
Abstract
Venous thromboembolism (VTE), which encompasses deep venous thrombosis (DVT) and pulmonary embolism (PE), is a common preventable complication in hospitalized patients. Risk assessment tools allow for easy stratification of patient VTE risk and have been demonstrated to reduce incidence of VTE. However, risk assessment tools remain underutilized in clinical practice. This scoping review aims to explore barriers and facilitators to VTE risk assessment usage to improve rates of hospital-acquired VTE and provide recommendations for future implementation strategies. Four databases (PubMed/MEDLINE, Embase, Cumulative Index to Nursing and Allied Health Literature, and Cochrane Database of Systematic Reviews) were searched from January 1990 through December 2025, and 59 studies were included after selection by three independent reviewers. Themes related to ‘decreased provider compliance’ and ‘difficulty of use’ were the most commonly cited barriers. For facilitators, the majority of themes surrounded ‘electronic medical record integration,’ ‘forcing functions,’ and ‘education.’ A prevalence of barriers and a paucity of facilitators contribute to decreased VTE risk assessment usage. Hospital administrators and clinicians should address current barriers and promote facilitators during VTE risk assessment initiatives to maximize patient quality improvement outcomes. (
Background
Hospital-acquired venous thromboembolism (HA-VTE) is a common preventable complication associated with significant mortality and long-term morbidity among hospitalized patients. According to the Centers for Disease Control and Prevention (CDC), VTE mortality is estimated at between 60,000 and 100,000 annually, and half of surviving patients will suffer from long-term complications such as postthrombotic syndrome or chronic thromboembolic pulmonary hypertension. 1 As a result, improving prevention of HA-VTE remains a key indicator of hospital quality of care.
Substantial evidence demonstrates that thromboprophylaxis reduces rates of HA-VTE in appropriately selected patient populations. As such, current guidelines for VTE prophylaxis recommend using pharmacological thromboprophylaxis (e.g., low-molecular weight heparin) and/or nonpharmacotherapy (e.g., sequential compression devices or ambulation) for moderate-risk and high-risk patients. 2 The prevention of HA-VTE has been a target for numerous quality initiatives, including the National Quality Forum, the Surgical Care Improvement Project, and the Surgeon General of the United States.3–5 However, VTE prophylaxis remains underutilized in both medical and surgical patients. 6
VTE risk assessment tools (e.g., Padua Prediction Score, IMPROVE risk scores, Geneva Risk Score, and the Caprini Score) all aim to create a simple method of estimating VTE risk in hospitalized patients. Although there is no universally accepted tool, all have been proven to promote the appropriate use of VTE prophylaxis in at-risk patients. However, provider compliance with risk assessment tools remains a challenge, with only one-third of physicians using a risk assessment model to guide treatment of those at risk for VTE.7–11
Proper implementation of VTE risk assessment tools ensures widespread usage by providers, identification of at-risk patients, and the prescription of prophylaxis. Although numerous institutions have adopted VTE risk assessment tools, implementation strategies vary. Recognizing there is no uniform approach to VTE risk assessment implementation, the objective of this scoping review is to understand the barriers and facilitators to implementing in-hospital VTE risk assessment using the Consolidated Framework for Implementation Research (CFIR).
Methods
Study overview
We conducted a scoping review using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) schema (Figure 1). The study protocol was registered with PROSPERO prior to initiating the review (PROSPERO Registration No.: CRD42022360033). We included articles from January 1990 through December 2025 with study populations that were: adults, humans, inpatients, and medical or surgical cohorts. Articles must have a specified VTE risk assessment model (e.g., Caprini, Padua, Autar, IMPROVE-RAM [International Medical Prevention Registry on Venous Thromboembolism Risk Assessment Model], Improve-DD, Rogers), address barriers or facilitators to VTE risk assessment implementation, and measure implementation outcomes. Examples of implementation outcomes include acceptability, adoption, appropriateness, feasibility, fidelity, cost, penetration, and sustainability. 12 Articles were excluded if they were conference proceedings, reviews, editorials, non-English speaking, or if the intervention was not clearly described.
