
Abstract

Keywords
Pulmonary embolism (PE) remains a leading cause of cardiovascular morbidity and mortality, with clinical presentations spanning a wide spectrum of risk profiles. 1 Over the past decade, the expanding availability of catheter-based therapies has transformed PE management, requiring nuanced patient triage and clinical acumen to provide optimal therapies. 2 To address this need in care, pulmonary embolism response teams (PERTs) have emerged as a multidisciplinary and systems-based solution, with a goal of integrating subspecialized clinical expertise and improving patient outcomes. PERTs aim to provide real-time collaboration of core experts across pulmonary/critical care, cardiology, vascular medicine, emergency medicine, and interventional disciplines, allowing for tailored management strategies that extend beyond anticoagulation alone. 3 Since the inception of PERTs in 2012, 2 adoption has expanded rapidly across academic and community centers. 2 However, due to variance in geographical and institutional resources, PERT programs remain heterogeneous in composition, 4 potentially contributing to disparities in treatment options. 5
In this issue of Vascular Medicine, the study by Nolan and colleagues 6 adds to the growing body of literature on the variability of PERT specialists in the treatment of patients with PE. This was a single-center, retrospective evaluation of patient outcomes in those managed with mechanical thrombectomy with either interventional radiology or vascular surgery. Over the course of 3.5 years, a total of 76 patients underwent intervention, with nearly half deemed to have high-risk PE. Though there are some differences in the time-to-intervention and procedure duration, the overall 30-day mortality, procedural complications, and major adverse outcomes between the two subspecialties are similar. Limited data on 6-minute walk testing at follow-up also showed no difference. The authors should be lauded for the first-of-its kind evaluation of subspeciality-specific outcomes using mechanical thrombectomy devices for patients with PE. The study also highlights an important strategy to limit physician call burden and encourage multidisciplinary collaboration across procedural specialties at a single institution.
However, there is a notable absence of comparison to interventional cardiology subspecialists included in this analysis, likely due to local practice patterns and institutional infrastructure. 6 Trends in practice patterns reflect increasing involvement of interventional cardiologists in the management of PE, particularly in academic centers. 7 Interventional cardiologists may bring a unique and relevant skill set to the management of high-risk PE, grounded in formal training in cardiovascular hemodynamics, right ventricular (RV) physiology, and the pathophysiology of acute RV failure. 8 Interventional cardiology fellowship training emphasizes invasive hemodynamic assessment, interpretation of pressure-flow relationships, and rapid decision-making in states of cardiogenic shock—core elements of high-risk PE management. 8 These specialists routinely manage patients with acute circulatory collapse, including the use of invasive monitoring, vasoactive therapies, and mechanical circulatory support, all of which are frequently required in patients with massive and intermediate-high-risk PE. 9 This training background aligns closely with the central determinants of morbidity and mortality in acute PE—namely RV dysfunction, elevated pulmonary vascular resistance, and impaired systemic perfusion—supporting the role of interventional cardiology within multidisciplinary PERTs at experienced centers. 10
Representation of interventional cardiologists in future studies will provide evidence to support the comprehensive multidisciplinary representation that PERTs seek to achieve. Consistent with 2026 pulmonary embolism guideline recommendations, PERTs should incorporate multidisciplinary expertise—including interventional cardiology, interventional radiology, vascular surgery, and pulmonary/critical care—to optimize hemodynamic assessment and support timely, individualized decision-making for patients with high-risk PE. 11 Multidisciplinary expertise is particularly relevant when procedural decisions may influence hemodynamic stability. Contemporary recommendations advise minimizing general anesthesia in high-risk PE due to its potential to worsen RV dysfunction through decreased sympathetic drive and positive-pressure ventilation. 12 In this context, the relatively high use of general anesthesia in this study invites further examination of sedation strategies, particularly in light of emerging data on the vulnerability of the failing right ventricle. Inclusion of specialists with formal training in invasive hemodynamics may influence such procedural decisions and merits consideration in future evaluations of PERT structure.
The issue of training and standardization is particularly relevant to the evolving role of proceduralists within the PERT framework. An underappreciated challenge in the current PERT landscape is the lack of uniform training and competency expectations. 13 Subspecialties may vary widely in their training in catheter-based interventions and hemodynamic support options, with exposure limited by institutional limitations on equipment availability. This is further demonstrated in this study, as the authors noted both interventional radiology and vascular surgery had independent training pathways for PE management, without inter-specialty training or proctoring to ensure uniform delivery of care. This highlights a prominent gap in the lack of formalized training guidelines for PE triage and management for proceduralists.
The geographical variability of subspeciality management of PE is unlikely to diminish. Given differences in training exposures based on regional availability, new operators coming into practice may not have been exposed to PE management at their training institution. Creating a uniform curriculum for all fellows, regardless of subspeciality, will be pertinent to deliver uniform care to patients with PE regardless of geography. Training should span 6 to 12 months, as case variability may limit exposure to truly high-risk and catastrophic PE cases. Core components of such training should include PERT triage calls, clinical evaluation of patients with PE according to best practices guidelines, recognition of when to choose to do intervention and what type, identification of when hemodynamic support is needed, reducing the risk and management of procedural complications, recognition of the effects of various medications on hemodynamics, application of proper follow-up, and determination of long-term anticoagulation (Table 1).
Core elements of an integrated training program for pulmonary embolism proceduralists.
