
Abstract
Background:
Venous stent preclinical testing typically uses large animal models. We created two models of infrarenal inferior vena cava (IVC) stenting to study patency, flow rate, wall shear stress, and endothelial coverage over the stents in a microsurgery rodent model.
Methods:
In Group 1, Sprague-Dawley rats underwent IVC stenting. Patency was measured by ultrasonography immediately postoperatively (POD-0) and at postoperative day 1 (POD-1). Stents underwent histological analysis up to 21 days postimplantation. Group 2 stented rats received periprocedural anticoagulation (enoxaparin 6 mg/kg SC) and were harvested to evaluate stent coverage using scanning electron microscopy (SEM). En face immunofluorescence (IF) staining was performed in Group 3. Human samples from stent occlusions were collected in the endovascular suite and compared with the animal histological findings.
Results:
In Group 1, 65% of the stented animals (13/20) were patent POD-0, increasing to 85% (17/20) by POD-1. Histologically, in-stent restenosis (ISR) was 6.2 ± 3.8%, and residual thrombosis (RT) was 32.01 ± 23.12% of the IVC total luminal stent area (LSA). These animals’ pathological processes are similar to those in humans. The mean IVC vein wall thickness (VWT) was 80.18 ± 13.14 μm. In Group 2, all animals were patent (21/21) postimplantation and remained patent in POD-1. IF demonstrated stent coverage with CD31+ endothelial cells. Total stent endothelialization by SEM reached 69.53 ± 14.84% at 7 days and increased to 91.51 ± 11.23% at 21 days.
Conclusion:
Quantifying rat venous stent patency and endothelialization via histology and microscopy revealed complete patency with anticoagulation and pathological occlusions (RT, ISR) when withholding anticoagulation. This rodent model will facilitate the preclinical testing of future venous stents.
Keywords
Background
Venous stenting procedures in the United States have increased significantly, with over 69,500 stents implanted from 2005 to 2025.1,2 The approval of the first dedicated venous stent by the US Food and Drug Administration (FDA) in 2019, along with ongoing technological progress and increased clinical awareness, has driven this rapid growth.3,4 Projections show that this trend will continue, possibly reaching 21,300 procedures annually by 2035 as venous thromboembolism (VTE) rates increase, with yearly costs between US$7 and US$10 billion.5–7 Despite advances in technology, stent complication rates remain significant. In a recent meta-analysis of 17 trials, venous stents achieved a primary patency of approximately 80% at 12 months. 8
Venous-specific pathological processes lead to stent complications, including in-stent restenosis (ISR), arising from diffuse intimal thickening (DIT), and thrombus formation. Modifiable factors that can be manipulated to improve outcomes include the technical performance of the procedure and stent design characteristics that affect flexibility, radial strength, and biocompatibility.9–15 Antithrombotic therapy is the mainstay of therapy for maintenance of arterial stent patency; however, there is no standard agent, dose, or duration that has been agreed upon as standard of care to prevent the progression of these pathological processes in veins. 16 Arterial stents have benefited from innovations such as gene and protein cargo delivery, peptide modifications, drug-eluting coatings, and novel biomaterials, including resorbable scaffolds, which promote endothelialization and reduce neointimal hyperplasia to improve clinical outcomes.17–23 However, these features are not available in venous stents, and the currently available preclinical models to test such features are expensive and require the use of large animals.
To address this gap, we developed a novel rat model of venous stenting that allows detailed assessment of venous stent performance using ultrasound, histology, scanning electron microscopy (SEM), and immunofluorescence (IF) with or without anticoagulation therapy, to better understand patency and stent endothelialization.
