
Abstract
Introduction:
The transition to an outpatient setting for endovascular treatment of lower-limb peripheral artery disease (PAD) remains slow, and obstacles persist. The aim of this study was to identify the obstacles to its development, according to vascular interventionalists.
Methods:
Between September 2022 and October 2023, all French vascular interventionalists, who were members of the participating societies, were asked to answer an online questionnaire on their outpatient setting practice for PAD endovascular treatment. The questionnaire explored patient selection criteria (medical and social), treatments, follow up, and potential obstacles.
Results:
Of the 279 respondents (43%), 228 (82%) were currently performing endovascular treatment of PAD on an outpatient basis. Most interventionalists (n = 179, 79%) declared that an outpatient setting practice did not alter their technical approach. Age, obesity, chronic limb-threatening ischemia (CLTI), and chronic renal failure were not considered exclusion criteria for an outpatient setting by more than half of the respondents. Long iliac and femoropopliteal thrombosis were considered exclusion criteria by 48 (21%) and 75 (33%) of them, respectively. Interventionalists estimated the rate of potentially eligible patients at 58.3 ± 22.5%. Social isolation (lack of comprehension, communication means, or company) was considered the main exclusion criterion for more than 90% of the respondents. Medico-legal risks were identified as the main obstacle for 39% of interventionalists not practicing outpatient care.
Conclusion:
This prospective study identifies, from the perspective of vascular interventionalists, medico-legal risks, social isolation, and the complexity of lesions as the main obstacles to the transition to an outpatient setting for endovascular treatment of lower-limb PAD.
Keywords
Introduction
In the evolving landscape of medical practice, the outpatient setting in surgery, defined by the American Hospital Association as a scheduled surgical procedure performed on patients who do not remain in hospital overnight, 1 stands as a testament to the pursuit of promoting minimally invasive interventions that promise enhanced patient outcomes and reduced healthcare burdens. The increasing incidence of cardiovascular risk factors among an aging population accounts for the increasing burden of lower-limb peripheral artery disease (PAD) worldwide and is regardless of income level. The incidence of PAD was estimated at 10 million patients worldwide and is considered as the third cause of cardiovascular morbidity. Endovascular therapies have revolutionized the treatment of PAD, leading to a shift from open to endovascular surgery for most PAD indications.2,3 The safety and efficacy of endovascular revascularization performed in an outpatient setting has been confirmed in many different studies over the past decade.4–7
To facilitate the development of outpatient surgery in France, national guidelines from the French Society of Vascular and Endovascular Surgery (SCVE) were released in 2019 to provide a framework for practitioners willing to integrate this practice and confront some legal issues. 8 However, obstacles seem to persist and the widespread adoption of an outpatient setting by vascular interventionalists seems to deal with the multifaceted challenges of both healthcare systems and clinical practice, which vary considerably among countries and regions. Although the proportion of French establishments offering endovascular treatments on an outpatient basis and with an activity of at least 10 patients per year has more than tripled since 2015 (10% vs 34.5%, respectively, in 2015 and 2022), it remains far below the 60% reported in the USA. In France, this rate also varies from zero to > 20% from one department to another. 9
The aim of this study was to assess the practice of lower-limb PAD endovascular repair performed in an outpatient setting in France and attempt to identify the medical, social, institutional, and psychological obstacles to its development, highlighting those that can be applicable more widely throughout the world. This survey-based study is, to our knowledge, the first one that assesses the point of view of vascular interventionalists on their daily practice. By exploring the intricacies of this management, we aim to shed light on the obstacles hindering its widespread adoption to identify potential avenues for overcoming these barriers in future.
Methods
Questionnaire and procedures
From September 2022 to October 2023, two national associations of vascular interventionalists asked their members to answer an anonymized online questionnaire on their practice of outpatient endovascular treatment for lower-limb PAD. The questionnaire, reported in the supplementary material, was completed on a voluntary basis. The questionnaire was designed by two of the co-authors and comprised 52 questions. Questions explored the interventionalists’ demographic and institution information, patient selection criteria (medical and social), endovascular procedures, follow up, and potential obstacles. Procedures were defined as aortic (excluding visceral or renal arteries), iliac, and infrainguinal endovascular revascularization for lower-limb PAD. Social isolation was defined as difficulty being accompanied at home following the procedure, and/or living a long way from any emergency department, and/or understanding difficulties (language or cognitive barrier), and/or having no access to phones or any other efficient communication modes.
This work is an anonymized user survey not involving any patient and did not require the approval of an ethics committee. No personal data were collected during this work.
