
Abstract
Background:
We initiated an institutional pathway for the outpatient treatment of low-risk patients with venous thromboembolism (VTE) and evaluated emergency department (ED) discharge rates and safety outcomes before and after pathway initiation. This pathway was augmented by the ability to schedule a 1-week follow-up with an outpatient provider in a vascular medicine clinic, a 30-day direct oral anticoagulant (DOAC) prescription, and anticoagulant education facilitated by the ED clinical pharmacist.
Methods:
A retrospective cohort of 1260 patients with VTE presenting to the ED between July 1, 2014, and June 30, 2018, was identified in the electronic health record (EHR) by a natural language processing algorithm scanning radiology reports for the presence or absence of pulmonary embolism (PE) or deep venous thrombosis (DVT). We compared patients who presented 2 years before and 2 years after pathway initiation (July 1, 2016) using a regression model to examine the independent effect of ED pathway initiation on discharge rates.
Results:
Patients with VTE before (N = 575) and after (N = 685) pathway initiation differed significantly in their prevalence of hypertension, prior hospitalization, and prior PE. Pathway initiation trended toward fewer ED discharges of low-risk patients with VTE (aOR = 0.74, 95% CI: 0.48 to 1.13). Older age, recent hospitalization, prior PE, and higher heart rate (HR) were associated with lower odds of ED discharge. There were no significant increases in ED return visits, hospitalizations, or bleeding events following pathway initiation.
Conclusions:
Initiation of a VTE discharge pathway was complicated by an increase in the proportion of patients with recent hospitalizations and prior PE in the postpathway period, which was associated with lower odds of ED discharge.
Keywords
Introduction
Venous thromboembolism (VTE), including deep venous thrombosis (DVT) and pulmonary embolism (PE), represents the third most common cardiovascular disorder, with an annual incidence of one in 1000 persons.1,2 The incidence of VTE has increased in both the United States (US) and Europe over the last two decades.3–5 The multinational RIETE registry reports only one in every 13 patients with PE eligible for home treatment is treated at home, suggesting a misalignment of patient severity and resource use. 6 Although high-risk PE is associated with considerable mortality, the 30-day mortality rate for intermediate and low-risk patients is 3–11% and < 1%, respectively.7–9 Depending on the criteria used, it is estimated that approximately 30–50% of patients with PE may be low risk and therefore safe for discharge from the emergency department (ED).10–14 Patients with DVT have a considerably lower risk of morbidity and mortality than with PE, so a similar opportunity to safely increase the proportion discharged from the ED is available as well.10,15,16
Risk stratification tools and monotherapy using direct oral anticoagulants (DOACs) have facilitated outpatient treatment of VTE. 17 In collaboration with stakeholders in cardiovascular medicine and emergency medicine, we developed a comprehensive institutional pathway for outpatient treatment of low-risk patients with VTE and implemented this pathway on July 1, 2016. 16 In an effort to evaluate the effect of this initial pathway, International Classification of Diseases, Ninth and Tenth Revision (ICD-9 and ICD-10) codes were first explored to identify ED patients with a diagnosis of VTE. This mechanism demonstrated poor positive predictive value, consistent with prior literature.18–20 Authors delayed the primary analysis to develop and separately publish a natural language processing (NLP) tool to accurately identify positive diagnoses of VTE. 21 Using this validated tool, we describe patient characteristics, ED disposition decisions, anticoagulation treatment, and 30-day adverse events in the 2 years prior to and 2 years following pathway initiation.
Methods
Design
A retrospective cohort of 1260 patients presenting to the adult ED between July 1, 2014, and June 30, 2018, and found to have VTE on imaging during the ED visit were stratified into two cohorts: those who presented within 2 years prior to and those who presented within 2 years after initiation of the discharge pathway (Figure 1). The 2-year pre- and postpathway windows were selected to provide stable comparison periods and reduce contamination from rollout effects. The pathway (Figures 2 and 3) was initiated on July 1, 2016, and added the following items to our care processes: (1) an institutional outpatient VTE guidance document; (2) a process for the ED provider to schedule a 1-week follow-up with an outpatient provider in a vascular medicine clinic; and (3) a 30-day DOAC prescription and anticoagulant education facilitated by the ED clinical pharmacist. The pathway was made available within an electronic folder containing institutional clinical workflow resources which were supported by targeted provider education. The pathway was supported by validated decision rules (e.g., Pulmonary Embolism Severity Index [PESI]), and enriched with additional criteria (troponin value, thrombus burden, additional comorbidities). Patients were operationally deemed low risk if they met all criteria sequentially moving from top to bottom within the pathway (see supplemental Figures S1 and S2 for complete details).
