
Abstract

Stiff-person syndrome (SPS) is a rare autoimmune neurological disorder with an estimated prevalence of one to two per million, characterized by progressive axial and limb rigidity, and painful, stimulus-sensitive spasms. 1 Its immunological hallmark is the presence of high-titer autoantibodies against the 65-kDa isoform of glutamic acid decarboxylase (GAD65), the rate-limiting enzyme in gamma-aminobutyric acid (GABA) synthesis. 2 SPS belongs to the broader ‘GAD antibody-spectrum disorders’ (GAD-SD), which also encompasses type 1 diabetes mellitus, autoimmune thyroiditis, cerebellar ataxia, and limbic encephalitis.2,3 Although the neurological pathogenesis of SPS is well characterized, potential extraneurological manifestations have received little attention. Nailfold videocapillaroscopy (NVC) is a validated, noninvasive technique widely used in rheumatology to assess microvascular integrity in systemic autoimmune diseases, 4 yet it has never been applied to patients with SPS. Here are described, to the author’s knowledge for the first time, significant capillaroscopic abnormalities in a patient with anti-GAD-positive SPS.
A systematic literature search was conducted across Scopus and Medline (PubMed) up to November 2025, combining terms for SPS and GAD65 with capillaroscopy, microcirculation, and endothelial dysfunction; no relevant publications were identified. The patient is a 53-year-old woman diagnosed with SPS in 2021 on the basis of progressive axial and lower-limb rigidity, painful spasms, continuous motor unit activity on electromyography, and elevated anti-GAD titers (50 IU/mL). She had no history of diabetes, thyroid disease, or connective tissue disease, and she was a nonsmoker. Notably, she reported rare, brief episodes of cold-triggered acrocyanosis of the hands, without the classic triphasic color changes of Raynaud’s phenomenon.
A comprehensive autoimmune work-up was negative, including antinuclear antibodies (ANA), an extractable nuclear antigen (ENA) panel, anti-Scl70, anticentromere, anti-RNA polymerase III, and antiphospholipid antibodies. Her current treatment comprises monthly intravenous immunoglobulins (IVIg), diazepam, gabapentin (800 mg three times daily), baclofen (25 mg twice daily), and medical cannabis (Bediol: Bedrocan, Veendam, The Netherlands; THC 6.3%, CBD 8.8%). Given the autoimmune nature of her condition, NVC was performed using a videocapillaroscope at 200× magnification on the second to fifth fingers of both hands, after a 15-minute acclimatization period at a controlled room temperature of 22–24°C. Images were quantitatively analyzed using the Capi-Detect algorithm, a machine learning tool that provides an automated, operator-independent classification of capillary morphology, including the identification of enlarged capillaries. 5
The analysis revealed a nonspecific abnormal pattern (Figure 1A), with diffuse peripapillary edema, a high proportion of enlarged capillaries (51.2%), three microhemorrhages, 22% tortuous capillaries, and a borderline-low capillary density of 7.03 capillaries/mm (Figure 1B). 6 No giant capillaries or avascular areas were observed, ruling out a scleroderma pattern. The patient had no history of Raynaud’s phenomenon, no clinical or serological evidence of connective tissue disease, and no history of diabetes mellitus or other systemic disorders typically associated with structural microangiopathy. Furthermore, no acute vasoactive medications or recent therapeutic modifications had been introduced prior to capillaroscopic assessment.
