
Abstract
Background:
Sclerotherapy is the treatment of choice for telangiectasias and reticular veins of the lower limbs, but long-term follow-up raises concerns about recurrence. This study aimed to evaluate the long-term outcomes of sclerotherapy for lower-limb telangiectasias and reticular veins over 3 years, focusing on disease control, pigmentation, and matting.
Methods:
A prospective, blinded cohort study followed patients treated with a single sclerotherapy session for telangiectasias (Study 1) or reticular veins (Study 2). Two groups were compae2-1358red: Group 1 received 0.2% polidocanol in 70% hypertonic glucose (PDHG) and Group 2 received 75% hypertonic glucose (HG) alone. Data were collected at 60 days and 3 years posttreatment. Analyses included recurrence, pigmentation, and matting. Photographic measurements were performed using ImageJ™ software.
Results:
A total of 43 patients were included in Study 1 and 35 in Study 2, with a mean follow-up of 36 months in both. The groups were epidemiologically similar. Recurrence occurred in both studies. In Study 1, almost all the patients had recurrence of telangiectasias, with no significant difference between treatments. In Study 2, recurrence was minimal and favored PDHG (p = 0.016). Pigmentation resolved mainly over time, with no significant intergroup or interstudy differences. Matting was more persistent in telangiectasias but nearly disappeared in reticular veins, with no significant group differences.
Conclusions:
Telangiectasia recurrence was common after 3 years, regardless of treatment. In contrast, reticular veins showed minimal recurrence, particularly with PDHG. Pigmentation generally resolved spontaneously. Matting was more persistent in telangiectasias than in reticular veins. These findings support the long-term viability of both approaches in clinical practice.
Keywords
Background
Sclerotherapy is a technique that uses the injection of a liquid or foam chemical agent to induce local endothelial irritation of the targeted varicose vein, reticular vein, or telangiectasia.1–3 Among the various techniques for the treatment of telangiectasias and reticular veins, chemical ablation of target veins using a sclerosant is the most commonly used, due to its simplicity, allowing a quick return to daily activities, and easy reproducibility.4,5 Sclerosants can be broadly classified, according to mechanism of action, into categories such as hypertonic (glucose and saline), detergents (polidocanol), and irritating substances (chrome glycerin). 4
Although sclerotherapy is generally viewed as a safe procedure, the professionals who perform it are concerned about potential complications.6,7 These can vary from minor issues, such as pigmentation spots (brownish lines or dots over treated veins) and matting (a network of small vessels forming in response to inflammation), to rare but serious complications like deep vein thrombosis, pulmonary embolism, and anaphylaxis.4,7–9
In studies carried out by our team, it was found that the association of 0.2% polidocanol diluted in 70% hypertonic glucose (PDHG) for the treatment of reticular veins and telangiectasias was more effective and safer in the short term (up to 60 days) when compared with 75% hypertonic glucose (HG).10,11 This was motivated by the discovery that the most common sclerosing agents used in Brazil were 75% HG alone and 0.2% polidocanol diluted in 70% HG, both of which are approved for use by the Brazilian National Health Surveillance Agency (ANVISA). 12
Owing to the heterogeneity and biases of studies comparing sclerosants, there is no definitive evidence supporting the superiority of any sclerosing agent in terms of efficacy. 4 Few studies have addressed the effectiveness of long-term treatment with sclerotherapy. Thus, the present study aims to objectively evaluate and quantify the long-term outcomes of patients treated with sclerotherapy. It also analyzes the effectiveness of treatment and the complications associated with the sclerotherapy of reticular veins and telangiectasias of the lower limbs.
Methods
Study design and patients
The study was conducted in accordance with the Declaration of Helsinki and international ethical standards and was approved by the local research ethics committee. Ethical approval for extended follow-up beyond this period was provided by the Human Research Ethics Committee of the Botucatu Medical School, under registration number CAAE: 63132816.6.0000.5411. Informed consent was obtained from all patients before their inclusion in the study, and they were allowed to withdraw at any time. In addition, consent for the publication of recognizable patient photographs or other identifiable material was obtained from all patients. The manuscript was prepared in accordance with the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement.
This is a cohort study that reevaluates results 3 years after sclerotherapy treatment, reassessing patients from two previous studies conducted at a single university center at the Clinical Hospital of the School of Medicine, Botucatu, São Paulo, Brazil. This reevaluation took place between 2017 (Study 1: telangiectasias) 10 and 2018 (Study 2: reticular veins). 11 Both studies used the same sclerosing solutions in randomized, parallel designs: 0.2% liquid polidocanol diluted in 70% glucose (2 mg/mL polidocanol + 700 mg/mL glucose = PDHG group) versus 75% hypertonic glucose alone (750 mg/mL glucose = HG group). The sclerosing agents were obtained at that time from the Health Tech Laboratory, São Paulo, Brazil. All patients were invited to a long-term reassessment of the treatment. The primary studies were randomized clinical trials (see the Supplemental Material for more information about previous studies).
Patient baseline characteristics were reevaluated, including age, body mass index (BMI), physical activity, smoking status, systemic arterial hypertension, dyslipidemia, hyperthyroidism, family and personal history of varicose veins, Fitzpatrick skin phototype, 13 and pregnancy history.
Inclusion and exclusion criteria
All patients who completed both primary studies (D60) were invited by phone, 3 years after treatment, to reassess treatment status (recurrence of vessels) and late complications (pigmentation and matting). Up to three attempts were made to contact the patients by phone. If there was no response, the electronic medical record was searched, and another attempt at contact was made.
Patients were excluded if they declined reassessment, were not found after following up all available forms of contact, or who had sclerotherapy performed on the target areas after the study session.
Photographic data acquisition and procedures
All participants underwent a duplex ultrasound examination before inclusion. Patients who presented with reflux in the great or small saphenous veins, accessory saphenous veins, or perforator veins were excluded from the study (only patients classified as CEAP [Clinical, Etiologic, Anatomic, Pathophysiologic] C1 were included).
The patients who participated in the first study had the target area of the lower limb photographed at the same spot where the sclerotherapy treatment was performed. The same high-definition digital camera (Nikon AF-S D7000 18–105 mm lens – Nikon Corporation, Tokyo, Japan) was used, adjusted by simultaneous comparison with previous photographs on a computer. Specifically, the parameters of the earlier studies were used as follows (the baseline study methods are described with more detail in the Supplementary Material):
The images were analyzed using the segmented line tool in ImageJ™ software (National Institutes of Health) by two expert evaluators who did not participate in the treatment session, following a previously validated methodology. 14 The intra-class correlation coefficient (ICC) for the evaluators was ICC = 0.99 (0.997–1) for telangiectasias and ICC = 0.99 (0.996–0.999) for reticular veins. This was considered excellent, and the final value was calculated as the average of the two evaluators’ measurements. The lengths of telangiectasias and reticular veins were objectively quantified, in addition to residual hyperchromic spots. The presence of matting was evaluated as present or absent.