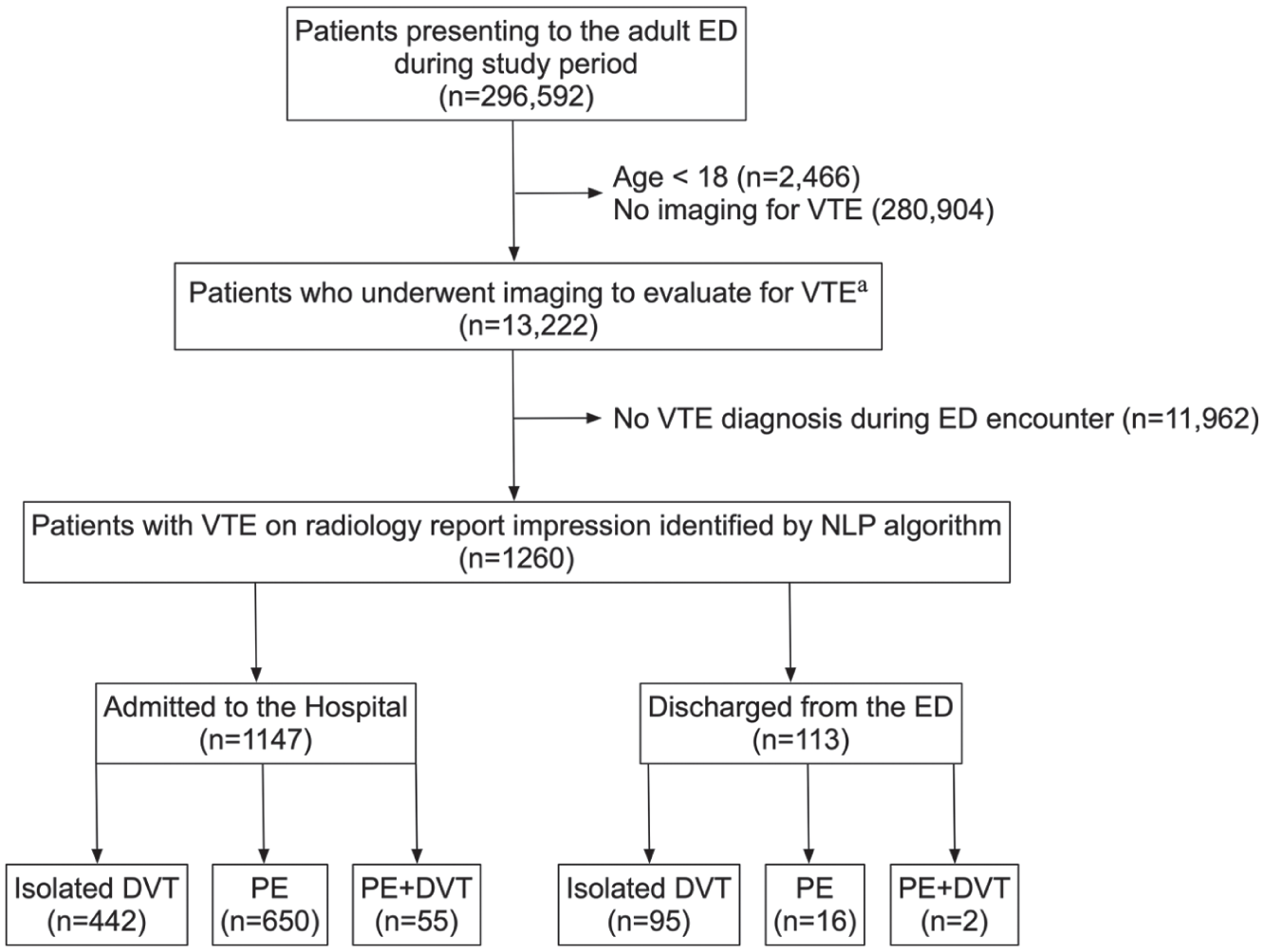
Patient flow diagram.
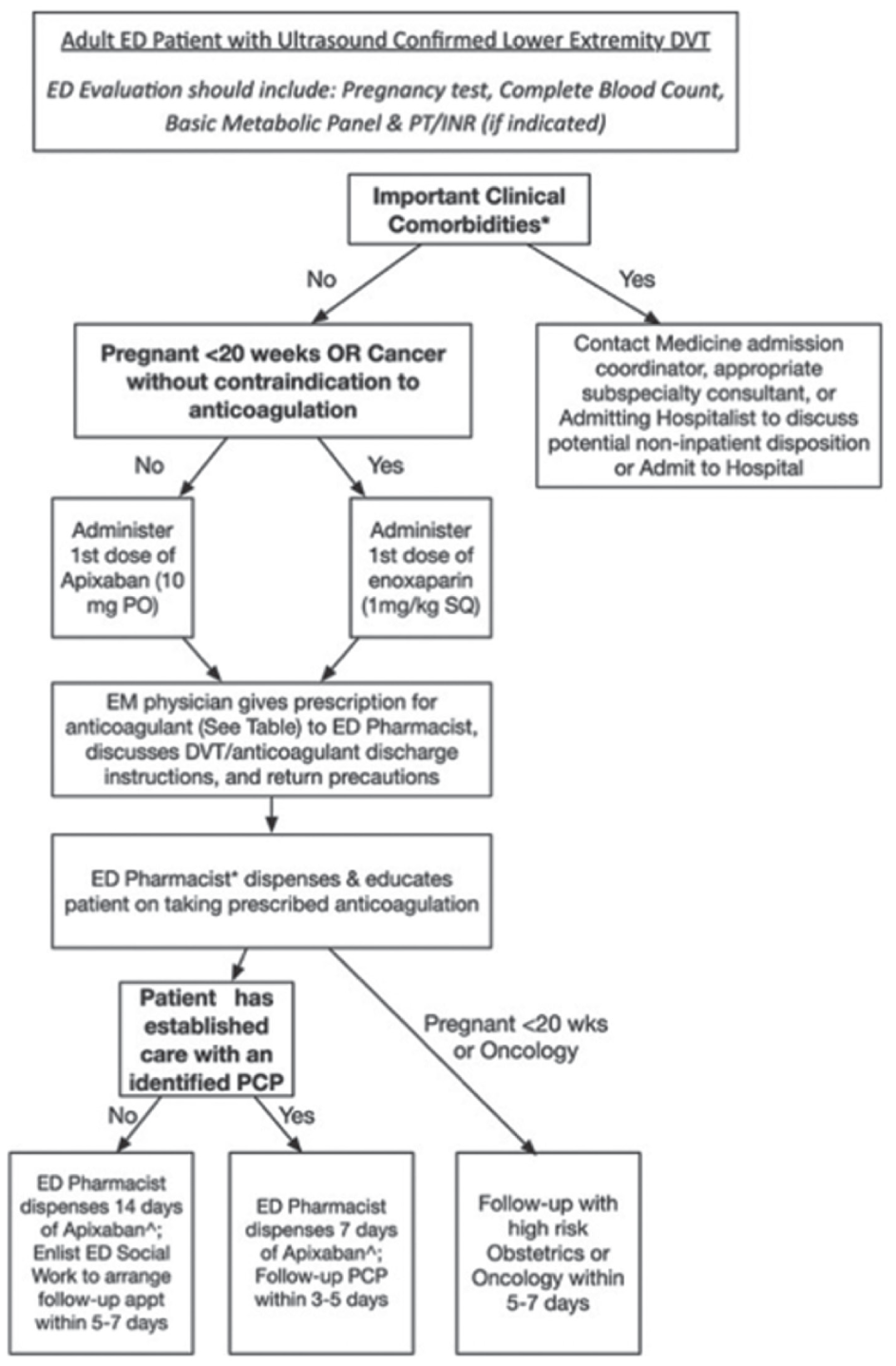
Outpatient deep venous thrombosis pathway. See full pathway details in Supplemental Figure S1.
