
Abstract
Background:
Hemodynamic failure, defined as insufficient postprocedural improvement in limb perfusion, occurs frequently after endovascular therapy (EVT). However, the predictors of hemodynamic failure and its clinical course have not been adequately investigated. This study aimed to investigate the predictors and clinical course of chronic limb-threatening ischemia (CLTI) with hemodynamic failure after EVT.
Methods:
This retrospective, multicenter analysis of the SAPLING database included 924 patients with CLTI and tissue loss who underwent EVT between April 2010 and March 2023, with skin perfusion pressure (SPP) measured pre- and postprocedure. Hemodynamic failure was defined as postprocedural SPP < 40 mmHg. Kaplan–Meier analysis evaluated cumulative wound healing, reintervention, and wound recurrence. Logistic regression and Cox proportional hazards models identified predictors of hemodynamic failure and wound healing.
Results:
Hemodynamic failure occurred in 52.2% (482/924) of cases. Multivariable analysis identified lower preprocedural SPP and the absence of wound blush as independent predictors. Stratified analysis revealed the highest hemodynamic failure rate in patients with preprocedural SPP < 20 mmHg and absent wound blush (66.5%). Patients with hemodynamic failure showed significantly lower wound healing rates and higher rates of reintervention and wound recurrence (all p < 0.05). Factors independently associated with delayed wound healing included age ⩾ 75 years, nonambulatory status, hemodialysis, hemodynamic failure, Wound, Ischemia, and foot Infection (WIfI) stage 4, and the absence of wound blush.
Conclusions:
Hemodynamic failure after EVT was common and strongly associated with delayed wound healing, reintervention, and wound recurrence. Preprocedural SPP and wound blush assessment may be useful for identifying patients at high risk for hemodynamic failure.
Keywords
Background
Chronic limb-threatening ischemia (CLTI) represents the most severe manifestation of peripheral artery disease (PAD), characterized by ischemic rest pain or tissue loss. 1 Revascularization strategies for CLTI include bypass surgery (BSX) and endovascular therapy (EVT). Although two recent randomized controlled trials have reported different results regarding the optimal revascularization approach, contemporary guidelines emphasize that the choice between EVT and BSX should be individualized, considering patient risk, wound severity, conduit availability, and anatomical complexity.2–4 Although hemodynamic failure—defined as insufficient postprocedural improvement in limb perfusion—occurs more frequently after EVT than BSX, and has been associated with higher rates of reintervention, 5 its impact on clinical outcomes has not been fully elucidated. Therefore, this study aimed to identify the predictors of hemodynamic failure after EVT and evaluate its association with wound healing, reintervention, and wound recurrence in patients with CLTI.
Methods
Study design
The study protocol conformed to the principles of the Declaration of Helsinki and was approved by the ethics committee of each participating institution. Because this investigation was based on a retrospective review of routinely collected clinical data, involved no interventional assignment, and did not use human biological specimens, the requirement for written informed consent was waived in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan.
This retrospective, multicenter analysis was conducted using the SAPLING database, an institutional collaborative database of patients with CLTI. The database comprised consecutive patients who underwent EVT at four cardiovascular centers between April 2010 and March 2023. Of 2085 eligible patients, we excluded those with ischemic rest pain without tissue loss (Rutherford class 4; n = 286) and those without available skin perfusion pressure (SPP) measurements either before or after EVT (n = 875). The final analytic cohort consisted of 924 patients with tissue loss and paired pre- and postprocedural SPP assessments (Figure 1).
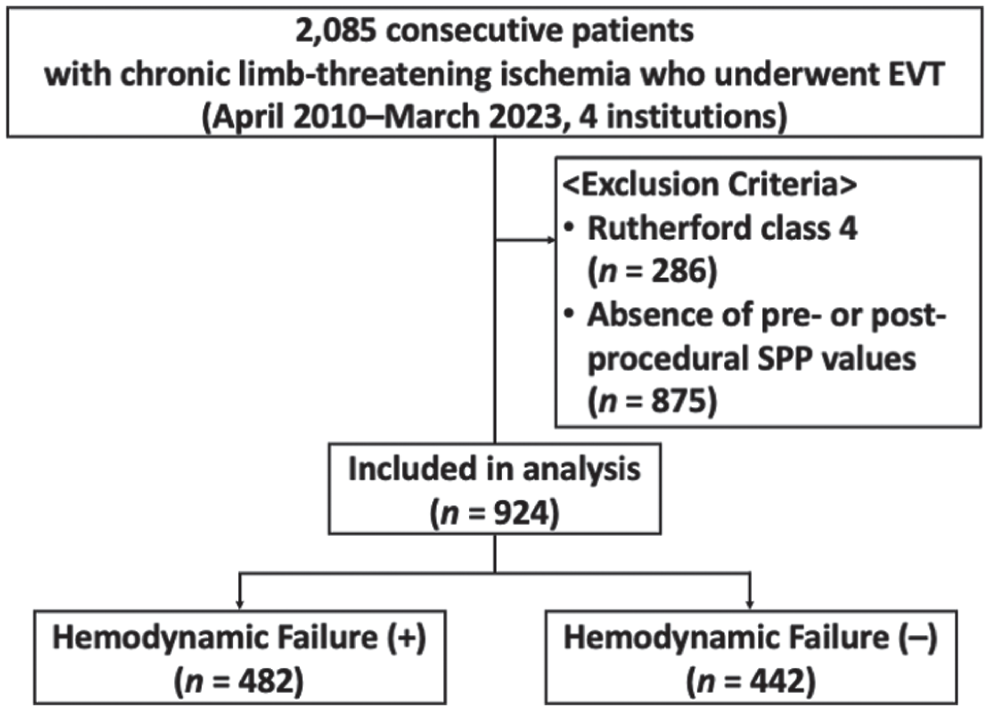
Study flow chart. Flow of patient inclusion and exclusion, resulting in 924 patients with chronic limb-threatening ischemia undergoing EVT with pre- and postprocedural SPP assessments.
