
Abstract
Introduction:
Supervised exercise training (SET) is recommended as first-line therapy for symptomatic peripheral artery disease (PAD), but pain and limited tolerance often restrict the effective training dose. Eccentric exercise, such as downhill walking, elicits lower metabolic and cardiovascular responses and may represent a viable alternative to traditional walking. This case report describes the feasibility and physiological and functional effects of a 12-week downhill-walking SET program in a patient with symptomatic PAD.
Methods:
A 61-year-old man with symptomatic PAD completed a 12-week downhill-walking SET program performed at a preferred walking speed with progressively increasing negative slopes (−4% to −14%). Pre- and post-SET assessments included a graded treadmill test with near-infrared spectroscopy of calf muscle oxygenation, a 6-minute walk test, and lower-limb functional performance tests.
Results:
Following SET, pain-free (+6%) and maximal (+29%) walking distances improved. These changes were accompanied by reduced calf muscle oxygen desaturation during exercise, an enhanced calf muscle oxygenation overshoot at exercise onset, and faster postexercise reoxygenation. Lower-limb functional performance improved (20−25%), and the time to pain relief after walking tests was reduced (–46%), yet the 6-minute walking distance remained unchanged.
Conclusion:
This case report describes the implementation of a downhill-walking SET protocol in a patient with symptomatic PAD. The intervention was feasible and was accompanied by changes in walking performance, muscle oxygenation, and functional measures. These observations highlight the potential of an eccentric-based walking approach and support further investigation of this protocol in larger studies involving patients with PAD.
Keywords
Introduction
The efficacy of supervised exercise training (SET) in symptomatic peripheral artery disease (PAD) is well established and strongly recommended as first-line therapy.1,2 Walking is the most used and investigated training modality; 2 however, comorbidities and exercise-induced pain limit participation in a substantial proportion of patients. In those with severe claudication, walking sessions often consist of brief exercise bouts separated by prolonged rest, thereby limiting the overall effective dose of exercise. This underscores the need for alternative approaches.
Eccentric (ECC) exercise elicits physiological and perceptual responses that may offer a promising alternative therapeutic approach for patients with PAD. We recently demonstrated that, when matched for mechanical work, a functional ECC exercise (stair descending) induced lower calf muscle oxygen desaturation—reflecting reduced exercise-induced ischemia—compared with concentric exercise. 3 This was associated with lower claudication pain, perceived exertion, and cardiovascular responses compared with concentric exercise. 3
If these responses translate to walking, downhill walking could enable longer exercise bouts and a higher cumulative training dose. Moreover, steep negative slopes may allow high mechanical loading with limited cardiovascular stimulation, providing an effective neuromuscular stimulus that is particularly relevant for this population. 2
We present the first case of a man with symptomatic PAD participating in 12-week downhill-walking SET, illustrating the feasibility and practical implementation of this ECC exercise-based training approach.
Patient information
The patient is a 61-year-old White man with intermittent claudication of the right calf (stage IIb Leriche-Fontaine) and a history of endovascular and surgical revascularization of the right lower limb. He is known to have multiple cardiovascular risk factors. His vascular history and the information available prior to SET are summarized in Table 1.
Clinical characteristics and vascular history of the patient prior to supervised exercise training.