Methods
This research followed University of Michigan Institutional Animal Care and Use Committee (IACUC) policies, US Government Principles for the Use and Care of Vertebrate Animals in Testing, Research, and Training, and ARRIVE guidelines 2.0. 24 Consent was waived by the institutional review board as the samples were part of routine clinical management. Human iliofemoral deep vein thrombosis (DVT) samples were obtained via biopsy during open or endovenous treatment.
Study design
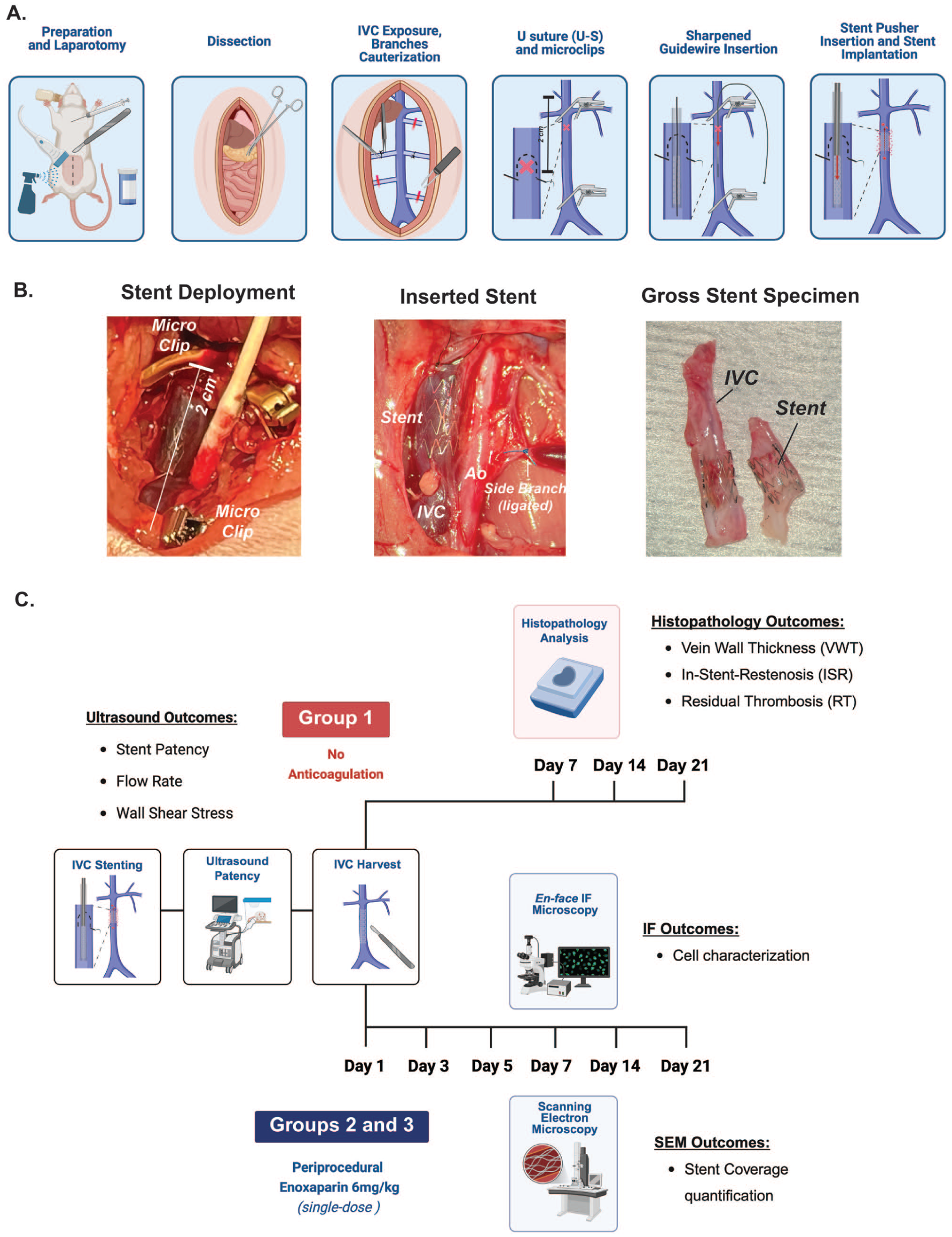
Sample size was defined a priori utilizing power calculations, for an alpha = 0.05 and power of 80%, allocating n ⩾ 3 animals per group per condition as specified in the supplemental data. Sprague-Dawley rats (Charles River Breeding Labs, USA) (n = 54) were assigned into Group 1 (n = 22), which included surgical shams (n = 1), a stasis thrombotic model (n = 1), and inferior vena cava (IVC) stenting (n = 20) with no anticoagulation therapy, with endpoints at 7, 14, and 21 days (n = 6–8), evaluating postoperative patency, flow rate, and wall shear stress by ultrasonography and histological characterization of the vein wall. Group 2 (n = 25) included surgical shams (n = 2) and stented rats with endpoints at 1, 3, 5, 7, 14, and 21 days (n = 3–4) to evaluate endothelial coverage using SEM. Group 3 (n = 7) included surgical shams (n = 2) and stented rats with endpoints at 1 (n = 1) and 21 days (n = 4), who received anticoagulation, to evaluate cell characterization using en face IF staining. Human histological samples from stent thrombosis were collected from the endovascular suite (n = 3) and compared with animal samples in Group 1.
Animal procedures
Adult male Sprague-Dawley rats, 8–10 weeks old, were anesthetized with 3% isoflurane. Eye lube (SKU-065441; Optixcare, USA) was used to prevent ocular damage. Preprocedure, the anteroposterior (AP) infrarenal IVC diameter was measured by ultrasound (ACUSON Antares; Siemens, USA) on B-mode to guarantee adequate sizing of the stent with an overstretch of the vein wall of approximately 20%, correlated with accepted human sizing. 25 Preoperatively, the abdomen was cleaned aseptically with gauze soaked in chlorhexidine scrub and solution (17030-003-16; Vetoquinol, USA). Buprenorphine 0.65 mg/kg (SKU-099114; Ethiqa XR, 1.3 mg/mL; Fidelis Animal Health, USA) was administered subcutaneously for analgesia. The abdomen of the rat was covered with ethylene oxide-exposed sterile Press’ n Seal (SKU PSS-140; Glad Products Co., USA). 26
Using a surgical microscope (M690; Leica, USA), through a midline laparotomy, the abdominal contents were reflected carefully, displacing organs on the right side, and covered with sterile saline-moistened gauze (Figure 1). The infrarenal IVC was carefully dissected from the aorta. The IVC posterior venous branches were cauterized with a low-temperature fine-tip Bovie cautery (AA00; Symmetry Surgical Inc., USA), and side branches were ligated using 7-0 DemeLENE (PM197011F13M; DemeTech, USA). Two 12 × 2.25-mm Heifetz microclips were temporarily placed (3795-28; SCANLAN, USA) on the infrarenal IVC and proximal to the IVC bifurcation approximately 1.5 cm apart. An 8-0 DemeLON (NL868007C7P; DemeTech) U-stitch was placed in the proximal IVC. A stent sheath was inserted retrograde through the U-stitch into the IVC and advanced to deploy a venous self-expanding 3 × 5-mm bare metal nitinol stent with a stent introducer. After the stent deployment and removal of the stent sheath, the U-stitch was tightened for hemostasis, and the microclips were removed (Figure 1). Muscle and skin layers were closed with continuous 3-0 DemeCRYL sutures (G183019F4P; DemeTech). After the procedure, the animals were monitored in a recovery cage with a heat source (a heating lamp) until they were fully recovered.