Statistical analysis
Descriptive statistics were calculated for the analysis of continuous variables: means ± SD, median (interquartile range), and minimum and maximum. For nominal values, absolute numbers and relative frequencies were determined. For quantitative variables, the normal distribution was verified using graphical methods such as histograms, boxplots, and Q-Q plots, and statistical tests such as Shapiro–Wilk test or Kolmogorov test. For quantitative variables, normally distributed, Student’s t-test was computed; for ordinal variables and quantitative variables where severe departures from normality were observed, the Wilcoxon–Mann–Whitney test was computed. For qualitative variables, the chi-squared test was computed or Fisher’s exact test if the expected frequency of < 20% of categories was under 5.
The significance level is defined as p < 0.05. All analyses were computed with SAS software version 9.4 (SAS Institute, Inc.).
Results
Questionnaires were collected from 279 respondents from a population of 654 vascular interventionalists (after removing duplicates) who were surveyed over a 12-month period (Figure 1), which is a response rate of 42.7%. Among the 279 respondents (278 vascular surgeons and one interventional radiologist), 228 (81.7%) declared they were already performing endovascular lower-limb PAD revascularization in an outpatient setting. They stated they had been practicing this type of management for an average of 8.2 ± 7.6 years. Fifty-one (18.3%) declared performing all lower-limb PAD endovascular procedures through an inpatient setting only. The median number of endovascular lower-limb PAD revascularization cases declared per practitioner was 150 (90–200) per year. Interventionalists used to practicing outpatient surgery declared an approximate number of 30 (10–87) procedures per year performed through this type of hospitalization. Among all respondents, 197 (70.6%) were private practice and 61 (21.9%) were working in public hospitals (Supplemental Figure S1). The median age of the respondents was 52 (42–60) years old. All French regions were represented (Figure S1).
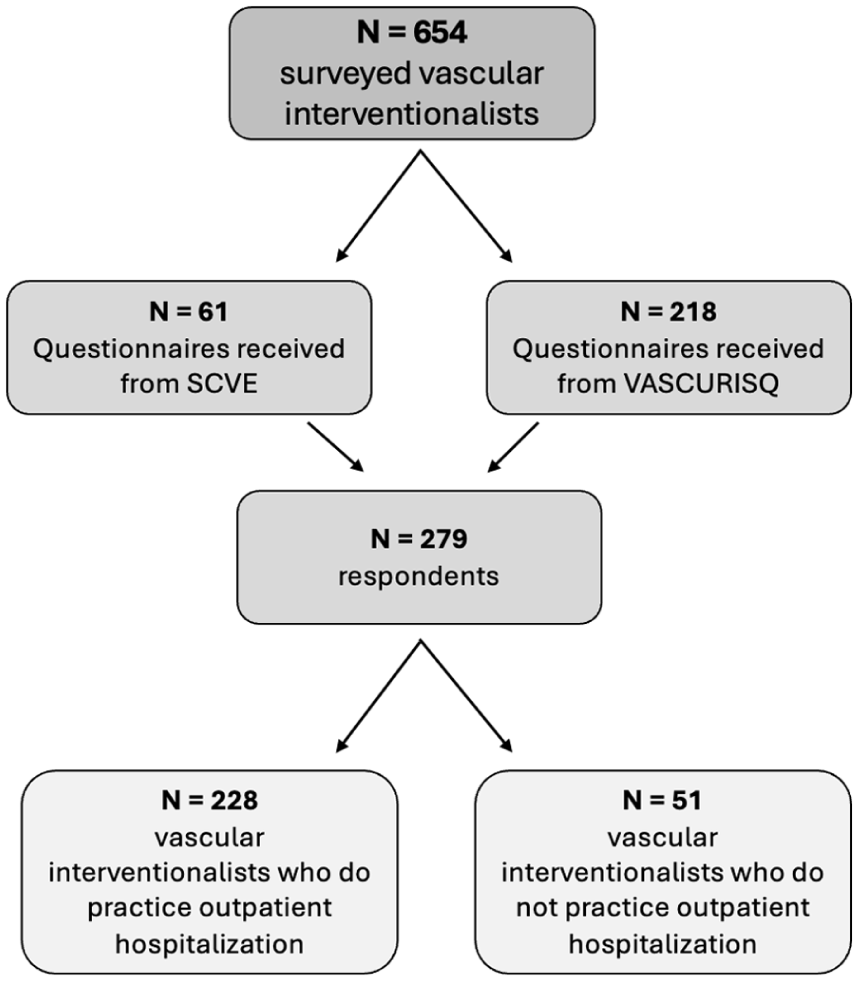
Study flow chart.