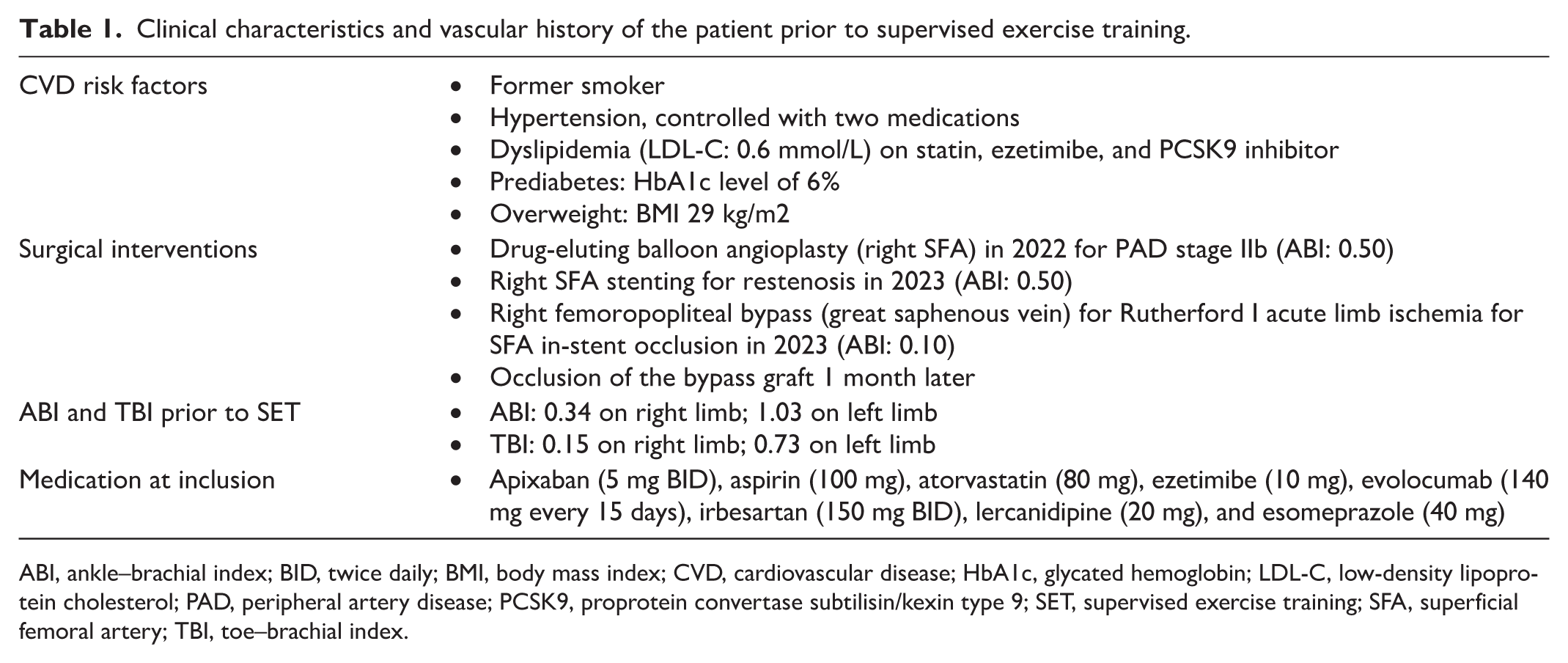
ABI, ankle–brachial index; BID, twice daily; BMI, body mass index; CVD, cardiovascular disease; HbA1c, glycated hemoglobin; LDL-C, low-density lipoprotein cholesterol; PAD, peripheral artery disease; PCSK9, proprotein convertase subtilisin/kexin type 9; SET, supervised exercise training; SFA, superficial femoral artery; TBI, toe–brachial index.
Assessments
Assessments were performed prior to and following SET.
Treadmill test
The patient performed a graded treadmill test to determine the pain-free (PFWD) and maximal (MWD) walking distances. 2 Then, the patient was instructed to sit down immediately and indicate when the claudication pain had completely disappeared. During the treadmill test, calf muscle oxygenation was assessed via near-infrared spectroscopy (NIRS; PortaMon, Artinis, The Netherlands). The NIRS probe was placed over the lateral gastrocnemius muscle of the most symptomatic leg. Calf muscle oxygen saturation (StO2) was continuously recorded throughout the test. Resting StO2 was measured over a 3-minute period in the seated position (hips and knees flexed at 90°). The 50% reoxygenation time (Treox 50%)—the time (in seconds) required for calf muscle StO2 to reach 50% of the recovery toward baseline from the value measured at the end of the test—was also recorded.
The 6-minute walk test
The patient was instructed to walk as far as possible within 6 minutes to determine the 6-minute walking distance (6MWD). 4 Following the test, the patient sat down and reported when the claudication pain resolved.
Lower-limb function
The patient was asked to ascend and descend a 12-step staircase as quickly as possible. 5 The test was performed twice, and the average time of the two attempts was recorded. Finally, the patient performed as many full chair stands as possible within 30 seconds. 5
Downhill treadmill walking supervised exercise training (SET)
Exercise training consisted of 36 supervised sessions, three times a week, over a 12-week period 2 (Table 2). Training sessions lasted 35–50 minutes and were performed at the participant’s preferred walking speed (PWS). This was determined by gradually increasing or decreasing the treadmill speed until the participant subjectively identified a comfortable walking pace; the final PWS was calculated as the average of two trials. 6 The patient’s PWS during training was 2.9 km·h–1.