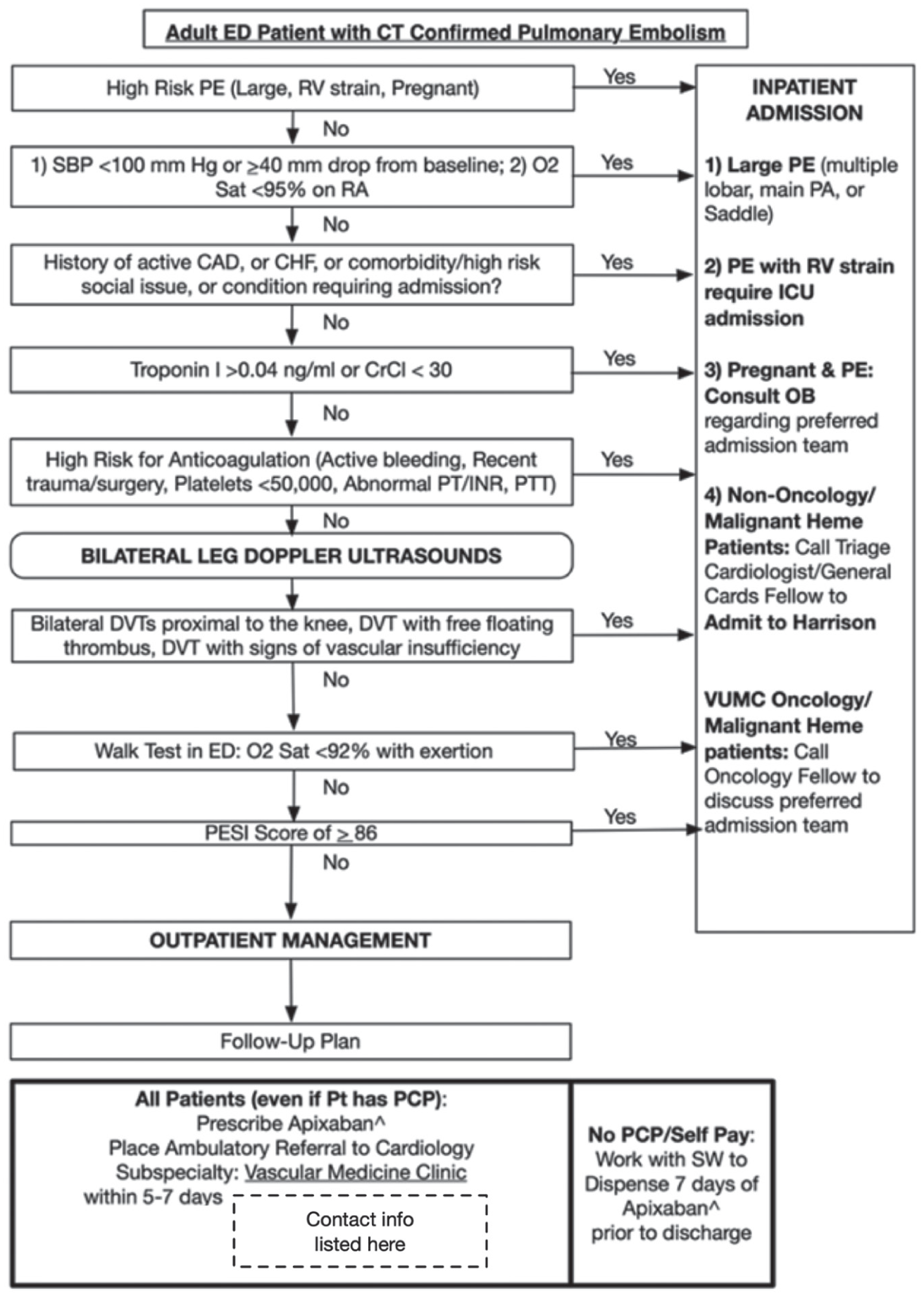
Outpatient pulmonary embolism pathway. See full pathway details in Supplemental Figure S2.
Individual encounter-level pathway use could not be directly measured retrospectively. Additionally, this study was not designed as a formal quality improvement intervention with prospective iterative testing, but rather as a retrospective observational evaluation of a clinically implemented care pathway. The pathway was developed as an institutional clinical operations initiative through collaboration among emergency medicine, vascular medicine, and pharmacy stakeholders, with the goals of standardizing risk stratification, facilitating timely specialty follow-up, and supporting outpatient anticoagulation.
Elixhauser codes were used to define comorbidities. 22 Other VTE risk factors such as recent surgery or trauma, recent hospitalization, prior PE, prior DVT, or hormone use were defined by Current Procedural Terminology (CPT) codes, ICD-9/10 codes, and predefined medication lists. All discrete values, such as vital signs and lab values were captured directly from the electronic health record (EHR). Echocardiographic measures of right heart dysfunction were also directly captured as discrete data elements from consultative cardiac echo reports. A right ventricular/left ventricular (RV/LV) ratio > 1.0 or a tricuspid annular plane systolic excursion (TAPSE) < 16 mm were considered evidence of right ventricular dysfunction. Bleeding events were characterized using ICD-9/10 diagnosis codes and an adaptation of a previously validated algorithm for bleeding-related hospitalization. 23 Diagnosis codes were added to enhance capture of in-hospital bleeding events. Major bleeding was defined by International Society of Thrombosis or Haemostasias (ISTH) 24 criteria and identified by the presence of CPT codes for transfusion of red blood cells or the presence of prespecified ICD-9/10 diagnosis codes for acute bleeding within a 30-day time frame from index ED presentation (supplemental Tables S1–S6). All-cause hospitalizations and ED return visits were captured by medical record extraction indicating an ED visit or hospitalization within a 30-day time frame from the index ED presentation. This study was deemed exempt by our local institutional review board (IRB #200674).
Population
Adults (age ⩾ 18 years) presenting to a quaternary care, academic ED in the Southeastern US were identified via the EHR using an institutional, NLP algorithm trained to identify the presence or absence of PE or DVT by scanning text within radiology report impressions. Imaging modalities scanned included computed tomography angiography (CTA) imaging or ultrasound imaging of the extremities. Prior to record extraction, the algorithm was internally validated and when compared with structured physician chart review was found to have a positive predictive value of 94% and negative predictive value of 99%. A similar algorithm for PE has been published previously. 21 The internal NLP algorithms scanning radiology reports for DVT have not yet been published but exhibit similar test characteristics.
Data collection
All occurrences of qualifying VTE were captured by the NLP algorithm during the index ED visit. Patient demographics, medical history, labs, medications, and outcome variables were extracted from the EHR using qualifying ICD-9/10 codes, CPT codes, and predefined medication lists.
