
Abstract
Background:
Carotid stenosis accounts for 20–30% of ischemic strokes. In France, management practices for symptomatic and asymptomatic disease remain heterogeneous. This study assessed the nationwide trends and outcomes of carotid endarterectomy (CEA) and carotid artery stenting (CAS) from 2011 to 2020.
Methods:
Using the French National Health Data System, we identified patients who underwent CEA or CAS for carotid stenosis. Symptomatic status was defined by stroke or transient ischemic attack within 6 months before intervention. Comorbidities were measured using the Charlson Comorbidity Index. The primary outcome was 30-day stroke or all-cause death.
Results:
Among 149,273 patients (85% asymptomatic), 4.8% of asymptomatic and 3.5% of symptomatic patients underwent CAS; the remaining patients underwent CEA. CAS recipients had greater comorbidity (Charlson ⩾ 3: 53% vs 39% in asymptomatic patients; 75% vs 66% in symptomatic patients). Thirty-day stroke/death occurred in 1.8% of asymptomatic patients (CAS 3.2% vs CEA 1.7%, p < 0.001) and 12.6% of symptomatic patients (CAS 15.5% vs CEA 12.6%). After multivariable adjustment, CAS was independently associated with higher risks of 30-day stroke and stroke/death compared with CEA. Five-year mortality was higher after CAS (28.5%) versus 20.9% after CEA. Cranial nerve injury was more frequent after CEA in symptomatic patients. Preoperative statin and antiplatelet use was lower in symptomatic patients (67.9% and 67.1%, respectively) versus asymptomatic patients (84.5% and 92.2%, respectively).
Conclusions:
CEA remains the predominant treatment for carotid stenosis in France, whereas CAS is mainly used in higher-risk patients. Early postoperative complications are more frequent in symptomatic cases, and lower preoperative medical therapy use highlights suboptimal secondary prevention in this group.
Keywords
Introduction
Strokes are the second leading cause of death and a major cause of long-term disability in France. Approximately 30% of patients who suffer a stroke remain dependent in daily activities, making stroke prevention a critical public health priority. Ischemic stroke accounts for the vast majority of cases, with significant carotid artery stenosis identified in 20–30% of them.1,2 In Europe, severe asymptomatic carotid stenosis (stenosis > 70%) is estimated at 0.5%. 3 For asymptomatic carotid stenosis, risk of stroke is estimated at 0.1% to 1.6% per year for stenosis < 80% (NASCET) and up to 2.4% per year for greater degrees of stenosis. 4 A recent study found that the estimated rate of ipsilateral carotid-related acute ischemic stroke in patients with severe asymptomatic stenosis without surgical intervention (> 70–90%) is 4.7% over 5 years. 5
Between 1990 and 2004, large randomized studies established that carotid revascularization should be indicated for symptomatic stenosis > 70% (NASCET), providing lasting benefits in mortality and stroke prevention over 8 years.6,7 This benefit was more pronounced when revascularization occurred within 14 days of the neurological event. 3 For severe asymptomatic carotid stenosis (⩾ 70% according to NASCET), carotid endarterectomy (CEA) in patients under 75 years old appeared to reduce the incidence of strokes/transient ischemic attacks (TIAs) and death at 5 years.3,8
However, current indications for revascularization of symptomatic and asymptomatic carotid stenosis through open surgery rely on outdated randomized studies and the results of carotid artery stenting (CAS) remain heterogeneous and uncertain.9–12 At the same time, the improved efficacy of medication in secondary stroke prevention challenges the results of invasive revascularization, particularly for asymptomatic stenosis.9,13
CEA is currently the standard revascularization technique, but since the 2000s, CAS has gained popularity. 14 The technique is less invasive compared with CEA, and a dedicated endovascular environment has been developed to ensure optimal performance and safety. Higher-risk patients with symptomatic carotid stenosis > 50% or asymptomatic stenosis > 80% may benefit the most, although recent studies have reported higher morbidity and mortality rates beyond 30 days compared with CEA.9,15
In real-world practice, particularly for asymptomatic cases, management strategies often vary widely between institutions and clinicians, reflecting a lack of updated consensus and clear indications. In this context, a comprehensive nationwide evaluation of current practices is essential to assess the actual use of revascularization procedures in light of evolving evidence.
The objective of this study is to analyze trends and outcomes associated with CEA and CAS in France between 2011 and 2020, using the National Health Data System (SNDS). The analysis distinguishes between symptomatic and asymptomatic cases, and aims to evaluate postoperative outcomes, perioperative medical management, and temporal trends in revascularization practice.
Methods
We conducted a retrospective observational cohort study, which included all patients who underwent carotid revascularization in France from 2011 to 2020. The data were extracted from the SNDS database. The SNDS integrates the claims database of the national compulsory health insurance system (SNIRAM) with the database of public and private healthcare facilities (PMSI) and the national death register (CépiDC), using a unique pseudonymized national identifier. 16 Covering approximately 99% of the French population (> 67 million people), it includes all reimbursed healthcare expenses, hospital discharge summaries with International Classification of Diseases, Tenth Revision (ICD-10) coded diagnoses, and surgical procedures coded under the CCAM French classification. Drugs are encoded according to the Anatomical Therapeutic Chemical (ATC) classification. Additionally, it provides information on dates and causes of death.