Comparisons were made through analysis of photographs obtained at short-term (D60) and long-term (3 years) follow-up in the present study.
Furthermore, to assess disease control and maintenance of previous results and adverse events (pigmentation and matting), patients were compared within the treatment groups to which they were assigned in the original studies: Group 1 (G1) = PDHG and Group 2 (G2) = HG.
Outcomes
The results were evaluated separately for patients who participated in Study 1 (telangiectasias) and in Study 2 (reticular veins). However, the same methodological criteria were used to evaluate the outcomes: the late recurrence outcome was calculated by subtracting the absolute final value from the initial one, in centimeters (3 years – D60), and results were compared by treatment group; intragroup late relapse over time was assessed by comparing initial (D60) and final (3 years) values; pigmentation regression between groups was determined by subtracting the initial absolute value, in centimeters, from the final value (D60 – 3 years); for intragroup pigmentation regression, initial (D60) and final (3 years) values were compared; to evaluate matting, the strategy involved comparing the number of affected patients at D60 and 3 years across both treatment groups and within groups over time; other risk factors related to recurrence were also compared, regardless of the treatment type.
Statistical analysis
For statistical analysis of the data generated in this study, SPSS version 22.0 (IBM Corp.) was used. All data were tested for normality using the Shapiro–Wilk test. Parametric data were analyzed using Student’s t-test (paired and unpaired) and the chi-squared test for categorical comparisons. Nonparametric data were analyzed using the Mann–Whitney test for unpaired data, the Wilcoxon test for paired data, and McNemar’s test or Fisher’s exact test for categorical variables, as necessary. The significance level adopted for all situations is 5% (p < 0.05) with 80% statistical power.
Results
Study 1 (telangiectasias)
Ninety-eight patients were initially evaluated in Study 1; of these, 62 (63.3%) returned for long-term follow-up (3 years): 29 in G1 (PDHG) and 33 in G2 (HG). Some patients were excluded because they had received additional sclerotherapy in the same area during that time. Importantly, no patient was excluded due to early recurrence or early retreatment. These patients were excluded only because they underwent more than one sclerotherapy session, which made it impossible to evaluate recurrence based solely on a single-session protocol, as required by the study design. Therefore, 20/51 patients (39.2%) in G1 (PDHG) and 23/47 patients (48.9%) in G2 (HG) were ultimately evaluated; the results are shown in Figure 1.
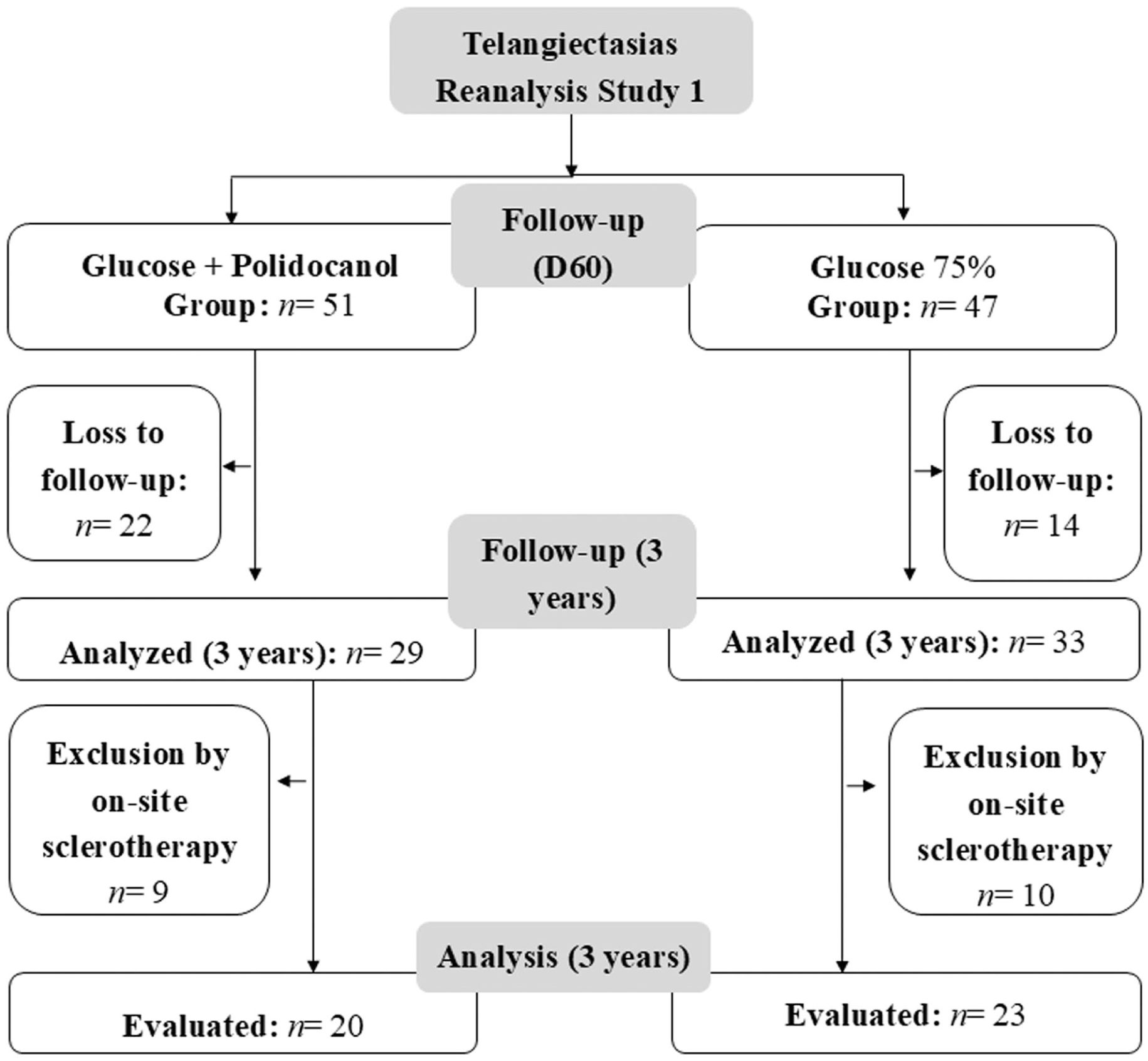
Study 1 flow chart (telangiectasias). D60, 60 days posttreatment.
