
Abstract
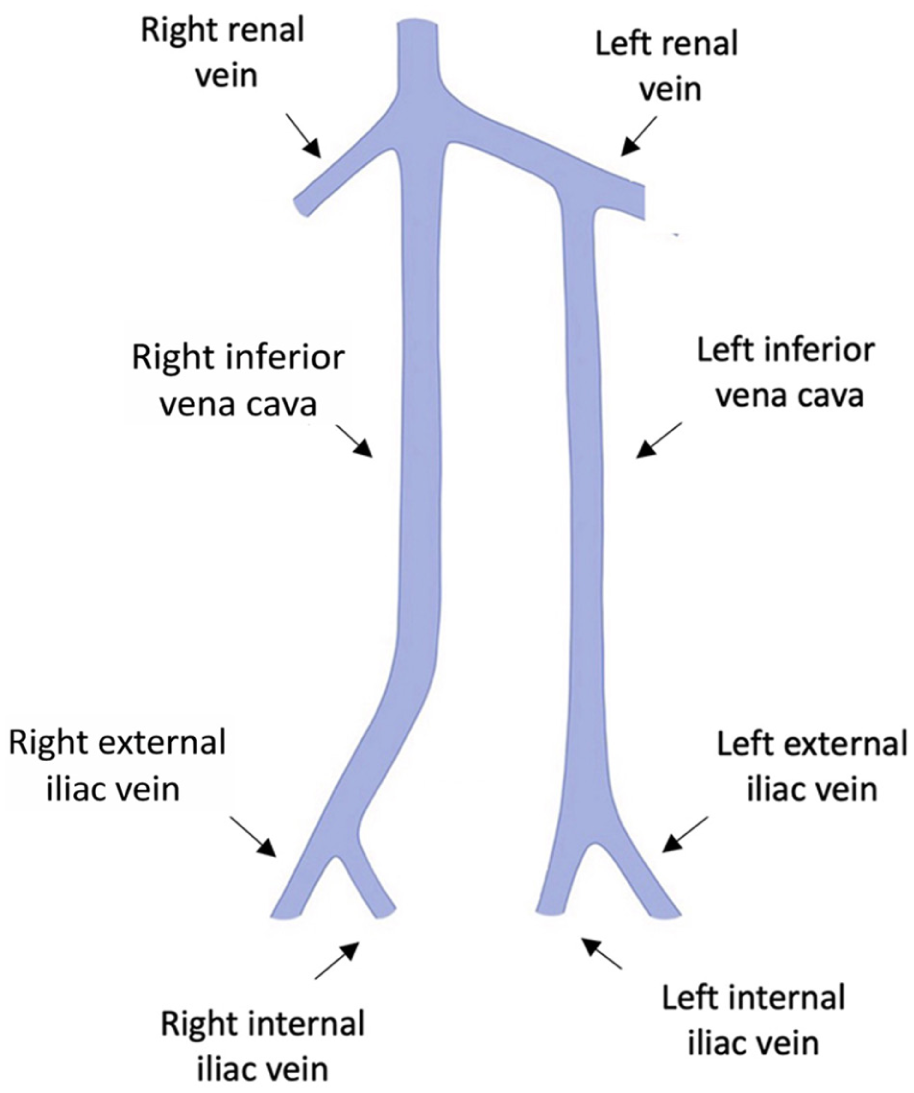
A 22-year-old woman with heterozygous factor V Leiden presented with acute right iliofemoral deep vein thrombosis and pulmonary embolism, with marked right-leg edema, pain, and difficulty walking. Magnetic resonance angiography demonstrated a duplicated inferior vena cava (DIVC) with azygos continuation, retroaortic left renal vein (Panel A), and thrombosis of the right iliofemoral axis. After an unsuccessful aspiration attempt elsewhere, she was treated with oral anticoagulation (edoxaban 60 mg) and thigh-high compression. Two months later, duplex ultrasound showed only partial recanalization with progressive symptoms and development of postthrombotic syndrome (PTS) (Villalta score of 11), prompting endovascular treatment.