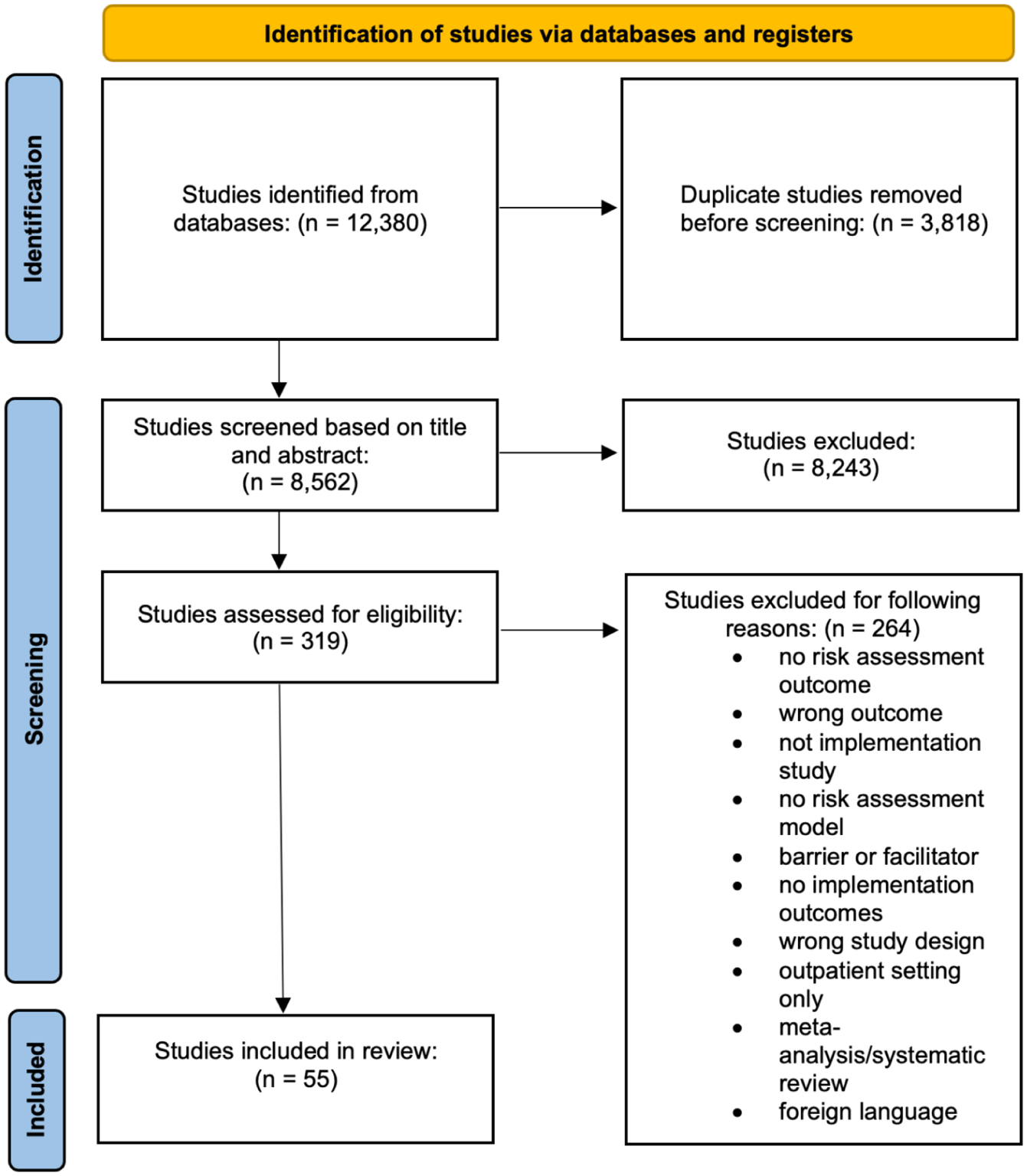
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart.
Conceptual framework
The CFIR is a widely used implementation framework that provides a structured approach to examining determinants of the implementation process and outcomes (Figure 2). It consists of five domains: Innovation (refers to the intervention being implemented), Inner Setting (refers to the implementation factors as they exist within an organization), Outer Setting (refers to the setting in which the inner setting exists), Individuals (refers to the roles and characteristics of the individuals involved with the intervention), and Implementation Process (refers to the strategies used to implement the innovation). The domains are further divided into 48 constructs and 19 subconstructs that provide additional clarification to each of the domains. We used the CFIR to map the implementation barriers and facilitators reported in the review studies.
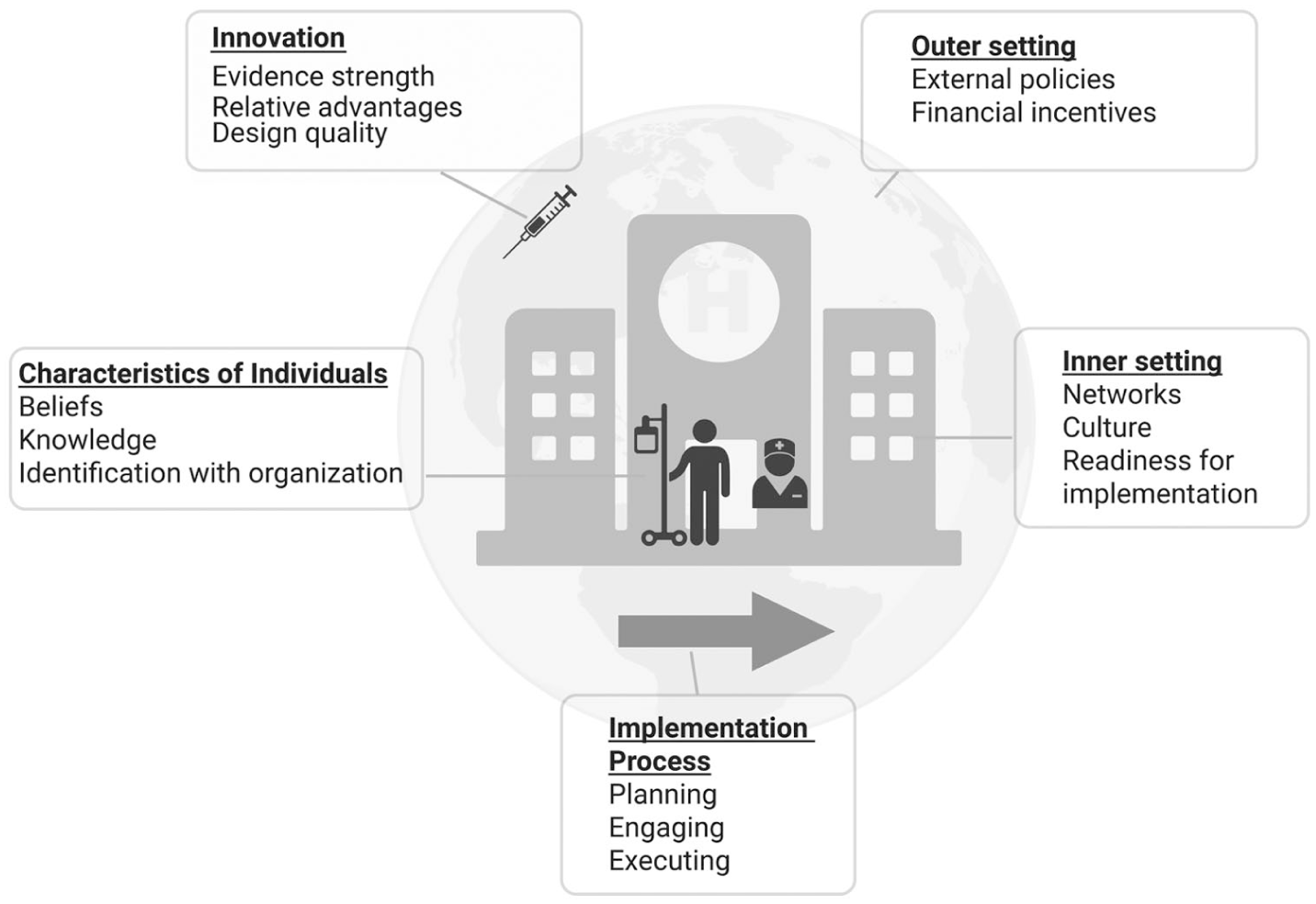
Consolidated Framework for Implementation Research (CFIR) construct.
Data sources and searches
We performed literature searches in the following databases: PubMed/MEDLINE, Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Cochrane Database of Systematic Reviews from January 1990 through December 18, 2025. Our search strategy was developed with the assistance of a research librarian. Search terms are provided in the Supplemental Appendix. Articles were imported into Rayyan (Rayyan Systems Inc.), a web-based application for systematic reviews, where duplicates were excluded.
Study selection
A two-stage screening process was conducted to select eligible studies. In the first stage of screening, one researcher screened titles for relevance to implementation of VTE risk assessment. In the second stage of screening, two researchers (CP and AO) independently reviewed full articles to ensure alignment with inclusion and exclusion criteria (Figure 1). Any disagreement occurring in the second stage of screening was resolved via consensus among three researchers (CP, AO, and SW)