Table 1 presents the epidemiological data for patients in Study 1 (telangiectasias) at the 3-year follow-up. The groups were largely homogeneous, except for mean age, which showed a statistically significant difference; however, the average age remained below 50 years in both groups. Notably, the sample showed low comorbidity prevalence, a high prevalence of family history of varicose veins, and a high proportion of patients with skin phototypes I–III in both groups.
Baseline characteristics of patients in Study 1 (telangiectasias).
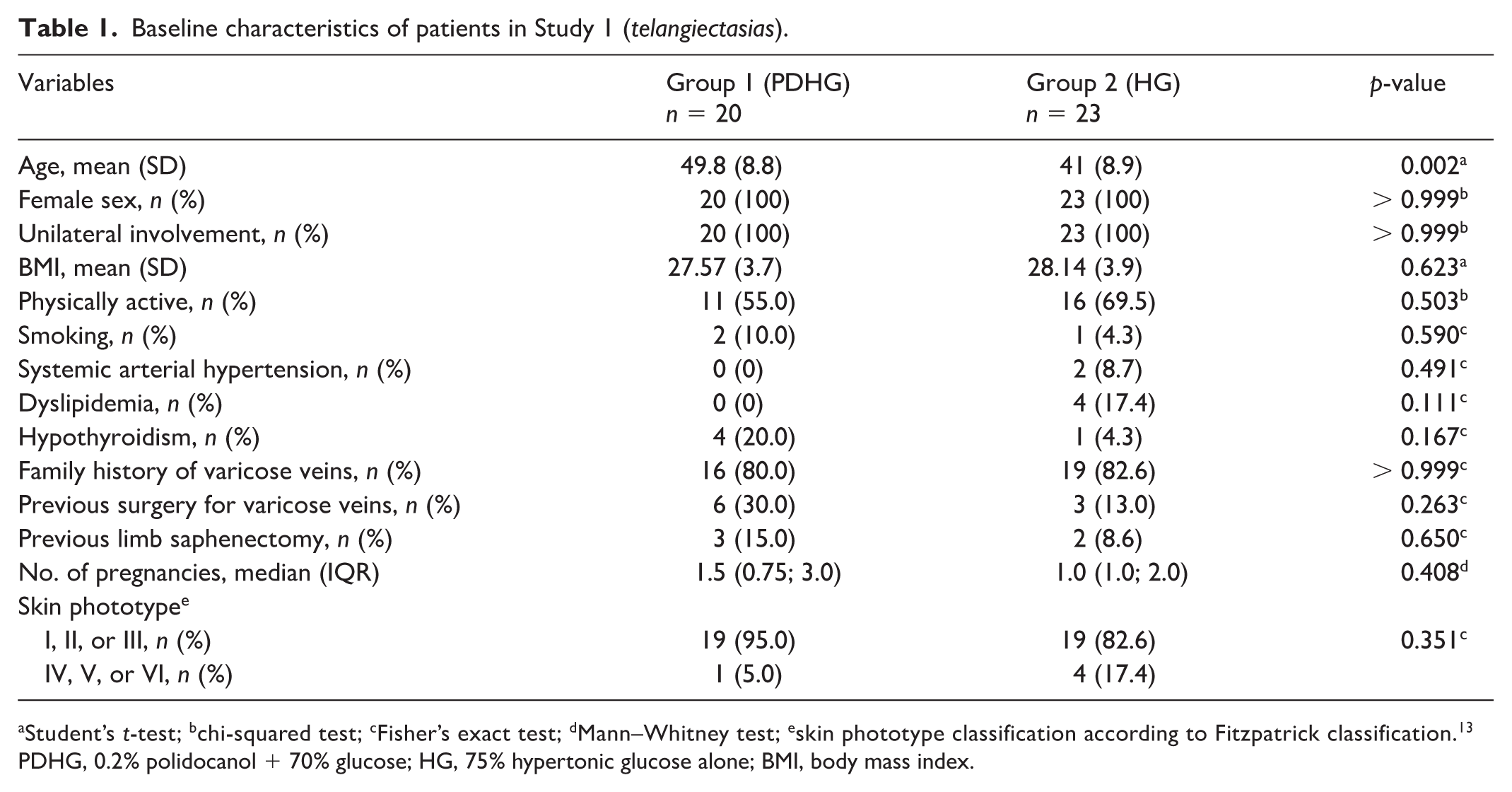
Student’s t-test; bchi-squared test; cFisher’s exact test; dMann–Whitney test; eskin phototype classification according to Fitzpatrick classification. 13
PDHG, 0.2% polidocanol + 70% glucose; HG, 75% hypertonic glucose alone; BMI, body mass index.
Table 2A shows the results for recurrence and complications, comparing the treatment groups. A significant recurrence of telangiectasias (measured in absolute length, cm) was observed in both groups, but there was no significant difference: G1 (PDHG) versus G2 (HG) (10.29 vs 7.91 cm; p = 0.733). Photographic analysis indicated that recurrence was sometimes associated with preexisting telangiectasias and sometimes not. Pigmentation generally decreased by 3 years, with no significant difference between groups. Regarding late matting, there was no difference in the number of affected patients between the groups.
Evolution of sclerotherapy for telangiectasias.
