatory bacteria (Akkermansia muciniphila and Faecalibacterium prausnitzii). 26 This may be important to mitigate the systemic pro-inflammatory state of PAD.
Diet
Optimizing nutritional status is often overlooked in the management of PAD, with poor quality diet and low levels of physical activity commonly resulting in protein and micronutrient deficiencies in this vulnerable cohort. 13 Diet is often worse as patients progress to the more advanced and severe stages of PAD. A 2019 review suggested that growing evidence on the interplay between diet and the gut microbiome may help further strengthen the importance of medical nutrition therapy in the various stages of the PAD process. 27 Nutritional supplementation (such as vitamin D, vitamin E, and omega-3 fatty acids) should be considered in all patients with PAD to augment endothelial function and thus prevent progression of the atherosclerosis process, as well as to improve wound healing in patients with CLTI and tissue loss. 27
Diet and nutrition are strongly linked to the composition and diversity of the human gut microbiome. 28 Different dietary compounds (carbohydrates, proteins, lipids) and microbial metabolites (such as SCFAs, ammonia, hydrogen sulfides, and bile acids) have been shown to modify the composition and function of the gut microbiota. 29 A comprehensive review by Ross et al. described the mechanisms by which certain diets shape the gut microbiota. 28 A high-fat diet or Western diet has traditionally been associated with many cardiovascular risk factors (including obesity, diabetes mellitus, hypertension, and dyslipidemia) that increase the risk of developing atherosclerosis. Studies have shown that the gut microbiota is altered in patients with obesity, with an increase in the Firmicutes to Bacteroidetes ratio. 30 In addition to the direct effects of this diet on cardiovascular health, it has been shown to significantly alter the gut microbiome diversity, resulting in reduced SCFA production and increased TMAO concentrations, thereby promoting the development of atherosclerosis. 28 In contrast, a high-fiber diet positively alters the composition of the gut microbiome, with increased levels of Lactobacillus and Bifidobacterium genera. 28
Gut microbiome in the management of PAD – supervised exercise training
Supervised exercise training (SET) is a noninvasive treatment strategy for patients with PAD and claudication. 31 There is a large body of evidence supporting the role of supervised exercise as part of the initial treatment strategy in all patients with claudication.31 –34 Randomized controlled trials have consistently demonstrated the beneficial effects of SET on symptomatic improvement in this cohort of patients, with a greater increase in both maximal and pain-free walking distance.31,32 Many factors influence the efficacy of exercise in providing symptomatic improvement in patients with PAD, and the effects of exercise on the composition and function of the human gut microbiota have been the topic of interest in many studies.35 –43
Short chain fatty acid (SCFA)-producing bacteria
What is becoming clear, however, is that communication between the gut and skeletal muscle (the gut–muscle nexus) is mediated via SCFA. 44 SCFAs such as propionate, acetate, and butyrate have multiple antiatherogenic actions. 45 Potential mechanisms that have been proposed to explain the efficacy of exercise include decreased adhesion of monocytes to the activated endothelium (thereby attenuating a key step in the development of atherosclerotic plaque), inhibition of vascular smooth muscle cell (VSMC) proliferation, and increased collagen deposition resulting in greater plaque stability. 46 In particular, butyrate has been shown to prevent atherosclerosis in mouse model studies. 47 SCFA-producing bacteria are increased during physical exercise, and this may support the idea that targeting the gut microbiome can provide a beneficial or additive effect on supervised exercise training.
Current research reports a higher abundance of health-promoting bacterial species and increased microbial diversity in athletes,35 –37,48,49 with one study demonstrating that the gut microbial composition of athletes is distinct from that of nonathlete individuals with elevated abundances of SCFA-producing bacteria including Veillonellaceae, Bacteroidetes, Prevotella, Methanobrevibacter, and Akkermansia. 50 Clarke et al. demonstrated significant differences in the gut microbial composition between male professional rugby players and a cohort of nonathlete male controls. 35 Notably, the athletes had significantly greater diversity of microbiota, with elevated levels of the Akkermansia genus. 35 A subsequent study of the same cohort concluded that athletes had a higher abundance of SCFA metabolic pathways. 36 In another study, Petersen et al. investigated the gut microbiome of cyclists and demonstrated higher levels of Akkermansia (a butyrate-producing, antiinflammatory bacteria), which has been shown to exert protective effects against atherosclerotic plaque progression in mice models.37,43
The question remains, however, as to how this change in gut microbial diversity and composition associated with exercise differs between supervised training in patients with PAD (aging and medically comorbid patients) compared to the high-intensity exercise performed by professional athletes. Further research is needed to investigate whether the duration and intensity of exercise is associated with significant differences in gut microbial composition, and whether this could be applied clinically to improve the efficacy of SET in patients with PAD and claudication.