Data extraction and analysis
Data extraction was completed by two researchers (DC and AS) using Rayyan. We extracted data including authors, publication year, country of study, study aim, study design, setting, population, description of intervention, information on barriers and facilitators, and implementation process details. Two authors (DC and AS) independently reviewed the included articles, and the quality of each study was appraised. Common themes identified were then classified and sorted according to the five CFIR domains, followed by a consensus-based analysis by two authors (DC and AS).
Results
Study selection
The database search yielded 12,380 studies. In total, 8562 articles were screened based on title and abstract after duplicates were removed. Our study selection process yielded 319 articles eligible for full-text review. After a consensus for inclusion was reached by three researchers (CP, AO, and SW), 55 studies were selected for scoping review (Figure 1).
Themes from the Consolidated Framework for Implementation of Research (CFIR)
Barriers and facilitators to implementation of the intervention were sorted within each CFIR domain (Figure 2). For our study, Innovation refers to how the VTE risk assessment model intervention or protocol was implemented. The Outer Setting refers to factors outside the hospital that impact the implementation of the risk assessment model; for example, government regulations. The Inner Setting comprises the hospital, rules and regulations within the hospital, and healthcare team structure. The Individuals domain refers to the providers and clinicians who are responsible for VTE risk assessment and prophylaxis. Finally, the Implementation Process domain refers to the process of carrying out the intervention and the steps leading up to it.
