
Abstract
Background:
The study compared adjunctive procedures in limbs with saphenous reflux treated by endothermal ablation (ETA) or cyanoacrylate closure (CAC). Secondary outcomes included adverse events (AEs), unscheduled care, and treatment costs.
Methods:
We retrospectively reviewed 654 limbs (327 CAC, 327 ETA). Demographics, Clinical, Etiological, Anatomical, and Pathophysiological (CEAP) classification, revised Venous Clinical Severity Score (rVCSS), adjunctive procedures, and AEs within 6 months were recorded. Costs included index and adjunctive procedures, unscheduled visits, and imaging; all costs are reported in US dollars.
Results:
Concurrent adjunctive procedures were more frequent in ETA than CAC (phlebectomy 48% vs 6%; sclerotherapy 40% vs 7%, both p < 0.001). The need for staged procedures did not differ, and rVCSS improvement was comparable (ETA 5.0 ± 2.2 vs CAC 4.8 ± 2.3, p = 0.4). ETA patients had more unscheduled visits (9% vs 3%, p = 0.006) and ultrasounds (7% vs 2%, p = 0.007). Initial CAC treatment costs were higher ($2479 ± 617 vs $2332 ± 449, p = 0.001). Overall costs were higher for CAC (+$210, 95% CI: $104-317, p <0.001). In ETA, AEs increased costs ($2520 vs $2354, p = 0.008), AE-related costs with CAC were not significantly different ($2571 vs $2496, p = 0.298).
Conclusions:
ETA was associated with more adjunctive procedures and unscheduled care. CAC achieved similar clinical improvement with fewer concurrent procedures and unplanned follow up. Although total expenditures converged, CAC had higher upfront charges, whereas ETA accrued more downstream costs related to adjunctive treatment and AEs.
Background
Saphenous vein incompetence can be treated using endothermal ablation (ETA) or nonthermal, nontumescent (NTNT) modalities. Tributary veins may be managed concomitantly or in a staged manner, each with specific advantages. Staging allows time for natural regression of tributaries, potentially avoiding unnecessary treatment.1,2 Conversely, proponents of concomitant treatment argue patients prefer a single comprehensive procedure, which may yield early quality-of-life benefits. 3 However, routinely treating tributaries may overtreat some patients and increase the risk of thrombotic events and other complications.4–7
Cost is another consideration. Phlebectomy increases procedural cost and also may have de novo complications that add further expense. A postmarket study of 50 limbs treated with cyanoacrylate closure (CAC) mandated staged tributary treatment, and only 14% underwent phlebectomy. 5 This rate was lower than in prior ETA-based studies.1–4
This study compares concomitant and staged adjunctive phlebectomy rates following CAC versus ETA and evaluates total limb treatment cost. Secondary outcomes include changes in Clinical, Etiological, Anatomical, and Pathophysiological (CEAP) classification and revised Venous Clinical Severity Score (rVCSS), adverse events (AEs), and unscheduled visits and imaging.
Methods
Study design
We conducted a single-site retrospective review of symptomatic limbs treated by six surgeons between October 1, 2015 and March 31, 2019. A total of 327 limbs treated with CAC (VenaSeal Closure System; Medtronic, Minneapolis, MN, USA) were included. Limbs treated for recurrent superficial thrombophlebitis or with only accessory vein ablation were excluded. A comparator group of 327 limbs treated with ETA, representing approximately 13% of all ETA-treated limbs during the study period, was selected using random sampling by limb. To reduce bias from evolving practice patterns, limb enrollment was matched month-to-month between groups. The study received institutional review board exemption with full HIPAA waiver from Western IRB on June 12, 2019 (
Data collection
Data extracted included demographics, CEAP clinical class, rVCSS, and procedural details. AEs were identified from electronic medical records (EMRs) and phone logs, including those managed remotely or in person. Adjunctive procedures performed concomitantly or within 6 months of the index procedure were recorded. Posttreatment CEAP and rVCSS were typically assessed at 3 months. Sclerotherapy was categorized as cosmetic or medically necessary and recorded as staged or concomitant.
Adjunctive procedures
There was no fixed practice protocol mandating staged versus concomitant phlebectomy. Decisions regarding adjunctive procedures were made at the discretion of the treating surgeon and were based on vein size, anatomy, and the patient’s presentation and preference. During the study period, practice patterns differed by ablation modality. When CAC was performed, surgeons generally favored a staged approach to tributary treatment, influenced in part by prior participation in CAC clinical trials in which concomitant phlebectomy was disallowed to avoid confounding outcomes; however, concomitant phlebectomy was not prohibited and was performed in a minority of CAC-treated limbs. In contrast, when ETA was used, surgeons were more likely to perform concomitant phlebectomy, reflecting prevailing practice patterns at the time. Selection of CAC versus ETA was also per the surgeon’s discretion, and was determined by patient appropriateness for chosen modality, patient preference, and insurance coverage. In general, modality selection was not based on anticipated need for adjunctive procedures.
Cost analysis
Cost analysis included index procedures, sedation, follow-up treatments within 6 months, and unscheduled visits or imaging. Medicare rates were applied for patients ⩾ 65 years old; commercial rates were estimated using the average of the three most common private insurers for those < 65 years old. Cosmetic procedures and prescription medications were excluded from the total cost. Although medication costs were collected, they were omitted from the final analysis due to uncertainty regarding patient compliance and variability in insurance coverage.
Statistical analysis
Categorical variables were summarized as counts and percentages, and continuous variables as mean ± SD. Between-group differences in patient-level characteristics were assessed using t-tests, chi-squared tests, or Fisher’s exact tests. Limb-level comparisons used generalized estimating equations (GEE) to account for within-patient correlation. Gaussian GEE was used for continuous outcomes and logistic GEE for binary outcomes. For categorical variables with more than two levels, chi-squared testing was used. GEE was also used to estimate the effects of CAC versus ETA and adjust for covariates including age, sex, race, body mass index (BMI), CEAP class, rVCSS, phlebectomy, and sclerotherapy at index. Both univariable and multivariable models were computed. All statistical analyses were performed in R (R Foundation for Statistical Computing), version 3.6.0.
Results
Patient group analysis
Each group included 327 limbs (310 patients in the ETA group and 251 in the CAC group). Patient ages ranged from 18 to 96 years, with a mean of 58 ± 16 in the CAC group and 54 ± 14 in the ETA group (p = 0.007). The ETA group included more non-White limbs (11% vs 6%, p = 0.023). There was no statistically significant difference in sex distribution. BMI was slightly higher in the ETA group (27 ± 6 vs 26 ± 5). Baseline patient demographics and clinical characteristics are summarized in Table 1.