Outcomes and definitions
The outcomes of interest were 1-year wound healing, reintervention, and wound recurrence. Hemodynamic failure was defined a priori as postprocedural SPP < 40 mmHg, corresponding to Wound, Ischemia, and foot Infection (WIfI) ischemia grade 2–3. CLTI was defined according to the global vascular guidelines (GVG). 6 Any amputation at or distal to the Lisfranc ligament was not considered a limb salvage failure. Nonambulatory status was assigned when patients were wheelchair-dependent or bedridden at admission. WIfI 7 classification was retrospectively graded from wound photographs, admission laboratory data, and medical records. Preprocedural angiography was used to assess the Global Limb Anatomic Staging System (GLASS). 6
Wound blush was defined as contrast opacification of the vessels around the wound in digital subtraction angiograms obtained immediately after EVT through the catheter introduced into the popliteal artery. 8 Angiosome-oriented revascularization was defined as revascularization of the infrapopliteal artery directly supplying the wound area, based on the angiosome concept described by Taylor and Palmer. 9 Wound healing was defined as the achievement of complete epithelization of all wounds without major amputation. 10 Reintervention was defined as any additional endovascular or surgical revascularization performed for delayed wound healing or recurrent stenosis or occlusion. Wound recurrence was defined as the development of a new ulcer at the same or an adjacent site after initial wound healing. Assessment of wound healing and wound recurrence was performed by the treating physicians at each participating center.
Baseline assessment, revascularization, and follow-up
Baseline limb ischemia was assessed using the ankle–brachial index (ABI) and SPP in routine practice. The severity and location of the lower-limb arterial lesions were initially evaluated with duplex ultrasound scanning (DUS), and clinically relevant lesions were confirmed by angiography before revascularization. Target lesions were considered for revascularization when angiography demonstrated ⩾ 75% diameter stenosis together with findings suggestive of functional relevance, including delayed contrast passage or an apparent translesional pressure gradient; when pressure assessment was performed, a mean gradient ⩾ 10 mmHg was considered significant.
Diagnostic angiography was generally performed prior to EVT; however, the timing and sequence of diagnostic angiography and therapeutic intervention were not standardized and depended on institutional practice and physician discretion. Accordingly, EVT was performed either during the same session or as a staged approach, particularly in cases requiring the treatment of both femoropopliteal (FP) and infrapopliteal (IP) segments. The treatment strategy was determined by the attending physician. Aortoiliac lesions were generally treated with primary stenting, FP lesions with a provisional stenting approach, and IP lesions with plain balloon angioplasty. Atherectomy devices were not approved for use in Japan during the study period.
Postprocedural SPP measurements were obtained according to local clinical practice. In general, SPP was measured several days to a few weeks after EVT, most commonly within approximately 1–2 weeks. Follow-up schedules and assessment modalities were determined by the treating physicians. Patients were typically assessed every 2–4 weeks until wound healing. Reinterventions were indicated in cases of recurrent ischemic pain or delayed wound healing, accompanied by recurrent occlusion or stenosis, and hemodynamic deterioration was assessed by ABI, DUS, or SPP.
Statistical analysis
Continuous variables are expressed as medians with IQRs, and categorical variables are expressed as counts and percentages. Group comparisons were performed using the Mann–Whitney U test for continuous variables and the χ2 test for categorical variables. Cumulative rates of wound healing, reintervention, and wound recurrence were estimated using the Kaplan–Meier method and compared with the log-rank test. Covariates included in the multivariable models were defined a priori based on prior literature and clinical relevance.6–8,11–15 Collinearity between preprocedural SPP and the WIfI ischemia grade was assessed, and variance inflation factors were confirmed to be below 2.0 for all included variables. Logistic regression was used to identify factors associated with hemodynamic failure, and Cox proportional hazards regression was used to evaluate factors associated with wound healing. A two-sided p-value less than 0.05 was considered statistically significant. Analyses were performed using JMP Pro 18 (SAS Institute Inc.).
Results
A total of 924 patients with CLTI (median age: 75 [IQR: 68–81] years; 61.6% men) were included in the analysis, of whom 482 (52.2%) exhibited hemodynamic failure (postprocedural SPP < 40 mmHg). Baseline clinical characteristics are summarized in Table 1, and lesion characteristics and procedural features are shown in Table 2. In addition, the baseline characteristics of included and excluded patients according to the availability of pre- or postprocedural SPP measurements are presented in Supplemental Tables S1 and S2. Compared with the included cohort, excluded patients were more frequently nonambulatory, suggesting that frailty and difficulty in the SPP measurements may have contributed to missing data.
Baseline clinical characteristics of patients with and without hemodynamic failure.