The study was performed according to current French Data Protection Authority regulations (Commission Nationale de l’Informatique et des Libertés [CNIL]). Access to the SNDS database was made available by the French National Agency for the Management of Hospitalization Data according to Reference Methodology 04. As this was a retrospective, longitudinal, and noninterventional study of an anonymized database and had no influence on patient care, ethics committee approval and patient consent were not required. This study was conducted in accordance with the STROBE guidelines for observational research. 17
Study population
All patients aged over 18 years with a primary diagnosis of symptomatic or asymptomatic carotid stenosis who underwent CEA or CAS were included from 2011 to 2020. Data collected over a 3-year period before inclusion enabled the differentiation between symptomatic and asymptomatic stenosis and the extraction of key information, including patients’ medical history and preoperative medication. We classified patients as having symptomatic carotid stenosis if they had an ICD-10 diagnostic code for stroke or TIA within 6 months prior to the revascularization procedure. This definition corresponds to a typical secondary prevention setting and was chosen to reflect real-world clinical decision-making. Regarding the type of revascularization performed, CCAM codes enabled the selection of patients treated either by CEA or CAS. Supplemental Appendix 1 lists the selected CCAM and ICD-10 codes for the procedure and diagnosis.
We divided the cohort into two groups: asymptomatic and symptomatic carotid stenosis. Each group was further divided into two subgroups based on treatment modality: CEA or CAS.
Patients’ medical history and comorbidities, categorized by the Charlson Comorbidity Index (CCI), were collected. A CCI of 0 or 1 indicated no comorbidities, a CCI of 2 indicated low comorbidity, and a CCI of 3 or higher indicated high comorbidity. 18 The ATC drug classification monitors medications prescribed to patients before and after surgery. Appropriate medical therapy was defined as the prescription of at least one evidence-based cardiovascular preventive medication (antiplatelet agent, statin, or angiotensin-converting enzyme [ACE] inhibitor/angiotensin-II receptor blocker [ARB]) prior to the index procedure.
Endpoints
The primary endpoint was a composite of all-cause mortality and stroke (including TIA) within 30 days of the index procedure (CEA or CAS), in accordance with international reporting standards. Secondary endpoints were all-cause death and/or stroke at 5 years, 30-day postoperative medical complications (coronary artery disease, arrhythmia, congestive heart failure, acute kidney injury, respiratory failure) or 30-day postoperative access-related complications (cranial nerve injury, bleeding, and infection), and 30-day reintervention rates. Stroke alone and stroke/death excluding TIA were additionally analyzed to facilitate comparison with international guideline benchmarks.
Statistical analysis
Data extraction and statistical analysis were conducted on the secure platform of the Système National d’Information Inter-Régimes de l’Assurance Maladie (SNIIRAM) of the Caisse Nationale de l’Assurance Maladie (CNAM). Descriptive data analyses were performed for all collected variables for the entire cohort. Baseline characteristics of the study population were summarized using means (SDs) for continuous variables and frequencies (percentages) for categorical variables. Categorical variables were compared using the Pearson’s chi-squared test, and the relationship between quantitative and qualitative variables was analyzed using the Kruskal–Wallis nonparametric test. Associations between treatment modality (CAS vs CEA) and clinical outcomes at 30 days and 5 years were assessed using a multilevel logistic regression model with random intercepts for centers. Explanatory variables included age, sex, CCI, major cardiovascular comorbidities, diabetes, renal disease, and preoperative medical therapy. Kaplan–Meier curves were constructed to display 5-year overall survival and stroke-free survival, stratified by treatment modality and symptom status. Log-rank tests were used to compare survival curves. Most analyses were performed using SAS version 9.4 (SAS Institute). Survival analyses were performed using the ggsurvfit package in R software version 4.4.3 (R Foundation for Statistical Computing).
Results
A total of 149,273 patients (28.7% women [n = 42,896]) were included over a 9-year period (2011–2020). The age distribution is represented in Supplemental Appendix 2.
Patients treated with CAS had significantly higher rates of congestive heart failure, coronary artery disease, peripheral vascular disease, and kidney disease compared with those treated with CEA (p < 0.001). A CCI ⩾ 3 was found in 44% (n = 65,831) of patients, significantly more prevalent in symptomatic patients (66%, n = 15,252) compared with asymptomatic patients (40%, n = 50,579). Among those treated with CAS, a higher proportion had a CCI ⩾ 3 compared with those treated with CEA; this difference persisted when stratified by symptomatic (75% vs 66%) and asymptomatic (53% vs 39%) carotid patients.
Additionally, 16% (n = 3627) of symptomatic patients lacked appropriate medical treatment (antiplatelet, ACE inhibitor, statin) before the intervention, compared with 2.2% (n = 2715) of asymptomatic patients. Indeed, before revascularization, 92% (n = 116,581) of asymptomatic patients were receiving antiplatelet therapy and 84% (n = 106,538) were on statins, compared with 67% (n = 15,545) and 68% (n = 15,672) of symptomatic patients, respectively. Postoperatively, 98% (n = 146,857) of all patients received appropriate medical therapy, with no significant differences between the groups. The demographic data are presented in Table 1.
Baseline characteristics.