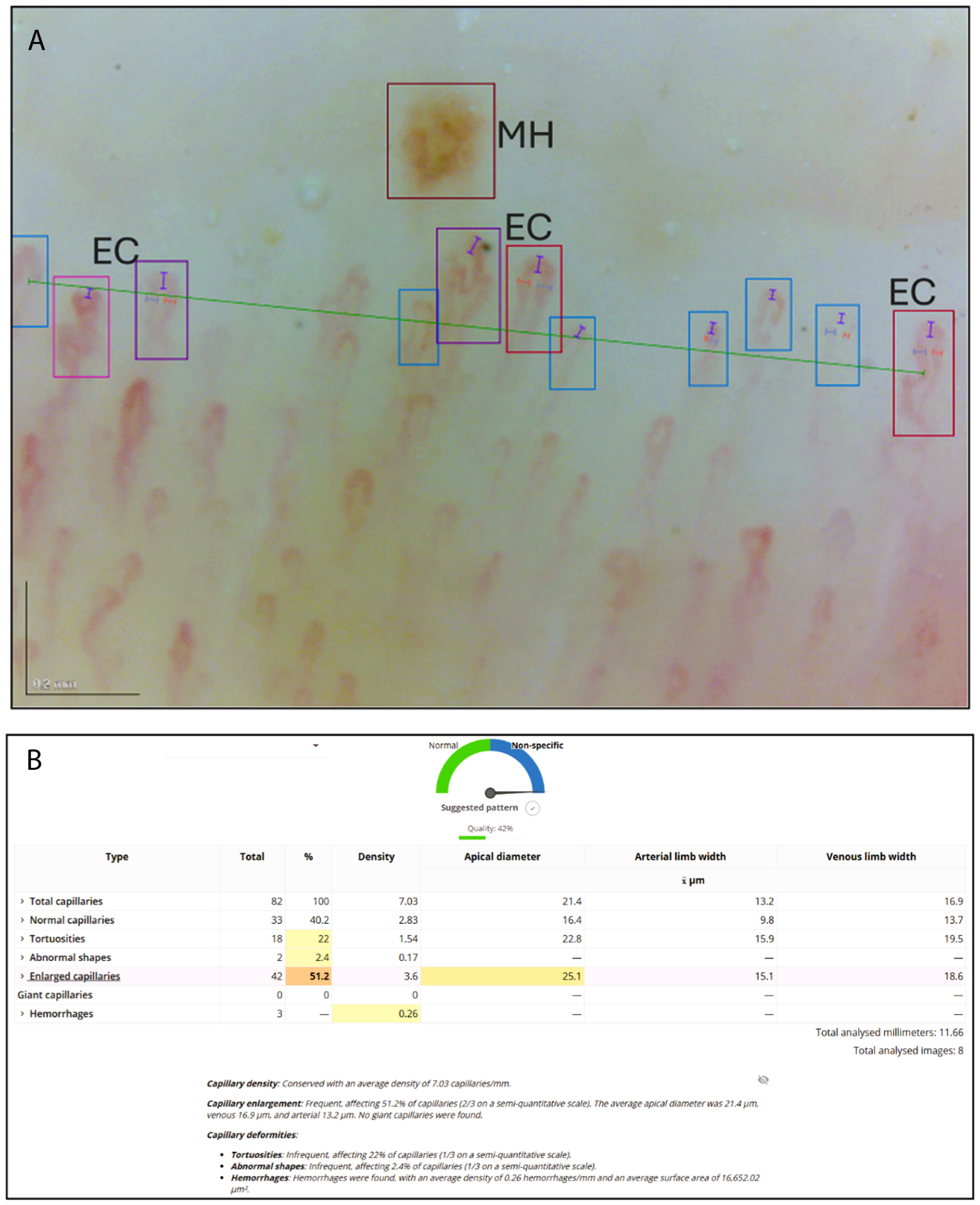
The proportion of enlarged loops is particularly striking: in healthy individuals assessed with semiquantitative criteria and defined diameter thresholds, the prevalence of dilated capillaries generally remains within the 10–15% range.7,8 A diffuse pattern exceeding 50% enlarged loops lies well beyond physiological variability, and is strongly suggestive of pathological microvascular involvement.
Several features of this case deserve comment. The negative connective tissue disease screening argues against an occult overlap syndrome as the explanation for these microvascular changes. The patient’s episodic acrocyanosis, although mild, provides a clinical correlate suggesting that the microvascular involvement is not entirely subclinical. Comparable nonspecific capillaroscopic abnormalities have been reported in other autoimmune conditions outside the scleroderma spectrum, including systemic lupus erythematosus, dermatomyositis, and Sjögren’s syndrome, where they are thought to reflect endothelial dysfunction. 9 It is tempting to speculate that a similar process may occur in SPS: endothelial cells have been shown to process and present GAD65 epitopes, facilitating transmigration of autoreactive T cells, 10 which could in principle lead to low-grade, chronic endothelial injury. However, this observation is limited to a single patient, and an incidental finding cannot be excluded. Nor can a contribution from the patient’s ongoing therapies be ruled out, although IVIg is generally regarded as endothelial-protective, and Bediol’s high CBD content is expected to exert predominantly antiinflammatory and vasodilatory effects. The absence of endothelial biomarkers and longitudinal follow-up further prevents firm pathogenic conclusions. These findings are therefore presented strictly as hypothesis-generating; confirmation in larger, controlled cohorts will be needed before any causal relationship between GAD65-directed autoimmunity and systemic microangiopathy can be established.
In summary, significant microvascular abnormalities on NVC are described in a patient with SPS, accompanied by mild clinical signs of peripheral vascular dysfunction. A graphical abstract is provided in the supplemental material. These preliminary observations raise the question of whether SPS may harbor a systemic vascular dimension that has so far gone unrecognized, and they warrant further investigation in dedicated studies.
Supplemental Material
sj-png-1-vmj-10.1177_1358863X261437082 – Supplemental material for Nailfold capillary abnormalities in a patient with stiff-person syndrome: Potential novel window into pathogenesis
Supplemental material, sj-png-1-vmj-10.1177_1358863X261437082 for Nailfold capillary abnormalities in a patient with stiff-person syndrome: Potential novel window into pathogenesis by Angelo Nigro in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.