Duplex ultrasound
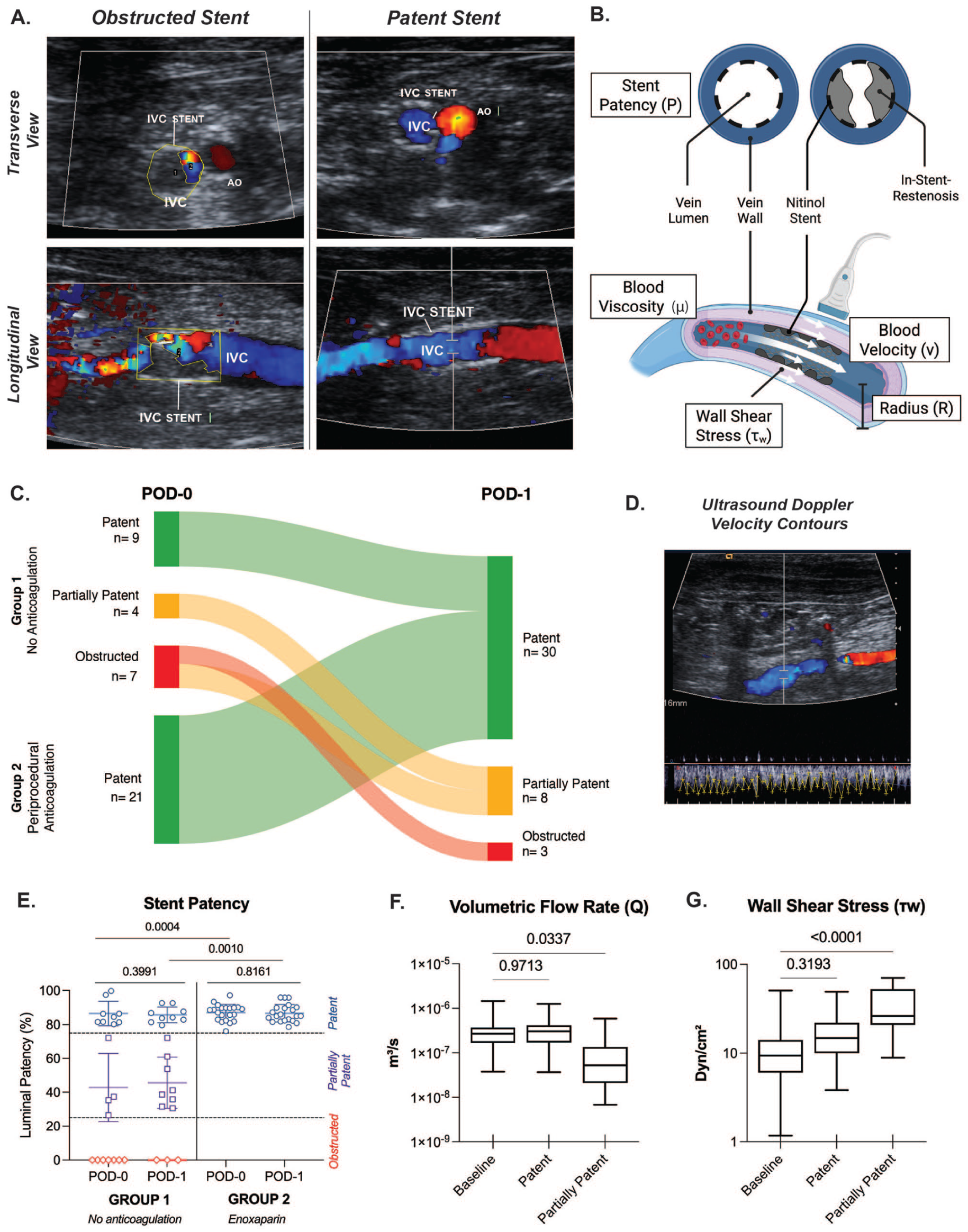
After closing the abdomen (POD-0) and on POD-1, color/pulsed-wave Doppler was performed to evaluate stent patency by assessing venous flow with a 10-MHz probe. The patency was determined as the IVC stent area with flow divided by the total IVC area. We characterized the mid-portion of the stent as patent (defined as > 75% of the intraluminal area visualized with spontaneous flow via color duplex), partially patent (< 75% and > 25%), or obstructed (< 25%). The area of the IVC with flow was measured using IVC longitudinal and transverse 2D images on ImageJ Fiji software (https://imagej.net/software/fiji/, National Institutes of Health, USA). To calculate the murine wall shear stress, we quantify the ultrasound spectral Doppler velocity contours from the IVC using the open‑source PlotDigitizer software (https://plotdigitizer.sourceforge.net, PORBITAL, USA). The digitized contours represent the peak velocities within the Doppler spectrum. Under the assumption of a parabolic velocity profile, mean velocities were calculated as one half of the maximum velocity. The time-averaged mean velocity across the contour was then used in Equation (1) to calculate the average flow rate, assuming a circular vessel cross-section to estimate the vessel area:

where

where
Histopathology
En bloc human biopsy samples were formalin-fixed for 8 hours and paraffin-embedded, sectioned, and slide-stained with hematoxylin & eosin (H&E) and Masson trichrome at the Orthopaedic Research Laboratories (ORL) Histology Core at the University of Michigan. The slides were classified by a cardiovascular pathologist according to previously defined pathological features: fresh thrombus, organizing thrombus, old thrombus, or DIT. 15 Images were taken using a brightfield microscope (Eclipse E400; Nikon, USA) with a Digital Sight camera (DS-Ri1; Nikon) and controller (DS-U4; Nikon).
Stents were harvested after 1, 3, 5, 7, 14, and 21 days of stent implantation. The IVC was carefully dissected from its proximal and distal ends, separated from the aorta, removed, and washed in sterile saline (PCS1650; Medline, USA) for 1 × 5 minutes. Rat IVC stent specimens in Group 1 were fixed in 10% neutral buffered formalin (MCHEM110; Medline) for 24 hours and subsequently processed for plastic embedding at the ORL Histology Core.30,31 Blocks were cut in half transversely and then sectioned at a thickness of 5 μm using a rotary microtome with a 55° angle tungsten carbide blade for plastic-embedded tissues. 32 H&E and trichrome stained slides were used to quantify vein wall thickness (VWT), ISR, and residual thrombosis (RT).33,34 Sham rats were housed and treated under the same conditions as the stented rats, but just underwent laparotomy with retroperitoneal dissection, without IVC stenting. The thrombotic stasis model was performed as described by Varma et al. 35 The mean VWT was quantified by taking 12 measurements from the intima to the adventitia per sample.36,37 In-stent restenosis was calculated as ISR% = residual lumen area/area of stent wire border. RT was calculated as RT% = thrombus area/total IVC lumen. The stent area (SA) percentage was calculated as SA% = stent struts area/total imaged IVC area.