Patient selection
Vascular interventionalists’ adherence to guidelines regarding patient selection is described in Figure 2. Out of the 228 interventionalists who practice outpatient surgery, 70 (30.7%) declared considering an age ⩾ 70 years old as a contraindication for outpatient management. Body mass index (BMI) ⩾ 30 kg/m2 was also considered a contraindication for 74 of them (32.5%). Sixty percent of the practitioners declared treating patients with chronic kidney disease (CKD) in an outpatient setting, with 43% considering CKD stage > 3b as a contraindication for outpatient management. However, 80 of them (35.1%) claimed treating patients assigned ⩾ 3 on the American Society of Anesthesiologists (ASA) Physical Status Classification System. Concerning clinical status and lesions, chronic limb-threatening ischemia (CLTI) was considered a contraindication for 46.9% of the interventionalists (n = 107). Some practitioners did not propose ambulatory management in cases of iliac thrombosis (21%, n = 48), femoropopliteal thrombosis > 15 cm (32.9%, n = 75), or below-the-knee thrombosis (33.3%, n = 76).
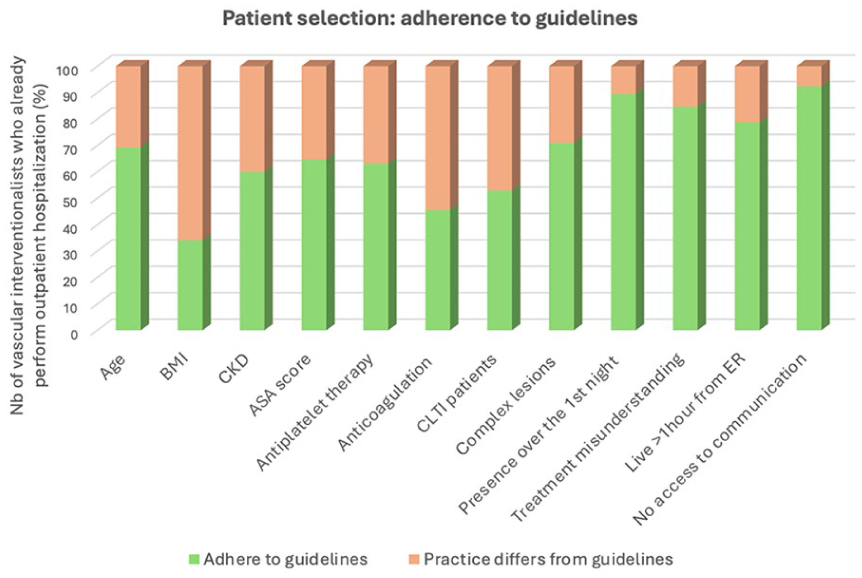
Adherence to the French guidelines regarding patient selection among vascular interventionalists who already use an outpatient setting. See Appendix for detailed criteria.8
Double antiplatelet therapy and anticoagulation therapy were considered as contraindications for outpatient management for 36.8% (n = 84) and 54.4% (n = 124) of the respondents, respectively.
Regarding social criteria, most of the interventionalists confirmed following the guidelines and thus did not propose ambulatory surgery to patients who were not accompanied for the first night following the procedure (89.5%, n = 204), were not able to understand their treatments (84.6%, n = 193), lived more than 1 hour from a medical center (78.9%, n = 180), or did not have access to a phone (92.5%, n = 211).