Statistical analysis
Demographic and clinical characteristics were compared before and after pathway initiation using the Wilcoxon rank-sum test and chi-squared tests (or Fisher’s exact tests) for continuous and categorical variables, respectively. Comparisons were stratified by VTE diagnosis of PE (with or without concomitant DVT) versus isolated DVT. VTE severity (based on patient comorbidities and vital signs) and anticoagulant use were compared before and after pathway initiation stratified by disposition from the ED. Aggregated ED discharge rates before and after VTE pathway initiation were calculated. Chi-squared tests were used to compare the ED discharge rate before and after VTE pathway initiation. To examine the independent effect of the VTE pathway on ED disposition (discharge from ED versus hospital admission), a logistic regression analysis was performed with ED disposition as the primary outcome. Using VTE pathway initiation as the main predictor, we adjusted for age, sex, recent hospitalization, prior PE, active malignancy, recent surgery, heart rate (HR), oxygen saturation, and systolic blood pressure (SBP). Interactions between pathway initiation and age as well as VTE diagnosis were evaluated to examine if the impact of the VTE pathway on the outcome of ED disposition varies by age and VTE diagnosis. VTE-related outcomes were calculated and compared before and after pathway initiation in those patients discharged from the ED. Outcomes included ED return visit, hospitalization, or bleeding events (defined as transfusion of blood product or presence of an ICD-9 or ICD-10 code related to bleeding during hospitalization; Tables S1–S6). We also evaluated a composite outcome of these outcomes at 30 days. Although the pathway included facilitated vascular medicine follow-up scheduling, appointment completion and attendance data were not consistently available for retrospective analysis. Kaplan–Meier plots and log-rank tests were performed to evaluate the effect of the ED discharge pathway on return ED visit and rehospitalization at 30 days; however, formal modeling was not feasible due to the limited number of events.
Results
A total of 1260 patients were identified and included in our cohort. There were 575 patients prior to pathway initiation, from July 1, 2014 to June 30, 2016, and 685 patients after pathway initiation, from July 1, 2016 to June 30, 2018. Median age in the overall cohort was 57 years (IQR = 43–68), 49.4% of patients were women, and 21.6% of patients were Black. Within the cohort, 537 (42.6%) patients were diagnosed with an isolated DVT and 723 (57.4%) with PE. Of the 723 patients with PE, 57 (7.9%) had a concomitant DVT diagnosed. Overall, patients with VTE before pathway initiation had a greater proportion of hypertension and exogenous estrogen use, whereas patients after pathway initiation had a greater proportion of recent hospitalization, prior PE, and prior myocardial infarction (Table 1).
Characteristics of patients diagnosed with venous thromboembolism stratified by 2 years pre and post outpatient care pathway implementation.
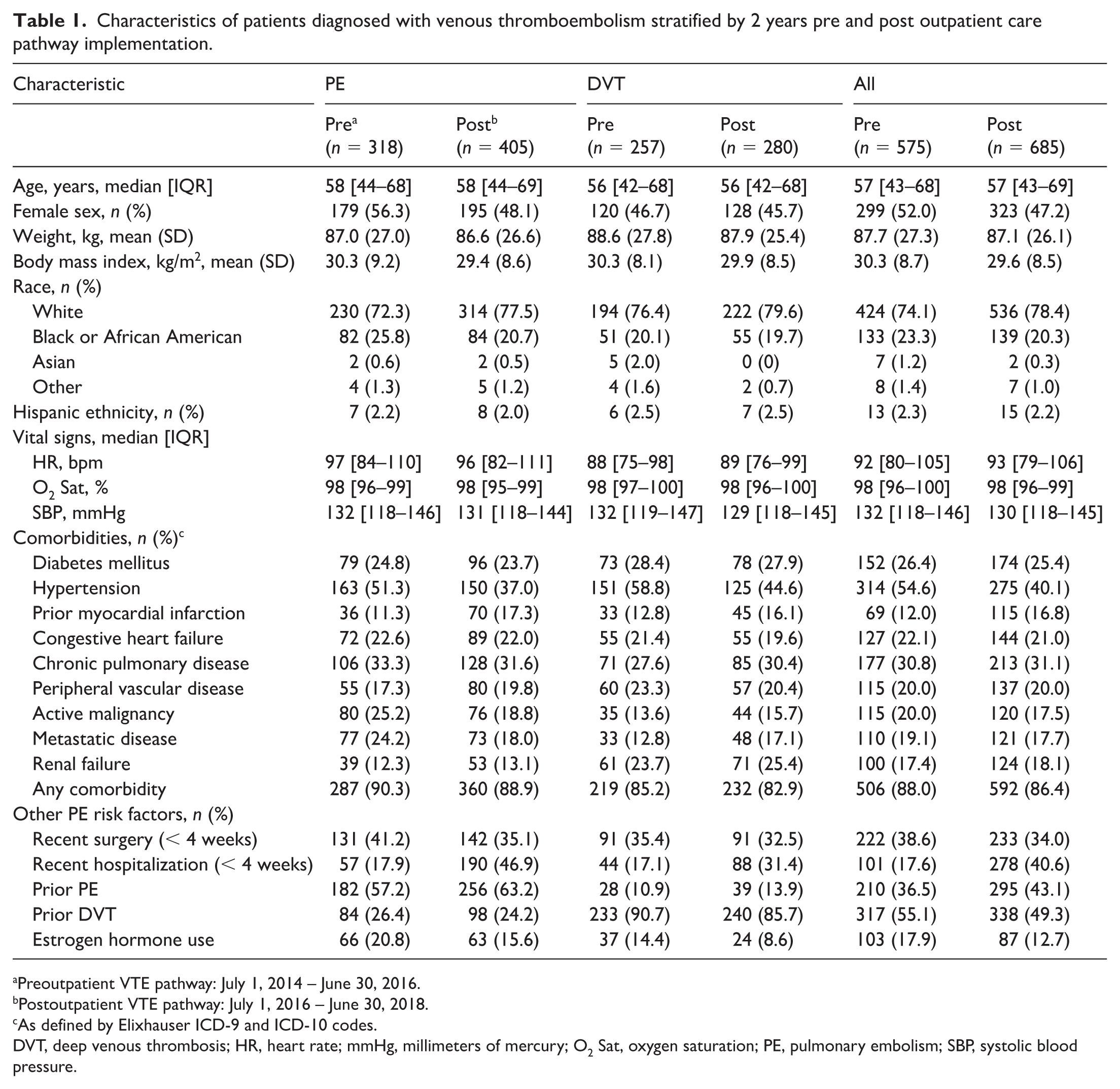
Preoutpatient VTE pathway: July 1, 2014 – June 30, 2016.