Scanning electron microscopy (SEM)
Harvested IVCs from Group 2 were fixed in a 10% formalin solution for 24 hours, followed by a 2-hour fixation in 5% glutaraldehyde and 2% paraformaldehyde solution (16536-06; Electron Microscopy Sciences, USA), ensuring minimal disturbance to the endothelial cells, followed by a phosphate-buffered saline (PBS) (10010049; Gibco, USA) wash to remove calcium deposits, 2 × 5 minutes. The samples were fixed in 1% osmium tetroxide (75632-10ML; Sigma-Aldrich, USA) for 60 minutes, followed by a series of ethanol (2701; Decon Laboratories, Inc., USA) washes for dehydration: 1 × 15 minutes each at 50%, 60%, 70%, 80%, 90%, 95% concentration, and 2 × 15 minutes at 100% concentration. 38 The IVCs containing the stents were longitudinally sectioned, creating two half-cylinders. For critical point drying, the conditions used were Tc: 23°C, Pc: 1.0 bar, and CO2 IN: medium for 4 hours (EM CPD300; Leica) at the University of Michigan Microscopy Core. Samples were then mounted on SEM holders (RS-MN-12-002920-3; Rave Scientific, USA), coated with a thin 10-nm layer of gold, and imaged using the scanning electron microscope (EVO15; Zeiss, USA) on the same day to maintain imaging quality. After SEM processing, the image quality was assessed in the two IVC sections for analysis per animal. Images were taken at 60× to 1000× magnification, with a scan speed of 6, and an electron high tension (EHT) of 5 kV. 39 Stent endothelial coverage (SEC) was calculated as the percentage of endothelial-covered area relative to the total stent area in 60× images. SEM images were analyzed using QuPath 0.6.0 software (https://qupath.github.io/, Queen’s University Belfast, UK).
En face immunofluorescence (IF) staining
For en face IF microscopy, the stented vessels in Group 3 were fixed with 4% formaldehyde solution (28908; ThermoFisher, USA) in a HEPES buffer (25-060-CI; Corning, USA) and permeabilized with 0.2% Triton X-100 (T9284; Sigma-Aldrich) in PBS (10010049; Gibco, USA).40,41 After washing with PBS for 5 minutes, the slides were blocked with 0.2% bovine serum albumin (BSA) (B4287-25G; Sigma-Aldrich) in PBS. The stented vessels were incubated for 2 hours in a PBS-BSA solution containing primary antibodies at 1/100 dilution: CD31-647 conjugate (34624S; Cell Signaling Technology [CST], USA) and αSMA-594 conjugate (36110S; CST). After double staining with 4′,6-diamidino-2-phenylindole (DAPI), the stented vessels were placed on Superfrost Plus microscope slides (1255015; Fisher Scientific, USA), mounted using Prolong Gold antifade reagent with DAPI (P36931; Fisher Scientific, USA), and coverslipped under micro-coverglass (72204-04;Electron Microscopy Sciences). Images were acquired and processed using an automated fluorescence microscope (BZ-X800E; Keyence Corp., USA) from the University of Michigan Frankel Cardiovascular Center. High-precision image stitching and Z-stacking for multilayer capture features were used to obtain full-focused images and advanced 3D analyses of the stent structures.
Statistical analysis
Statistical analysis was performed in Prism 10.6.0 software (https://www.graphpad.com, GraphPad). Statistical significance between groups was determined using Brown-Forsythe and Welch analysis of variance (ANOVA) tests with multiple comparison corrections or unpaired Student’s t-test with Welch correction. The presented quantifications were measured blindly by two separate individuals. Results were considered significant when p ⩽ 0.05. Data are presented as mean ± SD.
Results
Preprocedure, the infrarenal IVC diameters by ultrasound were 2.59 mm (± 0.14 mm). The mean rat weight was 521.80 ± 128 g. All the implanted stents were deployed in the infrarenal IVC. All the animals survived until their predefined time.
Ultrasound postimplantation and postoperative patency
In Group 1, the intraluminal stent area with flow was measured 15 minutes after skin closure at postimplantation (POD-0), with 65% (13/20) of the stented animals patent (patency > 75%: 9/20, patency < 75%: 4/20), and 35% (7/20) obstructed. After 24 hours, 85% of the stents (17/20) were patent (patency > 75%: 9/20, patency < 75%: 8/20) on postoperative day 1 (POD-1), with partial recanalization observed in four of seven obstructed stents (Figure 2A). The mean stent patency at POD-0 was 44.51 ± 40.54%, increasing at POD-1 to 56.82 ± 32.42%. Group 2, which received enoxaparin 6 mg/kg SC postprocedure, had complete patency in all animals (21/21) at both POD-0 (87.01 ± 4.83%) and POD-1 (86.67 ± 5.12%). There was a significant difference in the patency between Groups 1 and 2 at POD-0 (p = 0.0004) and at POD-1 (p = 0.0010) (Figure 2E). The mean volumetric flow rate at baseline (preoperative) was 3.48 × 10–7 ± 3.19 × 10–7 m3/s; for the patent stents, it was 3.33 × 10–7 ± 2.52 × 10–7 m3/s; and for the partially patent stents, it was 1.18 × 10–7 ± 1.68 × 10–7 m3/s. No significant differences were found between these groups. The mean wall shear stress at baseline was 12.62 ± 11.82 dyn/cm2, 17.46 ± 10.70 dyn/cm2 for the patent stents, and 34.64 ± 19.68 dyn/cm2 for the partially patent stents. There was a significant increase in the wall shear stress in the partially patent stents compared with the patented stents (p = 0.0011), and when compared to baseline (p ⩽ 0.0001).