Lactic acid bacteria
In addition to SCFA-producing bacteria, studies have demonstrated increased levels of lactic acid bacteria (LAB) in athletes. The unique ability of lactic acid bacteria to further convert lactate in the intestine may be an important link in establishing the association between gut microbiota, PAD and claudication, and SET (Figure 2). Lactate accumulation is a hallmark feature of the ischemia/reperfusion cycle that occurs in claudicants, with the consequent decrease in adenosine triphosphate (ATP) levels and intracellular pH leading to a cascade of reactions that ultimately result in tissue injury and/or death. 51 In a study by Scheiman et al., the bacterial genus Veillonella was found to be more prevalent among marathon runners compared to a nonathlete control group. 52 Scheiman et al. demonstrated that systemic lactate can cross the epithelial barrier into the gut lumen. 52 The lactate generated during sustained bouts of exercise can subsequently be metabolized by lactate-metabolizing organisms (including Veillonella species) and converted to SCFAs acetate and propionate that improve athletic performance 52 (Figure 2).
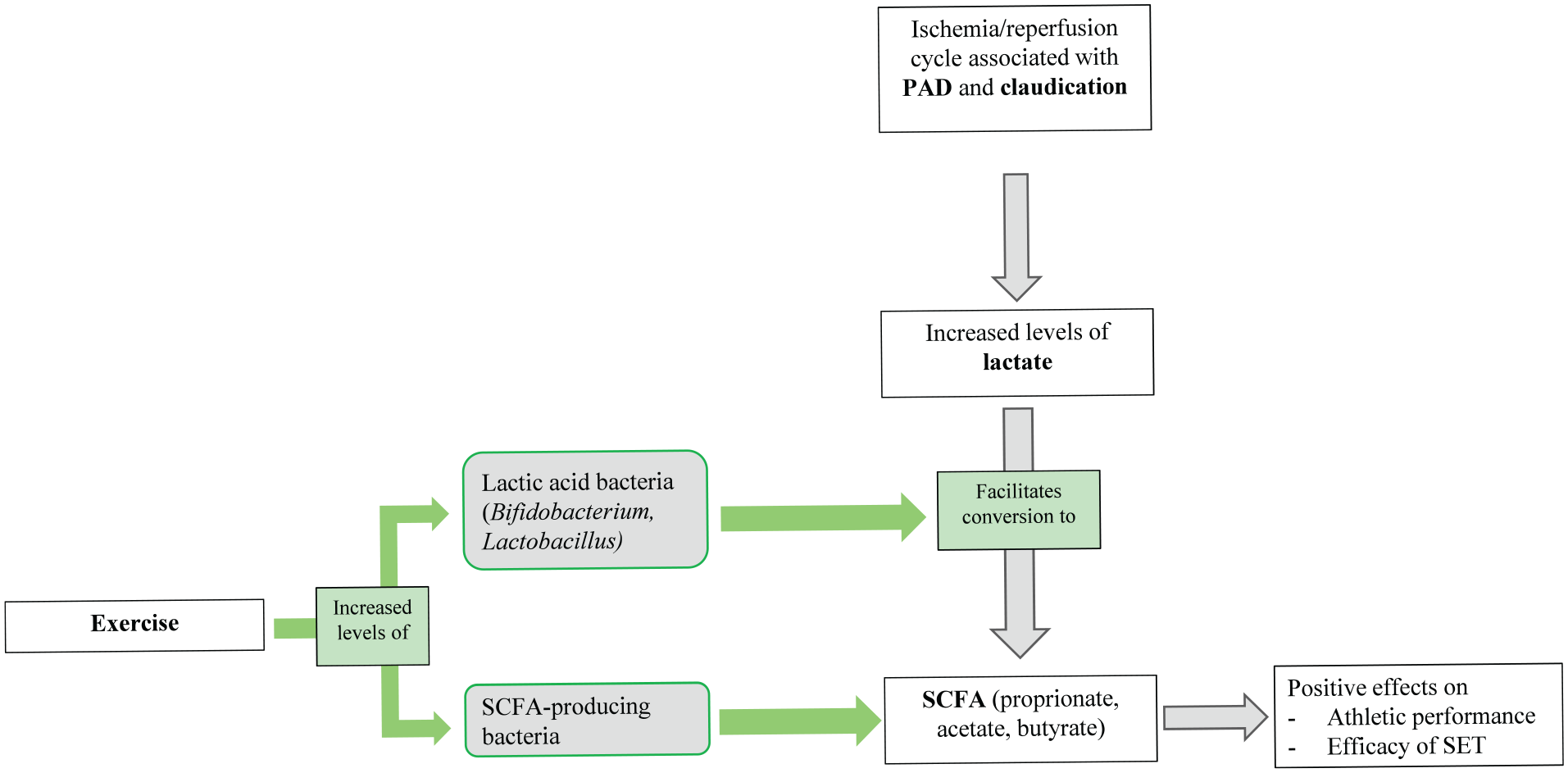
The positive effects of exercise on the gut–skeletal muscle nexus with higher abundance of SCFA-producing and lactic acid bacteria.
