
Abstract

A 39-year-old woman with a congenital slow-flow venous malformation (VM) involving the right shoulder, upper arm, and upper chest was referred for hematologic consultation. The VM had been partially resected in early childhood because of functional impairment. Since adolescence, she experienced frequent spontaneous bruising, dizziness when not using compression sleeves, and episodes of epistaxis. Her obstetric history included two spontaneous abortions. Surgical history was notable for splenectomy and cholecystectomy, during which hypofibrinogenemia was identified and managed with fibrinogen concentrate, vitamin K analogs, and tranexamic acid.
On examination, the VM extended over the right shoulder, upper arm, and chest as a reticulated bluish-purple discoloration with soft, compressible nodularity (Panel A). The lesion was most prominent over the deltoid and pectoral regions, with visible ectatic superficial veins and interspersed ecchymoses. She reported positional discomfort and pressure-induced pain, exacerbated by warm environments and physical exertion.

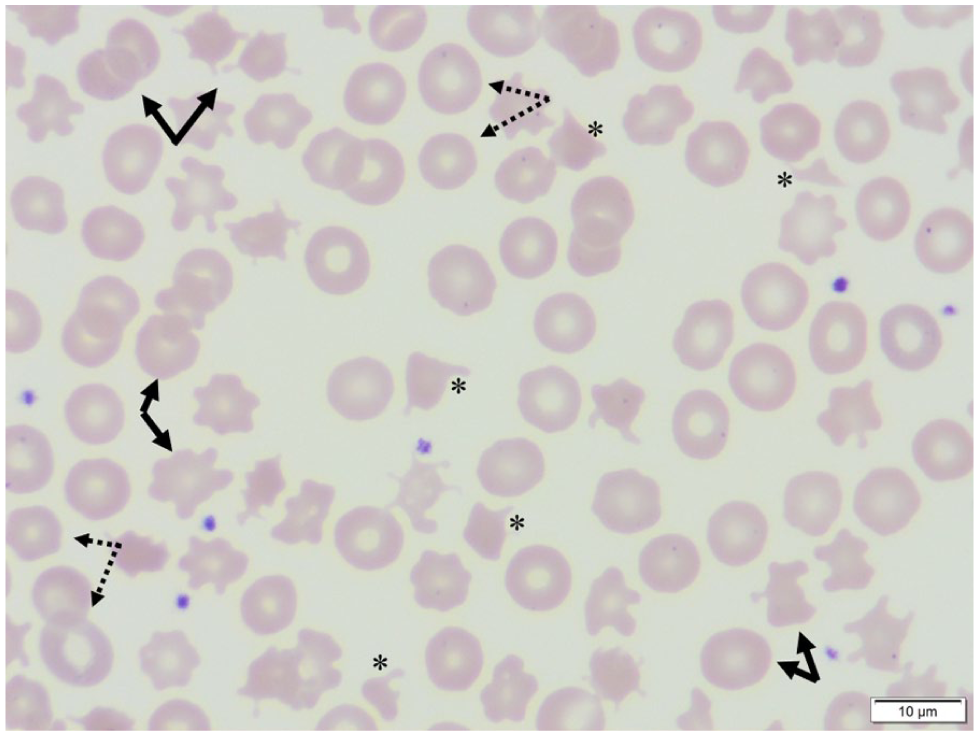
Laboratory evaluation revealed mild anemia (hemoglobin 11.0 g/dL; reference 11.7–15.5) and borderline thrombocytopenia (platelets 131 × 103/μL; 150–400 × 103/μL). D-dimer was markedly elevated (23,980 μg/L; normal < 500), and fibrinogen was critically reduced (0.62 g/L; 1.8–3.6). Prothrombin time was prolonged (13.5 s; 8.9–11.1) with INR 1.25, although activated partial thromboplastin time was normal (29.1 s; 24–35). Lactate dehydrogenase was 171 U/L (135–214). Total bilirubin was mildly elevated (1.44 mg/dL; 0.3–0.9) with direct bilirubin 0.66 mg/dL (< 0.3). A peripheral blood smear (Panel B) demonstrated schistocytes (asterisks), poikilocytosis (solid arrows), and anisocytosis (dotted arrows) consistent with chronic erythrocyte fragmentation secondary to localized intravascular coagulopathy (LIC).
This hematologic pattern—markedly elevated D-dimer, hypofibrinogenemia, and schistocytosis—supports persistent LIC progressing toward a chronic compensated disseminated intravascular coagulation (DIC) state, seen in extensive or deep slow-flow VMs, particularly with muscle involvement.1,2 LIC may acutely exacerbate with trauma, procedures, or spontaneous thrombosis and can rarely evolve into life-threatening DIC-associated hemorrhage.1,2 D-dimer and fibrinogen should be assessed at baseline and during symptom flares to guide timely intervention.2,3 Low-molecular-weight heparin is preferred for pain, thrombosis, or significantly abnormal parameters (including low fibrinogen) and for peri-procedural prophylaxis.1,2 Compression therapy remains integral to symptom control and reduction of stasis. 4 This case highlights schistocytes as a visible marker of LIC, underscoring the need for prompt evaluation to prevent progression to overt DIC.3,5
Footnotes
The panels are in color online.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.