Postoutpatient VTE pathway: July 1, 2016 – June 30, 2018.
As defined by Elixhauser ICD-9 and ICD-10 codes.
DVT, deep venous thrombosis; HR, heart rate; mmHg, millimeters of mercury; O2 Sat, oxygen saturation; PE, pulmonary embolism; SBP, systolic blood pressure.
Pre- and postpathway initiation characteristics and disposition decisions
Isolated deep venous thrombosis (DVT)
There were 257 (44.7%) and 280 (40.8%) patients diagnosed with isolated DVT in the pre- and postperiod, respectively. There were no significant differences in age, race, ethnicity, ED vital signs, and active malignancy between the pre- and postpathway cohorts. Patients before pathway initiation had a greater proportion of hypertension and estrogen medication use, whereas patients after pathway initiation had a greater proportion of recent hospitalization (17.1% vs 31.4%, p < 0.001). Of the patients with isolated DVT, 95 patients (17.7%) were discharged from the ED during the 4-year study period: 22.6% prior to pathway initiation and 13.2% after pathway initiation (p = 0.005) (Table 2).
Venous thromboembolism (VTE) severity and anticoagulation in patients pre and post outpatient care pathway implementation.
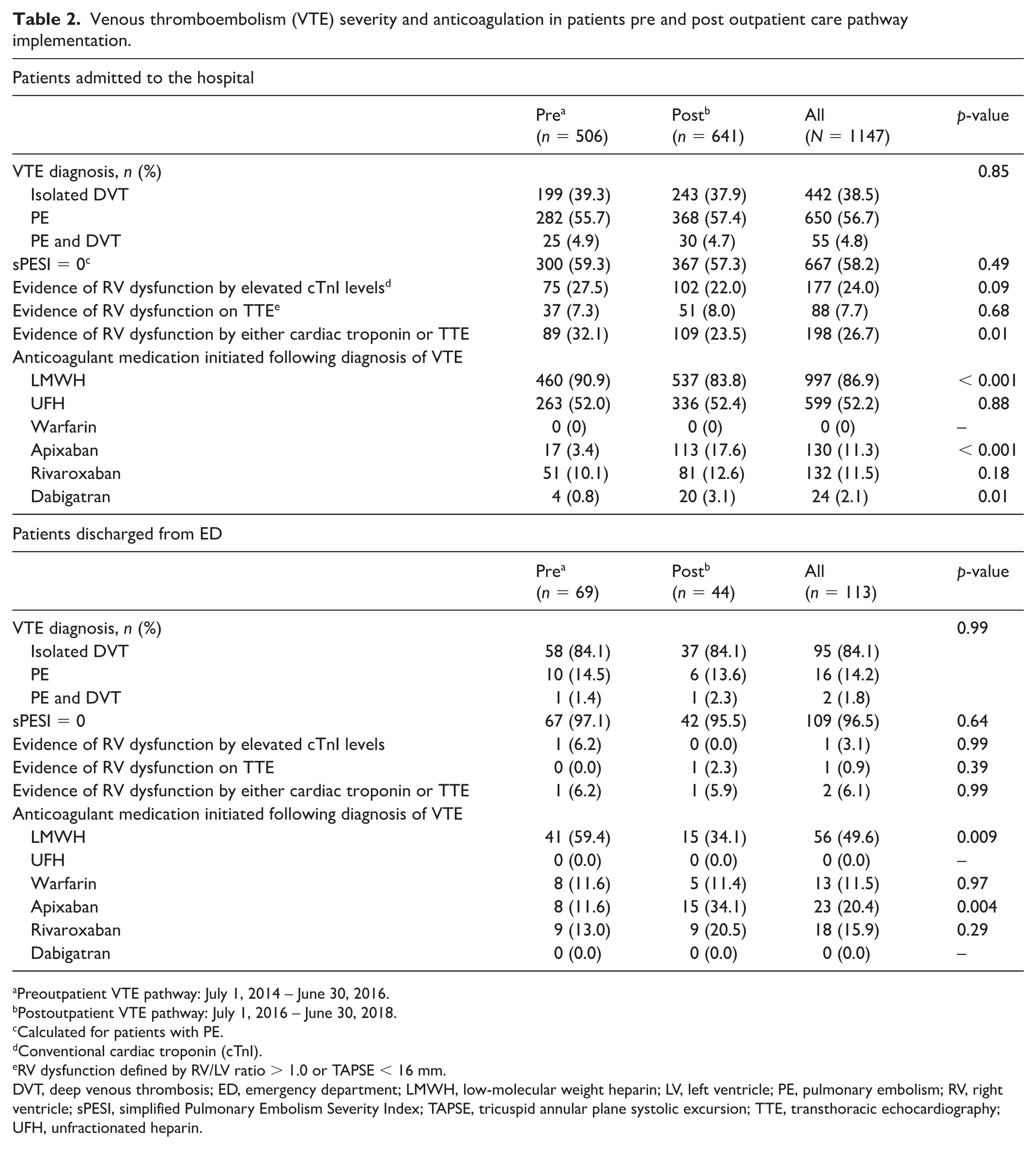
Preoutpatient VTE pathway: July 1, 2014 – June 30, 2016.
Postoutpatient VTE pathway: July 1, 2016 – June 30, 2018.
Calculated for patients with PE.
Conventional cardiac troponin (cTnI).
RV dysfunction defined by RV/LV ratio > 1.0 or TAPSE < 16 mm.
DVT, deep venous thrombosis; ED, emergency department; LMWH, low-molecular weight heparin; LV, left ventricle; PE, pulmonary embolism; RV, right ventricle; sPESI, simplified Pulmonary Embolism Severity Index; TAPSE, tricuspid annular plane systolic excursion; TTE, transthoracic echocardiography; UFH, unfractionated heparin.