Stent histological findings (Group 1)
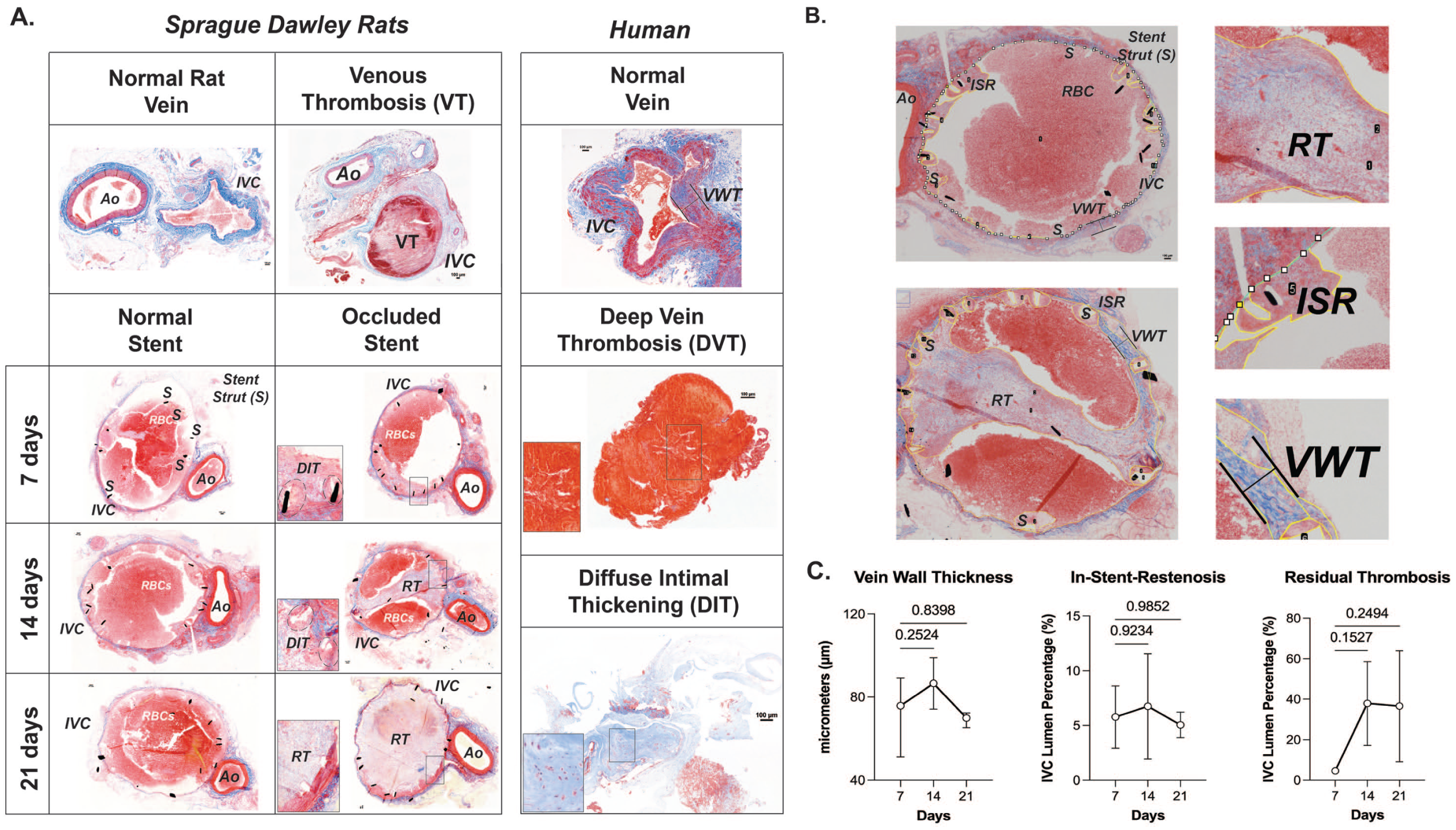
Histological changes in venous cross-sections stained from both Sprague-Dawley rats and humans were reviewed. Both samples showed similar features, including normal veins, DVT, and DIT (Figures 3A and 3B). The IVC generally exhibited a larger diameter compared to the aorta. In the rat model, venous thrombosis (VT) was identified on days 7, 14, and 21 after stent implantation without anticoagulation. Ultrasound assessment confirmed stent occlusion with reduced venous flow. 25 In Group 1, the mean VWT was 80.18 ± 13.14 µm, with no significant differences between days 7 (75.75 ± 13.20 µm), 14 (86.56 ± 12.40 µm) (p = 0.2524), or 21 (69.92 ± 4.08 µm) (p = 0.8389). Overall, the ISR% was 6.2 ± 3.8%. No significant differences were observed between the 7, 14, and 21-day time points. In 12/20 (60%) of the stented rats, RT was observed. Across all time points, the mean RT was 32.01 ± 23.12%. At 7 days, the RT was 4.59 ± 0.20%; at 14 days, 37.91 ± 20.69% (p = 0.1527); and at 21 days, 36.54 ± 27.42% (p = 0.2494) without significant differences (Figure 3C).
