
Abstract

Thoracic aortic aneurysm (TAA) is pathological dilation of the aorta associated with life-threatening events such as dissection or rupture. Because TAAs are often asymptomatic and detected incidentally, clinical management relies on imaging to characterize aneurysm size and growth, which remain primary determinants of surgical intervention given the increased risk of acute aortic events with larger or rapidly expanding aneurysms.1,2 Importantly, adverse events can still occur below threshold diameters, suggesting that objective markers are imperfect predictors of perceived or actual risk. 3
Although clinical management focuses on anatomical severity, research across cardiovascular populations demonstrates that subjective illness perceptions (i.e., patients’ beliefs and emotional responses to illness), predict distress, adherence, and rehabilitation engagement beyond clinical indicators.4–6 Little is known about how illness perception develops in TAA or whether it aligns with objective measures such as aneurysm size. Because engagement with lifestyle recommendations depends partly on how individuals interpret their condition, understanding whether surveillance experience shapes illness perception in TAA is clinically meaningful. This study examined whether aneurysm size was associated with subjective illness perception and whether time under surveillance modifies this relationship. We hypothesized that larger aneurysm size would predict greater illness concern, whereas longer surveillance duration would attenuate this association.
This cross-sectional study included patients with TAA receiving care at a rural-serving cardiac surgery clinic in eastern North Carolina. This study was reviewed and approved by the East Carolina University and Medical Center Institutional Review Board (UMCIRB), under protocol no. UMCIRB 22-002578. Data were collected during routine outpatient visits between April 2023 and June 2024. Participants were ⩾ 18 years old, English-proficient, and under active surveillance for a TAA for at least 1 month. Sixty-seven patients provided written informed consent and completed study procedures during a single clinic visit.
Illness perception was assessed using the Brief Illness Perception Questionnaire (BIPQ), a validated nine-item instrument assessing perceived consequences, timeline, control, identity, concern, understanding, and emotional response. 7 Items are rated 0–10; total scores range from 0–80, with higher scores indicating greater perceived illness threat. Aneurysm size (cm) was obtained from the most recent imaging study. Surveillance duration (years) was calculated from time of diagnosis to the study visit.
Analyses were performed in R version 4.5.1 (R Foundation for Statistical Computing). Bivariate correlations examined relationships among aneurysm size, surveillance duration, and BIPQ total score. Linear regression models tested whether aneurysm size predicted illness perception and whether surveillance duration moderated this association (aneurysm size × surveillance duration). Statistical significance was defined as p < 0.05.
Participants had a mean age of 65.9 years (SD = 10.1); the sample was predominantly men (73.1%) and White (80.6%). Mean aneurysm size was 4.36 cm (SD = 0.42) and mean time under surveillance was 3.32 years (SD = 3.30), with fewer than 5% of patients having a known connective tissue disorder (Table 1). The mean BIPQ total score was 29.8 (SD = 11.3). Scores varied widely across patients (median = 31; range 9–58), spanning low, moderate, and high illness threat categories.
Patient characteristics (N = 67).