Interventionalists who performed more than 30 outpatient procedures per year (n = 112) would more likely include patients under double antiplatelet therapy and anticoagulation, elderly patients, patients suffering from obesity, and patients presenting with CLTI or with complex lesions (Table 1).
Patient selection for an outpatient setting, determined by the annual volume of outpatient procedures by physicians who already perform in an outpatient setting.
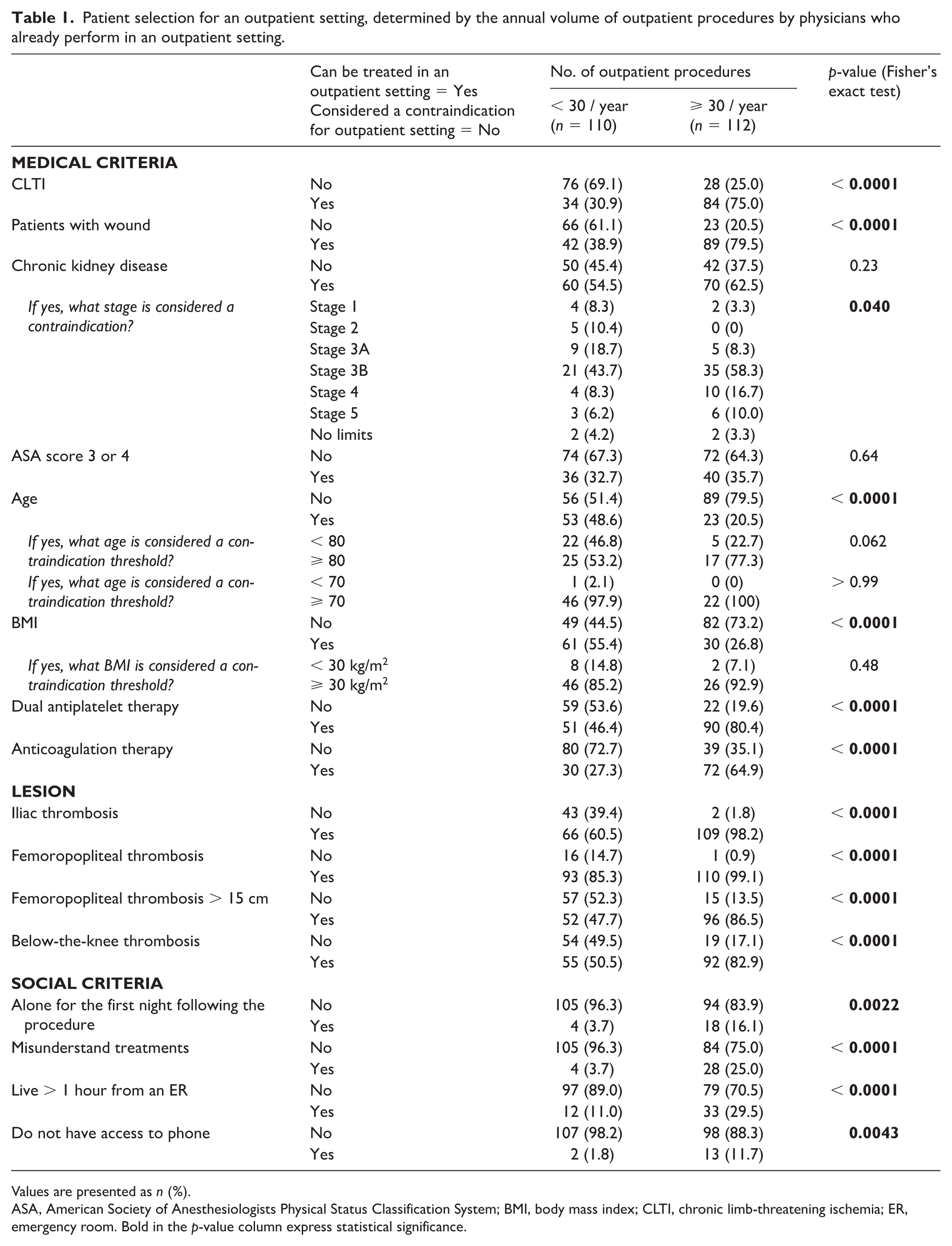
Values are presented as n (%).
ASA, American Society of Anesthesiologists Physical Status Classification System; BMI, body mass index; CLTI, chronic limb-threatening ischemia; ER, emergency room. Bold in the p-value column express statistical significance.
Outpatient setting
Among all respondents, different outpatient settings were described. A dedicated ward for ambulatory management was provided by the institution for 277 (99.3%) of them, whereas only 49 (17.6%) could benefit from a dedicated operating room. A significant 43% of the respondents (n = 121) declared performing outpatient procedures only on morning operating-room shifts.
Endovascular procedures
Procedural details such as type of anesthesia, use of ultrasound-guided puncture, approach, and preoperative heparin bolus are described in Table 2.
Procedure characteristics for vascular interventionalists (N = 228) who perform outpatient surgery for PAD.
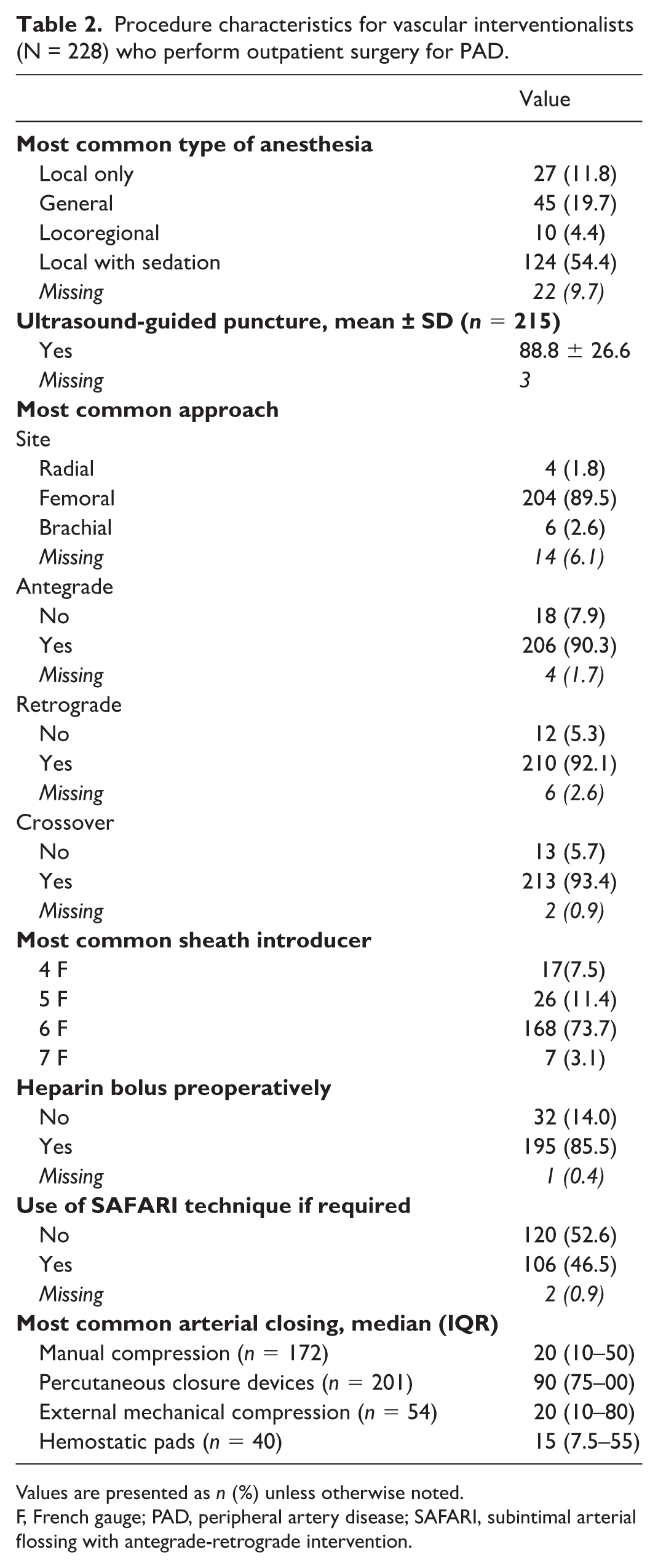
Values are presented as n (%) unless otherwise noted.
F, French gauge; PAD, peripheral artery disease; SAFARI, subintimal arterial flossing with antegrade-retrograde intervention.
Almost half of the respondents (n = 106, 46.5%) declared also performing subintimal arterial flossing with antegrade-retrograde intervention (SAFARI technique) in the outpatient setting.