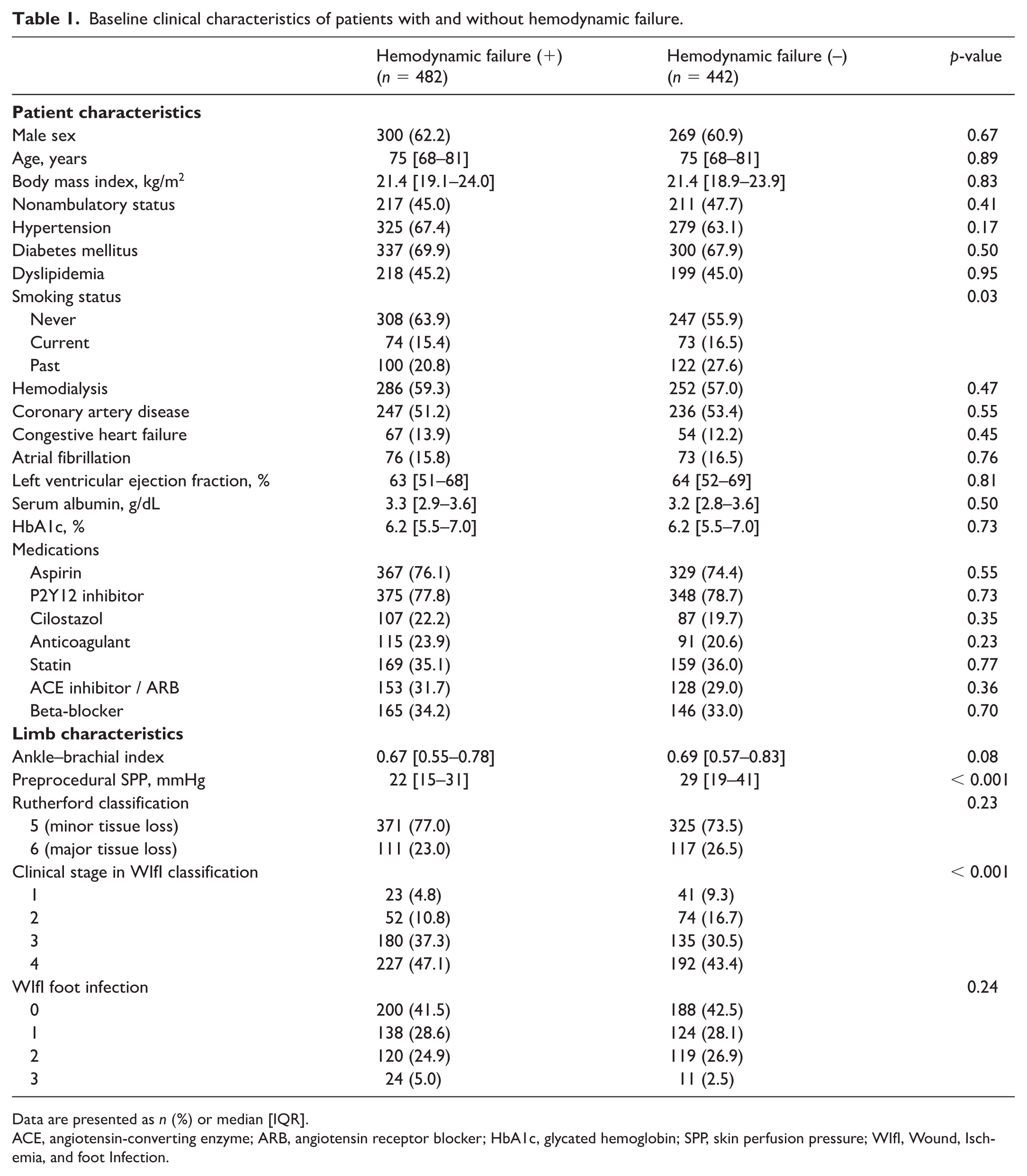
Data are presented as n (%) or median [IQR].
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; HbA1c, glycated hemoglobin; SPP, skin perfusion pressure; WIfI, Wound, Ischemia, and foot Infection.
Baseline lesion characteristics and procedural features of patients with and without hemodynamic failure.
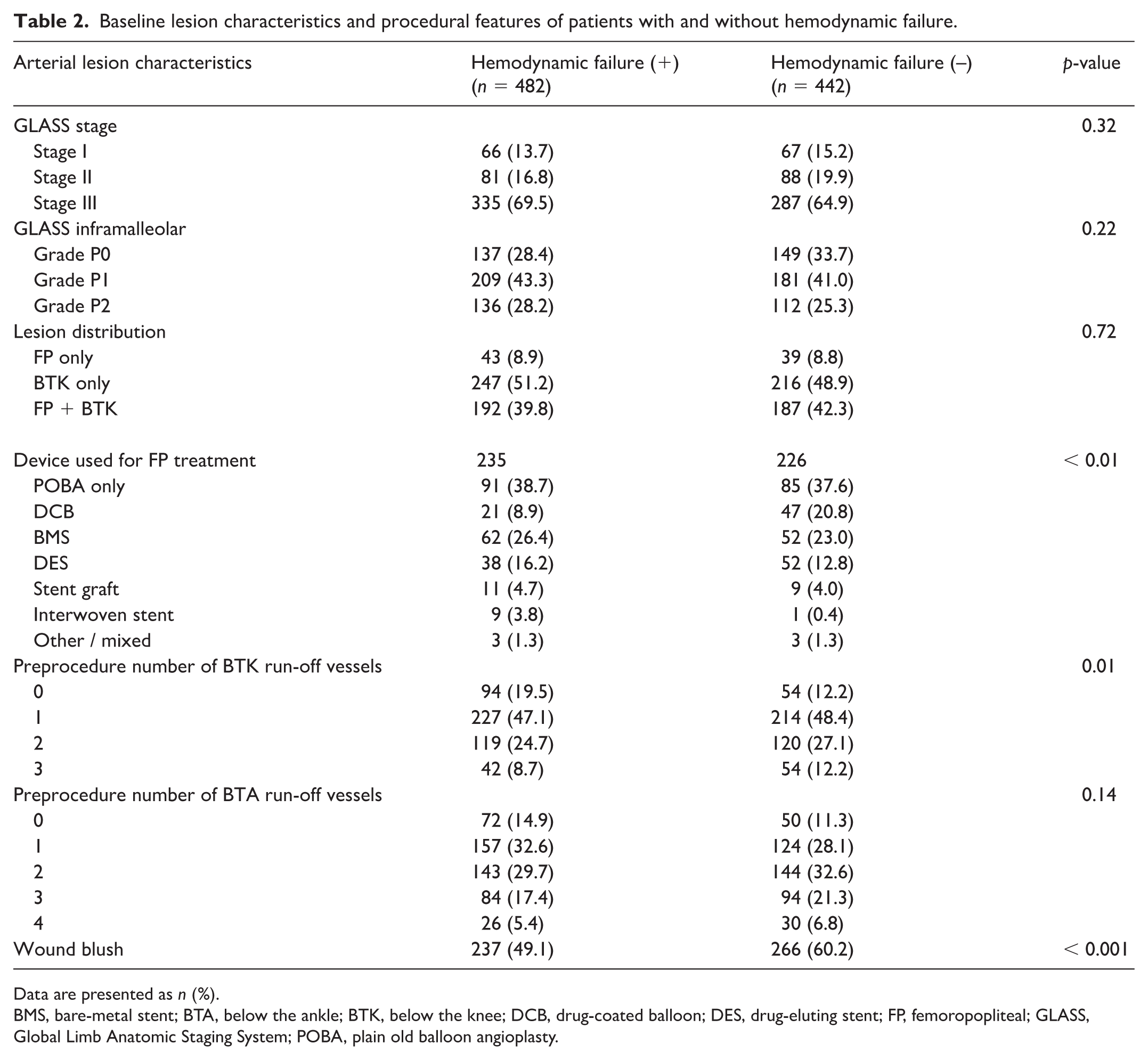
Data are presented as n (%).
BMS, bare-metal stent; BTA, below the ankle; BTK, below the knee; DCB, drug-coated balloon; DES, drug-eluting stent; FP, femoropopliteal; GLASS, Global Limb Anatomic Staging System; POBA, plain old balloon angioplasty.
Nonambulatory status was observed in 45.0% of the hemodynamic failure group and 47.7% of the nonfailure group (p = 0.41). Regarding wound severity, in the overall distribution of WIfI clinical stages, the proportion of WIfI stage 4 was significantly higher in the failure group than in the nonfailure group (47.1% vs 43.4%, p < 0.001), whereas the distribution of Rutherford classifications did not differ significantly between groups. Preprocedural SPP was significantly lower in the hemodynamic failure group (median 22 [IQR: 15–31] mmHg) than in the nonfailure group (29 [IQR: 19–41] mmHg, p < 0.001). The presence of wound blush was also significantly lower in the failure group (49.1% vs 