Pulmonary embolism (PE)
There were 318 (55.3%) and 405 (59.1%) patients diagnosed with PE in the pre- and postpathway period, respectively. A minority of patients with PE (7.9%) had a concurrent diagnosis of DVT. Like the subgroup with isolated DVT, comparisons across pre- and postpathway PE groups were similar with respect to age, race, ethnicity, ED vital signs, and active malignancy. Patients before pathway initiation had a greater proportion of hypertension. Patients after pathway initiation had a greater proportion of men, prior myocardial infarction, and recent hospitalization. Of the patients with PE, 18 (2.5%) were discharged from the ED during the 4-year study period: 11 (3.5%) prior to pathway initiation and seven (1.7%) after pathway initiation (p = 0.14). Of the patients discharged from the ED with a PE, 96.5% had a retrospectively calculated simplified PESI (sPESI) of 0. Two patients had evidence of RV dysfunction (Table 2).
ED discharge of patients with VTE
Overall, the discharge rate in the postpathway period was lower than in the prepathway period (6.4% vs 12.0%, p < 0.001). In our adjusted analysis, there was a trend toward decreased odds of discharge in the postpathway period when compared to the prepathway period (aOR 0.74, 95% CI: 0.48 to 1.13) for all patients with VTE. Older age, recent hospitalization, prior PE, and higher HR were associated with significantly lower odds of ED discharge. The proportions of patients with prior PE and recent hospitalization were significantly higher in the postpathway period. An increased SBP was associated with significantly higher odds of ED discharge (Figure 4).
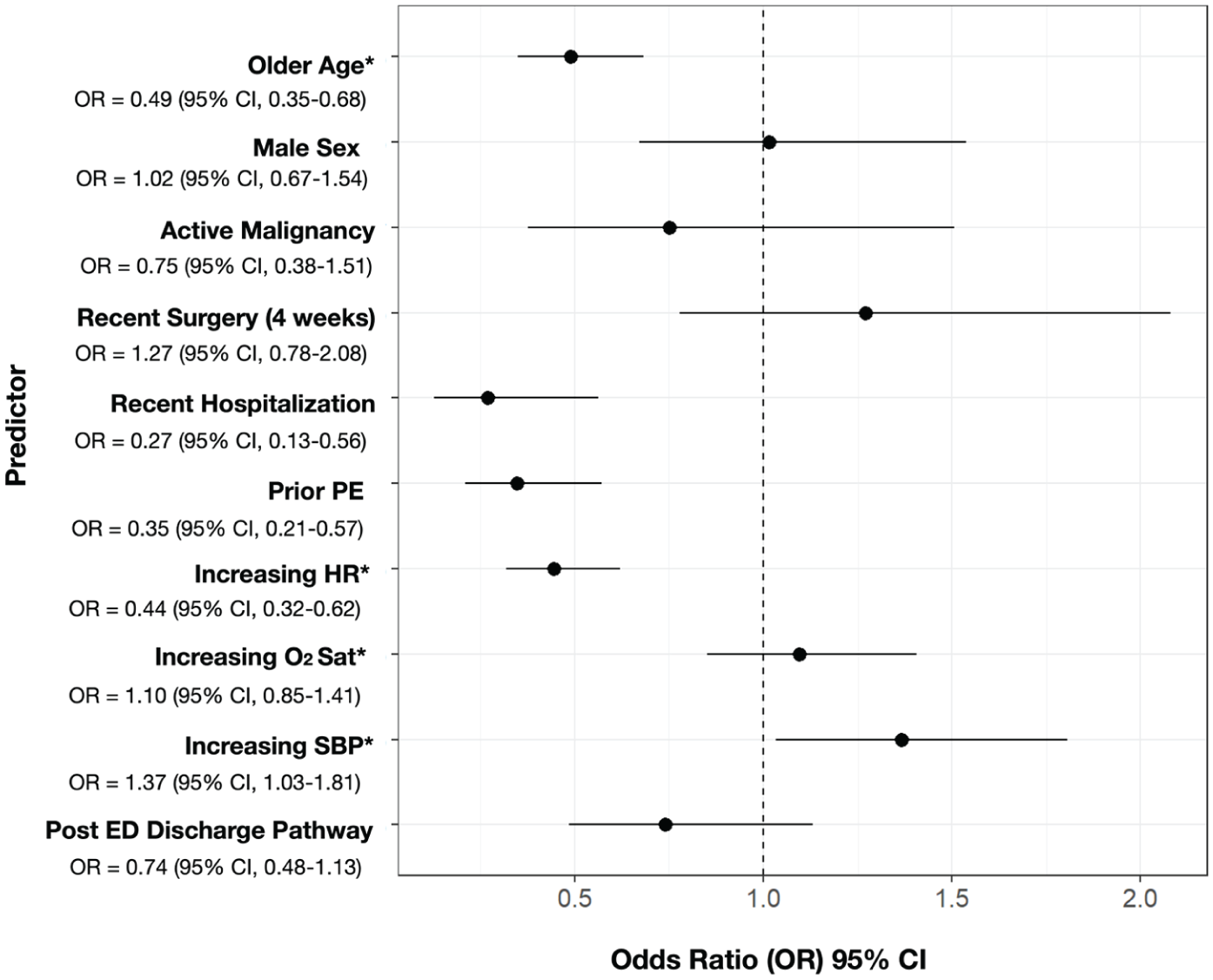
Odds ratio of emergency department (ED) discharge by age, sex, active malignancy, recent surgery, recent hospitalization, prior PE, HR, oxygen saturation (sat), SBP, and ED discharge pathway.
Outpatient anticoagulation
Of the 113 patients discharged from the ED during the study period, 56 patients (49.6%) were discharged on low-molecular weight heparin (LMWH), 23 (20.4%) were discharged on apixaban, 18 (15.9%) were discharged on rivaroxaban, and 13 (11.5%) were continued on their home warfarin (Table 2). More patients in the postpathway period were prescribed apixaban (34.1% vs 11.6%, p < 0.05) and fewer patients were prescribed LMWH (34.1 vs 59.4, p < 0.05). No patients were discharged from the ED on dabigatran or edoxaban.
Death, return to the ED, hospitalizations, and bleeding events at 30 days
Of the 113 patients discharged from the ED, 18.6% had an ED return, 5.3% were hospitalized, and 8.8% had a bleeding event at 30 days. There were no deaths recorded in patients who returned to the ED or were hospitalized in the 30-day period following the index ED visit. Compared to the prepathway period, there were no differences observed in the composite outcome of return visits to the ED, hospitalizations, or bleeding events during the postpathway period (p = 0.96) (Table 3). Formal Cox regression modeling was limited due to the small number of events, but Kaplan–Meier plots and log-rank tests showed no significant difference in the individual or composite outcomes between the pre- and postpathway groups.