Procedure, patient, and limb characteristics.
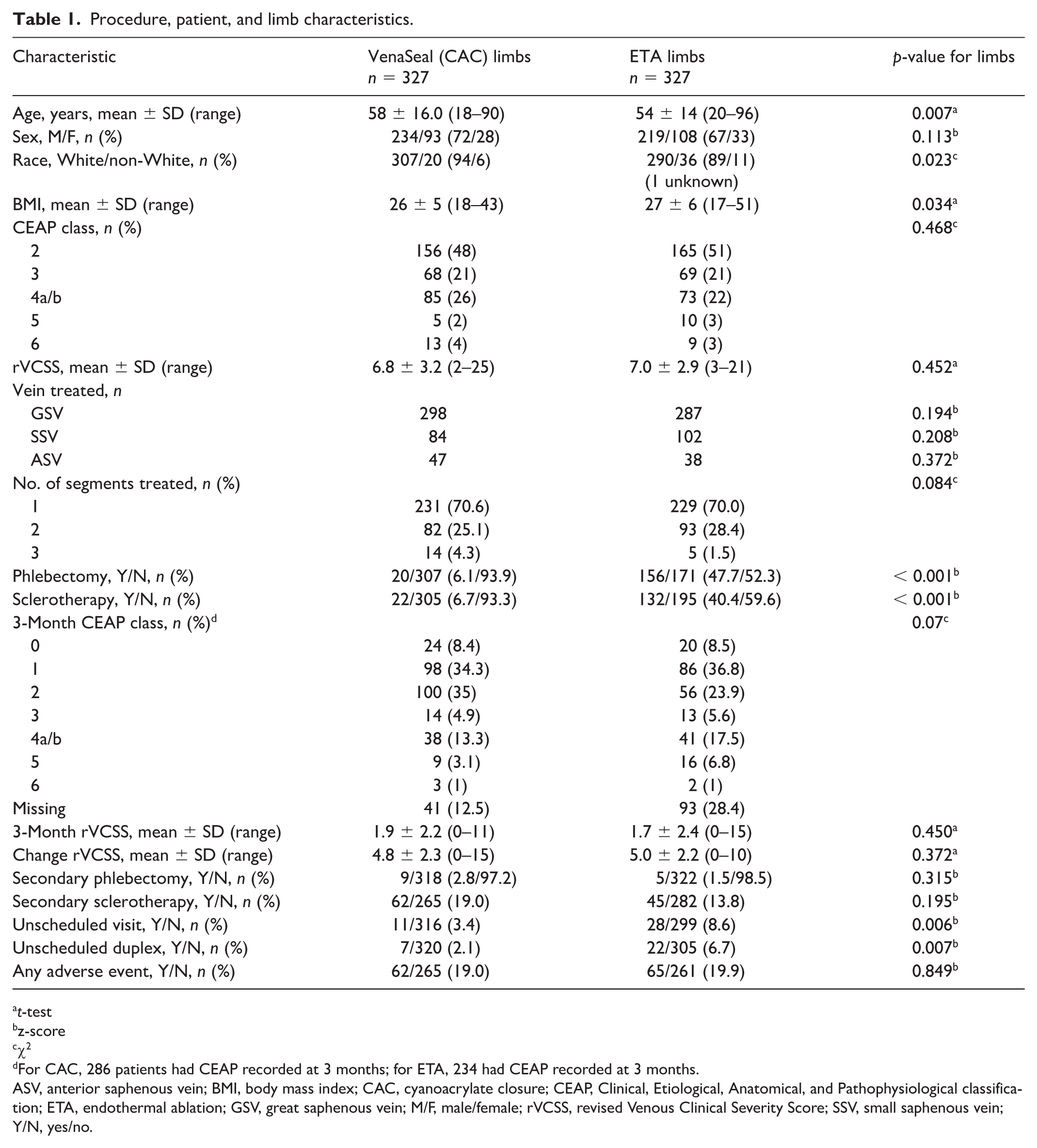
t-test
z-score
χ2
For CAC, 286 patients had CEAP recorded at 3 months; for ETA, 234 had CEAP recorded at 3 months.
ASV, anterior saphenous vein; BMI, body mass index; CAC, cyanoacrylate closure; CEAP, Clinical, Etiological, Anatomical, and Pathophysiological classification; ETA, endothermal ablation; GSV, great saphenous vein; M/F, male/female; rVCSS, revised Venous Clinical Severity Score; SSV, small saphenous vein; Y/N, yes/no.
Baseline CEAP clinical class distribution for the overall cohort was: 49.2% class 2, 21.0% class 3, 24.2% class 4, 2.3% class 5, and 3.4% class 6. No significant differences in CEAP class were seen between groups (χ2, p = 0.468). Baseline rVCSS was also similar (6.8 ± 3.2 for CAC vs 7.0 ± 2.9 for ETA, p = 0.452).
Procedures and outcomes
The ETA group included 223 limbs treated with radiofrequency ablation and 104 with laser ablation. There were no significant differences between groups in the types of veins treated (GSV, SSV, ASV) or the number of veins treated per limb (p = 0.084). Overall, 70% of limbs had one vein treated, 27% had two, and 3% had three. Bilateral same-day limb treatment was more common in the CAC group (32.3% vs 1.6%, p < 0.001) (Table 1). Procedural sedation was used in 66% of ETA patients and 3% of CAC patients.
At 3 months, CEAP clinical class distribution had shifted significantly across the entire cohort (p < 0.001 vs baseline): 8.4% were class 0, 35% class 1, 30% class 2, 5% class 3, 15% class 4, 5% class 5, and < 1% class 6. There was no significant difference between groups in 3-month CEAP class, although missing data were more frequent in the ETA group (28% vs 13%). rVCSS improved significantly in both groups (mean change: 5.0 ± 2.2 ETA vs 4.8 ± 2.3 CAC, p = 0.372), with final rVCSS values of 1.7 ± 2.4 (ETA) and 1.9 ± 2.2 (CAC).
Adjunctive procedures
Limbs in the ETA group were significantly more likely to receive concomitant phlebectomy (47.7% vs 6.1%, p < 0.001) and sclerotherapy (40.4% vs 6.7%, p < 0.001) compared to CAC-treated limbs. Rates of secondary phlebectomy within 6 months were low and not significantly different (1.5% ETA vs 2.8% CAC, p = 0.32). There was a trend toward more staged sclerotherapy in the CAC group (19.0% vs 13.8%, p = 0.07), but when cosmetic treatments were excluded, noncosmetic sclerotherapy rates were similar (10% ETA vs 13% CAC, p = 0.195). Total procedures performed during the index and follow-up periods were greater in the ETA group (Table 2; Figures 1 and 2).