Barriers for implementing venous thromboembolism (VTE) risk assessments
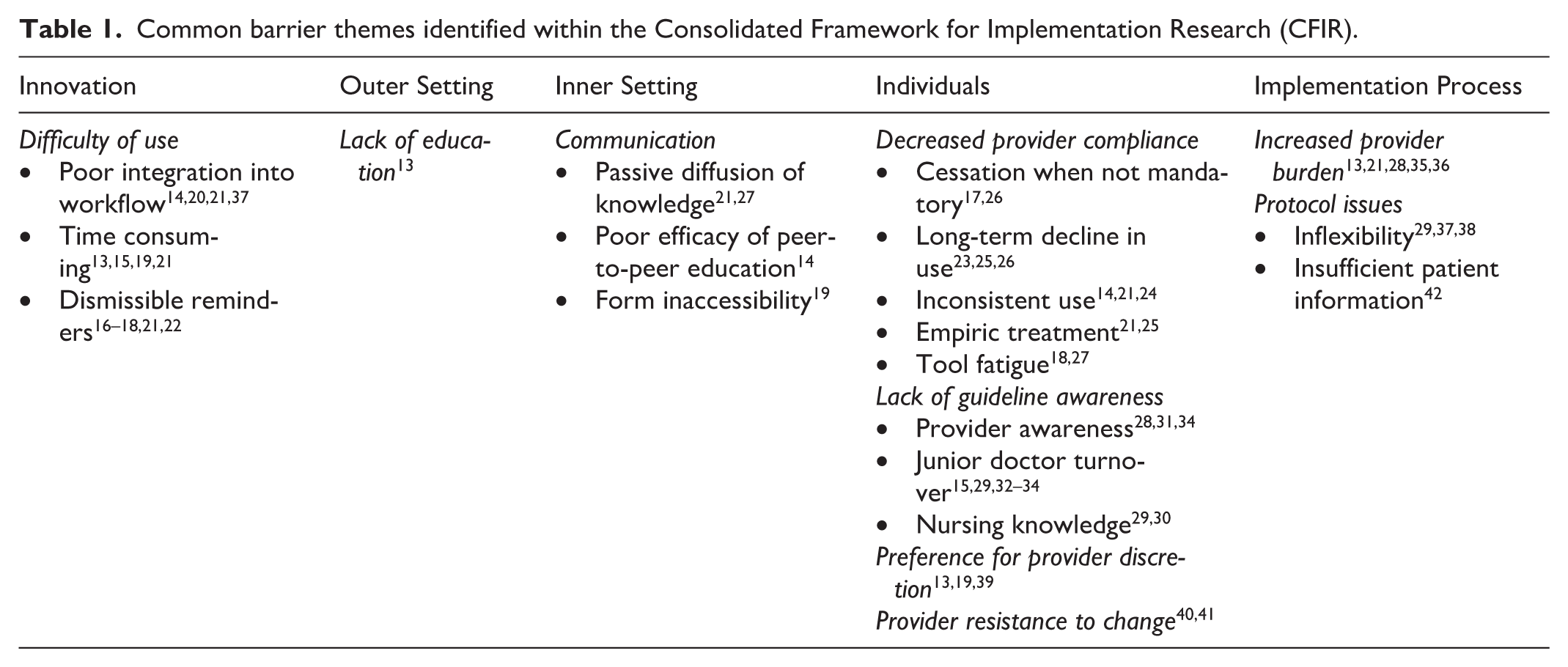
Three barriers under Innovation, one under Outer Setting, three under Inner Setting, 10 under Individuals, and three under Implementation Process (Table 1) were identified. The most common barrier themes were: difficulty of use,13–22 decreased provider compliance,14,17,18,21,23–27 lack of guideline awareness,15,28–34 and increased provider burden.13,21,28,35,36 Examples of barriers are described in Table 2.
Common barrier themes identified within the Consolidated Framework for Implementation Research (CFIR).
Cited examples of common barrier themes.
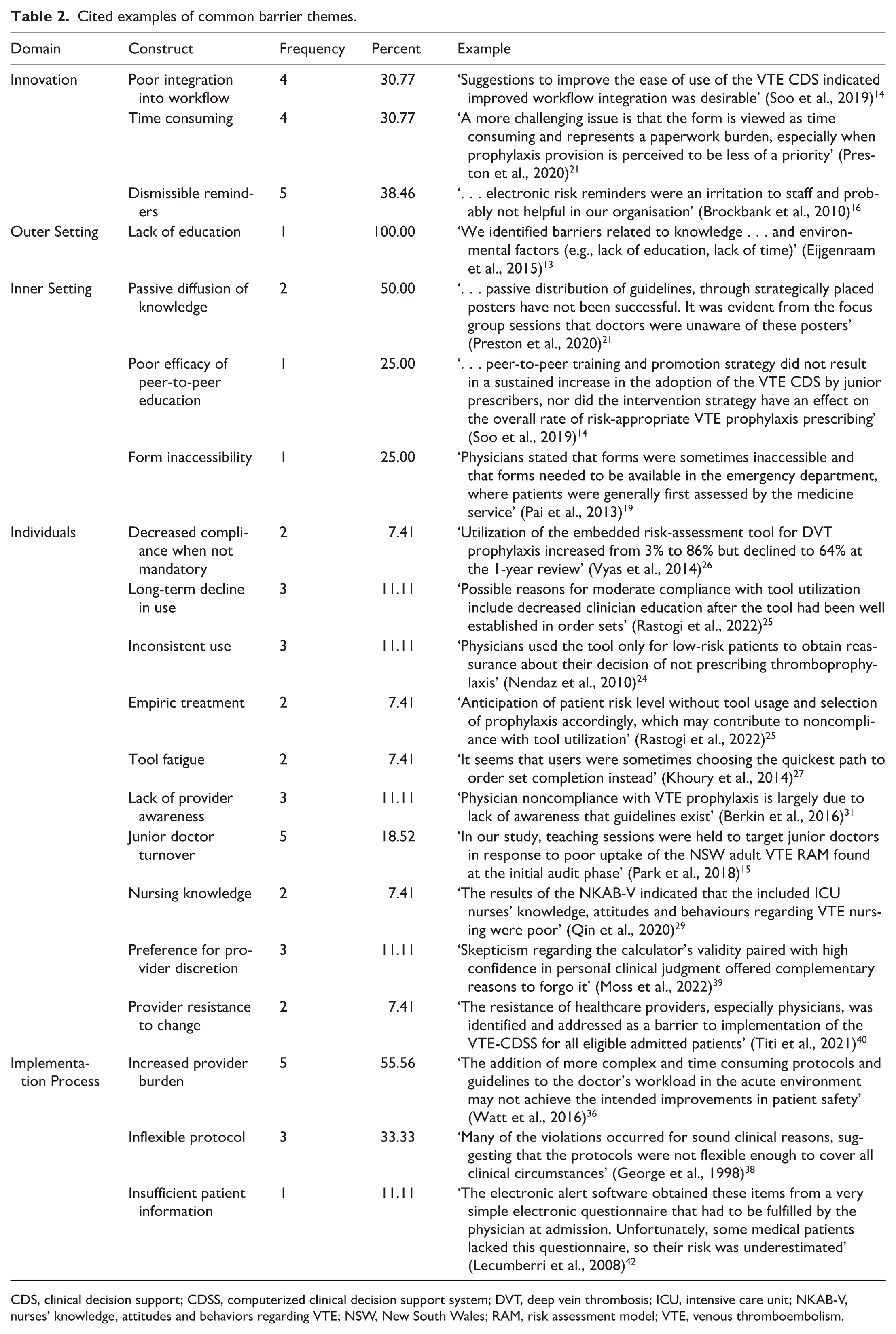
CDS, clinical decision support; CDSS, computerized clinical decision support system; DVT, deep vein thrombosis; ICU, intensive care unit; NKAB-V, nurses’ knowledge, attitudes and behaviors regarding VTE; NSW, New South Wales; RAM, risk assessment model; VTE, venous thromboembolism.
The most commonly reported barriers to VTE risk assessment implementation were identified in the Individual domain. Attending physicians were often cited as resistant to the implementation for various reasons. One study found providers mistrusted a ‘one size fits all’ approach due to the complex and heterogenous nature of hospitalized patients, 19 particularly in the setting of inflexible protocols.29,37,38 Providers may not understand the utility of using a VTE risk assessment tool, leading to inconsistent use either due to tool mistrust or a preference for using their own clinical judgment.13,19,39 Other barriers to provider adoption were due to changes in workflow 40 or fear of increased liability. 41 When interventions were not mandated, providers used their own unstandardized risk stratification frameworks, resulting in failed stratification of patient VTE risk.25,39