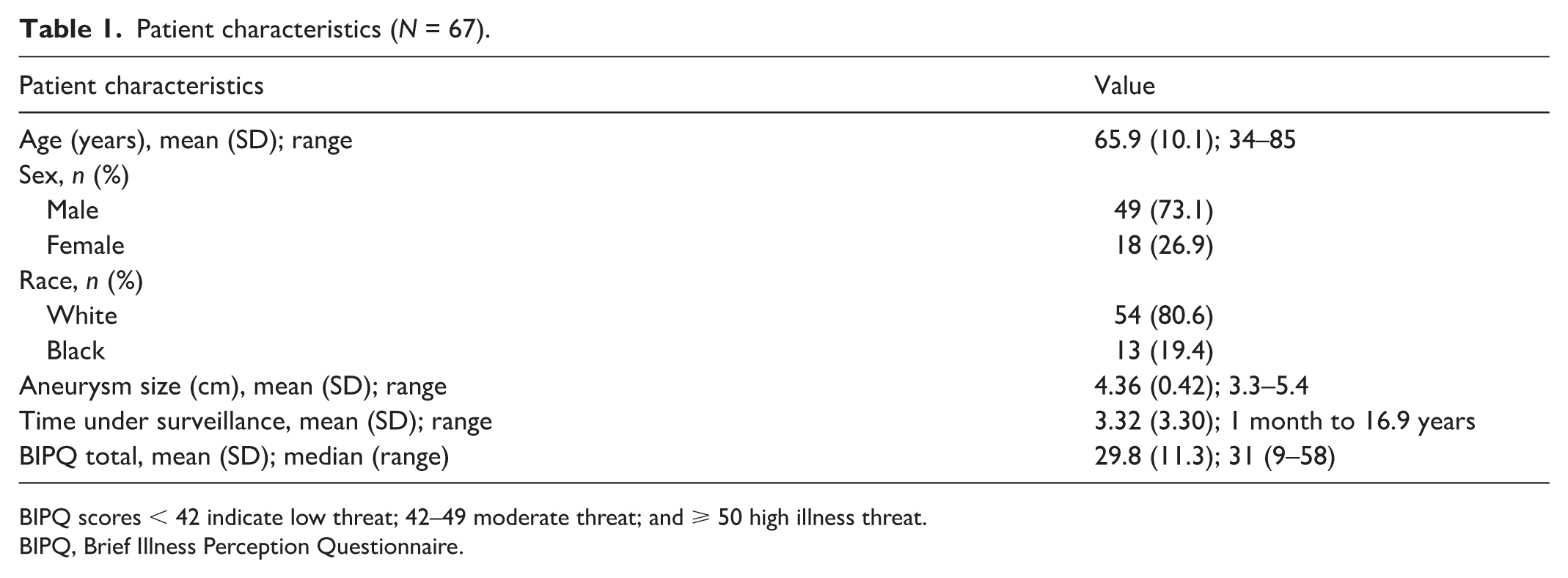
BIPQ scores < 42 indicate low threat; 42–49 moderate threat; and ⩾ 50 high illness threat.
BIPQ, Brief Illness Perception Questionnaire.
Aneurysm size did not significantly predict illness perception (B = 1.32, SE = 3.33, p = 0.69). Surveillance duration was also unrelated to illness perception (B = −2.90, SE = 5.88, p = 0.62) and did not moderate the association between size and BIPQ score (interaction B = 0.54, SE = 1.28, p = 0.68). The model explained minimal variance (R2 = 0.02) and correlations among the primary variables were small (|r| < .11).
Objective indicators of TAA severity were not associated with subjective illness perception in this sample. Aneurysm size did not relate to perceived consequences, emotional burden, or illness-related disruption, and time under surveillance neither predicted illness perception nor modified the effect of aneurysm size. These results indicate that patients’ psychological understanding of TAA may develop independently of anatomical metrics or surveillance duration.
The common-sense model of self-regulation proposes that illness perceptions reflect a combination of medical information, prior experience, and personal beliefs. 8 Although clinicians emphasize aneurysm diameter and stability, these data suggest such information may play a limited role in shaping patients’ internal models of illness. Prior research in cardiovascular populations shows that illness perceptions predict health behaviors and emotional outcomes independent of objective clinical data.4 –6 Our findings extend this pattern to TAA: smaller aneurysms do not reliably correspond to lower perceived illness threat. Routine imaging may also contribute to this disconnect. For some patients, serial measurements may be reassuring; for others, repeated focus on aneurysm presence may maintain vigilance, similar to ‘scanxiety’ described in oncology.9,10
Clinically, these findings underscore the need for providers to assess subjective illness perceptions rather than assuming psychological comfort based solely on anatomical indicators, particularly within specialized centers managing patients with aortic disease. Brief tools such as the BIPQ may help identify patients experiencing disproportionate concern despite reassuring imaging. Limitations include the single-site design, modest sample size, and cross-sectional methodology; results should therefore be interpreted cautiously, as unmeasured factors (e.g., family history, clinical setting, stress levels) may influence illness perceptions.
Aneurysm size and surveillance duration were not associated with illness perception in this sample of patients with TAA, suggesting that psychosocial assessment during surveillance may help identify concerns not reflected by objective clinical indicators.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Samuel F Sears has rececieved honoraria/consulting fees from Abbott, iRhythm, Medtronic, Philips, Solid Bioscience, and Zoll Medical; and research grants to East Carolina University from Thryv and CVRx. The remaining authors have no conflicting interests.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.