Total procedures per limb.
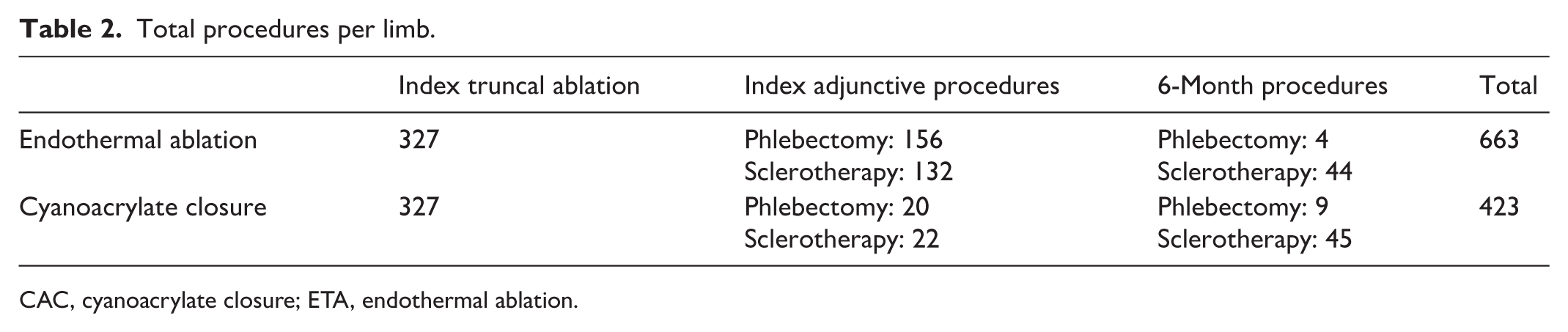
CAC, cyanoacrylate closure; ETA, endothermal ablation.
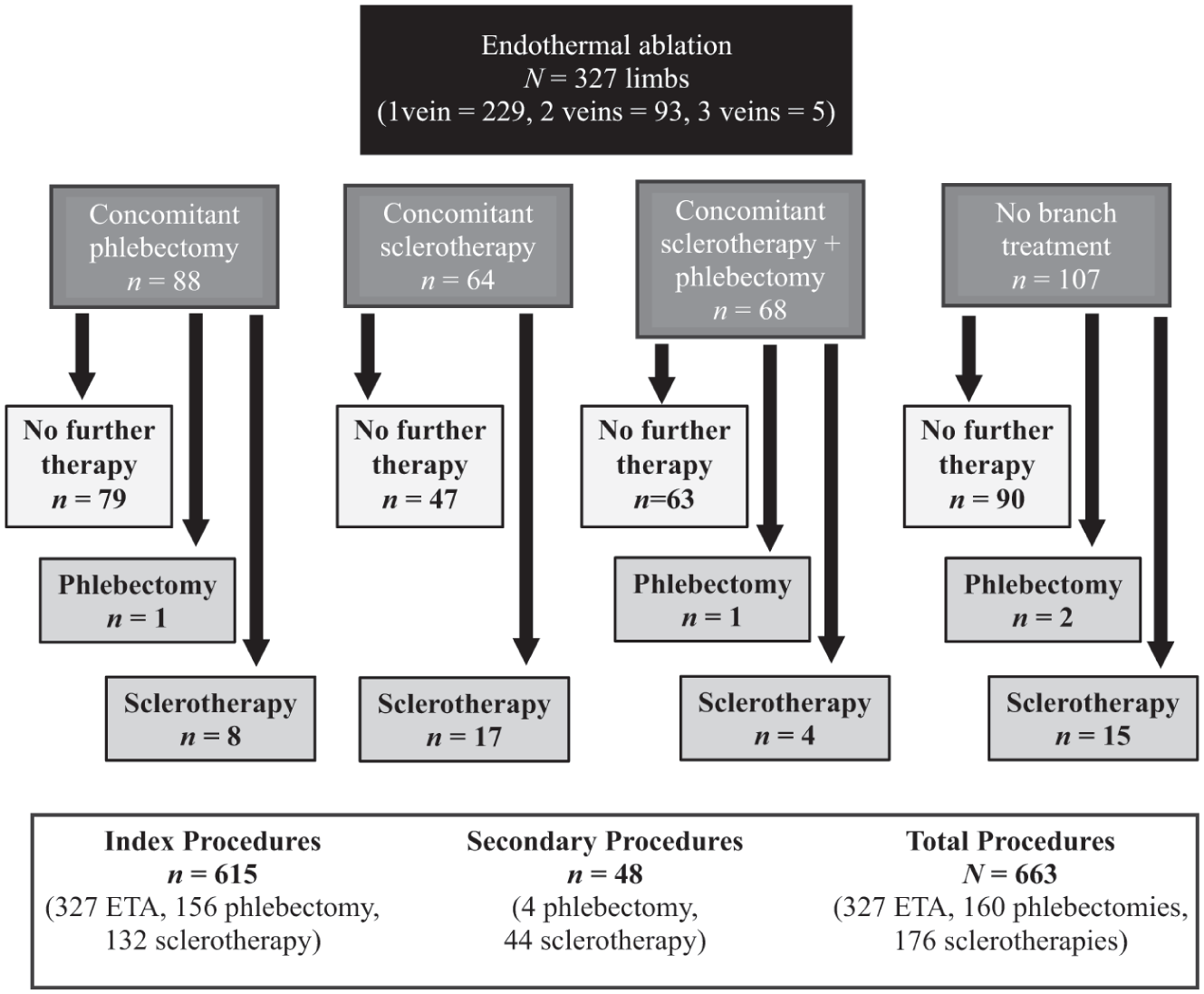
Procedures in the endothermal ablation (ETA) group.