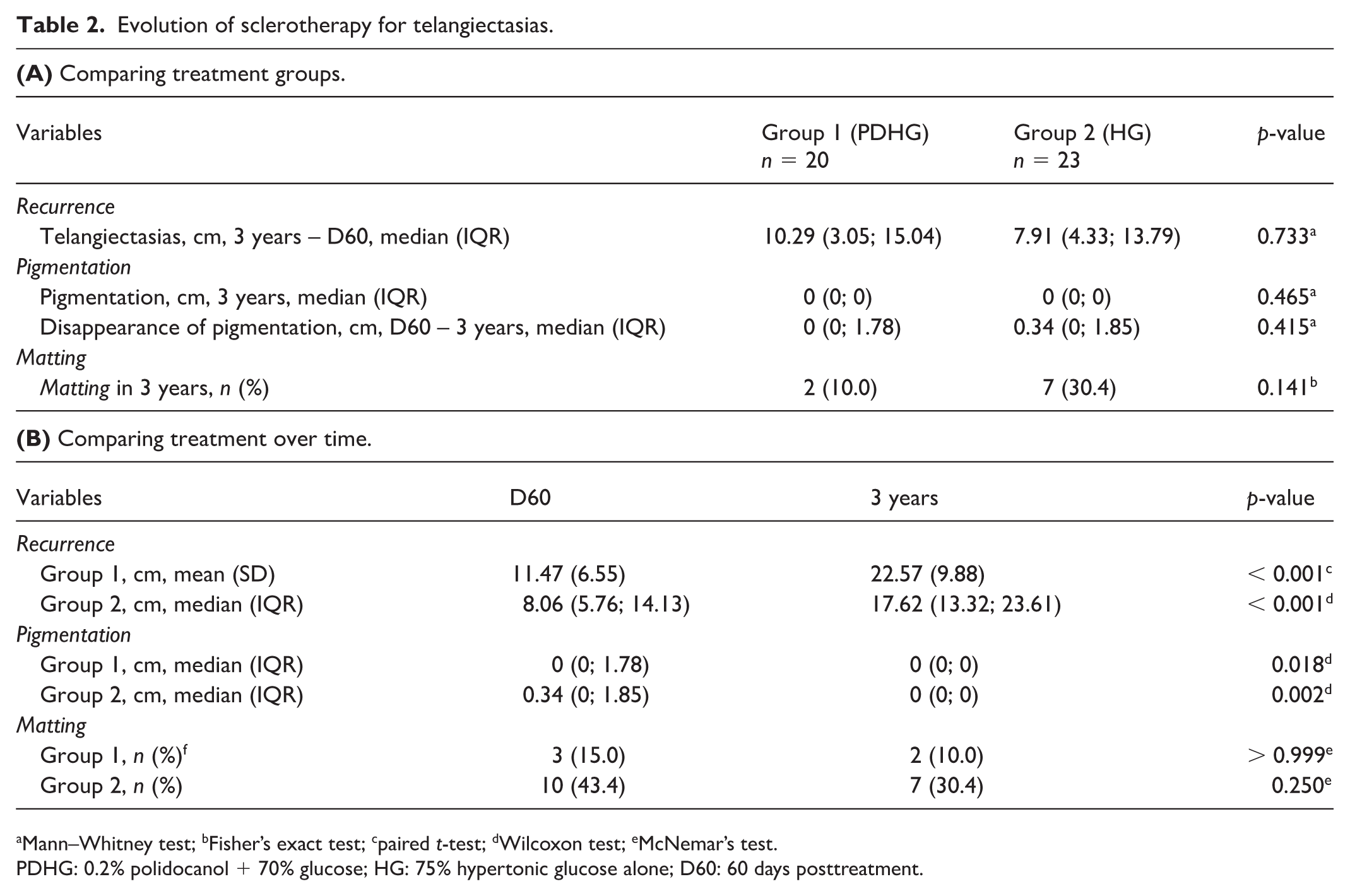
Mann–Whitney test; bFisher’s exact test; cpaired t-test; dWilcoxon test; eMcNemar’s test.
PDHG: 0.2% polidocanol + 70% glucose; HG: 75% hypertonic glucose alone; D60: 60 days posttreatment.
Table 2B presents the intragroup temporal comparison of recurrence, pigmentation, and matting. Recurrence of telangiectasias increased over time in both groups, with absolute lengths (cm) nearly doubling from D60 to 3 years. In contrast, pigmentation spots almost completely regressed in both groups over the same period. For matting, although there was an apparent reduction in intensity and frequency, the change was not statistically significant.
Figure 2 shows the evolution of telangiectasias in photographs of the treatment area over time (D0, D60, and 3 years), with clean images and highlighted vessels (ImageJ software).
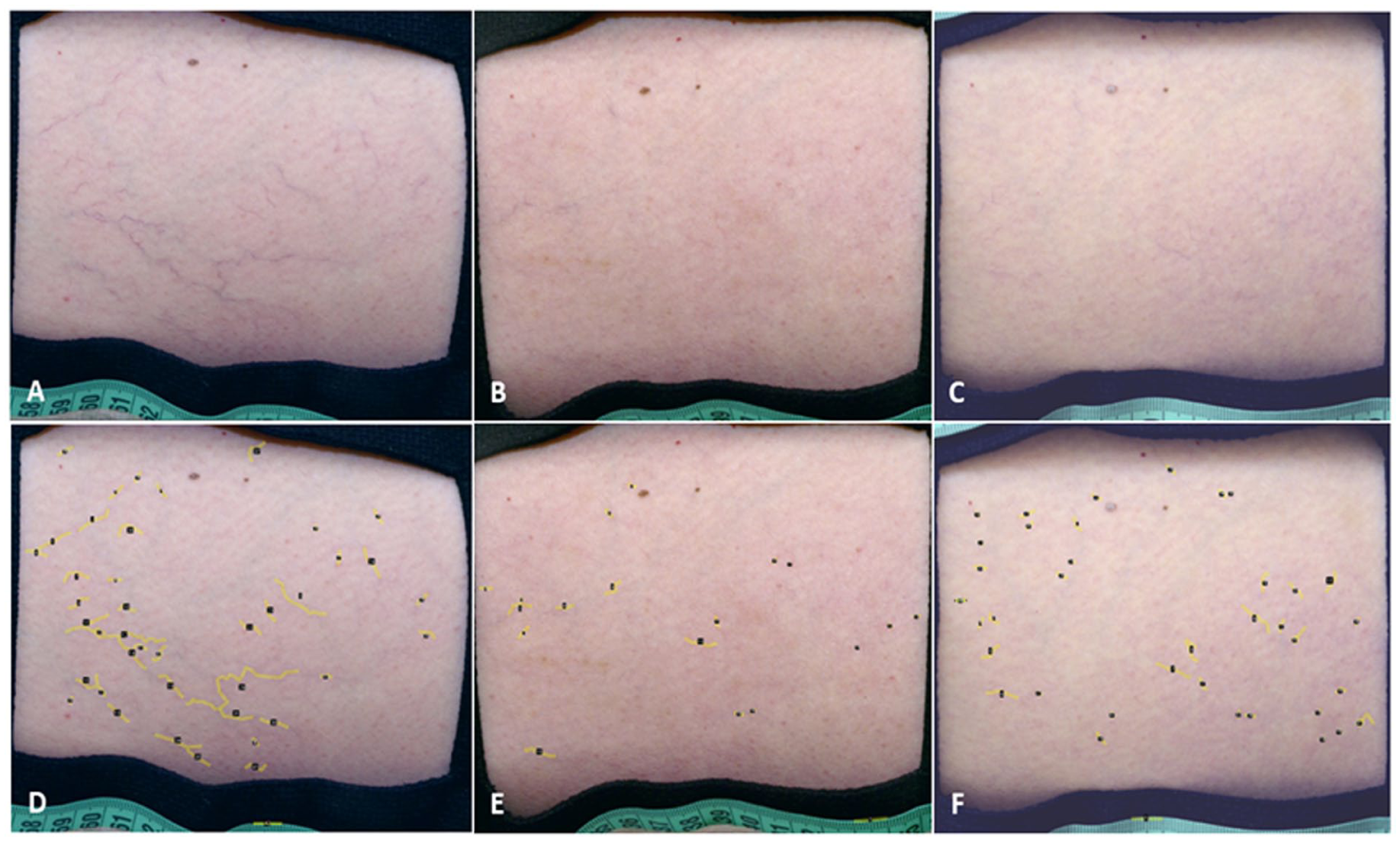
Photographs of the side of the leg of a participant in Study 1 (telangiectasias), without and with measurements in ImageJ software. (
Study 2 (reticular veins)
Ninety-three patients were evaluated in Study 2 (reticular veins); 53 patients (57%) returned for long-term evaluation (3 years): 28 in G1 (PDHG) and 25 in G2 (HG). Some patients were excluded because they had received additional sclerotherapy in the target area. As in Study 1, none of these exclusions were due to early recurrence or early retreatment. These patients elected to undergo additional sessions, making it impossible to assess recurrence after a single session, which was a requirement of the study design. Therefore, 20/43 patients (46.5%) in G1 (PDHG) and 15/50 patients (30%) in G2 (HG) were evaluated; the results are shown in Figure 3.