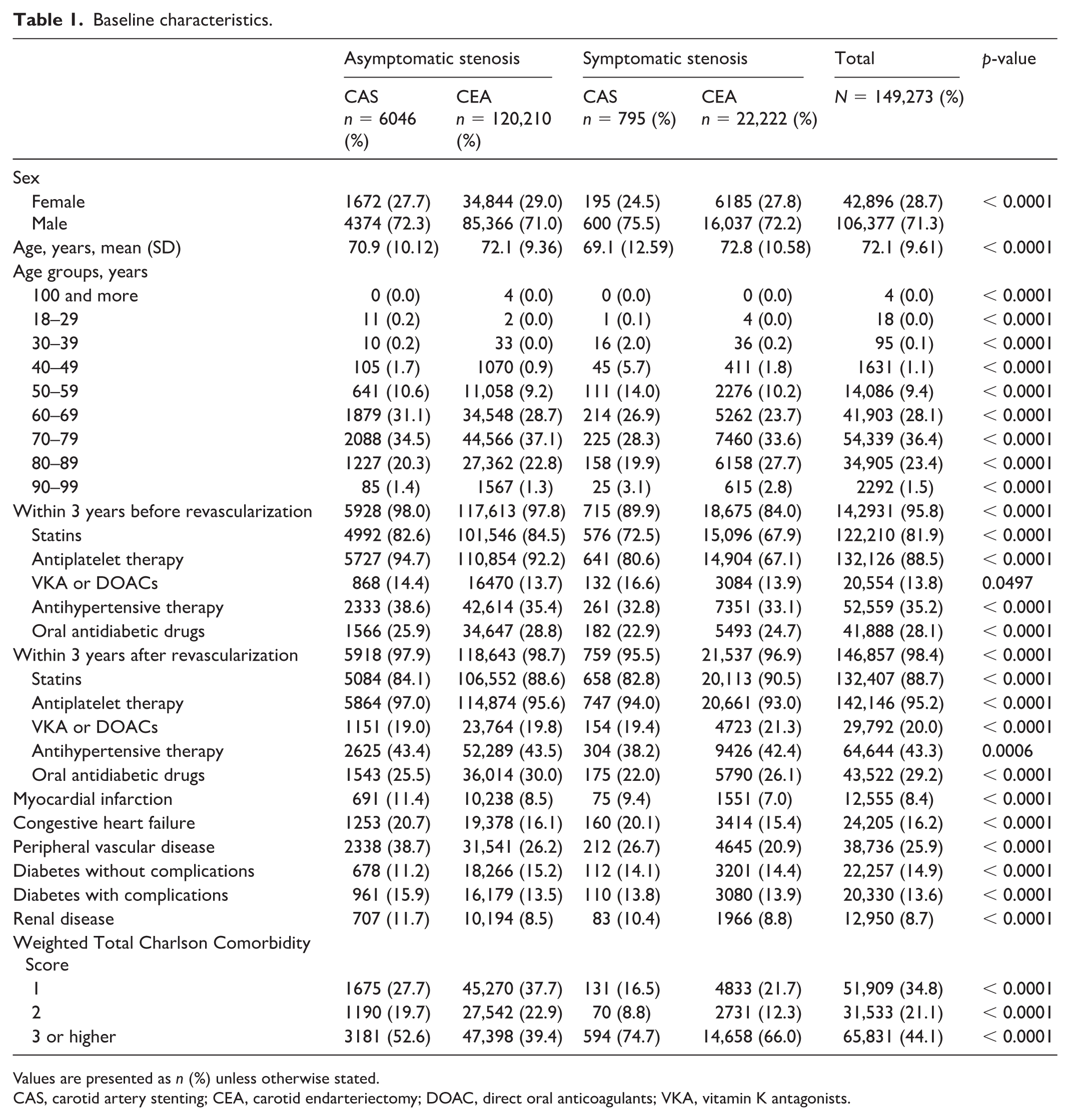
Values are presented as n (%) unless otherwise stated.
CAS, carotid artery stenting; CEA, carotid endarteriectomy; DOAC, direct oral anticoagulants; VKA, vitamin K antagonists.
Practices and annual trends
Regarding indication and type of revascularization, 84.6% of patients (n = 126,256) were asymptomatic and 15.4% (n = 23,017) were symptomatic (Figure 1). During the study period, CAS was performed in 4.6% (n = 6841) of patients, whereas CEA accounted for 95.4% (n = 142,432). In asymptomatic patients, 4.8% (n = 6046) received CAS and 95.2% (n = 120,210) received CEA; similarly, in symptomatic patients, 3.5% (n = 795) received CAS and 96.5% (n = 22,222) received CEA.