Gut microbiome in the management of PAD – endovascular intervention and open revascularization
PAD is a spectrum of disease, with CLTI representing the end-stage of PAD. It is associated with high morbidity (pain and limb loss) and mortality. Best medical therapy and aggressive risk factor modification is critical in patients with CLTI for both limb salvage and reduction of cardiovascular morbidity and mortality. Ultimately these patients will require surgical revascularization in the form of endovascular and open interventions. Early failure following minimally invasive endovascular intervention is common, leading to high rates of re-intervention. Predicting which interventions are more prone to failure is challenging as there are many factors associated with failure after intervention (including lesion length, severity, and location of disease). Here, we explore the potential role that the gut microbiota plays in the development of two important processes that greatly influence the treatment of PAD – neointimal hyperplasia and vascular calcification.
Neointimal hyperplasia
Neointimal hyperplasia refers to pathological remodeling of the vessel wall following arterial intervention, and this is due to proliferation and migration of VSMCs into the tunica intima layer. 53 It is a prevalent cause of restenosis after many vascular procedures, with up to 50% of treated vessels restenosing within 1 year due to neointimal hyperplasia. 53 The mechanisms underlying the variable propensity for neointimal hyperplasia between individuals are poorly understood. Studies have investigated the role of gut microbiota in mediating inflammatory and cell proliferative pathways that drive neointimal hyperplasia.53 –57
One study demonstrated the impact of gut microbiota on both systemic and local arterial inflammation and found that germ-free mice have attenuated neointimal hyperplasia development, with less local VSMC proliferation in the media and adventitia. 56 Another study found that germ-free mice develop significantly less neointimal hyperplasia 4 weeks after unilateral carotid ligation compared with an age- and sex-matched conventionally raised cohort. 55 Re-establishment of the gut microbiota in these germ-free mice through fecal transplantation resulted in restoration of the arterial remodeling response and consequent neointimal hyperplasia. 55
Microbiome-modulated metabolites derived from dietary nutrients have been studied as potential biomarkers for atherosclerotic disease burden, with one study demonstrating an association between specific microbe-derived metabolites and ankle–brachial index (a surrogate for disease burden) as well as postoperative cardiac events (in patients who underwent major vascular procedures including carotid endarterectomy, leg bypass, and major limb amputation). 57 The study of these microbiome-modulated metabolites opens possibilities for the development of novel biomarkers to identify and specifically treat those individuals who are more prone to complications such as neointimal hyperplasia.
Interestingly, a study by Nooromid et al. found that microbe-derived butyrate (SCFA) has a protective role in neointimal hyperplasia development after arterial injury. 53 In this study, vancomycin-treated mice had significantly more neointimal hyperplasia development after femoral artery injury, and this correlated with lower levels of SCFA (butyrate, acetate, and propionate) in stool and serum samples. 53 Patients with PAD are often treated with prolonged courses of potent antibiotics (for arterial ulcers or diabetic foot infections). Hence, it is important to consider whether the finding that antibiotics influence gut microbiota resulting in reduced SCFA levels and increased neointimal hyperplasia, translates to humans. Again, it would be interesting to study the role of probiotics in this patient cohort, and whether probiotic supplementation can negate the harmful effects of antimicrobial therapy on the gut microbiome and ultimately promote wound healing.