60.2%, p < 0.001). In terms of lesion characteristics, the distribution of FP and below-the-knee (BTK) lesions, as well as GLASS stages, were comparable between groups. However, the hemodynamic failure group had fewer preprocedural BTK runoff vessels (0 vessels: 19.5% vs 12.2%, p = 0.01). Concordance between the revascularized BTK target vessel and the angiosome of the wound was similar between the two groups (68.4% vs 68.6%, p = 0.96), indicating that angiosome-oriented revascularization was achieved at comparable rates in both cohorts.
Predictors of hemodynamic failure
On multivariable logistic regression (Table 3), a lower preprocedural SPP (per 1 mmHg increase; OR: 0.97; 95% CI: 0.96–0.98; p < 0.001) and absence of wound blush (OR: 0.73; 95% CI: 0.55–0.96; p = 0.02) were independent predictors of hemodynamic failure. Stratified analysis combining preprocedural SPP and wound blush demonstrated that patients with preprocedural SPP < 20 mmHg and absent wound blush had the highest rate of hemodynamic failure (66.5%), followed by an intermediate risk in those with either preprocedural SPP < 20 mmHg and wound blush (+) or preprocedural SPP ⩾ 20 mmHg and wound blush (–) (54.2%), and the lowest risk in those with preprocedural SPP ⩾ 20 mmHg and wound blush (+) (42.7%) (Figure 2).
Predictors of hemodynamic failure.