Regarding arterial closing, outpatient management did not contraindicate the use of exclusive manual compression for 172 (75.3%) respondents, even though only 36.6% (n = 63/172) of them use it in more than 30% of their cases. Percutaneous closure devices were used by 201/228 vascular interventionalists (88.2%) who performed outpatient surgery, for 82% of their cases on average. Fifty-four interventionalists (31.4%) used external mechanical compression devices but in 39.4 ± 36.7% of cases on average. Forty interventionalists (17.5%) declared using hemostatic pads during manual compression (such as Axiostat, Merit Medical, UT, USA) but in only 32 ± 34% of cases on average.
A total of 179 (78.5%) respondents declared that outpatient management did not impact their overall procedural choices. Only 21.3% (n = 48) declared that they were using more closure devices if the procedure was performed as an outpatient. Less than 10% of vascular interventionalists declared modifying their habits such as using less heparin or less stenting if practicing outpatient compared to inpatient surgery.
Postprocedure surveillance
Patients were kept in surveillance for an average of 4.7 ± 1.5 hours before they were authorized for discharge. A total of 207 (90.8%) respondents declared giving a report to the patient prior to discharge and 201 (88%) declared that patients are called back within the first 24 hours following the intervention, most frequently by a nurse (82%). Only eight respondents (3.5%) declared using a connected device or mobile application for patient monitoring postdischarge.
Obstacles to outpatient management
The remaining obstacles and gaps are described in Figure 3. Among the vascular interventionalists who do not practice outpatient surgery (n = 51/279), the main obstacles to the transition to ambulatory care in their institution were medico-legal risks (39.2%, n = 20), patient exclusion due to social criteria (19.6%, n = 10), lesions complexity (13.7%, n = 7), and lack of medico-economic incentive (11.8%, n = 6). One of them (1.2%) did not see any obstacle (Figure 3A).