Even when risk assessment tools were mandated, a commonly cited barrier was an increase in provider burden.13,21,28,35,36 Three studies reported that the process of performing risk assessments was too time consuming.13,15,19,21 One study found that patients were inappropriately labeled as low-VTE risk simply because choosing low-VTE risk was the fastest way to finish the assessment tool. 27 In contrast to forcing functions, having easily dismissible reminders in the electronic medical record (EMR) preserved clinician autonomy and alleviated burden but resulted in poor provider compliance.16–18,21,22 On the other hand, providing education and facility-specific statistics on VTE outcomes can help to shift provider attitudes and improve the frequency of prophylaxis assessment and utilization.16,31
Lack of communication regarding the presence of the VTE tool was a noted barrier in the Inner Setting. When junior providers (e.g., interns) and nurses were tasked with risk assessments, a lack of awareness resulted in failure to stratify risk. The annual turnover of new intern physicians was a commonly cited factor in inconsistent compliance to risk assessment.32,33 This barrier can be divided into two broad categories: education regarding the VTE prophylaxis risk assessment and communication about its whereabouts and availability. With regard to education, two studies found that ‘passive’ diffusion of knowledge alone regarding VTE prophylaxis tools with flyers or cards yielded little improvement to risk assessment tool use.21,27 With regard to access and availability, meetings with healthcare providers in one study revealed that many providers were unaware of the presence of posters or flyers, and that sometimes, nurses were unable to fill out prophylaxis checklists because they were occupied with treating patients. 21
Facilitators for implementing VTE risk assessments
There were seven total facilitators under Innovation, three under Outer Setting, two under Inner Setting, two under Individuals, and eight under Implementation Process (Table 3). The most common facilitators were ease of EMR integration,14,15,17,21–24,26,27,30,35,36,39,42–52 education,13,15,30,31,33,35,40,41,47–49,52–59 and VTE task force teaming.33,40,47,48,57,60,61 Examples of facilitators are described in Supplemental Table S1.