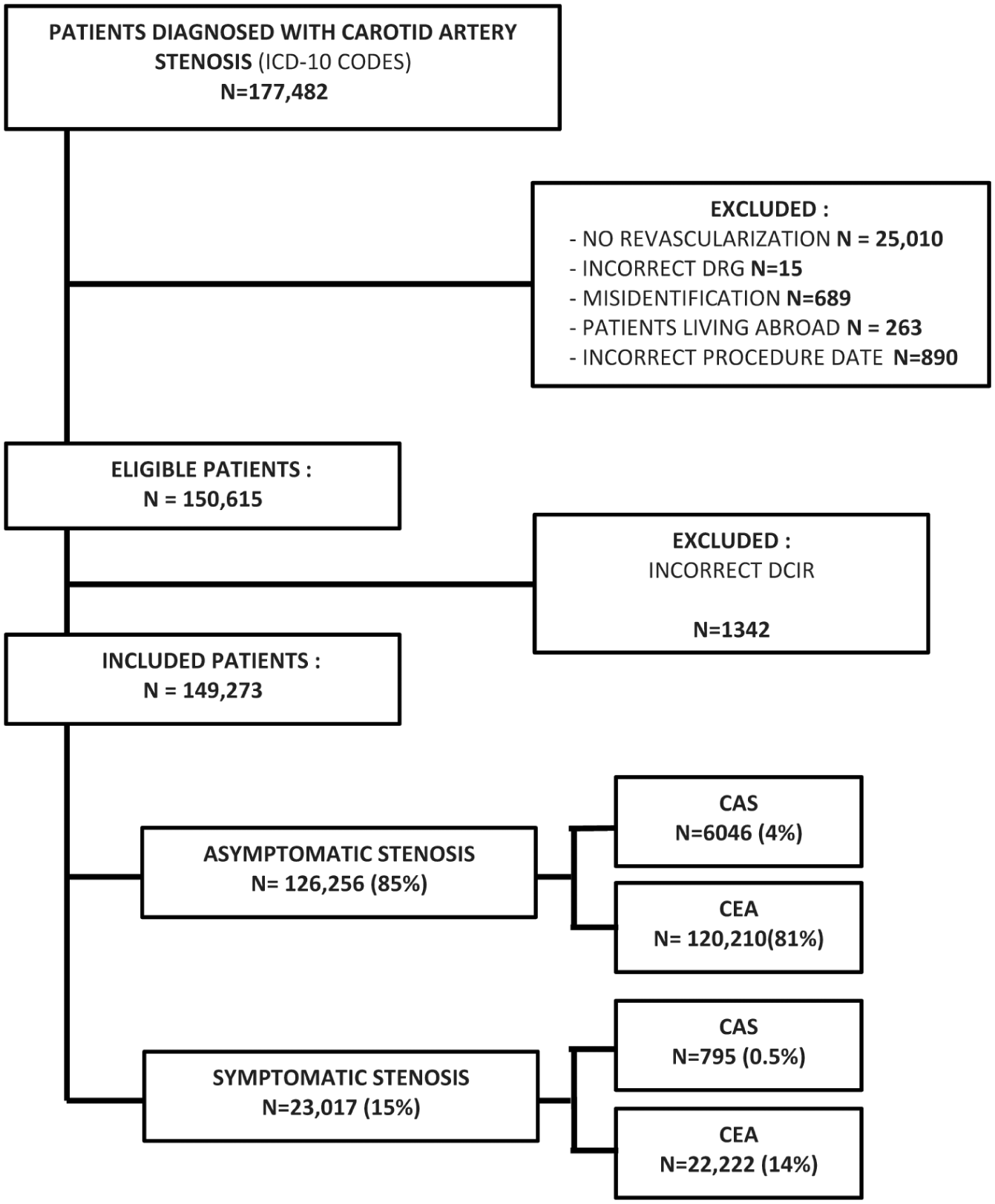
Flowchart of patient inclusion detailing those who underwent carotid revascularization for symptomatic or asymptomatic carotid stenosis from 2011 to 2020.
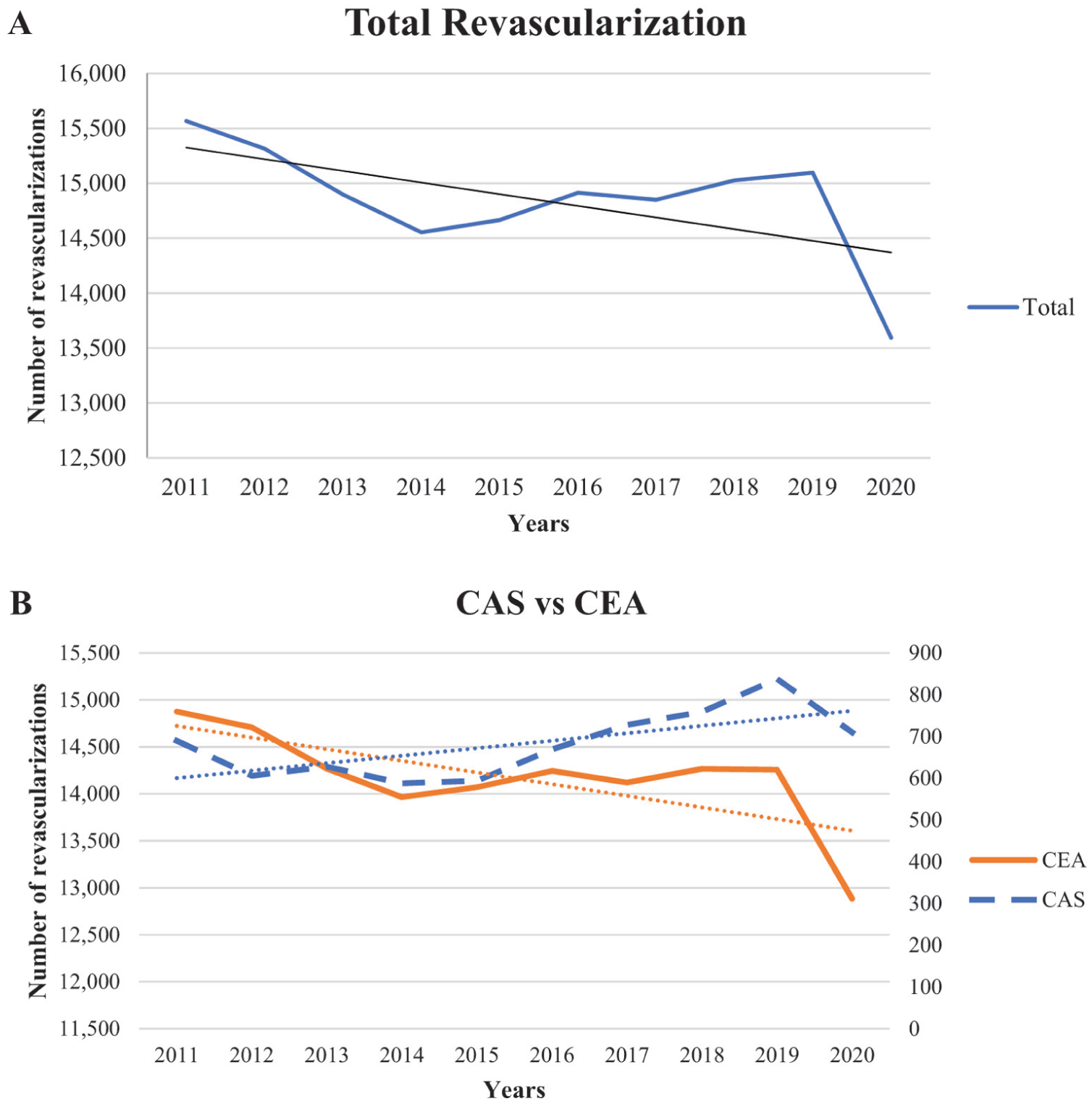
Over the 10-year study period, the annual number of carotid revascularization procedures evolved significantly, with variations observed in the relative use of CEA and CAS. Between 2011 and 2020, the overall volume of revascularization procedures declined by an average of 215 per year (Figure 2A). The overall volume of carotid revascularization procedures progressively declined, primarily driven by a reduction in CEA among asymptomatic patients (–2% per year). In contrast, procedures performed in symptomatic patients remained stable or slightly increased (+1.7% per year). Although CAS represented a small proportion of total procedures, its relative share increased over time. These findings reflect a gradual evolution in national practice patterns over the period 2011 to 2020 (Figure 2B). The distribution of procedures by type and by year is described in Supplemental Appendix 3.