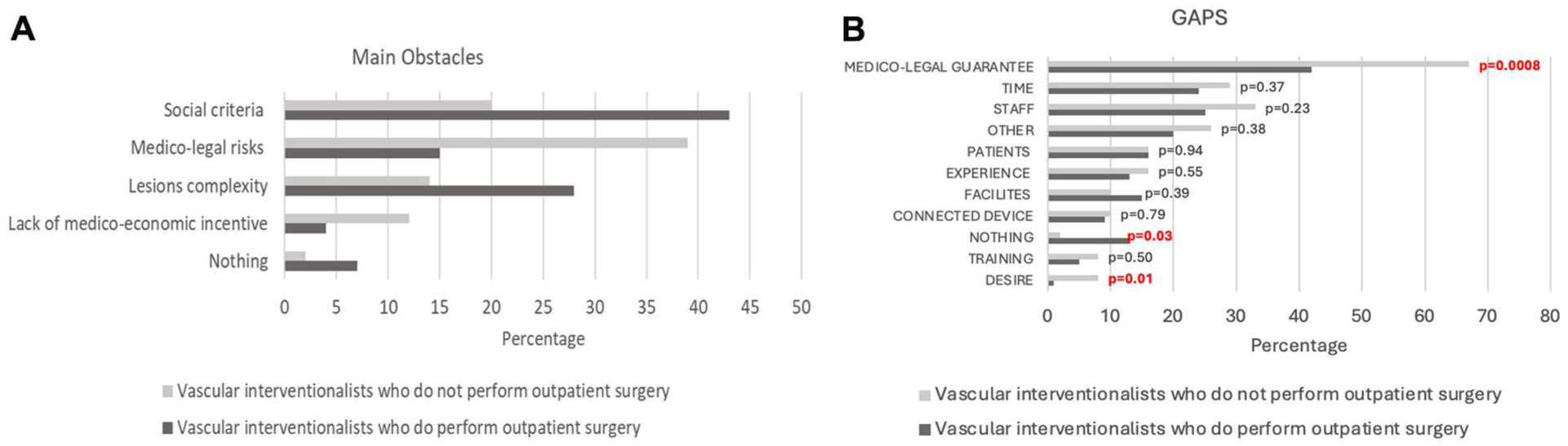
Criteria identified as obstacles and gaps in different proportions depending on vascular interventionalists who already do or those who do not practice outpatient surgery.
Among the vascular interventionalists who do practice outpatient surgery (n = 228/279), the main obstacles to the transition to ambulatory care in their institution were patient exclusion due to social criteria (42.5%, n = 97), lesions complexity (27.6%, n = 63), medico-legal risks (14.5%, n = 33), and lack of medico-economic incentive (3.9%, n = 9). Fifteen of them (6.7%) did not see an obstacle. The main reasons for conversion into inpatient hospitalization declared by those practitioners were procedural complications (32%, n = 73), postprocedural complications (28.5%, n = 65), social exclusion criteria (26.8%, n = 61), and organizational issues (3.5%, n = 8).
When asking all respondents what do they lack for developing outpatient surgery in their routine practice, the main highlighted elements were medico-legal guarantees (41.7% of those already practicing outpatient management, 66.7% of those who do not, p = 0.0008), lack of staff (25.4% of those already practicing outpatient management, 33.3% of those who do not, p = 0.23), lack of time (23.7% of those already practicing outpatient management, 29.4% of those who do not, p = 0.37), suitable patients (16.2% of those already practicing outpatient management, 15.7% of those who do not, p = 0.94), lack of experience (12.7% of those already practicing outpatient management, 15.7% of those who do not, p = 0.55), facilities (14.5% of those already practicing outpatient management, 9.8% of those who do not, p = 0.39), connected devices (9.2% of those already practicing outpatient management, 9.8% of those who do not, p = 0.79), desire (0.9% of those already practicing outpatient management, 7.8% of those who do not, p = 0.01), nothing (12.7% of those already practicing outpatient management, 1.9% of those who do not, p = 0.03) (Figure 3B).
On average, physicians already practicing outpatient management estimate that 58.3 ± 22.5% of their patients could be eligible for outpatient surgery in an ideal situation. This rate drops down to 38.8 ± 18.5% on average for physicians who do not practice outpatient surgery (p = 0.0003).
One-third of physicians already practicing outpatient surgery (n = 76, 33.3%) had observed an increase in outpatient care in their practice since the COVID-19 pandemic.
Discussion
This study is the first one describing real-world national practice of lower-limb PAD endovascular procedures performed in an outpatient setting. To our knowledge, no other survey-based study assessed the point of view of vascular interventionalists on their daily practice regarding outpatient surgery. Four years after the publication of the French guidelines for the management of ambulatory endovascular procedures for lower-extremity arterial disease, we observed wide discrepancies in the adoption of the outpatient setting in France.8,9 This study highlights social isolation, medico-legal risks, and the complexity of lesions as major obstacles to the development of outpatient endovascular treatment for lower-limb PAD.
This France-centered study is also of great interest to better understand the remaining improvement levers to the development of outpatient surgery in lower-limb PAD worldwide. Though endovascular revascularizations have moved considerably from inpatient to outpatient settings over the last 20 years in the United States,10,11 which is recognized as a pioneering country regarding outpatient care, most patients presenting with CLTI, for instance, continue to be treated as inpatients, and the 60% rate of outpatient surgery seems difficult to expand for various reasons. 12 Our study points out the remaining real-world obstacles that need to be tackled to improve the development of outpatient management. Notably, we highlight the reasons why targeted populations, who could potentially benefit from outpatient surgery, in the sense of what is demonstrated in the literature, still are excluded from outpatient management by most vascular interventionalists worldwide.
The French guidelines clearly state that age, CKD, CLTI, or the complexity of lesions should not be considered as contraindications for outpatient management, yet real-world practice data show that French vascular interventionalists still may be reluctant to include those patients. Among explanations stated by those practitioners, lack of time, staff, and remote follow-up means, such as connected devices, seem to play a major role.