Common facilitator themes identified within the Consolidated Framework for Implementation Research (CFIR).
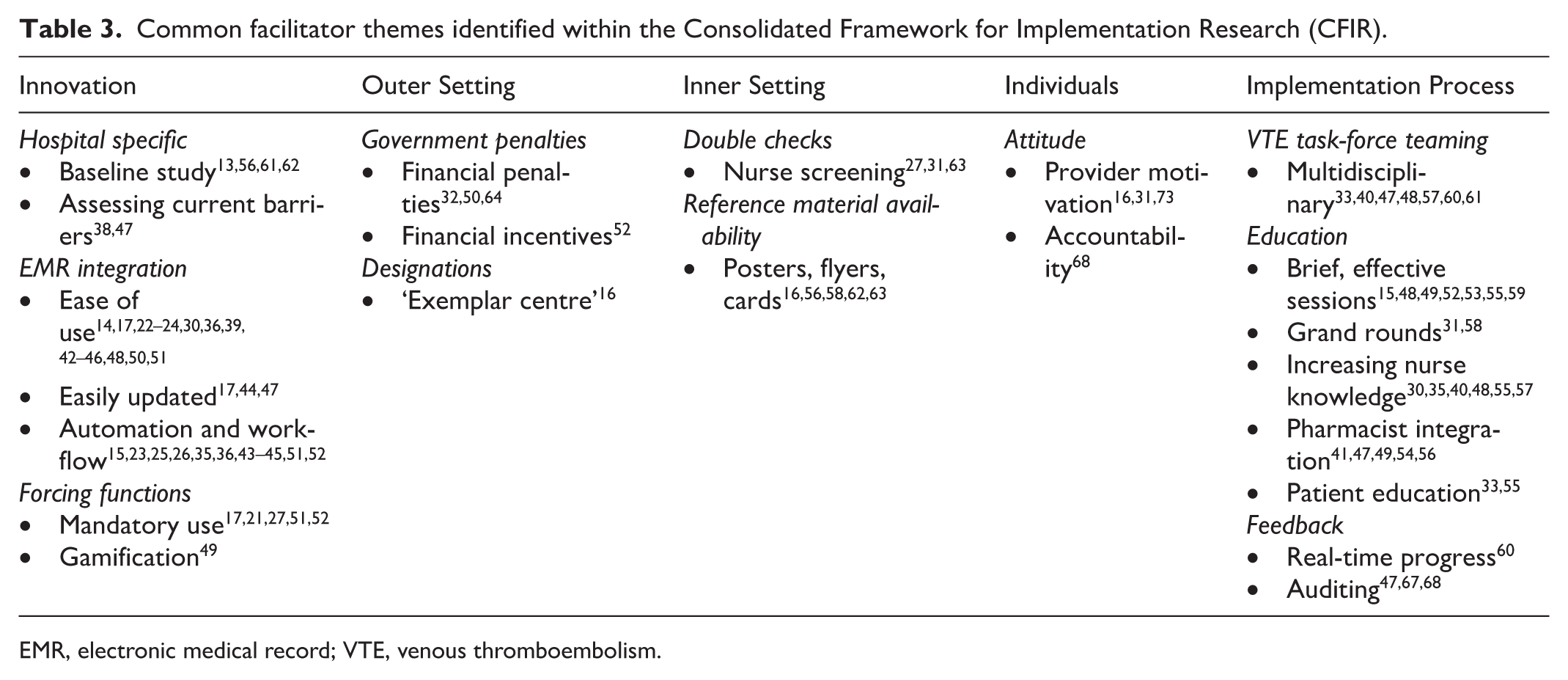
EMR, electronic medical record; VTE, venous thromboembolism.
The most commonly identified facilitators were in the Implementation Process domain. The creation of a multidisciplinary provider team in conjunction with provider education was critical to implementation.33,40,47,48,57,60–62 The most effective sessions were either brief or occurred during existing grand rounds sessions.31,58 Of note, the use of institution-specific statistics and outcomes was a good motivator for quality improvement during education sessions. 13
Shifting VTE prophylaxis assessment responsibility from attending physicians to nurses and pharmacists was successful in multiple studies. Many articles suggest the benefit of nursing education30,35,40,48,55,57 and pharmacist integration41,47,49,54,56 to distribute the responsibility of VTE risk assessment to more team members. Raising awareness of VTE to multiple team members ensures that more people can verify if a risk assessment was performed.27,31,63 Although lack of team awareness was a commonly cited barrier, multiple studies described significant benefits to educating either nurses or junior residents about the risk of VTE and the importance of conducting risk assessments.15,29,30,32–35,40,48,55,57
Within the Innovation domain, several institutions demonstrated a clear benefit to conducting a baseline study on their own institution regarding VTE incidence rate and identifying barriers to VTE risk assessment prior to the implementation of a risk assessment. A baseline study not only offers a point of reference to measure quality improvement in patient outcomes, but can be used as educational material to promote changes in provider attitude.13,56 Identifying those institution-specific barriers lends itself to the development of more tailored and beneficial implementation strategies.