Early postoperative results
At 30 days, the composite outcome of stroke (including TIA) or all-cause death occurred in 1.8% (n = 2275) of asymptomatic patients and 12.7% (n = 2922) of symptomatic patients (Table 2). Among asymptomatic patients, this outcome was significantly higher in those treated with CAS (3.2%, n = 195) compared with CEA (1.7%, n = 2080; p < 0.0001). In the symptomatic group, CAS was also associated with a higher rate (15.5%, n = 123) compared with CEA (12.6%, n = 2799). When considering stroke alone, the 30-day stroke rate was 2.3% (n = 140) after CAS and 1.0% (n = 1204) after CEA. This outcome occurred in 1.1% (n = 1344) of asymptomatic patients and 10.6% (n = 2436) of symptomatic patients.
Clinical outcomes in patients after CAS versus CEA stratified by symptomatic status.
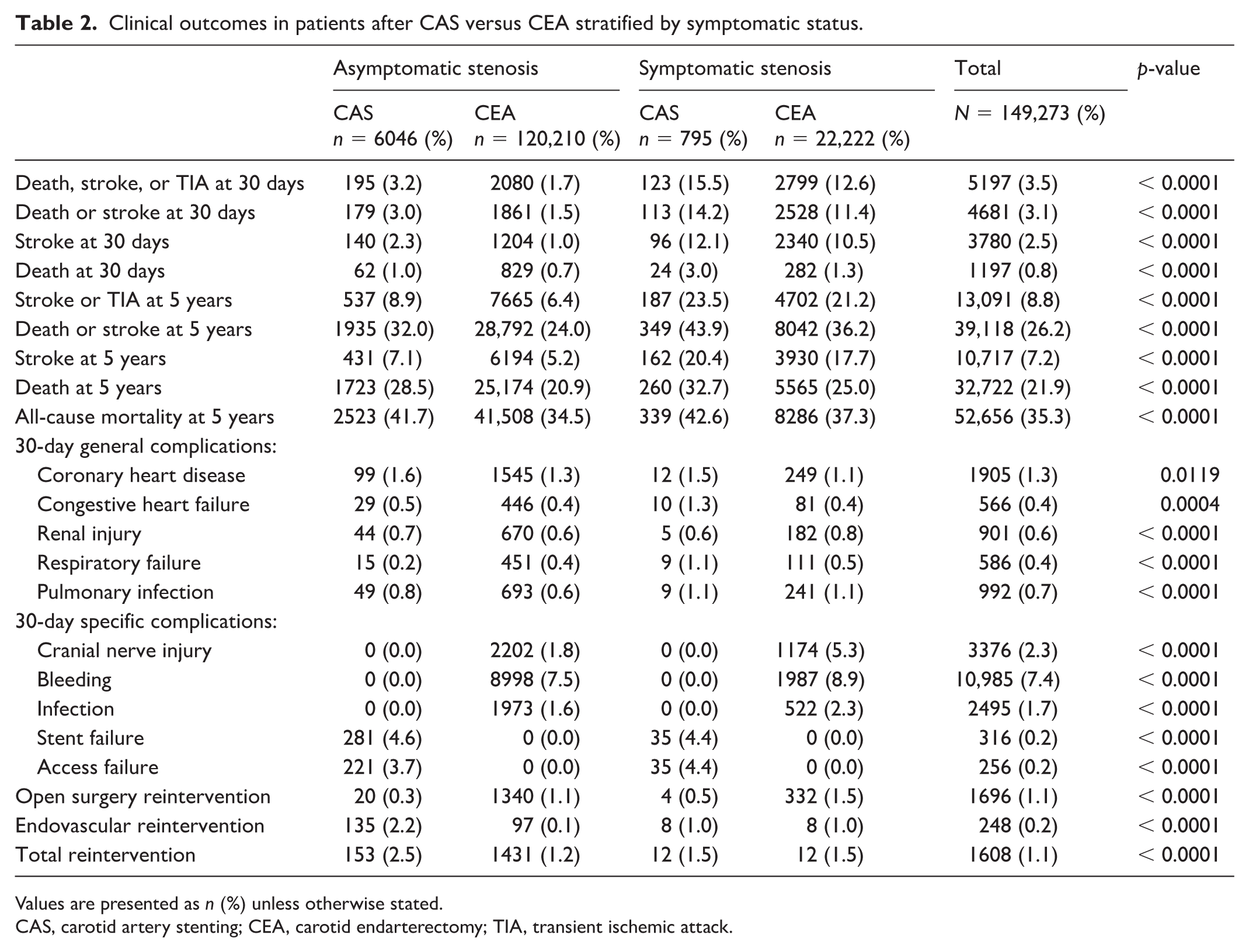
Values are presented as n (%) unless otherwise stated.