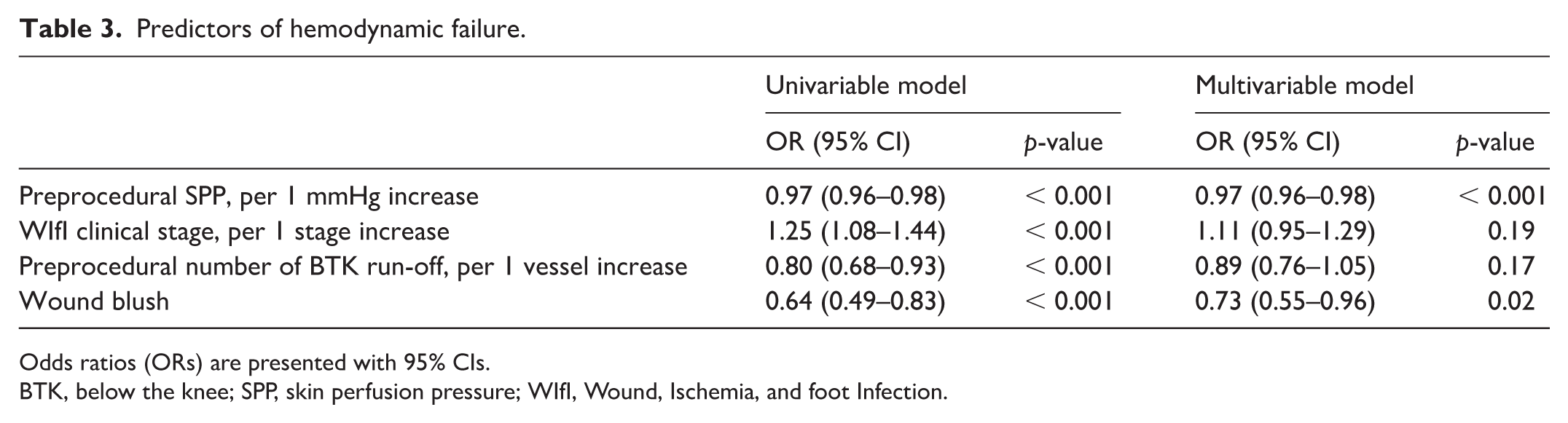
Odds ratios (ORs) are presented with 95% CIs.
BTK, below the knee; SPP, skin perfusion pressure; WIfI, Wound, Ischemia, and foot Infection.
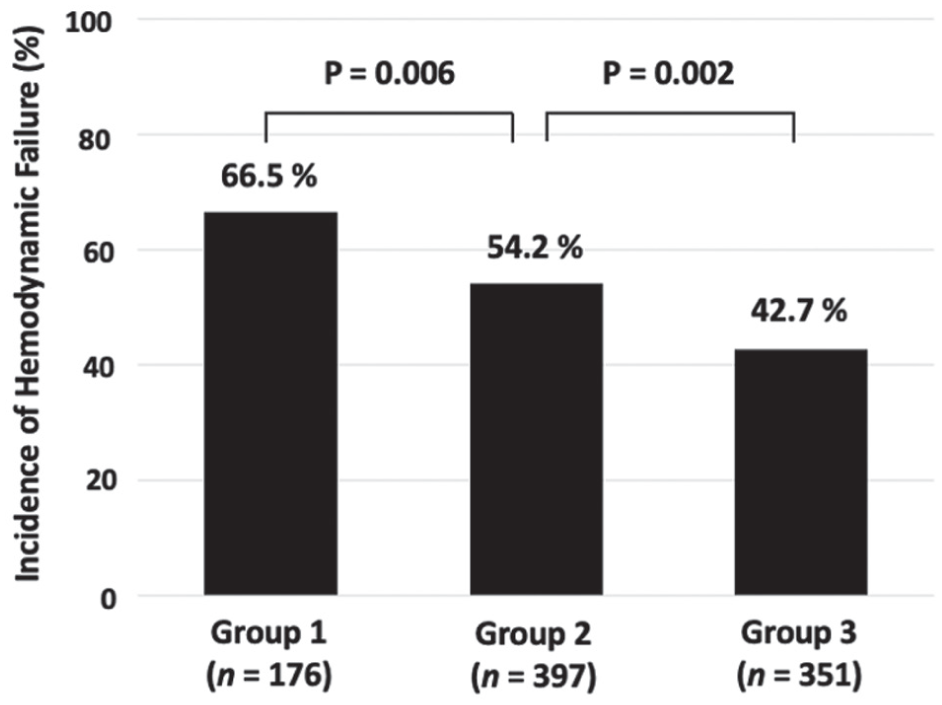
Stratified analysis of hemodynamic failure rates. Hemodynamic failure is stratified by preprocedural SPP and wound blush. Group 1: preprocedural SPP < 20 mmHg and absent wound blush; Group 2: preprocedural SPP < 20 mmHg with present wound blush, or preprocedural SPP ⩾ 20 mmHg with absent wound blush; Group 3: preprocedural SPP ⩾ 20 mmHg and present wound blush.
Wound healing rate and its predictors
At 12 months, Kaplan–Meier analysis demonstrated that patients with hemodynamic failure had significantly lower cumulative wound healing rates compared with those without failure (54.5% vs 64.6%; log-rank p = 0.004; Figure 3A). In contrast, the cumulative incidence of reintervention (53.5% vs 46.3%; p = 0.021; Figure 3B) and wound recurrence (24.6% vs 17.7%; p = 0.049; Figure 3C) was significantly higher in the hemodynamic failure group.