Endothelial coverage by SEM (Group 2)
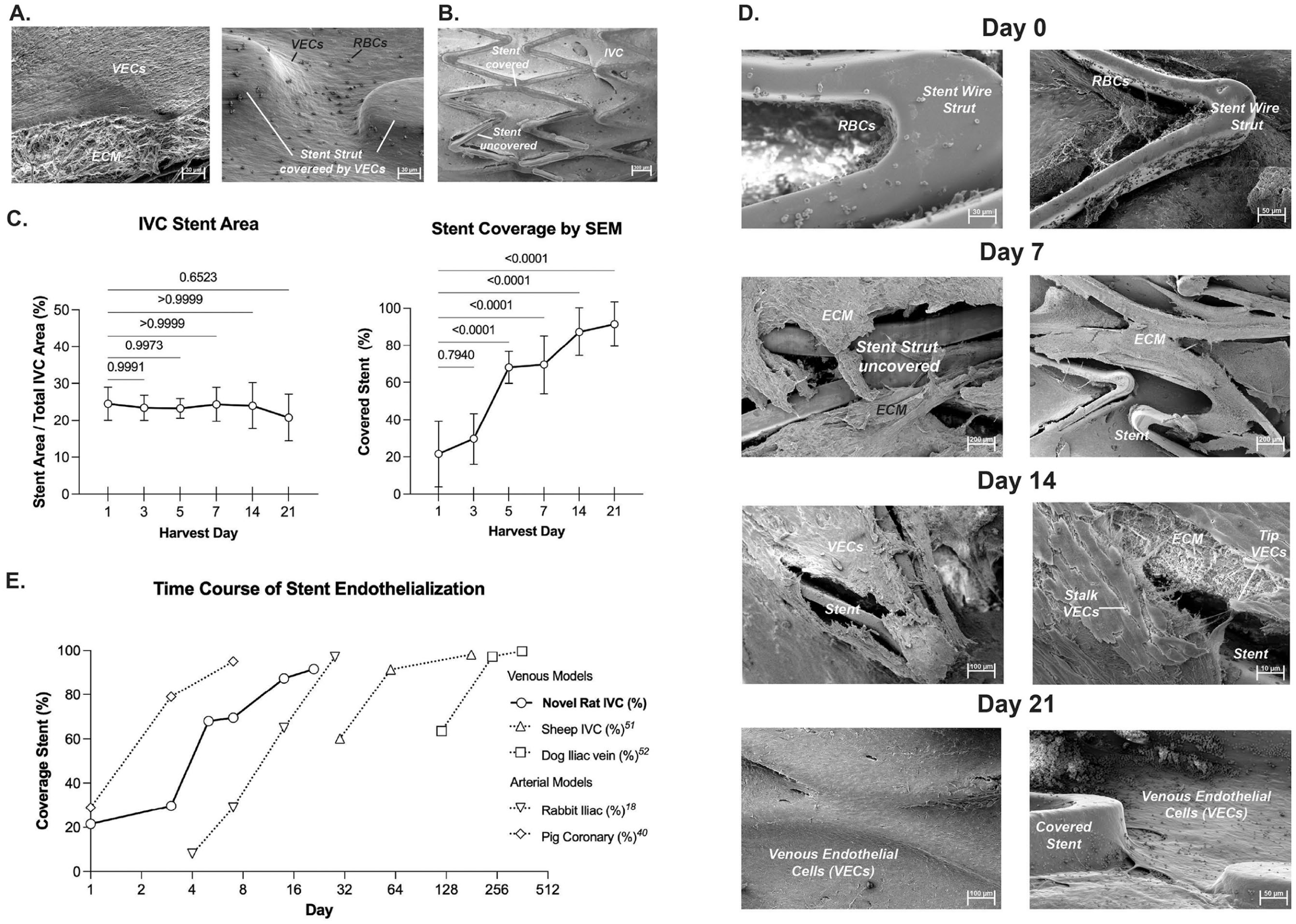
Across all animals, the area of each stent in relationship with the total area of the IVC was 23.35 ± 4.92%, with no significant differences among the groups. High-power magnification SEM (1000×) stent strut images showed fine surface morphology. A nonstented normal IVC exhibited an aligned monolayer of venous endothelial cells (VECs) situated above the extracellular matrix (ECM) (Figures 4A and 4B). Postimplantation, the ECM was exposed and visible through the stent fenestrae at day 7. The deposited ECM was later covered by endothelium growing from the nonstented edges until day 21, covering the stent (Figure 4C). After 1 day, stent coverage by endothelial cells was 21.57 ± 11.11%; after 3 days, it was 29.67 ± 8.55%; after 5 days, 68.06 ± 6.90%; after 7 days, 69.53 ± 14.84%; after 14 days, 87.33 ± 15.39%; and after 21 days, 91.51 ± 11.23% (Figures 4D–4F). By day 21, endothelial cells appeared to align parallel to the direction of blood flow on SEM images. This rapid progression after day 5 demonstrates that the rat IVC achieves near-complete stent endothelialization within approximately 3 weeks postimplantation.
En face IF staining (Group 3)
To better characterize the cell identity of the layer covering the venous stents, we first performed en face IF of DAPI, CD31, αSMA markers on IVCs of sham rats, which demonstrated the presence of VECs and alignment of blood flow direction on the IVC. After 1 day of stenting, we observed a few cells lining the stent struts. After 21 days, the stented vessels had a continuous surface coverage of positive CD31+ VEC cells (Figures 5A–5D). The overall morphology of these CD31+ VECs over the wire is similar to that observed on the IVC of the sham rat.