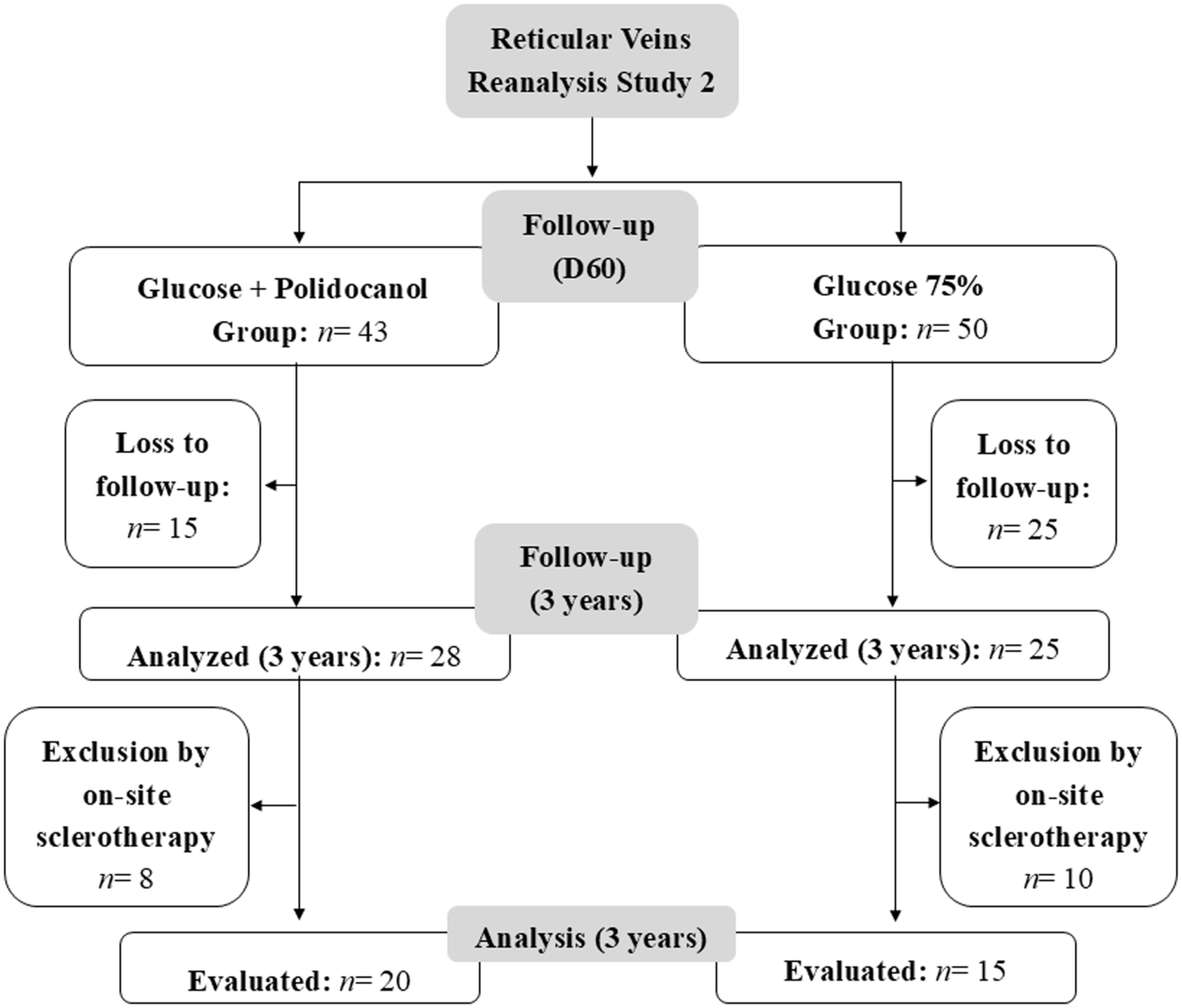
Study 2 flow chart (reticular veins). D60, 60 days posttreatment.