Venous thromboembolism (VTE)-related outcomes at 30 days in patients discharged from the emergency department.
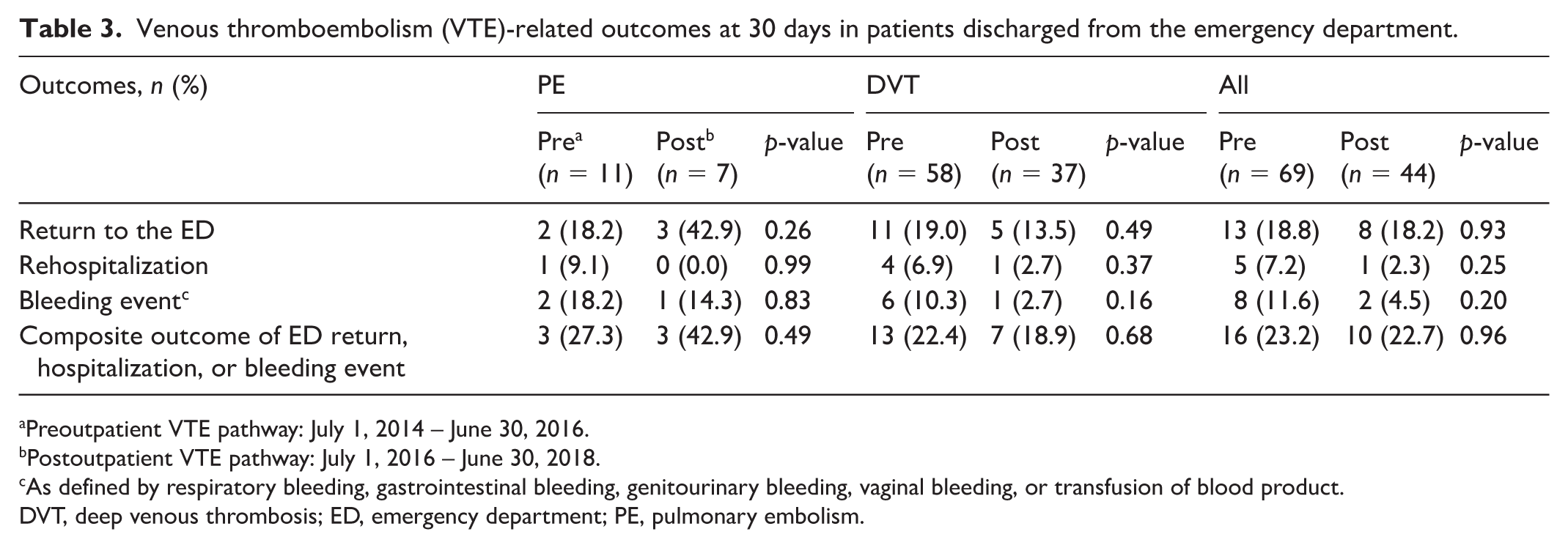
Preoutpatient VTE pathway: July 1, 2014 – June 30, 2016.
Postoutpatient VTE pathway: July 1, 2016 – June 30, 2018.
As defined by respiratory bleeding, gastrointestinal bleeding, genitourinary bleeding, vaginal bleeding, or transfusion of blood product.
DVT, deep venous thrombosis; ED, emergency department; PE, pulmonary embolism.
Discussion
We describe characteristics of a patient cohort who a quaternary care ED for VTE over a 4-year period. We report three important findings. First, patients in the postpathway period were a more medically complex population with more recent hospitalizations and a higher prevalence of prior PE when compared to the prepathway period. Older age, recent hospitalization, prior PE, and higher HR were all associated with significantly lower odds of ED discharge. The higher proportions of patients with a recent hospitalization and prior PE confounded our results and contributed to the lower proportion of low-risk patients with VTE discharged from the ED in the postpathway period. Second, there was a significant increase in the proportion of patients who received a DOAC and a decrease in the proportion of patients who received LMWH in the postpathway period, consistent with evolving national practice patterns and pathway guidance. Third, ED discharges in the postpathway period did not result in a significant increase in ED return visits, hospitalizations, or bleeding events at 30 days from discharge when compared to the prepathway period.
Overall, we demonstrate a continued unmet need to safely increase the proportion of patients discharged from the ED with VTE. In recent qualitative work by Westafer et al., clinicians reported common barriers to outpatient management of PE centered on beliefs, fever, and local culture. 25 Possible barriers may also include conservative provider practice patterns outside of traditional covariates embedded within clinical decision tools for ED-based risk-stratification. Routine incorporation of tools such as Hestia, PESI, or sPESI may have been more effective than our institutional protocol. 16 The complexity of the outpatient pathway and the inability to ensure adequate medication acquisition by the patients during off hours likely complicated patient selection for discharge. Our initial institutional protocol may have created unintended complexity and appealed to a more conservative management practice. We were unable to directly measure pathway use fidelity, ED length of stay, time-to-discharge, or prescription fill success in this retrospective dataset. In the absence of high-fidelity data, we cannot confirm pathway utilization; however, the requirement for coordinated follow-up scheduling, pharmacist availability, and medication access—particularly during off-hours—likely increased the operational burden of discharge decisions and may have discouraged pathway use. These process measures represent important targets for future prospective pathway redesign and evaluation.
Prior work by Vanni et al. found that when compared to clinical gestalt, both PESI and sPESI identified a lower proportion of candidates for early discharge. 26 Our PE pathway utilized PESI as a tool for risk stratification (Figure 3). However, for analysis purposes, given the complexity of assessing PESI retrospectively, we assessed the sPESI. There was no difference in the proportion of admitted patients with an sPESI of 0 in the postpathway period compared to the prepathway period (59% vs 57%, p = 0.48). Comorbidity profiles were relatively consistent across the pre- and postpathway periods, with the notable exceptions of a larger proportion of patients in the postpathway period with a history of PE (43% vs 37%, p = 0.02) and recent hospitalization (40.6% vs 17.6%, p < 0.001). A revised protocol encouraging the use of sPESI or Hestia criteria in addition to clinical decision making has since been instituted. Further protocol simplification is underway to generate a pathway that is easier to complete and incorporate into ED workflow.