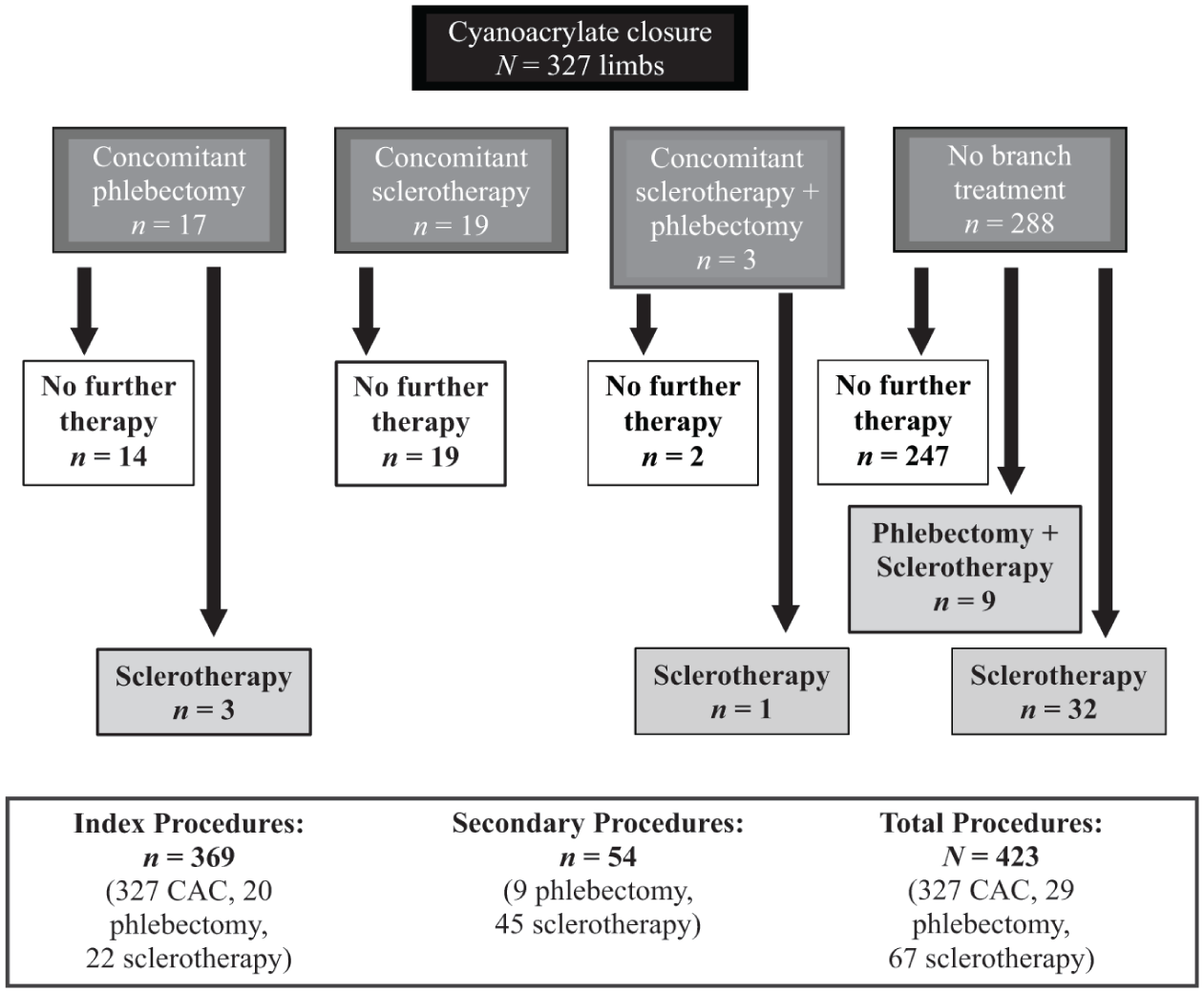
Procedures in the cyanoacrylate closure (CAC) group.
Univariable analysis (Supplemental Table S1, available online, available online) showed that, in addition to ETA treatment, phlebectomy at index was associated with male sex (OR 1.87, 95% CI: 1.29–2.73, p = 0.001), higher BMI (OR 1.19 per 5 units, 95% CI: 1.02–1.38, p = 0.024), CEAP class 3 (OR 2.31 vs class 2, 95% CI: 1.52–3.51, p < 0.001), and concomitant sclerotherapy (OR 2.90, 95% CI: 1.99–4.22, p < 0.001).
Concomitant sclerotherapy was associated with ETA treatment, CEAP class 5 (OR 3.70, 95% CI: 1.26–10.85, p = 0.017), CEAP class 6 (OR 4.04, 95% CI: 1.53–10.67, p = 0.005), increasing rVCSS (OR 1.15 per 1 point, 95% CI: 1.08–1.24, p < 0.001), and phlebectomy at index (OR 2.91, 95% CI: 2.00–4.25, p < 0.001).
Multivariable analysis (Table 3) confirmed that CAC-treated limbs were significantly less likely to undergo phlebectomy (OR 0.07, 95% CI: 0.04–0.13, p < 0.001) or sclerotherapy (OR 0.11, 95% CI: 0.06–0.19, p < 0.001). Male sex increased the odds of phlebectomy (OR 2.06, 95% CI: 1.30–3.27, p = 0.002) but decreased the odds of sclerotherapy (OR 0.40, 95% CI: 0.24–0.69, p < 0.001). CEAP class 3 increased phlebectomy risk (OR 3.35 vs class 2, p < 0.001), and classes 5 and 6 were associated with greater sclerotherapy use (ORs 3.71 and 7.61; p = 0.096 and p = 0.031, respectively).