Forcing functions, such as a hard stop inside the EMR that requires risk assessment completion before any further orders or documentation can be performed, were also cited as key facilitators to implementation.17,21,27,51,57 Fifteen articles found ease of use to be extremely important.14,17,23,24,30,36,39,42–46,48,50,51 One study in particular noted that gamification was an alternative to an electronic forcing function by empowering physicians to take an active role in the hospital VTE risk assessment initiative. 49 This came in the form of an inter-departmental competition regarding risk assessment tool compliance serving as a motivator.
Provider feedback during VTE interventions was a major theme across multiple studies. Real-time progress monitoring provided continuous awareness toward improvement of patient outcomes. 60 An alternative strategy includes auditing at set intervals and distributing audit results to clinicians regarding progress toward institution goals and the utility of the intervention. 47
The government and other regulatory agencies can play a role in if or how policies and interventions are implemented in healthcare settings. As an example, one study found that after the National Health Service (NHS) in the United Kingdom required mandatory collection of VTE risk assessment figures as part of its Outcomes Framework in 2010, hospitals were forced to implement changes that were compliant with this mandate. 50 However, these entities, along with local attitudes regarding VTE prophylaxis, can also place barriers to implementation of these interventions and policies. Three studies cited government regulations enforcing financial penalties32,50,64 and one cited financial incentives, 52 which were the most cited facilitators in the Outer Setting domain. An additional facilitator specifically within the United Kingdom is the designation of a hospital as a ‘VTE exemplar centre’. 16 This designation, although not providing explicit monetary reward, serves as a way for hospitals to distinguish themselves as centers providing exemplary care.
Overall, the majority of papers reviewed in this analysis cited barrier themes within the Individuals category and cited facilitator themes centered around Innovation and Implementation Process (Figure 3).
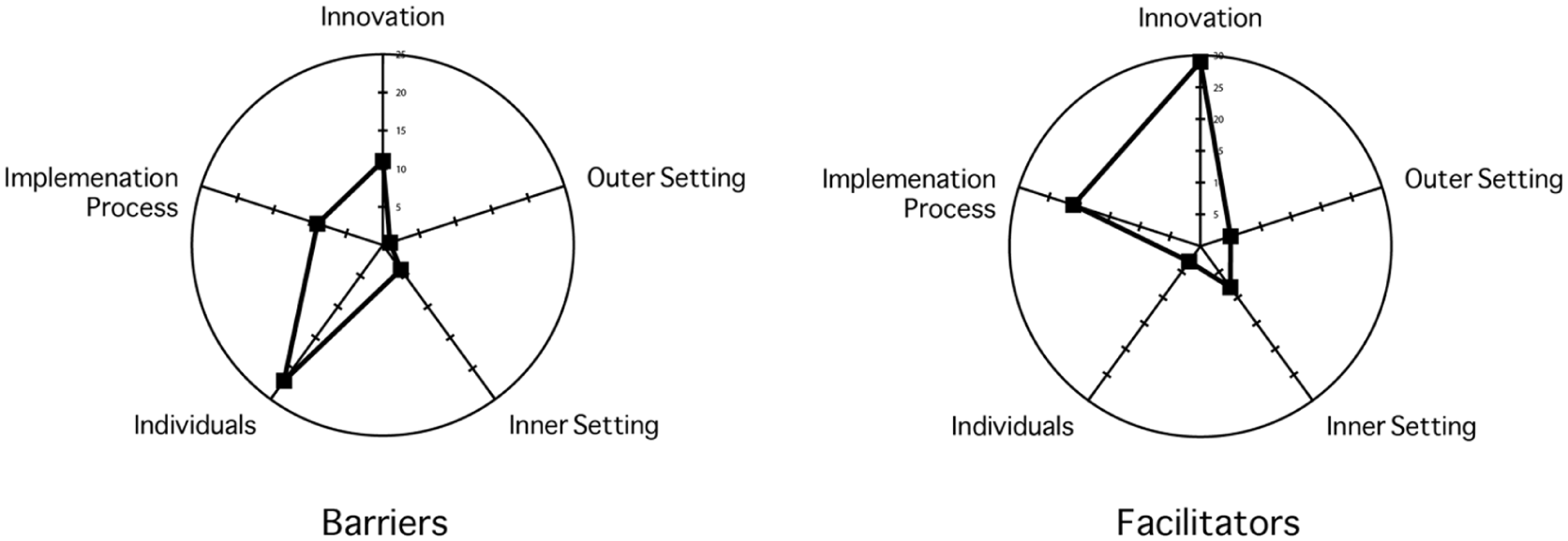
Radar plot comparing the number of articles citing the Consolidated Framework for Implementation Research (CFIR) themes.