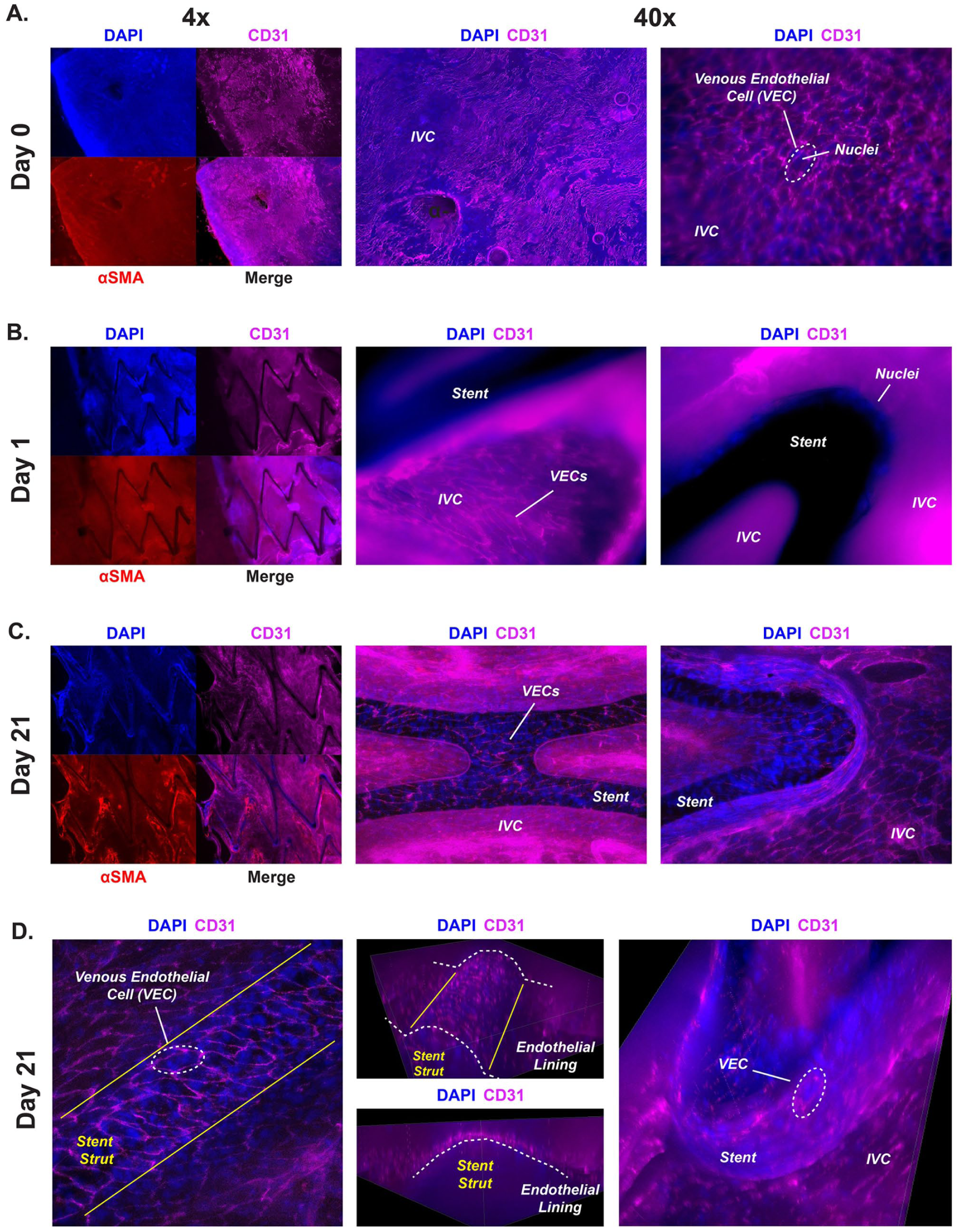
High-precision (40×) full-focused 3D image reconstruction featuring CD31 and DAPI staining suggests that the scaffold deposited next to the stent struts forms an endothelial lining resembling a speed bump-like appearance at 45° (Figure 5). We also demonstrated how the CD31+ VEC cells can grow vertically over the wire until a full monolayer is achieved. These detailed endothelial cell features cannot be observed unless specific 3D reconstructions are performed at high magnification in advanced IF imaging or by altering the angle of SEM imaging, as shown in Figure 4D, which shows the lateral side of a stent strut covered at 21 days.
Discussion
The main findings of these preclinical deep vein stenting models were complete stent patency by ultrasound with the use of a single dose of perioperative anticoagulation, and the virtually complete stent coverage by day 21 with CD31+ VECs. In the first stenting model without anticoagulation, 6% ISR was identified by histopathological analysis. Without anticoagulation, the stent patency improved after 24 hours as assessed by ultrasound. Histopathological analysis demonstrated a mean RT of 37% of the lumen of the stented vessels at 21 days without anticoagulation. This model can enable the use of preclinical thrombosis models and imaging methods to help characterize thrombosis resolution in deep vein stents.42–45
In our nonanticoagulated stenting model, we also observed a modest luminal ISR of 6%. We believe that this stenting model can evaluate the amount of ISR of the IVC, and facilitate the testing of future drug-eluting coatings. The structural and pathological characteristics of thrombosis, ISR, and DIT observed in human stented tissue have gained significant relevance due to their association with clinical outcomes.15,46 Recently, medical interest in the pathology of DIT within stents has intensified due to the capacity of these features to predict restenosis/occlusion. Zhao et al. suggested that integrating histopathological assessment into postthrombectomy evaluation can help optimize postthrombotic (PTS) management strategies for iliofemoral in-stent occlusion. They reported that DIT was the predominant feature in occlusions beyond 3 months and that old thrombus and RT higher than 30% predicted restenosis/occlusion. 47
In the second stenting model that received anticoagulation, all stents remained patent during the perioperative period, and endothelial coverage increased from 69% at 7 days to 91% at 21 days. Our data show that simply by withholding periprocedural anticoagulation, it is possible to generate a model that has histologic characteristics that mimic those of partially or completely occluded human venous stents. This model could be used to study combinations of anticoagulant, antiinflammatory, and antiplatelet therapies poststenting, and their patency outcomes. Establishing optimal medical therapy poststenting was recently identified as the number-one research priority outlined by the Society of Interventional Radiology Foundation (SIRF) Research Consensus Panel. 48
The time to complete stent endothelialization is a critical factor in determining the need and duration of antiplatelet therapy in arterial stents and remains an unanswered question in the field of venous stents. Historically, in vivo models and computational models have attempted to recreate endothelial behavior after stenting and forecast cell growth and drug interactions. 49 Nevertheless, no model can fully capture all the biological interactions present in clinical trials. In our animal study, rapid endothelialization was observed with SEM, consistent with other venous stent models and the SEM IVC findings in rats.50–52 In humans, the stent endothelialization of veins has only been documented in a case report using angioscopy after 30 days, with few studies examining cell features via SEM.53–55 This direct observation method for endothelial assessment was employed by Che et al. to confirm the full endothelial coverage of venous stents 3 months after implantation in the iliac vein of a sheep. 56
When compared to established arterial stent models, the pace of endothelialization in the rat IVC is intermediate — faster than the pace in larger venous animal models but generally slower than arteries (Figure 5E).18,39,50,51,57 Previous animal (porcine and rabbit) arterial models and human coronary stents have demonstrated faster endothelial coverage, reflecting a faster regenerative capacity, possibly due to different flow dynamics and biological differences.18,39,57–61 Overall, our rat model offers a more efficient method for studying venous stent endothelialization as an alternative to large animal models due to reduced space utilization, a short procedural duration, and reduced personnel requirements for surgical and anesthesia assistance.
