
Abstract
Randomized clinical trials are often criticized for enrolling patients who may not represent everyday practice. Trial participants are presumed to be more adherent, more intensively managed, and surrounded by a level of guideline‑directed medical therapy (GDMT) that is difficult to replicate in routine care.1–4 This concern has shaped much of the debate around asymptomatic carotid stenosis, where the benefit of revascularization is thought to hinge on the quality of background medical therapy. If trial patients receive unusually optimized care, how confidently can clinicians apply the results to the broader population? The publication of CREST‑2 (ClinicalTrials.gov Identifier: NCT02089217) 5 offers an important counterpoint to this longstanding narrative.
CREST‑2 5 was designed in an era when modern lipid‑lowering agents, antihypertensive strategies, and diabetes therapies should have steadily reduced baseline stroke risk. In such a landscape, the intensity of GDMT becomes central to interpreting any revascularization trial. Because CREST‑2 incorporated structured risk‑factor control and emphasized adherence to contemporary medical therapy, many assumed the study would enroll a highly optimized cohort—precisely the type of population that fuels concerns about limited generalizability. Whether CREST‑2 participants were truly receiving ‘trial‑level’ medical therapy is therefore essential for understanding how well its findings reflect the patients who undergo carotid revascularization in routine practice.
A meaningful test of external validity is whether trial participants resemble the patients who actually undergo the same procedures in real‑world settings. The TriNetX network, which aggregates data from millions of patients across diverse health systems, provides an opportunity to examine this alignment. Using relevant International Classification of Diseases, Tenth Revision (ICD‑10) and Current Procedural Terminology (CPT) codes, we identified a contemporary cohort of patients undergoing carotid revascularization and compared their baseline characteristics with those reported in CREST‑2 (Table 1). The query included data from January 1, 2016 to January 1, 2026, and all variables were analyzed as reported because TriNetX does not provide item‑level missingness. Standardized mean differences were used to quantify differences between groups: values < 0.1 are generally considered negligible, 0.1–0.2 small, and > 0.2 indicative of potentially meaningful imbalance. To align with the CREST‑2 population, we restricted the TriNetX cohort to patients with carotid stenosis and no prior cerebral infarction or transient ischemic attack (TIA) symptoms. Among these asymptomatic patients, we identified those who subsequently underwent carotid stenting or endarterectomy. This retrospective study was exempt from institutional review board review because it used only nonidentifiable data.
Comparison of baseline characteristics of the CREST-2 population and TriNetX.
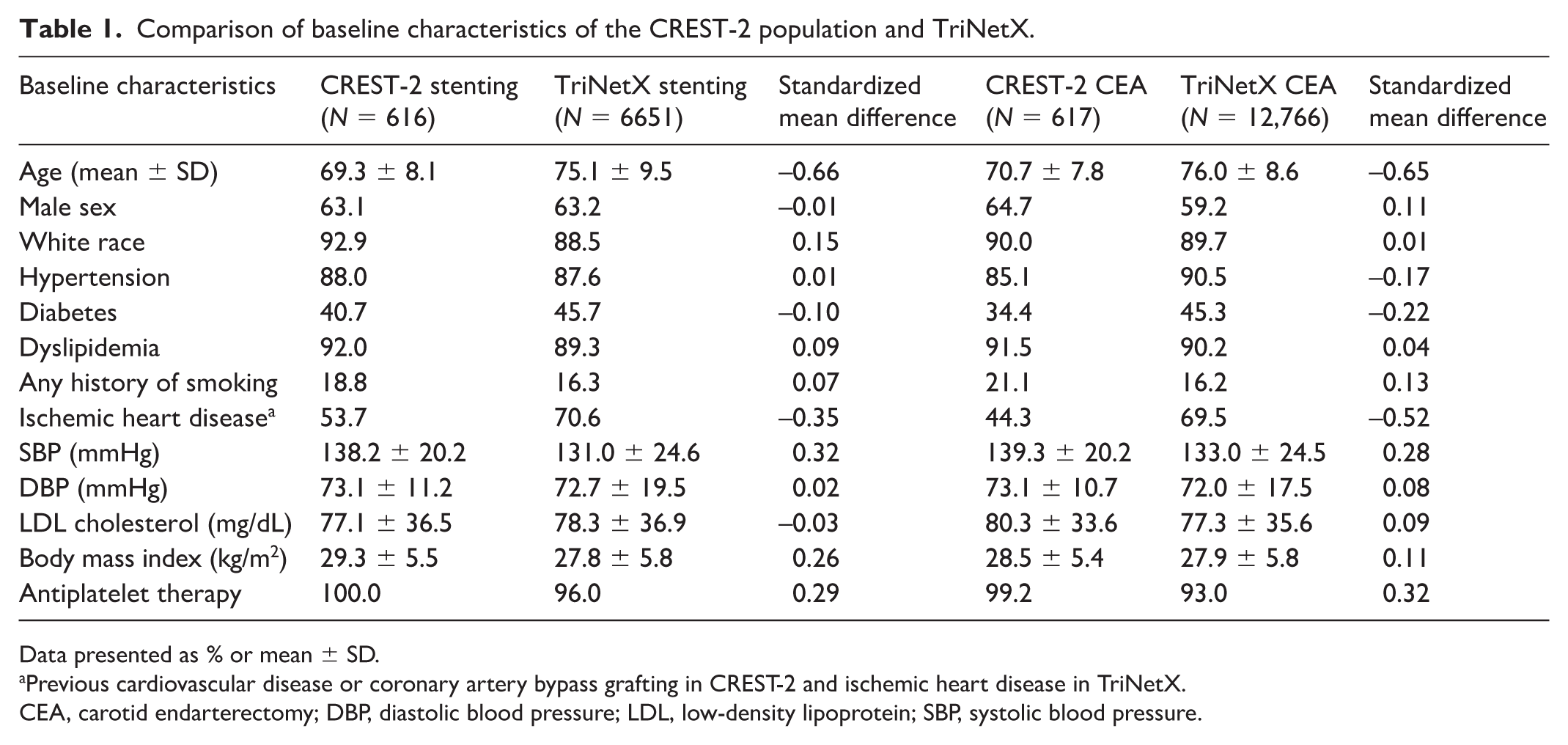
Data presented as % or mean ± SD.