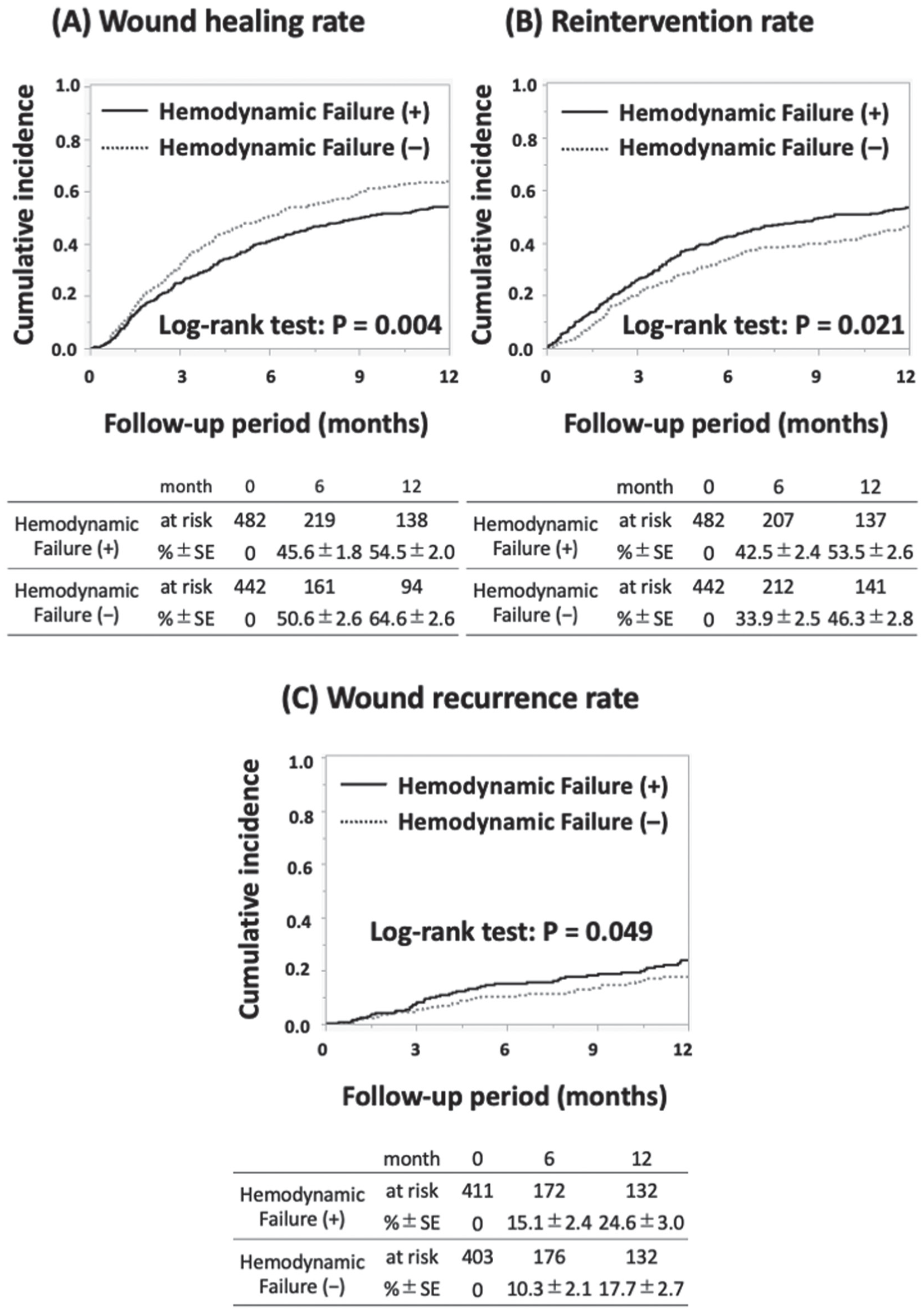
Cumulative Kaplan–Meier estimate of
On multivariable Cox regression (Table 4), age ⩾ 75 years (HR: 1.23; 95% CI: 1.03–1.48; p = 0.02), nonambulatory status (HR: 0.78; 95% CI: 0.65–0.94; p < 0.001), hemodialysis (HR: 0.69; 95% CI: 0.58–0.83; p < 0.001), hemodynamic failure (HR: 0.82; 95% CI: 0.69–0.97; p = 0.02), WIfI stage 4 (HR: 0.79; 95% CI: 0.66–0.95; p = 0.02), and the presence of wound blush (HR: 1.28; 95% CI: 1.07–1.53; p < 0.001) were independently associated with wound healing.
Predictors of wound healing.
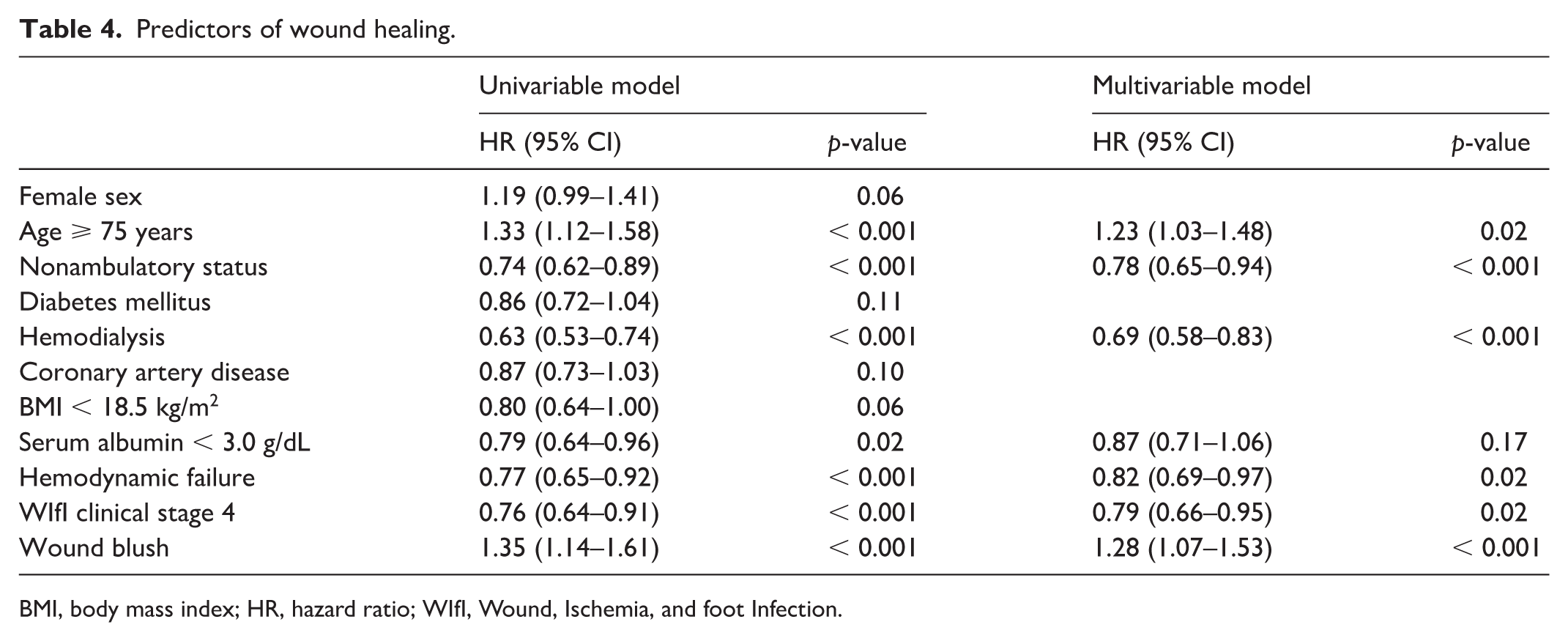
BMI, body mass index; HR, hazard ratio; WIfI, Wound, Ischemia, and foot Infection.