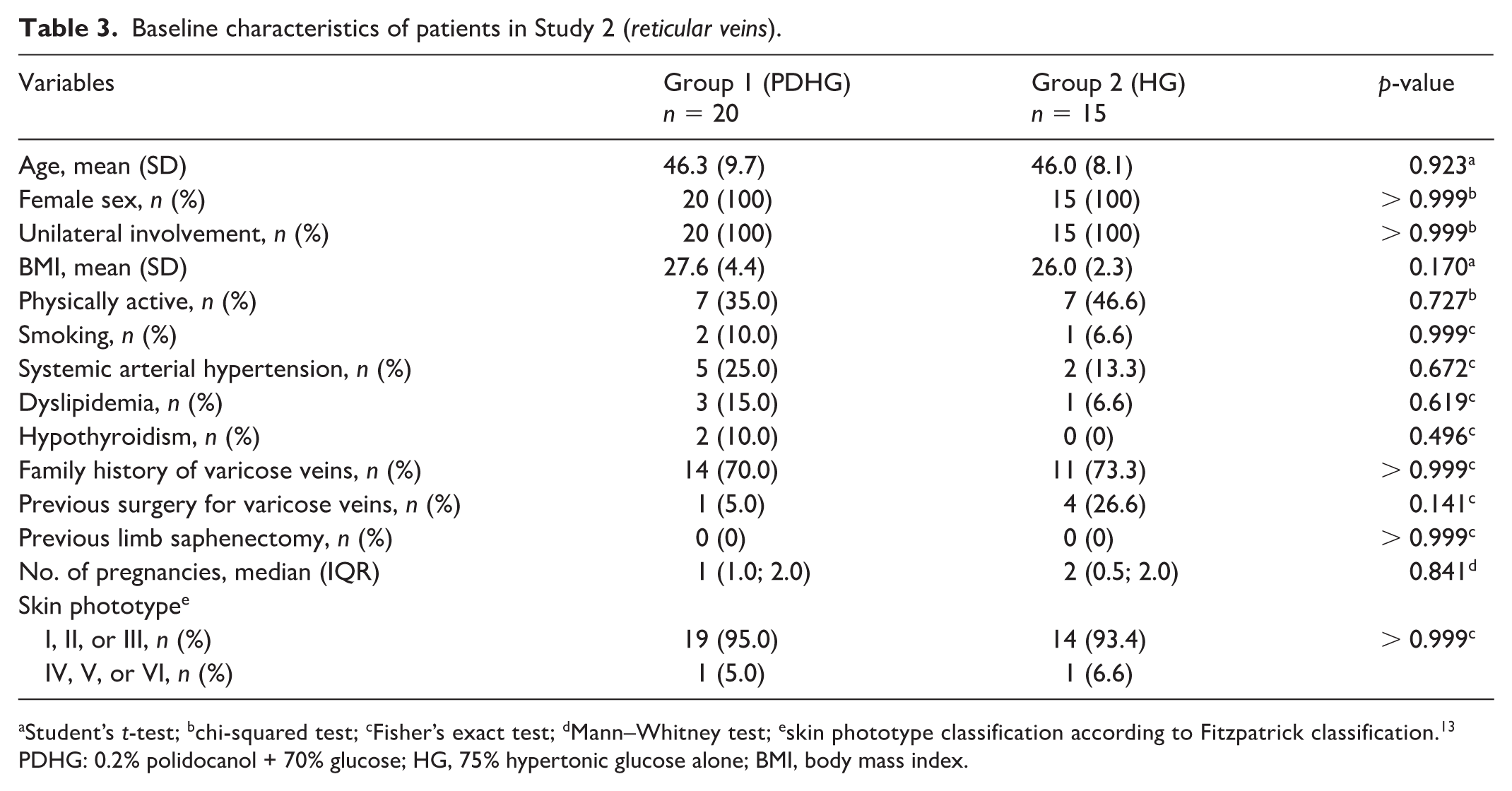
Table 3 presents the epidemiological data for Study 2 patients at the 3-year follow-up. Groups were homogeneous for all parameters evaluated. The mean age was below 50 years in both groups. As in Study 1, there was a low prevalence of comorbidities, a high prevalence of family history of varicose veins, and a predominance of skin phototypes I–III.
Baseline characteristics of patients in Study 2 (reticular veins).
Student’s t-test; bchi-squared test; cFisher’s exact test; dMann–Whitney test; eskin phototype classification according to Fitzpatrick classification. 13
PDHG: 0.2% polidocanol + 70% glucose; HG, 75% hypertonic glucose alone; BMI, body mass index.
Table 4A shows the intragroup temporal correlation of recurrence, pigmentation, and matting. Unlike telangiectasias, a significantly lower recurrence was observed for G1 (PDHG) compared with G2 (GH) (0.66 vs 6.62 cm; p = 0.016). Pigmentation tended to disappear by 3 years and was not affected by treatment. Finally, regarding late matting, no significant difference was observed between the groups.
Evolution of reticular veins.
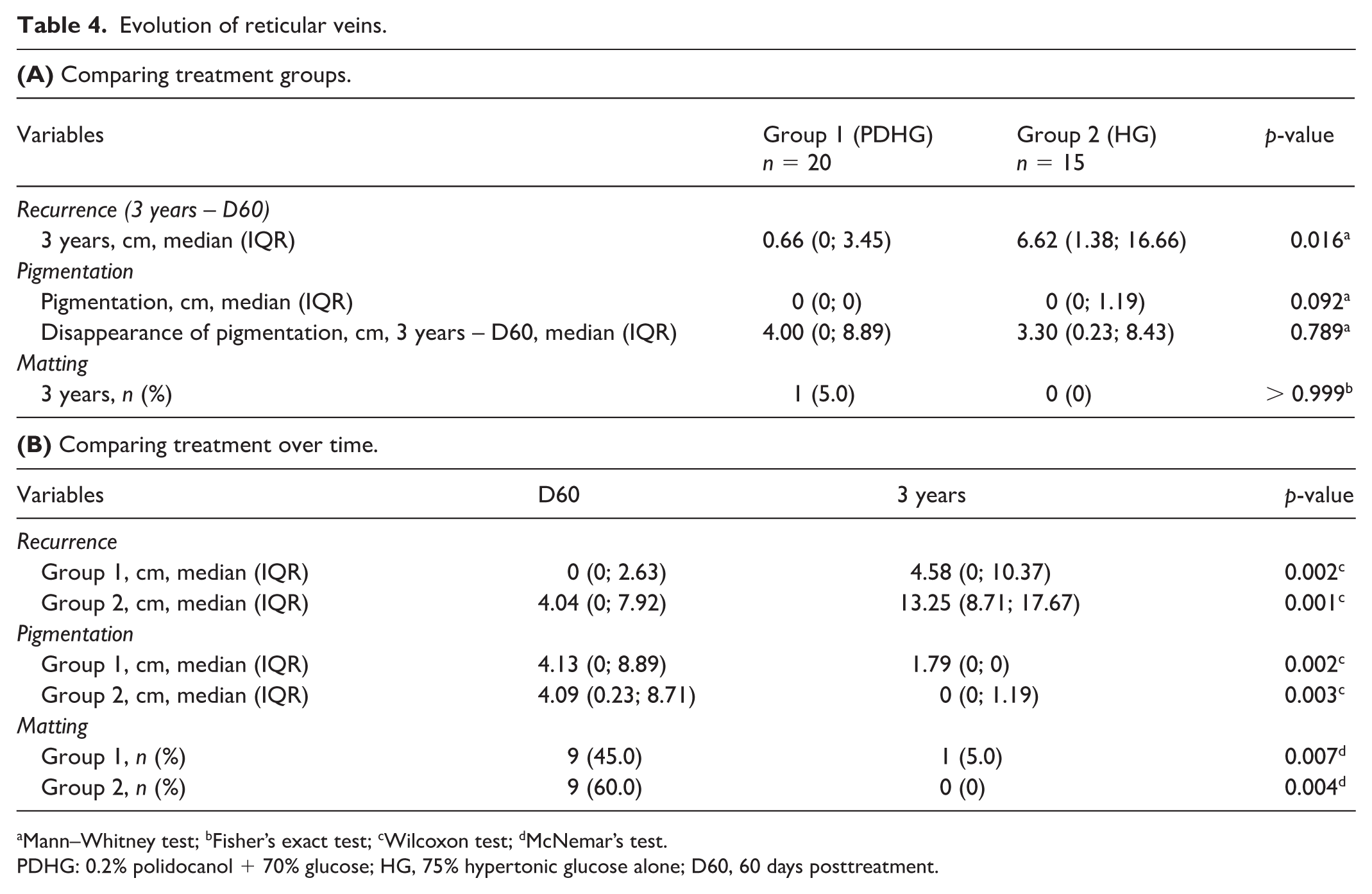
Mann–Whitney test; bFisher’s exact test; cWilcoxon test; dMcNemar’s test.