Previous cardiovascular disease or coronary artery bypass grafting in CREST-2 and ischemic heart disease in TriNetX.
CEA, carotid endarterectomy; DBP, diastolic blood pressure; LDL, low-density lipoprotein; SBP, systolic blood pressure.
What emerges from this comparison is a far narrower gap than many would have predicted. Across multiple domains relevant to GDMT, including traditional vascular risk factors, blood pressure control, lipid levels, and antiplatelet use, the CREST‑2 cohort aligned reasonably well with patients treated in routine practice. It should be noted that these comparisons reflect baseline characteristics only and do not assess medication intensity, adherence, or structured risk‑factor management. The real‑world population was less optimized in a few areas: mean age was higher in the TriNetX cohort, diabetes was more prevalent, and ischemic heart disease appeared more common. As noted in Table 1, CREST‑2 defined ischemic heart disease as prior cardiovascular disease or coronary artery bypass grafting (CABG), whereas TriNetX used the broader ICD‑10 category, contributing to the higher prevalence. The small differences in age and prevalence of diabetes in the TriNetX population likely represent a higher risk cohort of patients in the general population with asymptomatic carotid disease. Taken together, these differences are modest and expected, and they sit within a broader pattern showing that CREST‑2 participants generally resemble the patients who undergo carotid revascularization in everyday practice.
These findings should be interpreted with appropriate caution. This comparison evaluates baseline characteristics only; clinical outcomes were not analyzed. Real‑world data are inherently limited by heterogeneity in coding practices, missingness, and the absence of adjudication. Nonetheless, the overall pattern is consistent: CREST‑2 does not represent an unusually optimized or atypical cohort. Instead, its participants reflect the contemporary population of patients undergoing carotid revascularization, including those with substantial comorbidity burdens.
This alignment strengthens confidence in the applicability of CREST‑2’s results. When a randomized trial enrolls patients whose baseline characteristics and medical therapy resemble those encountered in routine care, its findings carry greater relevance for everyday decision-making. Although no single comparison can fully resolve questions of external validity, the convergence between CREST‑2 and real‑world cohorts offers meaningful reassurance to clinicians weighing revascularization for asymptomatic carotid stenosis. Rather than reinforcing the familiar critique that trial populations are too idealized, CREST‑2 provides an example of a contemporary vascular trial whose participants genuinely reflect the patients seen in practice.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mehdi Shishehbor was a site Principal Investigator for the CREST-2 trial, and he serves as a global advisor for Boston Scientific, Medtronic, Abbott Vascular, Inquis, Advanced NanoTherapies, and Inari. Ashkan Yahyavi has no conflicts to report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.