CAS, carotid artery stenting; CEA, carotid endarterectomy; TIA, transient ischemic attack.
After adjustment for baseline characteristics, CEA remained independently associated with a lower risk of 30-day stroke (adjusted odds ratio [OR] 0.65, 95% CI: 0.57–0.75) and 30-day stroke and/or death (adjusted OR 0.68, 95% CI: 0.60–0.77) compared with CAS (Table 3).
Multivariate analysis.
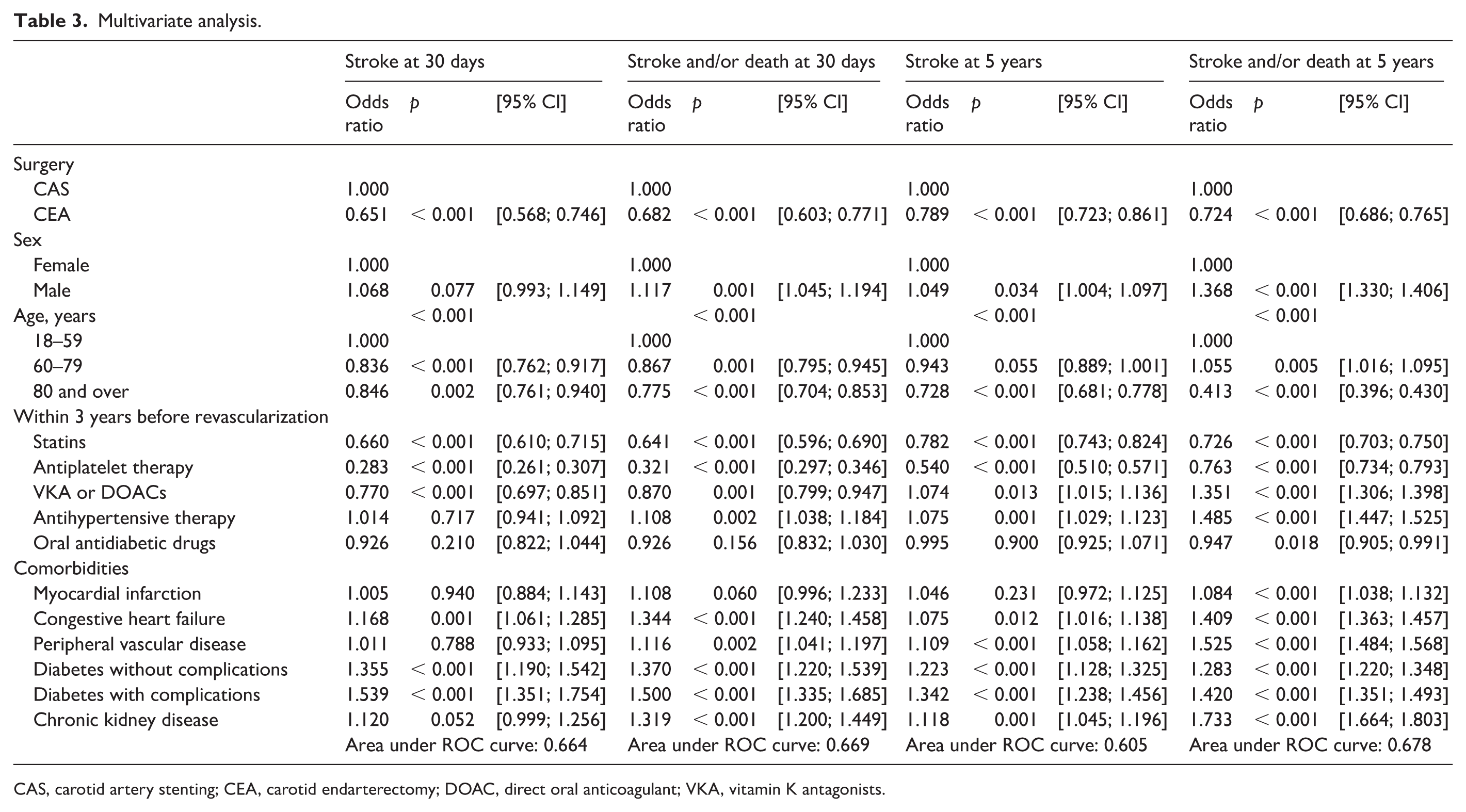
CAS, carotid artery stenting; CEA, carotid endarterectomy; DOAC, direct oral anticoagulant; VKA, vitamin K antagonists.
Regarding general complications within 30 days postprocedure, coronary insufficiency (defined as ischemic heart disease, including prior myocardial infarction, angina, or coronary revascularization) occurred in 1.3% (n = 1905) of patients, with significant differences between asymptomatic (1.3%, n = 1644) and symptomatic (1.1%, n = 261) patients, or between CAS and CEA (p < 0.001). The rate of other complications—including heart failure, acute kidney injury, respiratory failure, and pulmonary infection—was 2% (n = 3045) and similarly distributed across groups. For open surgical procedures, cranial nerve injury occurred more frequently in symptomatic patients (5.3%, n = 1174) compared with asymptomatic patients (1.8%, n = 2202). Bleeding and infection rates were similar across all groups. Endovascular access failure occurred in 3.7% (n = 256) of CAS procedures. The overall reintervention rate at 30 days was 1.1% (n = 1608), and it was higher after CAS (2.4%, n = 165) than after CEA (1.0%, n = 1443).