PDHG: 0.2% polidocanol + 70% glucose; HG, 75% hypertonic glucose alone; D60, 60 days posttreatment.
Table 4B presents the correlation of recurrence, pigmentation, and matting in the intragroup temporal comparison. Reticular vein recurrence was observed in both groups, with absolute lengths (cm) close to zero during the observation period (D60 – 3 years). Pigmentation spots, in absolute linear extension (length, cm), almost disappeared during the observation period (D60 – 3 years) in both groups. However, for matting, unlike in the treatment of telangiectasias, there was a significant reduction in the temporal comparison, tending toward zero by the end of the observation period.
Figure 4 illustrates the evolution of reticular veins in photographs of the treatment area over time (D0, D60, and 3 years), with clean images and highlighted vessels (ImageJ software).
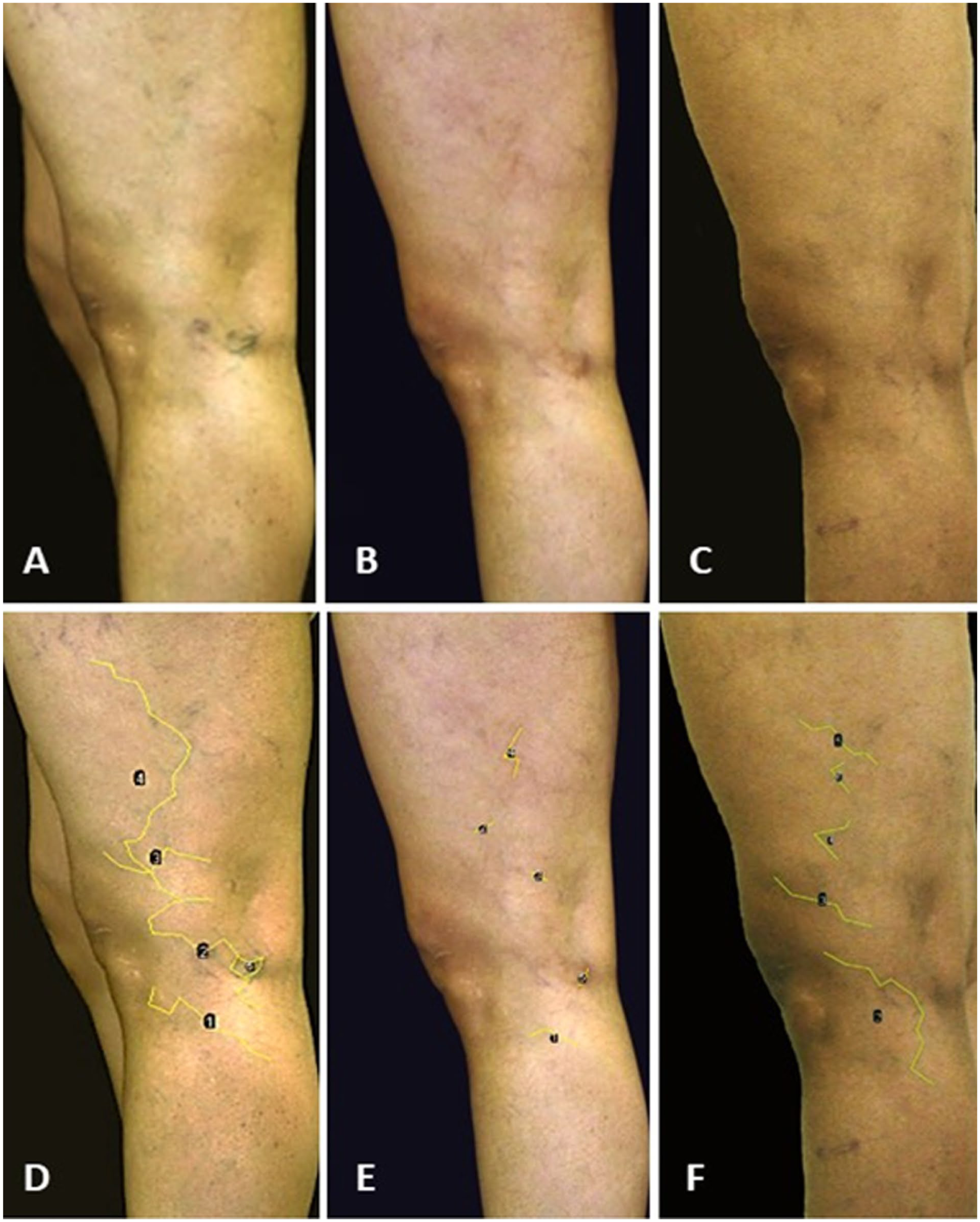
Photographs of the side of the thigh and leg of a participant in Study 2 (reticular veins), without and with measurements in ImageJ software. (
Discussion
Aesthetic concerns are the primary reason patients seek treatment for reticular veins and telangiectasias; however, symptoms such as pain, swelling, and leg heaviness may also improve with treatment. 13 Several studies have compared sclerosing agents; however, due to heterogeneity among study groups and potential biases, meta-analyses have not provided sufficient evidence to determine the most effective sclerosing agent. 4 Despite the simplicity of the technique, more effort should be made to reinforce evidence-based treatment and evolution over time. 15 The present study separately evaluates patients with predominant lesion type (telangiectasias and reticular veins), aiming to prospectively assess the recurrence and evolution of major complications approximately 3 years after a single treatment session, using the formulations most commonly employed in Brazilian clinics. It should be emphasized that no patient was excluded due to early recurrence or early retreatment. Patients were excluded only if they underwent additional aesthetic sclerotherapy sessions, which prevented recurrence from being evaluated based solely on the initial single treatment session, as defined in the study design.