Supervised treadmill downhill-walking exercise training protocol.
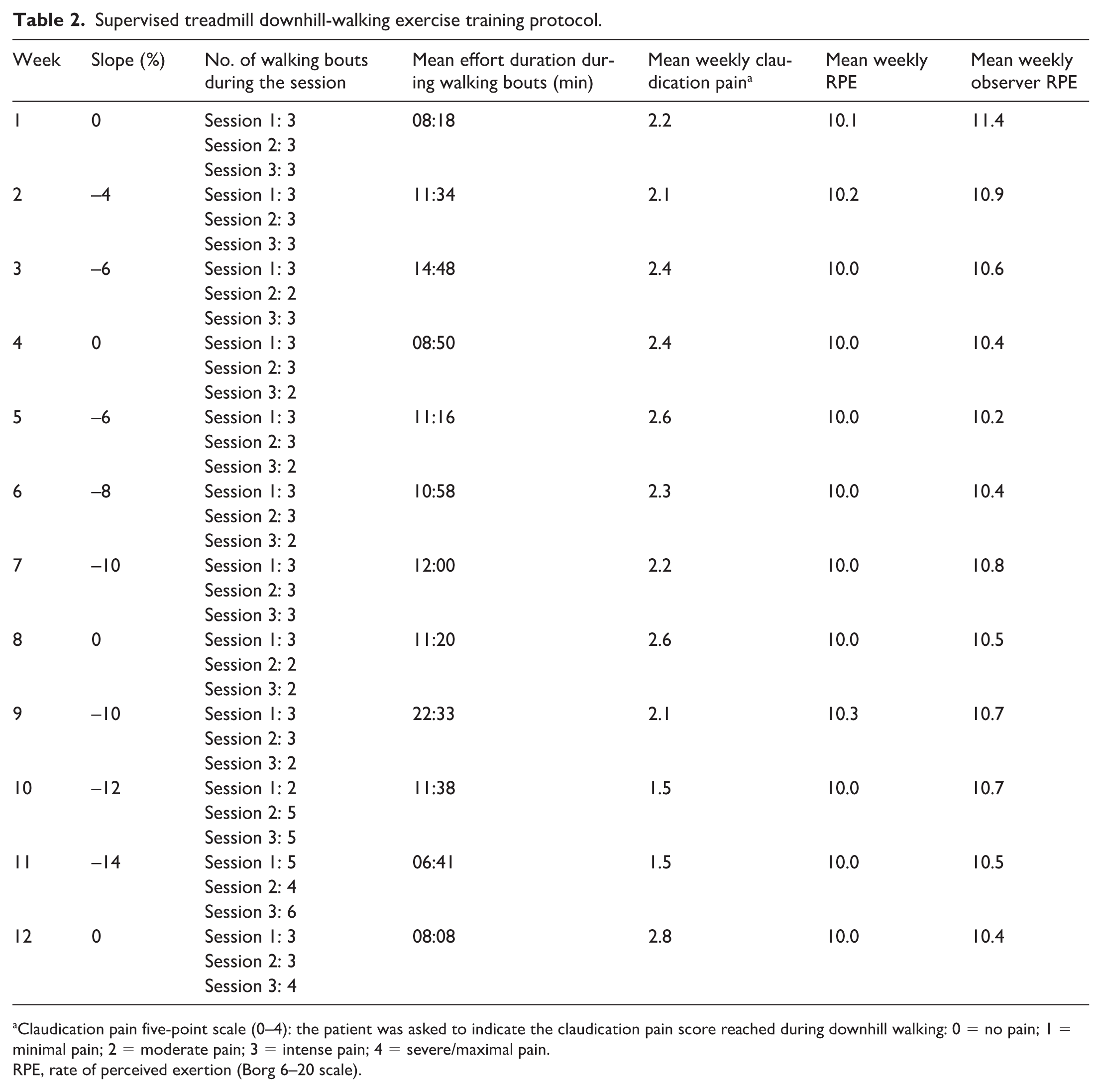
Claudication pain five-point scale (0–4): the patient was asked to indicate the claudication pain score reached during downhill walking: 0 = no pain; 1 = minimal pain; 2 = moderate pain; 3 = intense pain; 4 = severe/maximal pain.