Multivariable analysis of factors associated with concomitant phlebectomy and sclerotherapy at index procedure. a
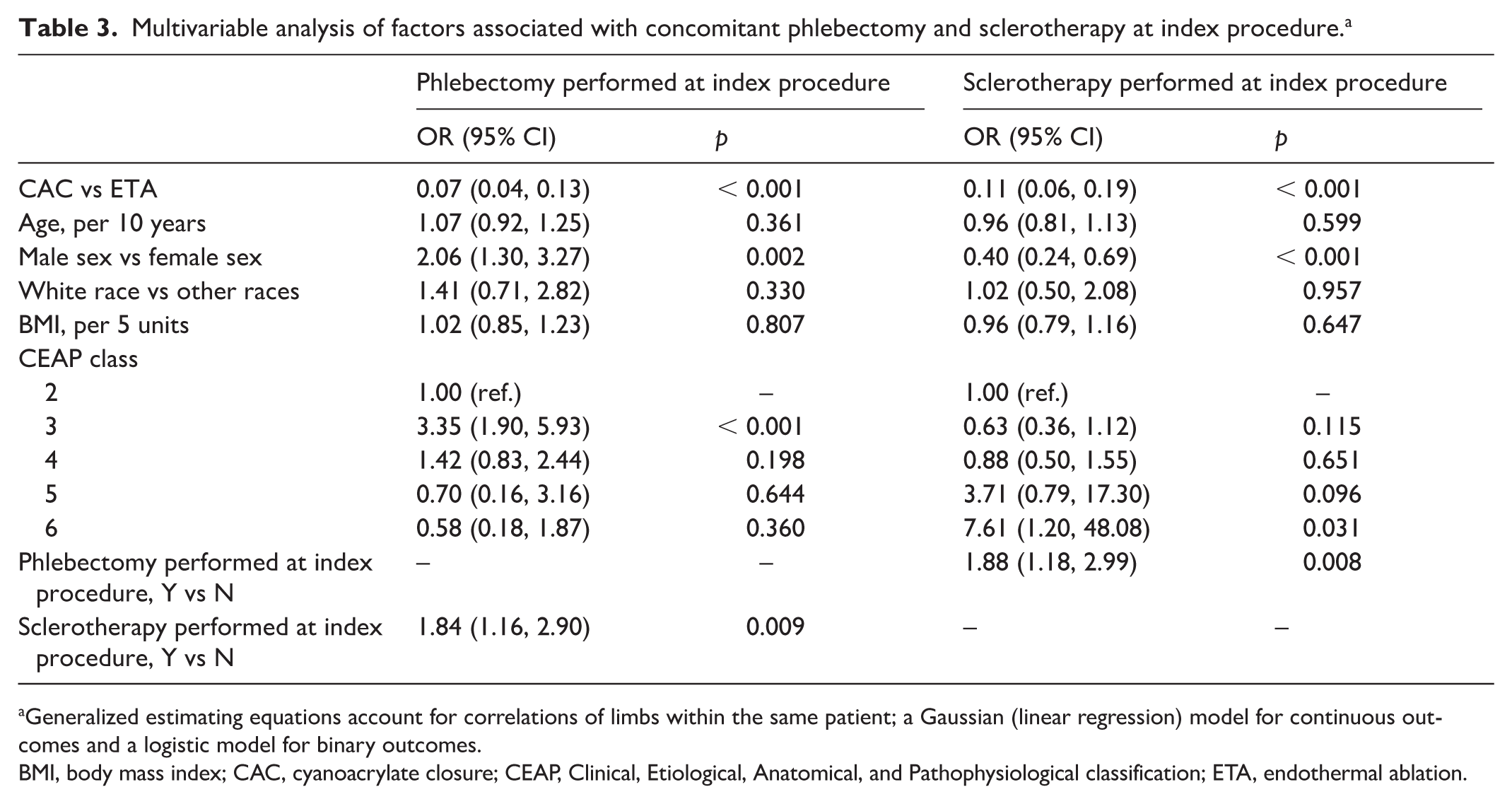
Generalized estimating equations account for correlations of limbs within the same patient; a Gaussian (linear regression) model for continuous outcomes and a logistic model for binary outcomes.
BMI, body mass index; CAC, cyanoacrylate closure; CEAP, Clinical, Etiological, Anatomical, and Pathophysiological classification; ETA, endothermal ablation.
Adverse events (AEs) and unscheduled visits
The ETA group experienced significantly more unscheduled visits (8.6% vs 3.4%, p = 0.006) and unscheduled duplex ultrasounds (DUS) (6.7% vs 2.1%, p = 0.007) compared to the CAC group (Table 1). In univariable analysis, CAC treatment was associated with lower odds of unscheduled visits (OR 0.37, 95% CI: 0.18–0.76, p = 0.006) and ultrasounds (OR 0.30, 95% CI: 0.13–0.72, p = 0.007). Male sex, phlebectomy, and occurrence of an AE were all associated with more unscheduled visits (ORs 2.26, 2.22, and 69.09, respectively; all p < 0.05). Older age (per 10 years, OR 1.31, p = 0.018) and CEAP class 5 (OR 5.32 vs class 2, p = 0.044) were associated with more unscheduled ultrasounds. There was a nonsignificant trend toward more ultrasounds in limbs that underwent phlebectomy (OR 1.98, p = 0.079).
AEs occurred in 65 ETA-treated and 62 CAC-treated limbs (p = 0.84), with no significant difference in overall AE frequency (Table 4). No AEs met criteria for serious AEs, including death, life-threatening events, hospitalization, or the need for surgical intervention. Multivariable analysis did not identify any patient or procedural characteristics associated with increased AE risk. Six ETA limbs and one CAC limb experienced two AEs. Total AEs were 70 for ETA and 62 for CAC, although the nature of events differed.
Adverse events associated with treatment.
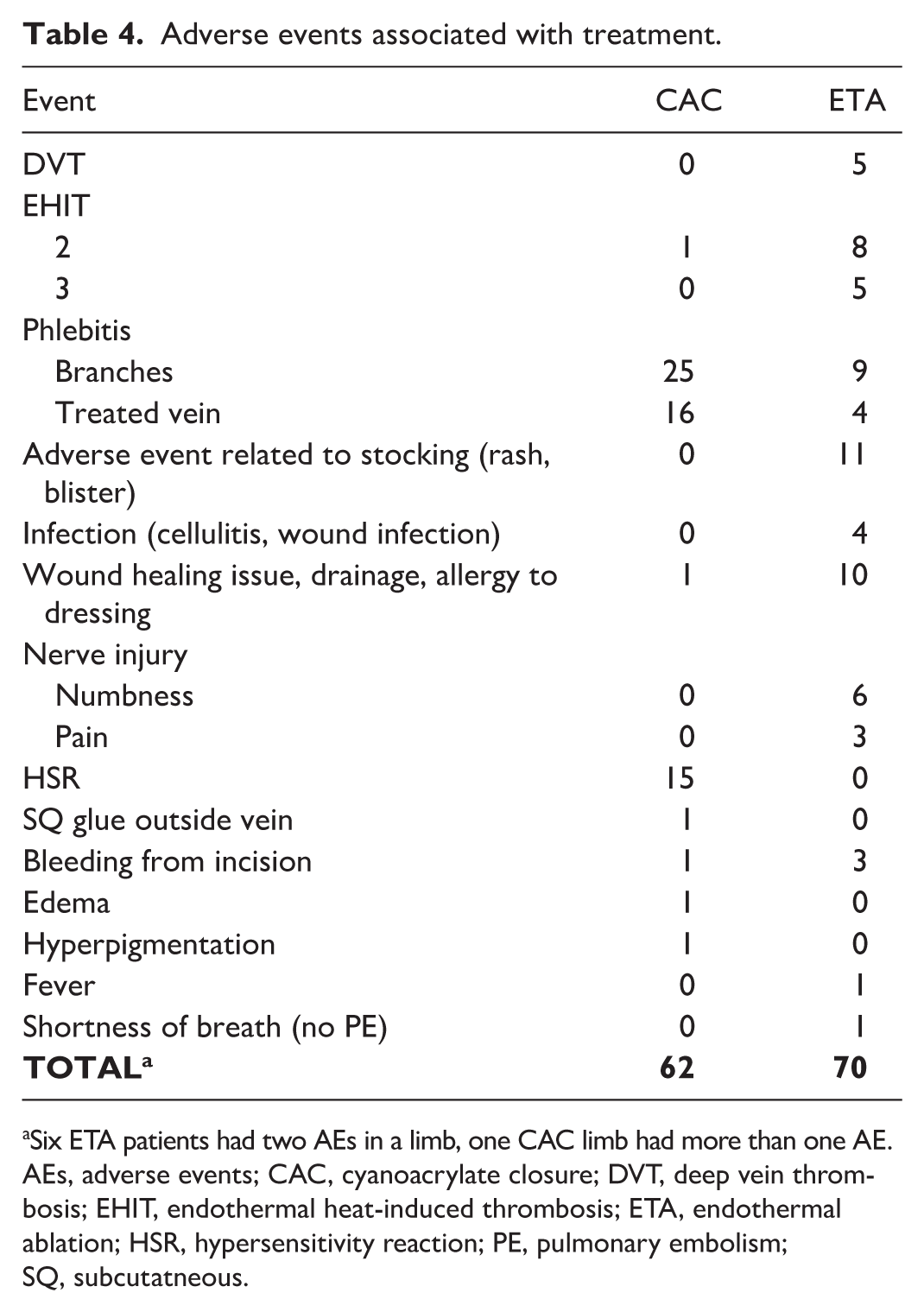
Six ETA patients had two AEs in a limb, one CAC limb had more than one AE.
AEs, adverse events; CAC, cyanoacrylate closure; DVT, deep vein thrombosis; EHIT, endothermal heat-induced thrombosis; ETA, endothermal ablation; HSR, hypersensitivity reaction; PE, pulmonary embolism; SQ, subcutatneous.
ETA-treated limbs had more thrombotic events (five calf/tibial DVTs, 13 EHITs), wound and stocking complications (n = 25), and nerve injuries (n = 9). CAC-treated limbs had more saphenous phlebitis (n = 16), branch varicosity phlebitis (n = 25), and hypersensitivity reactions (HSRs) (n = 15). All HSRs were mild to moderate; no reactions required prolonged or repeated steroid therapy or vein explantation. ETA had only four cases of saphenous phlebitis and nine of branch varicosity phlebitis.
There was a trend toward more AEs in ETA limbs treated with phlebectomy (24% vs 16%, p = 0.095), but this was not observed in the CAC group (p = 0.291). DVT/EHIT occurred more frequently in limbs that underwent phlebectomy (5.7% vs 1.7%, p = 0.005), but not sclerotherapy (2.6% vs 3.2%, p = 0.668). There was no association between AE frequency and bilateral treatment, vein type treated, or treatment modality.
Prescription medications for AEs were used in 23 limbs (six CAC, 17 ETA). One ETA limb required two medications. Anticoagulants were prescribed in 12 limbs (one CAC, 11 ETA), antibiotics in five (all ETA), steroids in five (four CAC, one ETA), and narcotic pain medication in two (one per group). One ETA patient with a nerve injury required referral to a pain specialist; costs related to this were unavailable.