Late results at 5 years
At 5 years, the overall survival without stroke was 69.3% (n = 103,460). The rate of stroke or TIA was 6.5% (n = 8202) in asymptomatic patients and 21.2% (n = 4889) in symptomatic patients. The overall mortality rate was 35.3% (n = 52,656), which was higher in symptomatic patients (37.5%, n = 8625) than in asymptomatic patients (34.9%, n = 44,031). Mortality was significantly higher in patients treated with CAS compared with those treated with CEA (41.8%, n = 2862 vs 35.0%, n = 49,794) (Table 2). After adjustment for baseline characteristics, CAS was independently associated with a higher 5-year risk of stroke (adjusted OR 1.27, 95% CI: 1.16–1.38) and death/stroke (adjusted OR 1.38, 95% CI: 1.31–1.46) (Table 3).
Kaplan–Meier analysis showed lower 5-year overall survival in patients treated with CAS compared with CEA in both asymptomatic (71.5% vs 78.4%) and symptomatic groups (67.7% vs 74.9%) (log-rank p < 0.001). Kaplan–Meier curves were truncated when fewer than 10 patients remained at risk (Figure 3).

Kaplan–Meier curve for 5-year overall survival, by procedure and symptom status.
Stroke-free survival followed a similar trend, with a higher cumulative incidence of stroke or TIA in CAS-treated patients (asymptomatic: 8.7% vs 6.4%; symptomatic: 22.2% vs 20.8%). Kaplan–Meier and cumulative incidence curves are provided in Supplemental Figures S1 and S2.
Discussion
This study offers a unique, population-wide insight into real-world carotid stenosis management in France, revealing striking contrasts with current international trends. Over 85% of carotid revascularizations were performed in asymptomatic patients, whereas CAS remained a minor approach used primarily in high-risk profiles. By analyzing temporal trends, comorbidities, medication patterns, and outcomes at both 30 days and 5 years, this study not only confirms known disparities in practice but also quantifies them at an unprecedented national scale.
One of the most striking findings is the predominance of procedures performed in asymptomatic patients, who represented 85% of the cohort. This proportion is considerably higher than what has been observed in other countries. For example, Venermo et al. reported that only 60% of carotid procedures in the United States and 76% in Italy were performed in asymptomatic patients, and some Nordic countries reported rates close to 0%. 19 This discrepancy raises questions about the persistence of historical practices in France, despite a growing body of evidence favoring best medical therapy in this population.
Another major contribution of our study is the detailed comparison between CEA and CAS, both in symptomatic and asymptomatic settings. Although CAS represented only 4.6% of procedures, it was more frequently performed in patients with a high comorbidity burden, consistent with its indication for high surgical risk patients. Indeed, more than 50% of patients undergoing CAS had a CCI ⩾ 3, compared with 40% for CEA in asymptomatic cases, versus 66% and 75% for CAS and CEA, respectively, in symptomatic cases. This targeted use of CAS aligns with current European guidelines. 20
From a temporal perspective, this study provides valuable insight into national practice evolution over a decade, highlighting a progressive reduction in revascularization volume and a cautious increase in CAS use in selected populations. Suggesting a progressive but cautious adoption of endovascular approaches in selected indications. These trends mirror those reported in North America, where CEA volumes have declined over time, although CAS rates there remain higher than in France.21,22
Regarding postoperative outcomes, our results confirm that symptomatic patients face a higher perioperative risk, with a 30-day stroke or death rate of 12.7%, compared with 1.8% in asymptomatic patients. According to the 2023 ESVS guidelines, acceptable 30-day stroke/death rates should be below 3% in asymptomatic patients and below 6% in symptomatic patients. In our nationwide cohort, periprocedural risks after CEA were largely consistent with these benchmarks. However, 30-day stroke/death rates following CAS approached or exceeded recommended thresholds in certain subgroups, highlighting the importance of careful patient selection, operator expertise, and adherence to procedural standards in routine clinical practice. These figures emphasize the importance of timing and preoperative optimization. Notably, more than 16% of symptomatic patients in our cohort were not receiving optimal medical therapy prior to intervention, which may have contributed to worse outcomes. By contrast, asymptomatic patients were more frequently treated with statins and antiplatelet agents before surgery, reflecting a more structured preventive approach.
At 5 years, stroke or TIA occurred in 21.2% of symptomatic and 6.5% of asymptomatic patients. These rates must be interpreted in light of recent observational and randomized studies. For instance, Chang et al. reported a 5-year ipsilateral stroke rate of only 4.7% in medically managed patients with severe asymptomatic carotid stenosis, suggesting that invasive treatment may not offer substantial additional protection in selected cases. 5
Our findings are broadly consistent with those recently reported by Steinmetz et al., who also analyzed nationwide French data on carotid revascularization over a 10-year period. 23 Their study similarly highlighted the predominance of asymptomatic procedures and the higher 30-day stroke or death rate after CAS compared with CEA. However, our methodology offers several advantages. First, we used the SNDS database, which integrates both inpatient and outpatient data, allowing for more complete capture of medication use and long-term follow-up. In contrast, Steinmetz et al. relied exclusively on hospital discharge data (PMSI), limiting their ability to assess postdischarge outcomes or medication exposure. Second, our definition of symptomatic status included a 6-month lookback period, enhancing sensitivity, whereas their classification was restricted to diagnoses coded during the index hospitalization. Lastly, our study includes Kaplan–Meier-based 5-year outcomes and detailed temporal trends in treatment volume, providing a broader perspective on the long-term implications of current practice.