RPE, rate of perceived exertion (Borg 6–20 scale).
Training was performed on a motorized treadmill (T150; COSMED, Rome, Italy) equipped with a reverse belt, capable of generating downhill walking through adjustable negative slopes. Negative slopes ranged from −4% to −14%. For safety, the patient wore a harness attached to an overhead support system (Figure 1).

Example of the treadmill setup used for downhill-walking supervised exercise training. The participant wore a safety harness connected to an overhead support system to prevent falls.
The training program followed a progressive block periodization model, consisting of three 4-week blocks of training. Each block was composed of 3 weeks of progressive increases in mechanical load. The fourth week of training was characterized by a decrease in mechanical load (level walking). Exercise intensity was systematically assessed during training sessions using the Borg scale, from both patient and observer perspectives, 7 together with claudication pain intensity. 2
Results
The patient successfully completed the entire training program, for a total of 36 sessions, with no adverse events reported. Downhill walking was well tolerated and allowed longer continuous walking bouts compared with level walking conditions, except in week 11, when additional bouts were introduced to allow longer recovery due to increased mechanical load (Table 2). Claudication pain decreased with steeper slopes, with exercise intensity remaining low across all declines (Table 2).
Following the training period, improvements were observed in treadmill walking performance (PFWD and MWD) and in lower-limb functional tests (Table 3). The 6MWD remained unchanged; however, the time required for claudication pain to completely resolve after the test was shorter compared with baseline (Table 3).
Walking and functional performance prior and following the downhill-walking training program.
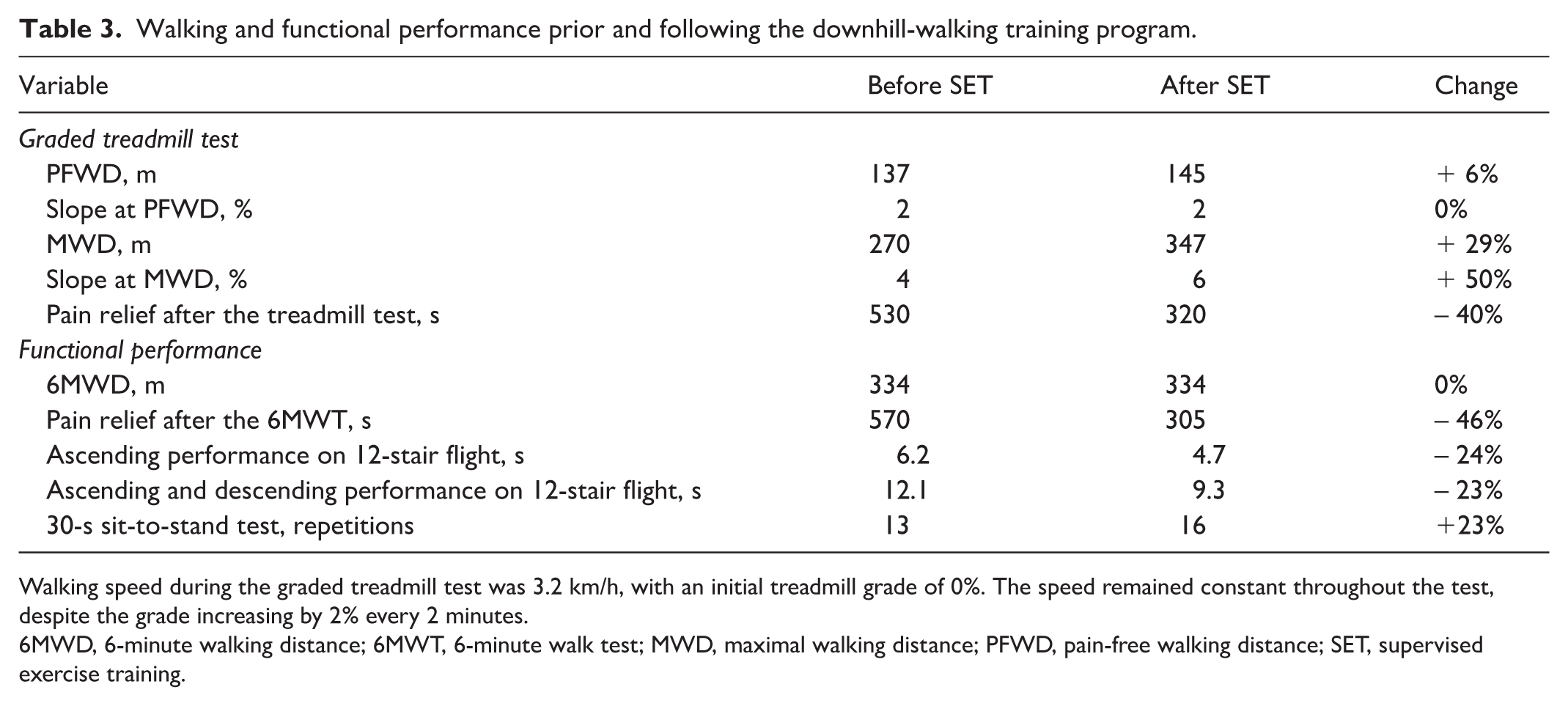
Walking speed during the graded treadmill test was 3.2 km/h, with an initial treadmill grade of 0%. The speed remained constant throughout the test, despite the grade increasing by 2% every 2 minutes.