Technical considerations
For successful stent implantation, several considerations are crucial. First, maintain the rat’s temperature with a heating source for survival and to monitor anesthesia during procedures. Keep total anesthesia under an hour per procedure. Second, to prevent blood loss while separating the aorta from the IVC, start at the infrarenal IVC and continue distally. Third, when the IVC was sutured, the first two sutures should leave enough space for adequate canulation with the stent sheath and to avoid postimplantation IVC narrowing. Fourth, during stent deployment, it is recommended that the stent sheath is maintained with one hand while the stent introducer is pushed with the other hand, slowly maintaining alignment with the IVC.
In Group 2, which received anticoagulation, a superficial skin hematoma was observed, presenting as a palpable abdominal mass that was confirmed by ultrasound in three anticoagulated rats. The rats showed no gastrointestinal symptoms and remained hemodynamically stable. Two of the superficial hematomas resolved spontaneously. Only one rat with a persistent hematoma required treatment with ultrasound-guided aspiration under anesthesia after aseptic preparation, which involved removing 2 mL of sanguineous fluid without recurrence or complications in accordance with institutional animal care guidelines. Finally, immunohistochemistry is not recommended for plastic-embedded nitinol stent staining, as this process which requires advanced cutting techniques, drastically disrupts the morphology, and presents antigen retrieval difficulties. 62 En face IF is a more robust method for cell characterization.
Limitations
The main limitation of our study arises from its focus on only one venous stent design, with predetermined animal baseline conditions including a fixed stent and IVC diameter. These considerations were established to increase the reproducibility of this model, but may not be fully reflective of the changes that the respiratory rate, hematocrit, and temperature can have on local hemodynamics and shear rates. These conditions, together with the assumed circular vessel cross-sectional area, the assumed steady-state Newtonian flow, and the predefined blood viscosity, make the observed hemodynamics and wall shear stress calculations rough approximations rather than exact measurements. Second, human stenting encompasses substantial differences in vessel diameter, flow, and immunobiology. 63 Our model does not completely reflect the complexity of the human postthrombotic condition; instead it resembles nonthrombotic iliac vein lesions (NIVL).
In this study, it was not possible to compare the rates of ISR formation observed between the groups at later time points by histological analyses without substantially increasing the number of animals. This is because the animal specimens can only be processed for plastic embedding for detailed histological morphology (Group 1), or for SEM/IF microscopy (Groups 2 and 3). This limitation can be addressed by novel imaging modalities that can overcome the resolution limitations of ultrasound, such as molecular magnetic resonance imaging (MRI) and fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT).64,65
Finally, en face IF and SEM have been the gold standard for assessing stent endothelialization; however, other emerging methods, such as intravascular ultrasound (IVUS), optical coherence tomography (OCT), micro-CT, and others, are being investigated and should be compared in future studies.66–77 Further characterization of cell proliferation (Ki-67), apoptosis (Caspase-3), spontaneous thrombolysis (tissue plasminogen activator [tPA]), immune cell characterization (CD68), and other features of VECs (von Willebrand factor [VWF], vascular endothelial [VE]-cadherin) can be achieved with advanced IF imaging by using conjugated antibodies in the far-infrared wavelengths. With the incorporation of these technologies, it will be possible to characterize the role of anticoagulation and antiaggregation in venous in-stent restenosis prevention.
Future directions
Future uses of this model should focus on postthrombotic stenting to investigate the whole spectrum of the disease, allowing for comparative studies of different stent designs in combination with antithrombotic/antiplatelet and antiinflammatory therapies. Another area of recent development is the study of biomaterial interactions to improve endothelialization, similar to the approach taken by Wu et al. in sheep and Oliver et al. in rabbits.78,79 Finally, future studies should incorporate the use of unbiased technologies (transcriptomics and proteomics) to establish the specific drivers of stent failure (DIT and ISR) more accurately.80–82
Conclusions
The results of this study demonstrate that this novel preclinical model for venous stenting, characterized by ultrasound imaging, histopathology, and microscopy, enables the identification of pathological processes (thrombosis, ISR, DIT) present in human pathological stents and can correlate with clinical outcomes, helping to tailor and optimize management strategies. Administering a single periprocedural dose of anticoagulation allows for the analysis of stent coverage (SEM) and cell phenotype (IF) up to 21 days after stenting. With this robust model, we provide the means to further assess the performance of new stent designs, coatings, and pharmacological combinations in the future.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X261436329 – Supplemental material for Histopathological and duplex characteristics of deep venous stents: A novel microsurgical small animal model
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X261436329 for Histopathological and duplex characteristics of deep venous stents: A novel microsurgical small animal model by Oscar Moreno, Trevin Eggleston, Catherine E Luke, Amber Clay, Kate Micallef, Kiran Kumar, Sabrina Rocco, Kevin Hughes, David Gordon, Daniel D Myers, Thomas W Wakefield, Peter K Henke and Andrea T Obi in Vascular Medicine
Footnotes
Acknowledgements
We would like to thank the University of Michigan Frankel Cardiovascular Center for their support with microscope equipment assistance, Hongyu Liu for his help on IF imaging, Carol Whitinger and Emma Snyder-White from the Orthopaedic Research Laboratories (ORL) Histology Core for their assistance during the histology processing, Jing Liang and Megan Bennett from the Microscopy Core for their help with SEM sample processing and imaging, and Ismael Assi for his help with the wall shear stress calculations.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Daniel Myers and Andrea Obi received funding for preclinical trials related to deep vein stenting from Medtronic. Kevin Hughes is currently a Principal R&D Engineer at Medtronic. The remaining authors have no conflicting interests.
Funding
This work was supported by the Elizabeth Anne Baiardi Research Fund, the Jobst Foundation, the National Institutes of Health (P30AR069620), and Medtronic. Medtronic provided custom stents at no cost and supported the development of this microsurgical technique in animals. Medtronic did not participate in data analysis or interpretation of the results. Medtronic reviewed the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.