The role of CAS remains debated. Although randomized studies such as SAPPHIRE, EVA-3S, and SPACE have shown mixed results, its use has expanded in many countries, reaching up to 14% of procedures in the United States and 12.8% in Germany.9,24–27 In France, CAS remains underutilized but has shown a progressive increase over the decade, possibly reflecting growing confidence in its safety profile and improvements in endovascular devices and techniques. Nevertheless, in our cohort, CAS was associated with significantly higher perioperative stroke or death rates compared with CEA, both in symptomatic and in asymptomatic patients, which is consistent with prior meta-analyses. 20
Our study also highlights a paradoxical situation: symptomatic patients are more likely to experience poor outcomes, yet less likely to receive optimal medical treatment before intervention. This finding reinforces the need for better integration of pharmacologic strategies in the acute management of cerebrovascular disease. Studies have shown that statins and antiplatelet agents not only reduce stroke recurrence but may also improve functional outcomes. 28 The lower use of optimal medical therapy among symptomatic patients may partly explain their acute presentation. Suboptimal control of vascular risk factors may contribute to plaque instability and thromboembolic events, thereby precipitating neurological symptoms rather than merely reflecting healthcare disparities.
Several randomized trials have attempted to reassess the role of revascularization in asymptomatic carotid stenosis. The SPACE-2 trial failed to demonstrate superiority of CAS or CEA over best medical therapy, but was underpowered due to poor recruitment. 13 Similarly, the French ACTRIS trial, which aimed to compare CEA + medical therapy versus medical therapy alone, was prematurely terminated due to insufficient inclusion. 29 The recently published CREST-2 trials provide contemporary randomized evidence regarding the management of asymptomatic high-grade carotid stenosis. In CREST-2, carotid artery stenting combined with intensive medical therapy reduced the 4-year risk of periprocedural stroke or death or ipsilateral stroke compared with medical therapy alone, whereas carotid endarterectomy did not demonstrate a statistically significant benefit. 30 These results refine the interpretation of modern revascularization outcomes and highlight the importance of procedural safety and optimized medical therapy in asymptomatic patients.
Finally, our study has limitations. Although adjusted analyses were performed, residual confounding cannot be excluded given the observational nature of administrative data and the absence of anatomical and procedural variables. It is not possible to determine the laterality of stroke relative to the treated artery, which may have led to overestimation of stroke rates. Although medication exposure is recorded, actual patient adherence cannot be confirmed. Lastly, the observed decrease in procedures between 2019 and 2020 corresponds temporally to the COVID-19 pandemic, during which elective carotid interventions were widely deferred. No coding inconsistencies were identified upon data validation.
This large-scale study highlights the need to re-evaluate current practices regarding the management of asymptomatic carotid stenosis in France. In an era of increasingly effective medical prevention, the risk-benefit ratio of surgical intervention must be re-examined, particularly in patients with low annual stroke risk. The publication of the CREST-2 trial is a key milestone in determining whether carotid revascularization remains justified in this setting. In parallel, efforts should be made to promote systematic medical optimization prior to intervention, especially in symptomatic patients, and to encourage shared decision-making through multidisciplinary teams. The increasing use of CAS in high-risk patients is promising, but further studies are needed to refine selection criteria and optimize procedural safety. Finally, the SNDS database offers a unique opportunity to develop long-term follow-up models, including analyses of cognitive function, quality of life, and functional independence, which are currently lacking in carotid disease research.
Conclusion
This national cohort study confirms that carotid revascularization in France is predominantly performed in asymptomatic patients, often despite limited evidence of benefit in this group. CEA remains the main approach, whereas CAS is used selectively in high-risk profiles but carries higher perioperative risk. Symptomatic patients face greater complication rates and are less likely to receive optimal preoperative medical therapy, highlighting a gap in stroke prevention strategies. These results support the need for better patient selection, standardized care pathways, and stronger adherence to evolving evidence and guidelines.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X261442959 – Supplemental material for Carotid endarterectomy and stenting in France: A 10-year nationwide evaluation of practice and outcomes
Supplemental material, sj-docx-1-vmj-10.1177_1358863X261442959 for Carotid endarterectomy and stenting in France: A 10-year nationwide evaluation of practice and outcomes by Clement Willot, Maxime Dubosq-Lebaz, Soxna Faatimatu Kine Fall, Xavier Lenne, Thomas Mesnard, Benjamin O Patterson, Amelie Bruandet and Jonathan Sobocinski in Vascular Medicine
Supplemental Material
sj-docx-2-vmj-10.1177_1358863X261442959 – Supplemental material for Carotid endarterectomy and stenting in France: A 10-year nationwide evaluation of practice and outcomes
Supplemental material, sj-docx-2-vmj-10.1177_1358863X261442959 for Carotid endarterectomy and stenting in France: A 10-year nationwide evaluation of practice and outcomes by Clement Willot, Maxime Dubosq-Lebaz, Soxna Faatimatu Kine Fall, Xavier Lenne, Thomas Mesnard, Benjamin O Patterson, Amelie Bruandet and Jonathan Sobocinski in Vascular Medicine
Footnotes
Acknowledgements
An editorial by Bellamkonda et al. 31 accompanies this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.