The estimated total cost of prescribed medications was $360 (USD) for CAC limbs and $5308 for ETA limbs, based on local pharmacy pricing.
Cost analysis
The unadjusted total cost of limb treatment was 6.7% higher in the CAC group but did not reach statistical significance ($2485 ± 617 vs $2328 ± 549, p = 0.463). Univariable cost comparisons for index and total procedures are shown in Table S2.
Multivariable linear regression (Table 5) showed that the initial treatment cost was significantly higher in CAC-treated limbs (difference: $253, 95% CI: $153–353, p < 0.001) and in those undergoing phlebectomy ($270, 95% CI: $178–362, p < 0.001). Older age was associated with lower cost (per 10 years: −$129, 95% CI: −$158 to −100, p < 0.001).
Multivariable analysis of factors associated with cost of index procedure and total cost at 3 months. a
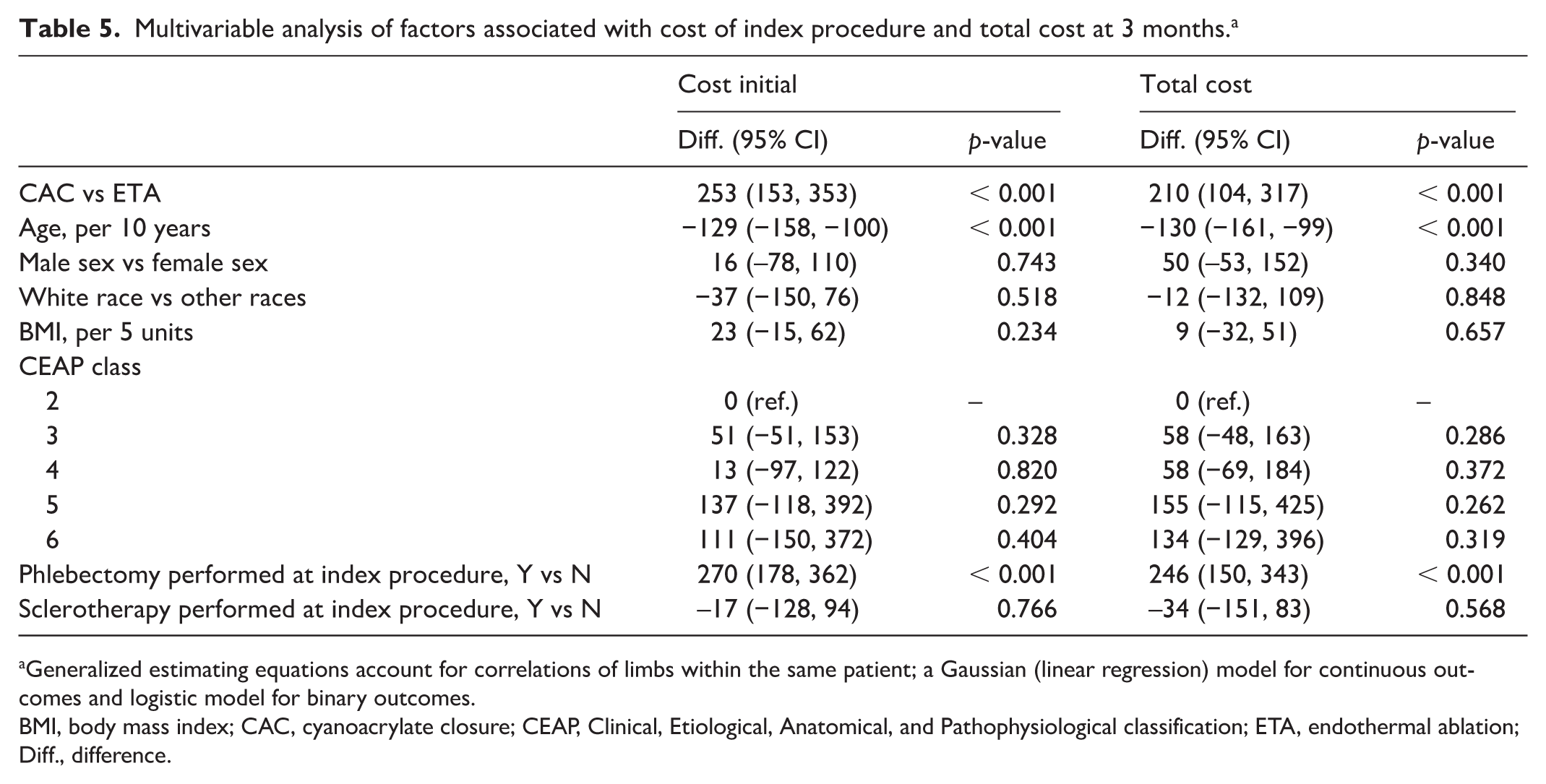
Generalized estimating equations account for correlations of limbs within the same patient; a Gaussian (linear regression) model for continuous outcomes and logistic model for binary outcomes.
BMI, body mass index; CAC, cyanoacrylate closure; CEAP, Clinical, Etiological, Anatomical, and Pathophysiological classification; ETA, endothermal ablation; Diff., difference.
When accounting for all costs incurred within 6 months—including adjunctive procedures, unscheduled visits, and DUS—the total per-limb treatment cost remained higher in the CAC group (difference: $210, 95% CI: $104–317, p < 0.001). Again, increasing age was associated with lower total cost (–$130 per decade, 95% CI: −$161 to −99, p < 0.001).
In ETA-treated limbs, total cost was significantly higher in those with AEs compared to those without ($2520 ± 104 vs $2354 ± 55, p = 0.008). In the CAC group, limbs with AEs also had higher mean costs ($2571 ± 148 vs $2496 ± 76), although this difference was not statistically significant (p = 0.298). Medication costs were excluded from total cost comparisons due to variability and uncertainty in prescription fill rates. However, the estimated pharmacy cost of AE-related medications was substantially higher in the ETA group ($5308 total vs $360 for CAC limbs).
Discussion
For a new treatment to be adopted, it must demonstrate safety and efficacy and offer meaningful advantages over existing options. These advantages may include improved patient experience, shorter recovery, fewer follow-up visits, or lower overall cost. Even if more expensive upfront, a new modality may be worth the investment if it reduces indirect burdens on patients, providers, and the healthcare system. CAC offers potential advantages in terms of rapid recovery. In the WAVES trial, patients returned to normal activities in a mean of 2.4 days and missed only 0.2 days of work. 5
Saphenous vein incompetence can be treated effectively with either CAC or ETA. Both have established long-term efficacy and safety. In randomized trials, they show similar outcomes in vein closure, rVCSS, and quality-of-life measures. 8 These clinical outcomes must be weighed alongside economic impact and the burden of adjunctive care.