Discussion
In this multicenter study of patients with CLTI undergoing EVT, lower preprocedural SPP and absence of angiographic wound blush were identified as independent predictors of hemodynamic failure, defined as insufficient postprocedural improvement in limb perfusion. Patients with hemodynamic failure exhibited significantly lower 1-year wound healing rates, as well as higher rates of reintervention and wound recurrence, compared with those without failure. SPP has been reported as a potentially useful, objective, and noninvasive marker for assessing ischemia in CLTI. 16 Regarding preoperative SPP, Urabe et al. and Yamada et al. identified 40 mmHg as the threshold for predicting wound healing.11,12 With respect to postoperative SPP, previous studies have reported that higher values are associated with favorable wound healing. 13
Furthermore, Utsunomiya et al. and Lee et al. proposed predictive cutoff values of 30 mmHg and 50 mmHg, respectively.14,15 In line with these previous reports, our analysis extends prior observations by focusing on postprocedural hemodynamic failure as a clinically meaningful intermediate endpoint and by demonstrating that the combination of preprocedural SPP (< 20 mmHg) and angiographic wound blush enables further risk stratification. This combined assessment identified a subgroup with particularly high rates of hemodynamic failure and adverse limb outcomes.
In contrast to previous studies that primarily examined SPP in isolation, our findings suggest that integrating physiologic measures (SPP) with angiographic markers (wound blush) may improve risk discrimination, especially in patients with advanced CLTI. However, we were unable to determine an optimal postprocedural SPP cutoff, likely due to missing data and variability in measurement timing, highlighting the need for prospective studies with standardized assessment protocols.
Mechanisms of hemodynamic failure
Several mechanisms may underlie hemodynamic failure following EVT. First, early recoil in IP arteries has been frequently reported and likely contributes to inadequate postprocedural perfusion. 17 Second, small artery disease (SAD) 18 —defined as disease distal to the pedal arch—may limit improvement in wound perfusion despite successful proximal revascularization. It is important to note that these mechanisms were not directly measured in the present study and should therefore be regarded as hypotheses rather than definitive explanations. Although no significant difference was observed in the concordance rate between angiosome-oriented revascularization and the wound territory, anatomical concordance does not necessarily guarantee effective in-line flow or sufficient tissue-level perfusion, particularly in the presence of poor runoff or microvascular dysfunction. 19
In the present cohort, patients with hemodynamic failure had a higher prevalence of having no preprocedural infrapopliteal runoff than those without hemodynamic failure. Although postprocedural BTK runoff was not systematically recorded in the database, this finding suggests that many patients had advanced distal arterial disease at baseline. Residual distal outflow limitation may therefore have persisted in some patients despite treatment of the selected target vessel. This may help explain why hemodynamic failure occurred even though the concordance rate between the revascularized BTK target vessel and the wound angiosome was similar between groups. In advanced CLTI, anatomically appropriate target vessel selection does not necessarily translate into sufficient distal runoff or tissue-level perfusion at the wound site. This discrepancy may partly explain why hemodynamic failure occurred despite similar anatomical strategies across groups. Notably, lesion characteristics and GLASS stage were comparable between groups. One plausible explanation is that participating sites were centers with substantial EVT expertise, potentially maintaining a consistent technical success rate even in anatomically complex disease. In addition, GLASS primarily captures anatomic complexity in the FP and IP segments and may not directly reflect foot-level perfusion or the extent of physiologic improvement at the wound site. Therefore, anatomic severity as assessed by GLASS may not translate linearly into postprocedural perfusion adequacy, particularly when microvascular dysfunction or distal perfusion limitations predominate.