Vascular calcification
Vascular calcification is defined as the pathological deposition of calcium phosphate crystals within the medial or the intimal layers of an artery. 58 Intimal calcification, or the calcification of atherosclerotic plaques, is often linked to inflammation. Medial calcification, which occurs independently of inflammation and the atherosclerotic process, is characterized by transformation of VSMCs into osteoblast-like cells.59,60 This can be observed with aging, as well as certain disease states including diabetes mellitus and chronic kidney disease (CKD). Understanding the role of gut microbiota-derived metabolites in the development of vascular calcification is critical in the treatment of patients with PAD, given the well-established association between calcification and poor outcomes following endovascular procedures.61,62
Though there are limited studies on whether patients with vascular calcification demonstrate a specific gut microbial profile, existing studies on patients with CKD (which represents an important subset of patients with PAD) may help advance knowledge in this area.59,60,63 –65 Studies on patients with CKD have demonstrated an abundance in the bacterial phyla Firmicutes, Proteobacteria, and Actinobacteria, with an associated decrease in levels of Lactobacilli and Roseburia. 63 Furthermore, fecal analysis of dialysis patients has shown a decreased level of the SCFA butyrate, and this could be associated with the development of vascular calcification in this cohort. 64 Future studies are needed to determine if gut dysbiosis in the absence of other risk factors, such as CKD, increases an individual’s risk of developing vascular calcification. This will have several implications in the surgical management of patients with PAD. First, identifying those with a gut microbiota profile susceptible to vascular calcification is important when considering endovascular versus open revascularization. Furthermore, modulation of gut microbiota in patients with diabetes mellitus or CKD may be a potential strategy to reduce vascular calcification and allow for a greater range of treatment options and a higher interventional success rate in this cohort of patients.
Wound healing
Wound care is vital in the management of patients with PAD. These patients often present with necrotic ulcers in the context of CLTI, diabetic foot ulcers, or pressure-related neuropathic ulcers. Wound healing is influenced by many local (infection, pressure, edema, foreign bodies) and systemic (age, nutrition, immunosuppression, smoking) factors, and studies have suggested that modulation of the gut microbiome may help promote wound healing through regulation of the systemic inflammatory response.66 –72 As discussed above, the systemic pro-inflammatory state that is seen in patients with PAD is a result of gut dysbiosis, which leads to a reduction in SCFA-producing bacteria such as Veillonellaceae and Akkermansia.11,71 A study by Mohtashami et al. demonstrated the potential for certain strains of Lactobacillus to improve the healing of diabetic wounds through inflammatory regulation. 68 The proposed mechanism by which these organisms aid in the wound healing process is through modulation of inflammatory cells within the wounds (by enhanced migration, proliferation, and greater viability of fibroblasts and macrophages). 68 In addition to the promising role of probiotics described in the previous sections, the use of probiotics containing either SCFA-producing bacteria or Lactobacillus strains may also aid in the positive regulation of gut microbiota to improve wound healing in this vulnerable cohort.
Potential treatments targeting the gut microbiota
Probiotics are food supplements containing live bacteria that confer a benefit to the host when ingested in adequate amounts. 73 The majority of probiotic strains are representatives of the LAB group, including Bifidobacterium and Lactobacillus that are capable of lactic acid fermentation (the metabolism of carbohydrates and conversion into ATP and lactic acid).42,73 Probiotic supplementation has been shown to beneficially modify a number of major atherosclerosis-associated cardiovascular risk factors including hypertension and dyslipidemia, although not all probiotic strains have been shown to be antiatherogenic. 73 A study by Bielik et al. demonstrated that the combination of high-intensity training in competitive swimmers and use of probiotics conferred a greater benefit in increasing gut bacterial diversity, reflected by an increase in the abundance of lactic acid bacteria. 74
Future studies could focus on whether the findings demonstrated in professional athletes (the relative increase in lactic acid bacteria and SCFA-producing bacteria) can be replicated in patients with PAD. It would be interesting to study the role of probiotics in this population and, in particular, whether the use of probiotics containing LAB could augment the beneficial effects of supervised exercise training in patients with intermittent claudication.
Furthermore, studies have demonstrated that the levels of microbial SCFAs and certain butyrate-producing bacteria (such as Firmicutes) are both inversely proportional with age. 75 Age is an important consideration, especially in the vascular disease cohort, and this finding further highlights the need for targeted research into dietary interventions and supplementation with SCFAs and probiotics containing SCFA-producing bacteria. With multiple factors including age, diet, and exercise playing a role in the function, composition, and diversity of gut microbiota, the potential to manipulate dietary intake with the use of probiotics provides a promising avenue to help mitigate the debilitating symptoms of claudication within the aging PAD population (Figure 3).