Before the VeClose and WAVES trials, our practice routinely performed phlebectomy or sclerotherapy at the time of truncal ablation. However, both trials mandated staging of tributary treatment to avoid confounding short-term endpoints. We observed that tributary regression—especially with CAC—was more common than expected. In WAVES, 14% of CAC-treated limbs underwent phlebectomy, and 66% underwent sclerotherapy at 3 months. 5 In the current study, 8.9% of CAC-treated limbs received phlebectomy and 25.7% underwent sclerotherapy during the 6-month study period. This lower rate compared to WAVES may reflect the absence of trial-related incentives to perform completion procedures.
Limbs treated with ETA underwent significantly more phlebectomy and sclerotherapy overall. A concern with the staged approach of CAC is that reduced adjunctive treatment could compromise outcomes. However, rVCSS and CEAP class improvements were equivalent between groups, and overall AE rates were similar. Importantly, ETA’s higher use of adjunctive procedures correlated with increased costs, AEs, unscheduled visits, and DUS. Whether a more conservative, staged tributary approach with ETA would yield similar results remains unclear. Our findings suggest that staged care may be sufficient in many patients, regardless of the ablation method.
We observed that staged or concomitant sclerotherapy—when separated from cosmetic indications—was not associated with increased cost or AE rates in either group. Our practice typically favors phlebectomy for larger tributaries and sclerotherapy for smaller ones. However, we do not routinely document tributary diameter, so this study cannot compare the effectiveness of phlebectomy versus sclerotherapy. Ongoing studies, such as a UK trial comparing foam sclerotherapy to phlebectomy, may help answer this question. 9
Although we did not collect pain scores or return-to-work timelines, our AE review suggests that ETA-related AEs may have a greater impact on recovery. Thrombotic events, nerve injuries, and wound complications were more common in the ETA group—some likely related to adjunctive procedures rather than the ablation method itself. Prior studies have linked phlebectomy to increased thrombotic risk,6,7 and we observed a similar association. Recent studies reinforce these observations: a prospective comparison found CAC safer than radiofrequency ablation (RFA) for small saphenous vein reflux, 10 and a 2024 Japanese registry demonstrated low complication rates with CAC, supporting its favorable safety profile. 11 Together, these studies support the continued relevance of our findings, despite evolving reimbursement patterns. Twelve ETA patients in our study experienced dermatitis or blistering from postprocedure compression stockings. Although contact dermatitis has been described, 12 this finding is rarely reported after ETA and may have emerged here due to our systematic review of phone logs. In contrast, the most common AEs in the CAC group were HSRs and phlebitis, consistent with findings from WAVES.5,13 These events were typically self-limited and did not prolong recovery. HSRs observed after CAC were clinically consistent with delayed, localized inflammatory responses, most consistent with a Type IV mechanism, rather than acute IgE-mediated reactions. Importantly, CAC-related HSR did not result in increased unscheduled visits, imaging, or downstream healthcare utilization in this cohort.