We found that covariates such as age and HR, used in the sPESI clinical decision tool to risk stratify patients for ED discharge, were associated with decreased odds of ED discharge. It also stresses the importance that other covariates, such as recent hospitalization and prior PE, may play in the discharge decision-making process. Despite the growing body of clinical trial and real-world evidence suggesting that outpatient treatment of low-risk PE is both safe and efficacious, there continues to be significant practice variation between the outpatient management of DVT and PE. In the US, approximately half of patients with DVT are discharged from the ED, and fewer than 10% of patients with PE receive outpatient management.27–29 We report similar discharge rates of low-risk PE, with only 2.5% of patients discharged from our ED between 2014 and 2018. Our findings add to the existing literature and support safe discharge in low-risk patients with VTE.30–32 In this analysis, rates of return visits to the ED, hospitalization, and bleeding events were infrequent in the 113 patients discharged from the ED and similar to prior trials.30,32 With the increasing use of DOACs during the pathway period, we observed an expected reduction in the use of LMWH as an outpatient medication between the pre- and postpathway periods (59.4% vs 34.1%, p < 0.001).
There were seven important limitations to this study. First, this retrospective analysis was completed using data from a 2014–2018 patient cohort. Although it predates current practice by 8 years, it highlights limitations in practice patterns 13 years after the earliest trial work, 13 but before the publication of additional trials.30–32 Second, although we identified patients with VTE using an institutional NLP algorithm, respiratory, gastrointestinal, genitourinary, and vaginal bleeding outcomes were identified by both ICD-9 and ICD-10 codes. These bleeding events were not adjudicated to standardized criteria for clinically relevant nonmajor bleeding. 33 Because the analysis spans the years 2014–2018, it includes the timepoint of October 1, 2015, when ICD diagnosis codes were converted from ICD-9 to ICD-10. There is inherent variability in equivalence mapping between ICD-9 and ICD-10. 34 Prior literature has demonstrated inefficiencies of identifying patients using these diagnosis codes.18–20
Third, we included patients based on initial presentation to the ED. We did not exclude patients with VTE of undetermined chronicity, or those with the possible incidental findings of VTE. The greater number of patients with PE in the postpathway period may have resulted in a greater conflation of new versus chronic PE. Additionally, the inclusion of patients with chronic or incidentally discovered VTE likely biased discharge rates downward, as these patients may have been less appropriate ED discharge candidates. Fourth, because pathway eligibility criteria were not fully captured as discrete structured EHR variables, we could not reliably reconstruct pathway eligibility status for all encounters and, therefore, could not formally evaluate concordance between pathway eligibility and ED disposition. Although we could not reconstruct full pathway eligibility, among admitted patients with PE, nearly 60% had an sPESI of 0, suggesting that a substantial proportion of patients meeting physiologic low-risk criteria were nevertheless admitted. The sPESI clinical decision tool was applied retrospectively to identify patients with PE at high risk for 30-day mortality, yet this tool was derived and validated to be used in a prospective fashion. 35 Covariates within the sPESI include history of cancer and history of chronic cardiopulmonary disease, and our use may have been able to uncover components not easily available during acute presentation. Using ICD codes for both of these diagnoses is associated with the limitations noted above.
Fifth, decisions to admit or discharge are not limited to the presence or absence of VTE. Although we accounted for this in our modeling, patients within the cohort may have been admitted for unrelated reasons pertaining to new or existing comorbidities. This may explain the higher postpathway hospital admission rates, where a significantly higher proportion of patients had a recent hospitalization. Sixth, unmeasured temporal confounders may have also influenced case mix and disposition decisions, including changes in CTA utilization and diagnostic thresholds, increased detection of smaller or incidental PE, and coding differences associated with the ICD-9 to ICD-10 transition. Further, we were unable to measure provider- and system-level operational factors such as ED crowding, time of day, pharmacist availability, and real-time follow-up capacity, all of which likely influence pathway uptake and discharge decisions. Finally, because annual discharge counts were small, we did not perform formal year-over-year, quarter-to-quarter, or month-to-month modeling (i.e., interrupted time series (ITS) analysis). Secular trends in anticoagulation practice and outpatient management may, therefore, partially account for observed differences between study periods.
Conclusion
We observed an increased proportion of patients with recent hospitalizations and prior PE in the postpathway period. Discharge of low-risk patients with VTE trended toward fewer patients in the postpathway period, where these characteristics were both more frequent and associated with lower odds of discharge. The detailed pathway may have also contributed to fewer discharges of patients with VTE. There were no significant increases in ED returnd, hospitalizations, or bleeding events following pathway initiation.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X261434829 – Supplemental material for Initiation of an emergency department discharge pathway for low-risk patients with venous thromboembolism: Factors impact real-world practice
Supplemental material, sj-docx-1-vmj-10.1177_1358863X261434829 for Initiation of an emergency department discharge pathway for low-risk patients with venous thromboembolism: Factors impact real-world practice by William B Stubblefield, James Barclay, Jesse O Wrenn, Doug Conway, Scott Nelson, Quinn S Wells, Dario Giuse, Zhao Zuo, Alexandra M Baird, Tyler Barrett, Shi Huang, Karen Beauchamp, Alan B Storrow, Sean P Collins and Joshua A Beckman in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr Wrenn reports grant research support from the National Institutes of Health (NIH) / National Heart, Lung, and Blood Institute (NHLBI). Dr Wells reports consulting for Novo Nordisk and Nashville Biosciences; grant support from NIH and American Heart Association. Ms Beauchamp was employed at Bristol Myers Squibb-Pfizer (BMS) at the time this work was conducted. Dr Storrow reports grant research support from NIH/NHLBI, Patient-Centered Outcomes Research Institute (PCORI), and Agency for Healthcare Research and Quality (AHRQ). Dr Collins receives grant research support from the NIH/NHLBI, PCORI, BMS, and Department of Defence; consultant support/other from Reprieve Cardiovascular, Tosoh, Prenosis, Abbott, and Corteria. Dr Beckman reports consulting for Novartis, JanOne, Merck, Medtronic, Mingsight, and Tourmaline; grant support from NHLBI, AHA, and BMS. The remaining authors have no conflicting interests.
Funding
Bristol Myers Squibb-Pfizer (BMS) provided funding support for study execution and data analysis. Study design, interpretation, data analysis, and manuscript preparation were done independently by the investigator group. This work was also funded by NIH/NHLBI grant K12HL133117 (Dr. Stubblefield). All statements in this report, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of the funders.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.