Our study suggests that, even though eligibility criteria tend to broaden with vascular interventionalists’ experience of outpatient surgery, lesion complexity remains an obstacle for almost 28% of those who already perform lower-limb PAD revascularization on an outpatient basis. Almost 33% of them declared not proposing ambulatory management to patients with femoropopliteal thrombosis greater than 15 cm or below-the-knee thrombosis, for instance, for whom the endovascular approach is the first-line treatment and which accounts for a large number of patients in the lower-limb PAD population with a surgical indication. This might change over the coming years with the release of the most recent European guidelines, which broaden the spectrum of endovascular therapies among femoropopliteal lesions. 3
Lack of time and experience, expressed by 23.7% and 12.7% of interventionalists who practice outpatient surgery, respectively, could partially explain these remaining exclusion criteria. Time is surely a crucial point to consider on a daily schedule as a 4-hour postoperative surveillance is recommended, and confirmed in real-life data, giving preference to morning operating-room slots. Clinical trials including complex lesions such as chronic total occlusions (CTO) will be necessary to assess the feasibility and safety of those kinds of revascularization in an outpatient setting.
CLTI also stands out as a major obstacle, although multiple studies including these patients showed satisfying results in terms of safety and efficacy. Almazedi et al. presented a cohort of 301 patients, 43% of whom were patients with CLTI, treated for ambulatory PAD angioplasties with a 92% success rate, 4% minor complications and 1% major complications, with no differences for patients with CLTI. 13 Similarly, Spiliopoulos et al. presented a cohort of 652 day-case treatments for PAD, 24.6% of whom were patients with CLTI. They related a 97.1% technical success rate with no major complications noted after same-day discharge and no major amputations at the 30-day follow up in the CLTI group. 14 Zayed et al. described a cohort of diabetic patients with CLTI (n = 66) concluding that percutaneous transluminal angioplasty is feasible and safe as a day-case procedure in this population. 15 Nonetheless, it is undeniable that special attention must be paid to these patients who are prone to greater comorbidities, more complex lesions, and social isolation, requiring more operating time and closer follow up.
From a technical point of view, 179 (78.5%) vascular interventionalists declared that outpatient management did not impact their overall technical procedural approaches. Interestingly, even though more than 80% of them use closure devices, exclusive manual compression was not considered as a contraindication for 75.3% of the respondents. This was similarly assessed in the literature. The FREEDOM-OP trial, for instance, confirmed the feasibility and safety of manual compression for same-day discharge after lower-limb revascularization using a 5-F femoral sheath approach, with a 97% technical success rate, major access-related complications of 4.5%, and a total in-hospital admission rate of 11%. 16 Similarly, an outpatient setting did not impact the choice of sheath catheter sizes, which corroborates with the results of the Bio4amb trial where similar outcomes were found using 4- or 6-F sheaths. 17
Where the guidelines and real-word French, as well as international, data seem to converge, is the importance of social exclusion criteria. Among an aging patient population, often prone to social precariousness and isolation, the outpatient setting can be considered an additional challenge. Though a few studies showed the safety of performing outpatient angioplasty in a remote population, French guidelines maintained the need to be accompanied to benefit from outpatient surgery.8,18 Nonetheless, even by excluding these isolated and precarious patients, our study shows that there is definite room for improvement in the number of outpatient lower-limb PAD procedures, as vascular interventionalists claimed that up to 58.3 ± 22.5% of their patients could benefit from ambulatory surgery in an ideal world, versus 34% on average today. Remote postoperative follow up could be a key component of outpatient development. Innovative features, such as connected devices or mobile applications, could be an improvement factor for both vascular interventionalists and patients. However, these technologies will also take time to spread out, as these devices will need to be evaluated medically and economically. Some have already been approved and could be implemented on a larger scale.19–21 An on-going trial in our group (ABALONE), a stepped-wedge cluster randomized controlled trial, is aiming to increase the use of the outpatient setting for endovascular treatment of lower-limb PAD by proposing a care pathway adapted to people without an accompanying person at home on the night of the procedure. This study aimed to evaluate such devices and their potential role after outpatient lower-limb PAD endovascular procedures (ClinicalTrials.gov Identifier: NCT05756491). 22
Our study also highlights some elements that are specific to the French medico-economic situation. First, financial incentives were pointed out as a potential leverage effect. It is recognized that reimbursement changes (diagnosis-related group [DRG]-based hospital payment) favoring outpatient procedures was a turning point in the widespread adoption of outpatient surgery in the United States, for instance, more than a decade ago. 12 Until 2019 in France, the health insurance reimbursement to hospitals for lower-limb PAD endovascular interventions were in favor of an inpatient setting, which may have slowed down the development of outpatient interventions. In 2019, reimbursement became the same whatever the intervention setting for a hospital stay no longer than 1 day. 23 The true impact of this financial measure on the rate of outpatient endovascular interventions is, however, complex to assess. Indeed, we observed a spatio-temporal evolution toward more outpatient interventions in France from 2015 to 2022, with a rather steady increasing trend. 9 Since 2015, the proportion of establishments offering endovascular treatments on an outpatient basis and with an activity of at least 10 patients per year has more than tripled (10% vs 34.5%, respectively, in 2015 and 2022). 24 This trend was not homogeneously reproduced in Europe as DRG-based hospital payments in Germany, for instance, do not incentivize outpatient surgery. Other financial and industrial incentives are also taking place, such as the widespread use of atherectomy devices in the United States for which the reimbursement is linked to outpatient management.