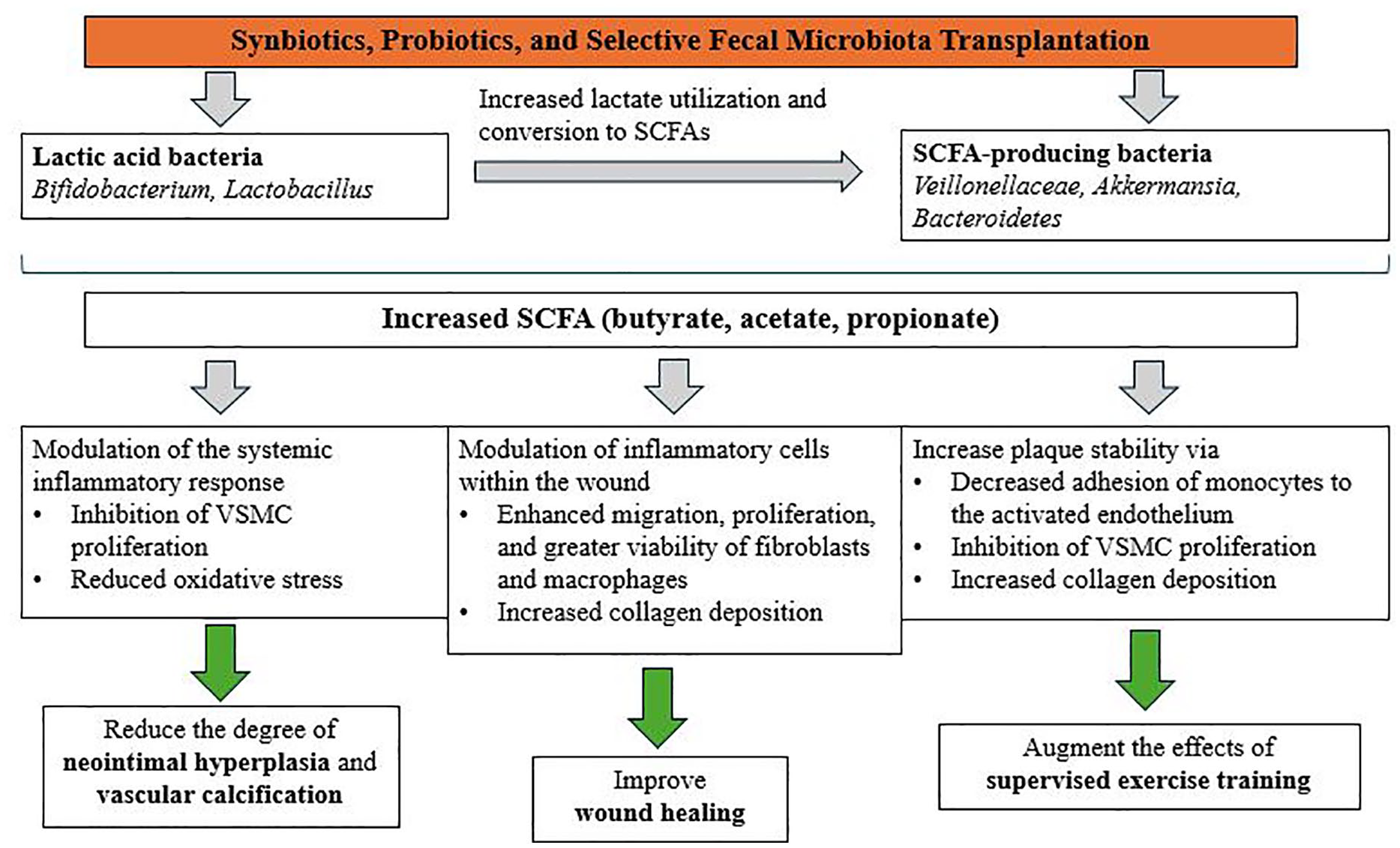
Proposed role of probiotics in the management of peripheral artery disease.
Conclusion
In the age of personalized medicine, human gut microbiota has served as an exciting focus of many studies as a potential therapeutic target for various diseases. Gut dysbiosis plays a crucial role in the development and progression of atherosclerosis and PAD, either through a systemic immune response to certain bacterial products or via direct bacterial infection of atherosclerotic plaque. This review has provided an overview of how gut microbiota plays a role in the various stages of treatment for patients with PAD and has highlighted the potential for gut microbiota as not only a therapeutic target, but also as a diagnostic and screening tool. Most notably, the effects of exercise on SCFA-producing bacteria and lactic acid bacteria raise the possibilities for modulation of the gut microbiome in improving PAD symptoms and improving treatment outcomes. Given that age is a risk factor for PAD and the diversity of the gut microbiome is known to decrease with age, it is imperative that future research focus on the potential for personalized treatment which targets the gut microbiota (such as synbiotics, postbiotics, NAD supplementation, selective antibiotics, exercise, senolytics, and fecal microbial transplantation) to be utilized as adjuncts to already existing treatment options for PAD.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.