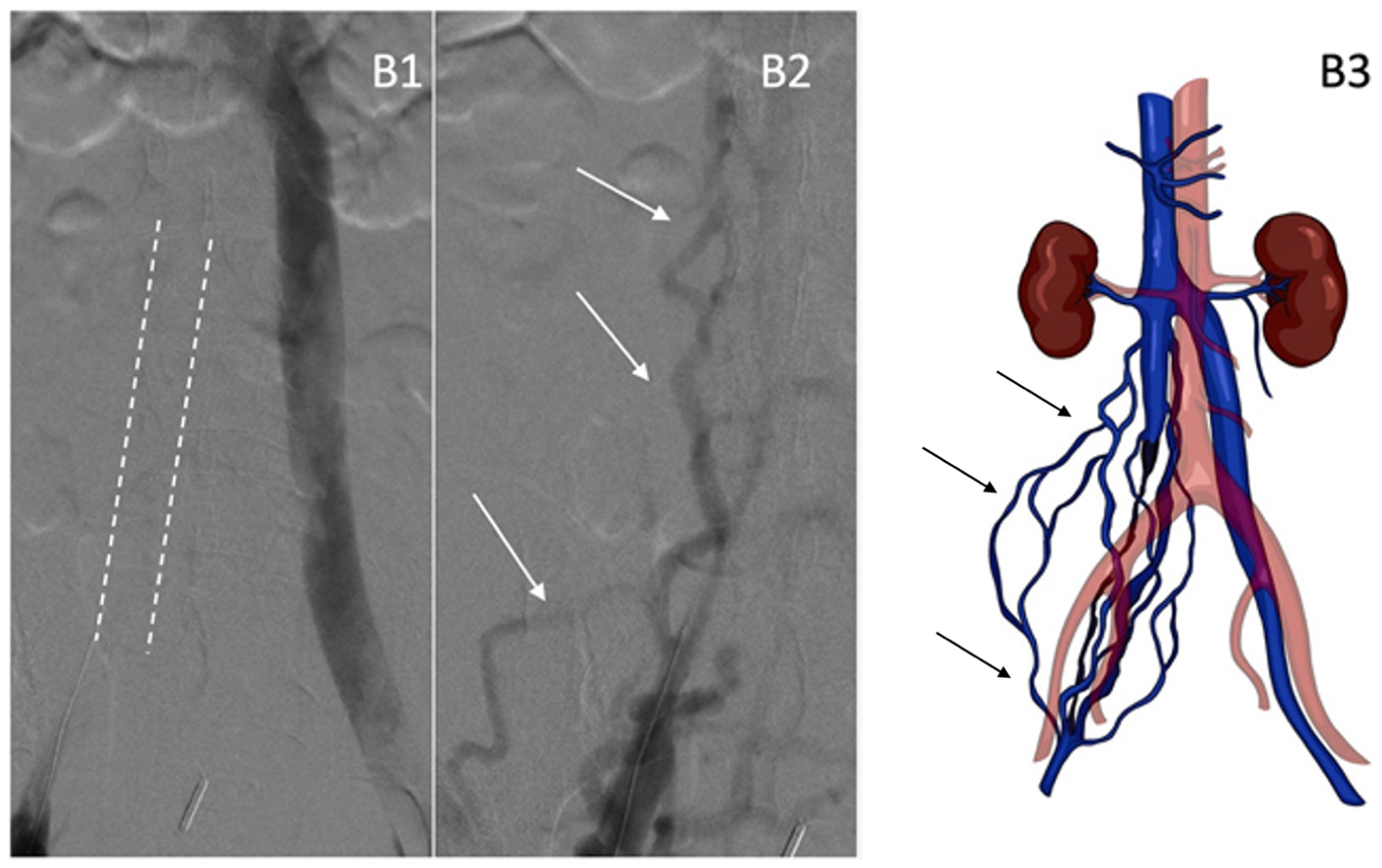
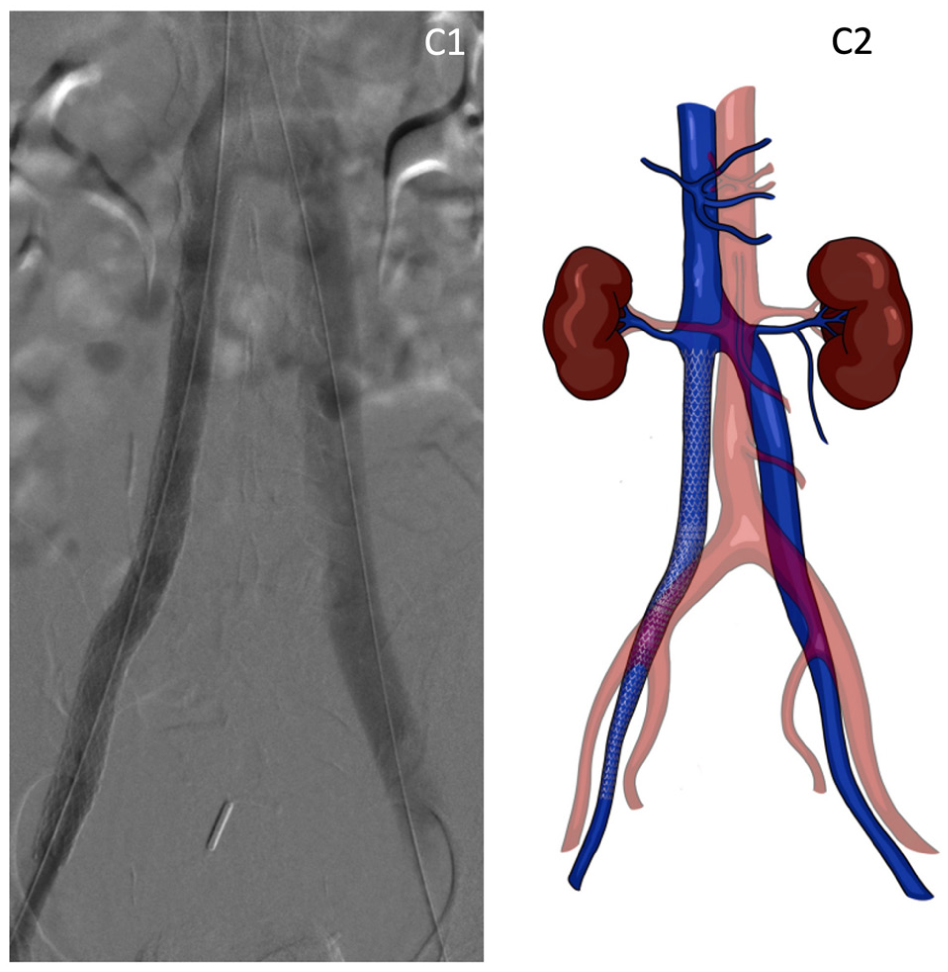
The procedure was performed under general anesthesia in a hybrid suite. Access was obtained from the right internal jugular vein and both mid-femoral veins, with systemic heparinization. Venography confirmed chronic occlusion of the right iliac axis (Panel B1: dashed outline) and right-sided cava with prominent pelvic collaterals (Panels B2 and B3, arrows). The lesion was crossed with a hydrophilic 0.035-inch wire and catheter, then exchanged for a stiff guidewire. Sequential balloon venoplasty was performed with intravascular ultrasound-guided sizing of venous stents. A VICI 16 × 90 mm (Boston Scientific, Marlborough, MA, USA) and an Abre 14 × 150 mm (Medtronic, Minneapolis, MN, USA) were deployed across the obstructed segments with postdilatation. Completion venography demonstrated restored right iliocaval outflow (Panels C1 and C2). The patient was discharged on postoperative day 2 on edoxaban and compression, with duplex follow-up. Symptoms improved at 1 month (Villalta score of 4) and remained stable at 5 months.
DIVC is the most common caval anomaly, often detected incidentally on cross-sectional imaging (reported prevalence ~ 0.2–3%) 1 and may coexist with pelvic venous variants. Although DIVC-associated deep vein thrombosis is uncommon, young patients with extensive thrombosis and thrombophilia may develop early PTS, causing chronic pain, edema, and disability. Evidence-based guidance for treating symptomatic venous obstruction in DIVC is limited. 2 When conservative therapy fails and quality of life is impaired, iliocaval venoplasty and stenting can re-establish outflow and reduce venous hypertension.3,4 Intravascular ultrasound helps define the lumen and optimize stent landing zones. In selected patients with symptomatic PTS and DIVC, endovascular iliocaval recanalization with venoplasty and stenting is feasible and can deliver meaningful symptom relief.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Domenico Baccellieri is a consultant for Becton Dickinson, Medtronic, and Philips. The other authors have no conflicting interests.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.