The long enrollment period of this study should also be considered when interpreting the findings. Between 2010 and 2023, EVT devices, procedural strategies, wound care, and systemic medical management evolved substantially. In the present cohort, infrapopliteal interventions were performed using balloon angioplasty alone, reflecting the treatment environment in Japan during the study period. In contrast, treatment options for femoropopliteal disease expanded over time, including the introduction of drug-coated balloons, drug-eluting stents, and stent grafts. A previous analysis from the same SAPLING database demonstrated temporal changes in patient and treatment characteristics, with lower reintervention rates in later periods but no significant improvement in mortality or major amputation. 20 These findings suggest that advances in treatment strategy may have improved durability in some vascular segments; however, the overall limb prognosis in CLTI may remain constrained by increasing patient frailty, comorbidities, and distal arterial disease complexity. Therefore, the impact of calendar time and evolving treatment options should be acknowledged when interpreting the association between hemodynamic failure and clinical outcomes in the present study.
Clinical implications
Preprocedural SPP and wound blush assessment can identify subgroups at particularly high risk of hemodynamic failure. In the present cohort, infrapopliteal interventions were performed using balloon angioplasty alone, reflecting the treatment environment in Japan during the study period. Therefore, the generalizability of our results to Western practice—where atherectomy and drug-coated devices are available—should be interpreted with caution.
In patients with markedly low preprocedural SPP and absent wound blush, the physiologic limitation of perfusion may persist despite technically successful EVT. In such cases, adjunctive strategies targeting microcirculatory improvement—such as low-density lipoprotein (LDL) apheresis 21 —may be considered, as these therapies have been reported to enhance tissue perfusion and support wound healing in selected CLTI populations. Importantly, preprocedural SPP and wound blush may also help clinicians recognize the potential limits of an EVT-first approach and support multidisciplinary decision-making that includes surgical bypass, percutaneous deep venous arterialization (pDVA) in selected cases, or—when revascularization is unlikely to achieve meaningful wound healing given patient frailty and goals of care—palliative limb management. Such a framework may be particularly relevant for patients with very low physiologic reserve, extensive tissue loss, or severe distal perfusion impairment.
Future prospective studies should evaluate the standardized timing of postprocedural SPP measurement, validate combined physiologic–angiographic risk models, and assess whether treatment strategies guided by these markers can improve limb-related outcomes in CLTI.
Study limitations
First, SPP measurement was performed at the discretion of the treating physicians, leading to potential variability in measurement timing and technique across centers. Although postprocedural SPP was generally measured within several days to a few weeks after EVT, the absence of a standardized protocol may have influenced the classification of hemodynamic failure 22 and limited the identification of an optimal postprocedural SPP cutoff. Second, more than 40% of the original cohort was excluded because SPP could not be obtained. Excluded patients were more frequently nonambulatory and had lower serum albumin levels (Table S1), suggesting a frailer population. Because SPP measurement requires patients to remain at rest, missing data were likely not random and may have introduced selection bias.
Third, information on microvascular pathology, such as SAD distal to the pedal arch, and the presence of pedal arch continuity was limited. These factors may affect wound perfusion and healing but could not be fully captured in this study. Similarly, microcirculatory dysfunction and tissue-level perfusion were not directly assessed and therefore could not be incorporated into the analysis. Fourth, postprocedural BTK runoff was not systematically recorded; therefore, we could not directly evaluate whether residual BTK runoff after EVT mediated the association between poor baseline runoff and hemodynamic failure.
Fifth, because this study included patients treated over a long period, temporal changes in EVT devices, procedural strategy, wound care, and medical therapy may have influenced clinical outcomes. The present analysis was not designed primarily to evaluate treatment-era effects, and residual confounding related to calendar time could not be fully excluded. Sixth, the diagnostic and procedural workflow was not standardized across centers. Although diagnostic angiography was generally performed before EVT, the timing and sequence of angiography and intervention were left to institutional practice and physician discretion, and EVT was performed either during the same session or as a staged approach. This procedural heterogeneity may have influenced lesion assessment, treatment strategy, and postprocedural hemodynamics. Finally, detailed procedural data, including balloon size, inflation pressure, and adjunctive pharmacological therapies, were not consistently available and may have impacted postprocedural perfusion.
Conclusions
In this multicenter study of patients with CLTI undergoing EVT, hemodynamic failure—defined as postprocedural SPP < 40 mmHg—was observed in more than half of the patients and was independently predicted by lower preprocedural SPP and absence of wound blush. Hemodynamic failure was significantly associated with delayed wound healing, increased reintervention, and higher wound recurrence. These findings suggest that preprocedural SPP and intraoperative angiographic wound blush may help identify patients at high risk of poor hemodynamic response after EVT, allowing for earlier consideration of alternative or adjunctive therapeutic strategies.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X261452653 – Supplemental material for Predictors and clinical course of chronic limb-threatening ischemia with hemodynamic failure after endovascular therapy
Supplemental material, sj-docx-1-vmj-10.1177_1358863X261452653 for Predictors and clinical course of chronic limb-threatening ischemia with hemodynamic failure after endovascular therapy by Hiroaki Nohara, Yosuke Hata, Osamu Iida, Sho Nakao, Taku Toyoshima, Motoki Yasunaga, Akito Kawamura, Haruya Yamane, Kuniyasu Ikeoka, Yasuyuki Egami, Masami Nishino, Yohei Sotomi and Yasushi Sakata in Vascular Medicine
Footnotes
Acknowledgements
The authors thank the medical staff at Osaka Rosai Hospital, Kansai Rosai Hospital, Osaka Keisatsu Hospital, and NHO Osaka National Hospital for performing the catheterization procedures and data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The data are available from the corresponding author upon reasonable request and with permission from the ethics committees of the participating institutions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.