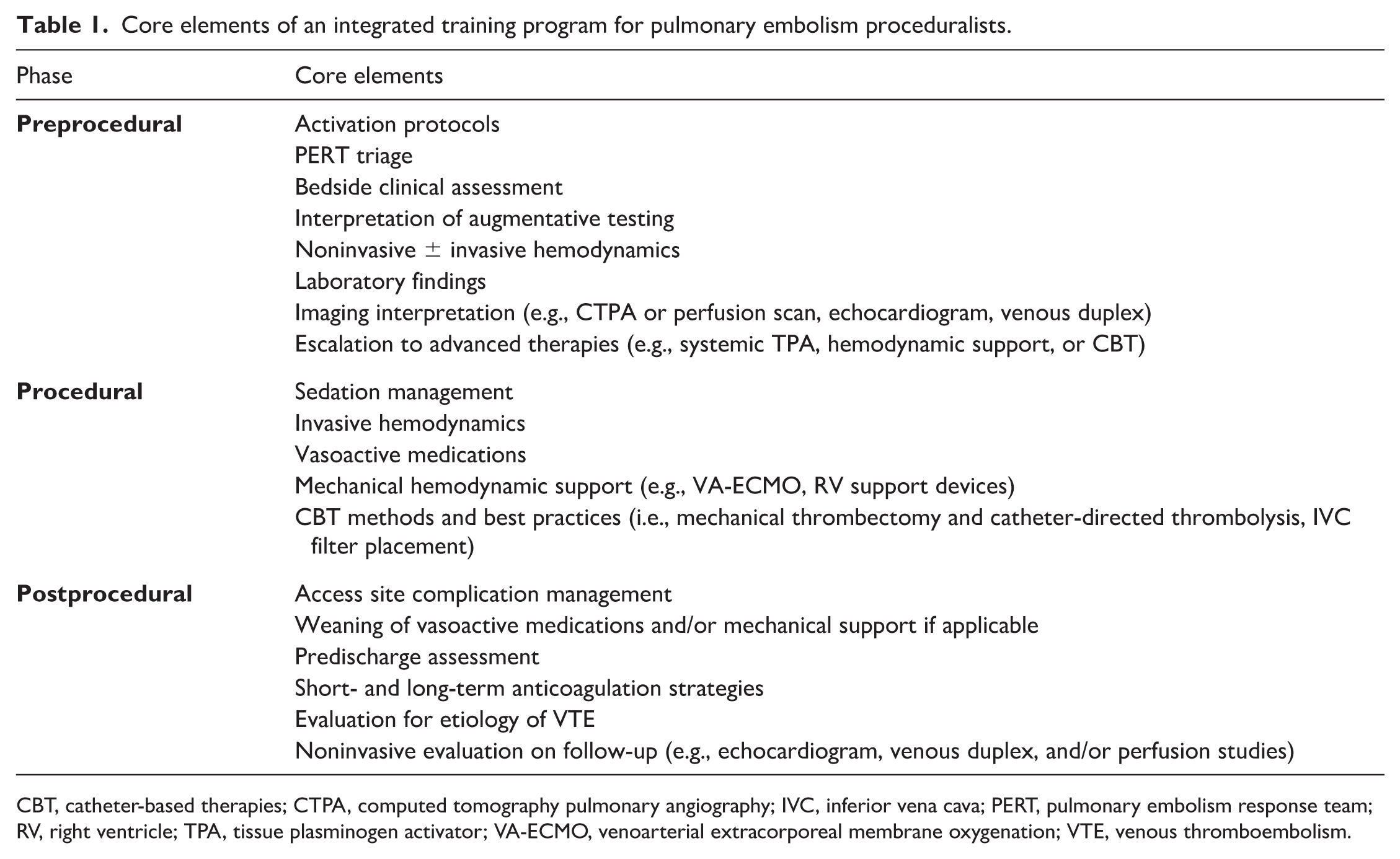
CBT, catheter-based therapies; CTPA, computed tomography pulmonary angiography; IVC, inferior vena cava; PERT, pulmonary embolism response team; RV, right ventricle; TPA, tissue plasminogen activator; VA-ECMO, venoarterial extracorporeal membrane oxygenation; VTE, venous thromboembolism.
As PERT models continue to evolve, standardization of team structure and PE-specific training pathways will be essential. Establishing consensus recommendations on team composition, competency benchmarks, and quality measures could promote greater consistency and reliability of care across diverse practice settings. Such models may be particularly valuable for community hospitals, where rapid access to specialized input can influence early management decisions with downstream consequences. A model of interdisciplinary PERT calls may be necessary, according to local expertise, to help minimize the call burden for operators. However, clinical competency and quality standards should be set to ensure procedural safety and optimal patient outcomes. The findings by Nolan et al. 6 are reassuring in that procedural outcomes were similar across specialties, underscoring that multiple pathways can deliver safe care. The next step for the field, however, is ensuring that all pathways are supported by shared training standards and multidisciplinary integration. As PERTs and PE management continue to mature, deliberate efforts toward standardization, inclusive multidisciplinary representation, and rigorous evaluation will be essential.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr Castro-Dominguez serves as a consultant for Medtronic and Boston Scientific. Dr Li serves as a consultant for Abbott Vascular, Boston Scientific, Inari Medical, Inquis Medical, and Medtronic. Dr Sreepathy has no conflicting interests.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.