In both studies, more than 50% of patients reported a family history of varicose veins. Skin phototypes I to III were predominant; however, due to the limited sample size, no definitive conclusions could be drawn regarding these parameters. 14 Nevertheless, some authors report that phototype influences pigmentation. 8 Comorbidities were uncommon, likely due to the relatively low age of the patients in the sample, which is supported by epidemiological data on the occurrence of mild chronic venous disease.8,16,17
It is known that reticular veins and telangiectasias can recur in the medium and long term, requiring repeated treatment sessions at defined intervals. 17 Lucchi et al. 18 followed up patients who underwent sclerotherapy with glycerin or polidocanol for the treatment of telangiectasias for 5 years and observed that the recurrence of telangiectasias can be more directly attributed to the evolution of the disease than to the recurrence itself.
Our study presents a reassessment of a single intervention after approximately 3 years, with objective analysis and group dissociation of telangiectasia and reticular vein treatment, comparing 0.2% polidocanol diluted in 70% HG versus 75% HG alone. In line with the study’s conditions, recurrence was observed in practically all patients with telangiectasias, without correlation to the treatment received for either condition. Recurrence may be related to disease progression, genetic predisposition to telangiectasias, matting areas serving as sources of neovascularization, inadequate treatment of downstream reticular veins, or incomplete treatment of the telangiectasias themselves. In any case, the data obtained reinforce established knowledge that the treatment of telangiectasias frequently requires more than one session, ongoing monitoring is necessary, and there is a genetic tendency associated with this clinical condition. 16
However, interestingly, the treatment results show that reticular vein treatment is more stable over time and has less recurrence, maintaining a favorable relationship with group 1, treated with 0.2% polidocanol plus 70% glucose, even in the long term. It is essential to clarify that this study was based on a particular regional characteristic of the medical treatment of telangiectasia and reticular veins, in which pure polidocanol liquid is not commonly used. 12
In the literature, pigmentation is reported in 10–30% of patients with vessels between 0.1 mm and 5 mm in diameter, but mainly after treatment of veins larger than 1 mm.8,9,18,19 It is often associated with a higher concentration of the sclerosing agent, excessive intravascular pressure, and rapid injection. It shows a positive relationship with sodium tetradecyl sulfate (STS) and polidocanol compared with hypertonic saline.9,18,20 However, in our previous studies, polidocanol in combination with HG resulted in less pigmentation than HG alone for the treatment of telangiectasias.9,10 Furthermore, it is described that pigmentation can be transient or permanent: transient being the lesions that resolve spontaneously within 1 year after the procedure, and permanent being the ones that persist after 1 year. 19 Spontaneous resolution occurs in 70% of cases within 6 months but can persist for more than 1 year in up to 10% of patients. 19 Goldman et al. 19 observed an 80% clearance rate of hyperchromic spots over 6–24 months, whereas some spots persisted for up to 5 years. Santiago et al. 20 performed sclerotherapy with HG in 42 patients with reticular veins and varicosities and observed, during a 2-month follow-up, mild pigmentation in 15 limbs (35%) and moderate pigmentation in one limb (2.3%). After 6 months, only the limb that presented with moderate pigmentation and one limb that presented with mild pigmentation (2.3%) still showed hyperchromic spots. Pigmentation spots appear gradually after the treatment session, peaking after 6–8 weeks. As observed in our previous studies (D60), spots were present in both groups, with a favorable trend in the group treated with PDHG for reticular veins and a statistically significant difference for telangiectasias. In the present study, pigmentation spots measured by absolute values for length (cm) were practically abolished after 3 years of follow-up in both studies, with no association with the treatment group, confirming the most recent optimistic data in the scientific literature. Reina et al. 21 also observed that time is the primary treatment for this uncomfortable complication. It should be noted that professional experience also influences pigmentation outcomes. Therefore, all outcomes, including the need for multiple treatment sessions, possible adverse events, and variable results, must be discussed and clarified with the patient before treatment to avoid insecurity and frustration.
Finally, the incidence of matting is estimated at 15–24% among patients undergoing sclerotherapy. It is thought to be related to an exaggerated response to drainage vessel obstruction, destruction of the endothelium, and inflammation, with hormonal factors considered a related agent. 7 These data were observed during the follow-up of the participants in our studies. Matting practically disappeared in all participants in Study 2 (reticular veins) and did not disappear at all in Study 1 (telangiectasias), despite becoming much less intense. This may be related to the intensity of telangiectasia treatment, which was concentrated in a single region during the initial study, potentially causing greater inflammation and persistence in these patients, consistent with previous literature. Thus, less concentrated sessions on specific points should lead to less inflammation and lower matting rates, highlighting the importance of adherence to the treatment and justifying greater attention during the session.
A key strength of this study is the use of a quantitative analytical method supported by free-to-use software, which enabled evaluators to compare individual veins in photographs. This method was recently validated by the study team and proved superior to the homogeneity of results achieved in most studies in the literature, which use a subjective rating scale assigned by independent evaluators as a form of analysis. With advances in computer technology, there is a need to improve techniques for evaluating sclerotherapy outcomes to protect patients and professionals, as we have done in our studies.8,16
As a limitation, the study had a small sample of patients, mainly because this was a very late assessment, and many cases had been submitted to new treatments in the area of interest or were satisfied with previously obtained results. Our study did not include intermediate assessments during this period, so it is not possible to trace progress between evaluations. Additionally, the patients mostly had mild venous disease, which may have reduced adherence to follow-up visits.
Conclusion
Sclerotherapy of reticular veins demonstrated long-lasting efficacy during the 3-year follow-up, whereas telangiectasias exhibited higher recurrence rates during the same period. Furthermore, the type of sclerosing agent influences the choice, favoring the 0.2% polidocanol combined with 70% hypertonic glucose group for reticular veins. The medication had no impact on the recurrence of telangiectasias. Most cases of postsclerotherapy pigmentation resolved spontaneously in both telangiectasias and reticular veins, with no influence of the sclerosing agent type during the observation period. Matting persisted after telangiectasia treatment but resolved spontaneously after reticular vein treatment.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X251412739 – Supplemental material for Long-term follow-up of sclerotherapy of telangiectasias and reticular veins in lower limbs: Glucose versus polidocanol diluted in glucose
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X251412739 for Long-term follow-up of sclerotherapy of telangiectasias and reticular veins in lower limbs: Glucose versus polidocanol diluted in glucose by Matheus Bertanha, Vinicius Tadeu Ramos da Silva Grillo, Caio Paiva Pellizzer, Lenize da Silva Rodrigues, Pedro Luciano Mellucci Filho, Pedro Luiz Toledo de Arruda Lourenção and Marcone Lima Sobreira in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was funded by São Paulo Research Foundation (FAPESP) protocol number 2016/15004-0.
Data availability statement
The raw data underlying this study will be made available upon reasonable request from the corresponding author.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.