6MWD, 6-minute walking distance; 6MWT, 6-minute walk test; MWD, maximal walking distance; PFWD, pain-free walking distance; SET, supervised exercise training.
Following SET, calf muscle StO2 increased at the initiation of exercise (overshoot), and a lower calf muscle oxygen desaturation was observed compared with the pre-SET condition (Supplemental Figure S1). A faster muscle reoxygenation time (Treox 50%) was also observed (Figure S1).
Discussion
This case report describes the implementation of a downhill-walking SET protocol in a patient with symptomatic PAD. The primary aim was to explore the feasibility and practical application of an ECC-based walking intervention in a clinical context where conventional walking modalities were poorly tolerated.
Downhill walking allowed a greater exercise dose than traditional level or uphill walking, which the patient could barely tolerate at a 3–4% positive slope due to symptom limitation. Very steep negative slopes (−14%) produced high mechanical loading with low cardiovascular stimulation and perceived exertion, but the longest bouts were observed between −6% and −10%. The patient poorly tolerated the −14% slope during and after training, indicating that such extreme grades may compromise feasibility despite their theoretical mechanical advantages. These findings suggest that moderate downhill grades may optimize the balance between exercise dose and adherence. Future studies should determine whether a clinical benefit is primarily achieved by extending bout duration at moderate slopes or by increasing the slope with shorter bouts. Such research should rigorously assess tolerability and safety as central drivers of clinical effectiveness.
Within this practical framework, the patient’s treadmill performance, functional measures, and muscle oxygenation were monitored to document preliminary responses to this innovative exercise training approach. Following the intervention, the patient demonstrated longer treadmill walking time, improvements in functional performance, and faster pain relief. The improvements in treadmill performance and pain relief following SET were accompanied by a greater calf muscle StO2 increase at the initiation of exercise (overshoot), reduced oxygen desaturation during exercise (indicating less ischemia), and faster postexercise reoxygenation compared with pre-SET, potentially reflecting microvascular adaptations. 8 Improvements were also noted in lower-limb neuromuscular function, consistent with prior reports. 9
It is important to consider potential limitations and safety issues associated with ECC exercise, particularly in clinical populations. ECC exercise may induce delayed onset muscle soreness, transient reductions in force, and a limited range of motion due to local inflammation and connective tissue damage. 10 These responses are usually mild and resolve within a few days, but unaccustomed loading could lead to more pronounced muscle damage. Careful progression and monitoring are therefore highly recommended.
Overall, this case report describes the feasibility of implementing a downhill-walking SET program as an ECC training modality in a patient with symptomatic PAD. Although improvements in functional outcomes were observed, the single-case design precludes any conclusions regarding clinical effectiveness. Further studies, including controlled trials, are required to determine the potential clinical relevance of downhill-walking interventions in patients with PAD.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X261445927 – Supplemental material for Downhill-walking exercise training in a patient with symptomatic peripheral artery disease: A case report
Supplemental material, sj-docx-1-vmj-10.1177_1358863X261445927 for Downhill-walking exercise training in a patient with symptomatic peripheral artery disease: A case report by Stefano Lanzi, Anina Pousaz, Marco Fresa, Lucia Mazzolai and Davide Malatesta in Vascular Medicine
Footnotes
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.