A higher incidence of superficial phlebitis following CAC has been reported in prior randomized trials, including the VeClose trial, 8 and may reflect a localized inflammatory response to the presence of an intravascular adhesive rather than procedural or anatomic factors. In the present study, treated vein length did not differ between groups, making extent of ablation an unlikely contributor. Differences in compression practices and earlier return to activity after nontumescent CAC may also contribute, although these mechanisms remain speculative. Importantly, phlebitis in this cohort was self-limited and did not result in increased serious AEs or downstream healthcare utilization.
Though CAC had higher initial costs, ETA limbs accrued more downstream costs due to unscheduled visits and imaging. These visits also impose time and logistical burdens not captured in billing data. In contrast, AEs in CAC limbs were often handled remotely or during routine follow-up, minimizing added expense.
Long-term AE impact also warrants consideration. Many ETA-related AEs—like wound issues and stocking reactions—are tied to phlebectomy or postprocedure protocols. Conversely, CAC-related phlebitis might have been preventable had tributaries been treated concomitantly. These observations underscore that both under- and over-treatment of tributaries may lead to complications, regardless of the ablation method. At present, decisions about tributary treatment strategy rely on physician judgment and patient preference. Future studies may help define when staged versus concomitant care is most appropriate.
Although CAC is inherently more expensive than ETA, this cost difference narrowed in our study due to three factors: (1) higher likelihood of bilateral same-day treatment with CAC; (2) more adjunctive procedures in the ETA group; and (3) greater frequency of unscheduled follow-up and DUS in ETA-treated limbs. Notably, bilateral treatment was much more common with CAC, in part because the treatment volume is kit-limited rather than constrained by tumescent anesthesia or postprocedural soreness.
Our study did not include indirect costs—such as time off work or caregiver time—which likely further favor CAC. This is especially relevant for older patients whose adult children may need to accompany them to appointments. Hidden costs like these are real but difficult to quantify.
Strengths and limitations
Strengths of this study include its relatively large sample size, consistent data abstraction methods across treatment groups, and calendar-month matching of limbs to reduce confounding from time-related changes in clinical practice. We evaluated a broad and practical range of outcomes, including procedural costs, AEs, and unscheduled care utilization.
We also applied an inclusive definition of AEs, capturing not only major complications like thrombosis or nerve injury but also minor but real concerns such as phlebitis, blistering, and stocking reactions. This approach—supported by detailed phone log reviews—likely yields a more accurate picture of ‘real-world’ recovery experiences than studies that rely solely on structured follow-up visits.
Limitations include the retrospective design and occasional incomplete documentation—particularly for rVCSS in the ETA group, where scoring was recorded less consistently. Some AEs may have been missed if patients sought care outside our clinic. Conversely, some events captured over the phone might not have been classified as AEs had the patient been evaluated in person.
Selection of ablation modality and adjunctive treatment strategy was not randomized, and the specific factors influencing the choice of CAC versus ETA were not prospectively captured. Modality selection reflected real-world physician judgment, patient preference, and insurance coverage during the study period, which may have introduced confounding. Additionally, practice patterns such as more frequent concomitant phlebectomy with ETA and more frequent staging with CAC, reflect single-center practice and may not be generalizable to all clinical settings.
Another limitation is the use of cost estimates based on Medicare or private payer averages, which may not perfectly reflect actual reimbursement for every patient. We excluded prescription medication costs from total treatment cost due to variation in insurance coverage, fill status, and availability of coupons or samples. This analysis reflects care delivered in an outpatient vein practice setting and is therefore most applicable to similar outpatient practices. Although absolute reimbursement varies by region, payer mix, and site of service, the relative contribution of upfront device cost and downstream resource utilization to overall cost differences remains informative. This work was not intended to represent a formal cost-effectiveness or reimbursement modeling study, but rather a pragmatic comparison of relative resource utilization between treatment strategies in routine outpatient practice.
The study period predates subsequent changes in reimbursement patterns for venous interventions, and absolute cost estimates may not reflect current payment structures. However, the comparative framework of this analysis, including differences in upfront procedural costs, adjunctive treatment patterns, and downstream healthcare utilization, remains relevant when interpreting relative resource use across treatment strategies.
Importantly, the procedures in this analysis were performed 6 or more years ago. Although reimbursement has decreased for both CAC and ETA in the interim, the relative cost difference between the two modalities has also narrowed. Thus, although absolute costs reported here may overestimate today’s reimbursement, the overall trend and comparative findings likely still hold. Finally, our practice patterns—such as liberal phlebectomy use with ETA and conservative staging with CAC—reflect decision-making within a single high-volume vein center in a defined geographic region and may not generalize to all providers or practice settings. External validity may therefore be limited, and results should be interpreted in this context.
Conclusions
In this single-center retrospective analysis, CAC and ETA produced similar clinical improvements despite differences in treatment approaches. Adjunctive procedures were more common with ETA; though overall AE rates were similar, complication profiles differed. ETA was associated with more wound complications, nerve injuries, thrombotic events, and follow-up utilization, whereas CAC resulted in more phlebitis and HSRs. Higher downstream utilization contributed to narrowing the initial cost difference between CAC and ETA over time. These findings suggest that staged tributary management, particularly with CAC, can achieve comparable clinical outcomes and potentially reduce the number of adjunctive procedures and overall healthcare utilization.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X261434818 – Supplemental material for Adjunctive procedure utilization and cost comparison of cyanoacrylate versus endothermal ablation for saphenous vein reflux
Supplemental material, sj-docx-1-vmj-10.1177_1358863X261434818 for Adjunctive procedure utilization and cost comparison of cyanoacrylate versus endothermal ablation for saphenous vein reflux by Kathleen Gibson, Kim Glorieux, Renee Minjarez, Elena Foster, Moni Neradilek and Nayak Polissar in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors disclosed the following potential conflict of interested with respect to the reserach, authorship, and/or publication of this article. Dr Gibson receives research support from Medtronic and Gore; she is on the scientific advisory board and is a speaker for Medtronic, Boston Scientific, Gore, and Phillips. Dr Minjarez receives research support from Bard. The remaining authors have no conflicting interests.
Funding
The study was funded with an investigator-initiated research grant from Medtronic. Medtronic had no role in the study design, data collection, data analysis, data interpretation, or manuscript preparation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.