Discussion
VTE risk assessments increase utilization of thromboprophylaxis and reduce the rates of HA-VTE. However, despite growing evidence in support of VTE risk assessment and prophylaxis, risk assessment use is not ubiquitous. The CFIR provides a framework to characterize and contextualize barriers and facilitators to implementation and to identify gaps in the current literature. Identifying and addressing these are critical to improving uptake of VTE risk assessment models, decreasing preventable VTE, and reducing costs and complications related to thromboprophylaxis overuse. The main findings of our paper were that the most commonly described barriers existed within Individuals and Inner Setting, whereas the most commonly cited facilitators related to Innovation and Implementation Process.
This analysis provides multiple evidence-based considerations for hospitals and organizations implementing VTE risk assessment tools. First, VTE risk assessment implementation must be easy to use with smooth integration into existing workflows. Previous work has shown that even physicians who are aware of the benefits of VTE risk assessment will have inconsistent tool usage. Therefore, a lack of knowledge regarding VTE risk assessment is not the only factor contributing to underutilization of VTE risk assessments. 12 Initiatives that intervened with existing provider workflows or added excessive burden led to decreased compliance. For example, smooth integration could involve EMR integration, such as a risk assessment tool built into the EMR admission order set. These automated tools guide VTE risk assessment, prompting physicians to prescribe thromboprophylaxis without significantly increasing physician burden. 65 Our data confirm findings of a smaller review of facilitators of VTE prevention in oncology patients, in which the importance of ease of workflow and EMR implementation emerged as a significant finding. 66
Second, there should be an element of provider incentive or forcing function to maximize usage of the VTE risk assessment. Provider compliance was the most frequently cited barrier to usage across all domains. Multiple intervention studies found declining rates of VTE risk assessment utilization following the initial implementation – a problem exacerbated when risk tools are not mandated. However, forcing functions, while effective in prompting providers to carry out VTE risk assessment, could contribute to provider burden. When risk assessment tools were mandated, some providers experienced tool fatigue and selected options that allowed them to complete the assessment the fastest. Tool misusage negates the utility of the risk assessment and must be considered when implementing forcing functions. However, despite the risk of increased provider burden, forcing functions consistently leads to improvement in VTE risk assessment usage and outcomes.
Third, implementation efforts should be led by multidisciplinary teams and directed toward a broad contingent of staff members, including junior and senior providers, nurses, and pharmacists. The inclusion of nonphysician providers in implementation efforts can help alleviate physician burden for completing risk assessments and ensuring appropriate VTE prophylaxis. Making VTE information easily accessible to everyone in the healthcare setting is also beneficial. Additionally, audits of team performance, public reporting, use of a physician champion, and tying risk assessment to performance measures promote sustained compliance with risk assessment.67,68
Finally, financial incentives or penalties are a very effective method of ensuring VTE prophylaxis implementation from the Outer Setting. Government mandates for VTE risk assessment and prophylaxis have the potential to facilitate the widespread adoption of these tools across multiple organizations. Indeed, a mixed methods review including 26 studies found benefits to multidisciplinary teams and government mandates in facilitating appropriate VTE risk assessment and management. 69 Nonfinancial incentives, such as the designation of a hospital as an exemplary center for care, are also noted as potential facilitators. Nevertheless, Outer Setting barriers and facilitators remain a large gap in this scoping review. Based on our review, studies have primarily focused on hospital-specific facilitators, barriers, and outcomes. Studies on nationwide guideline adherence or ‘pay-for-performance’ payment models could help fill this gap in the literature. 70 Another notable gap was in the Inner Setting. Compared to studies in the business literature on corporate culture and organization in implementation of various business initiatives and strategies, we found no similar studies in our review.71,72 As many hospital systems strive to become high reliability organizations, the impact of specific cultural barriers and facilitators to VTE risk stratification is a critical area for investigation.
There are limitations to this scoping review. This study included only articles written in English, which limits the scope of analysis. Although several international studies were included, cultural themes unique to nonnative English-speaking nations may not be identified. In addition, our scoping review did not discriminate between patients admitted to medical versus surgical units. Therefore, some nuances in VTE risk assessment that are unit-dependent may be lost.
Conclusion
This review aimed to identify common barriers and facilitators to the implementation of an in-hospital VTE risk assessment for VTE prophylaxis using the CFIR. The ease of use and integration of a VTE risk assessment into existing workflows are associated with successful implementation. Regarding clinician-specific barriers, a forcing function is a highly effective way to maximize the usage of a VTE risk assessment. Multidisciplinary approaches are integral to offsetting physician workload. Although government regulation and financial factors promote VTE risk assessment usage, future studies on how value-based care improves VTE are warranted. The results from this review can be utilized to create implementation strategies that promote VTE risk assessment use and avoid ineffective or counterproductive techniques.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X261419462 – Supplemental material for Barriers and facilitators to implementation of hospital-wide venous thromboembolism risk assessment models: A scoping review
Supplemental material, sj-docx-1-vmj-10.1177_1358863X261419462 for Barriers and facilitators to implementation of hospital-wide venous thromboembolism risk assessment models: A scoping review by Daniel S Cheah, Akshay Seenivasan, Chloé A Powell, Spencer Wilson, Geno Merli and Andrea T Obi in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.