As highlighted by this study, many factors come into play, such as patient preferences and interventionalists’ willingness, but also manpower in the establishments to open and organize the outpatient ward. In addition, this change occurred concurrently with the COVID-19 pandemic, which will have modified the management of care in many establishments, including outpatient surgeries.25–27
Second, France is specific regarding the fact that all endovascular procedures performed in an outpatient setting are taking place among hospital care. In addition to the shift to outpatient procedures in the United States, there have been significant changes within the outpatient category.10–12 Thus, outpatient surgeries can be performed in the hospital outpatient department (HOPD), office-based labs (OBLs), or ambulatory surgery centers (ASCs). Recently, OBLs have vastly increased their share of outpatient endovascular procedures versus the HOPD. This could partially explain the lower prevalence of outpatient surgery in that indication in France, where our study showed that only 17.6% of the respondents could benefit from a dedicated operating room and 43% of the respondents reported performing outpatient procedures only on morning operating-room shifts. These facilities might ease the choice of outpatient setting when a dedicated and more convenient institution and operating room are available.
Legal concerns also appear as a leading obstacle for French vascular interventionalists. Our study may be biased by the fact that more than 70% of respondents worked in private practice and therefore may be more exposed to medico-legal risk. Beyond medical guidelines, incentives regarding legal protection could be a path to explore. Discussion with primary care payers and private insurance could be initiated to that aim, as outpatient surgery appears to be a safe answer to reduce costs and hospital stays for endovascular procedures. Surely this point can be easily solved in view of the vast majority of leading centers dedicated to outpatient surgery in the United States for instance are private.
Finally, it is worth pointing out that given the majority of respondents are French vascular surgeons, meaning they practice both open and endovascular surgery, we did not assess the population of endovascular-only specialists. These specific populations of practitioners, more broadly spread internationally, may have different habits and inclusion criteria regarding outpatient management.
Our study may be biased by the wide representation of vascular interventionalists who already perform ambulatory care, especially when it comes to statistical comparisons of the two groups. However, this could also be considered an upside, as it enhances the external applicability of our study to countries with a higher adhesion to outpatient surgery. We can also point out that the wider feedback of those practitioners may lead to more thoughtful ideas on improvement.
What we learned from practitioners who are not performing outpatient surgery for arterial disease is that very few are reluctant to integrate outpatient management in their practice. Indeed, only four (7%) expressed a lack of desire to modify their practice whereas all others did identify overcoming obstacles. Thus, this study shows that the principle of an outpatient setting seems widely accepted. Any remaining obstacles are therefore based on difficulties other than just psychological concerns.
The results of the present study could feed discussions with vascular societies, governments, and industrialists on the different actions they could promote to foster the wider transition to outpatient settings worldwide. If stronger medico-legal protection, specific financial incentives, or the development of more convenient and dedicated structures seem to be the levers more specifically suitable for the French situation, then dedicated training on outpatient management, the development of connected devices, and stronger clinical data to assess the feasibility and security of treating complex lesions in an outpatient setting are definitely newly identified gaps that could be explored and applied internationally.
Conclusion
This study, carried out on a large sample of vascular interventionalists, is the first to take stock of outpatient surgery practice and its potential obstacles, 5 years after the publication of the French guidelines. Social isolation, medico-legal risks, and the complexity of lesions appear to be major obstacles to the development of outpatient endovascular treatment for lower-limb PAD that can be broadly applicable worldwide.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X251379455 – Supplemental material for Remaining gaps and obstacles in the outpatient setting for peripheral artery disease endovascular revascularization: Lessons learned from the French experience
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X251379455 for Remaining gaps and obstacles in the outpatient setting for peripheral artery disease endovascular revascularization: Lessons learned from the French experience by Alexandra Hauguel, Tatiana Bayan, Lucie Kraepiel, Nolwenn Le Meur, Laure Azéma and Yann Gouëffic in Vascular Medicine
Footnotes
Appendix
•
—
—
—
—
—
—
—
—
•
—
—
—
—
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
BIOTRONIK France provided financial and statistical support for this research. The funder participated in the statistical analysis.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.