
Abstract
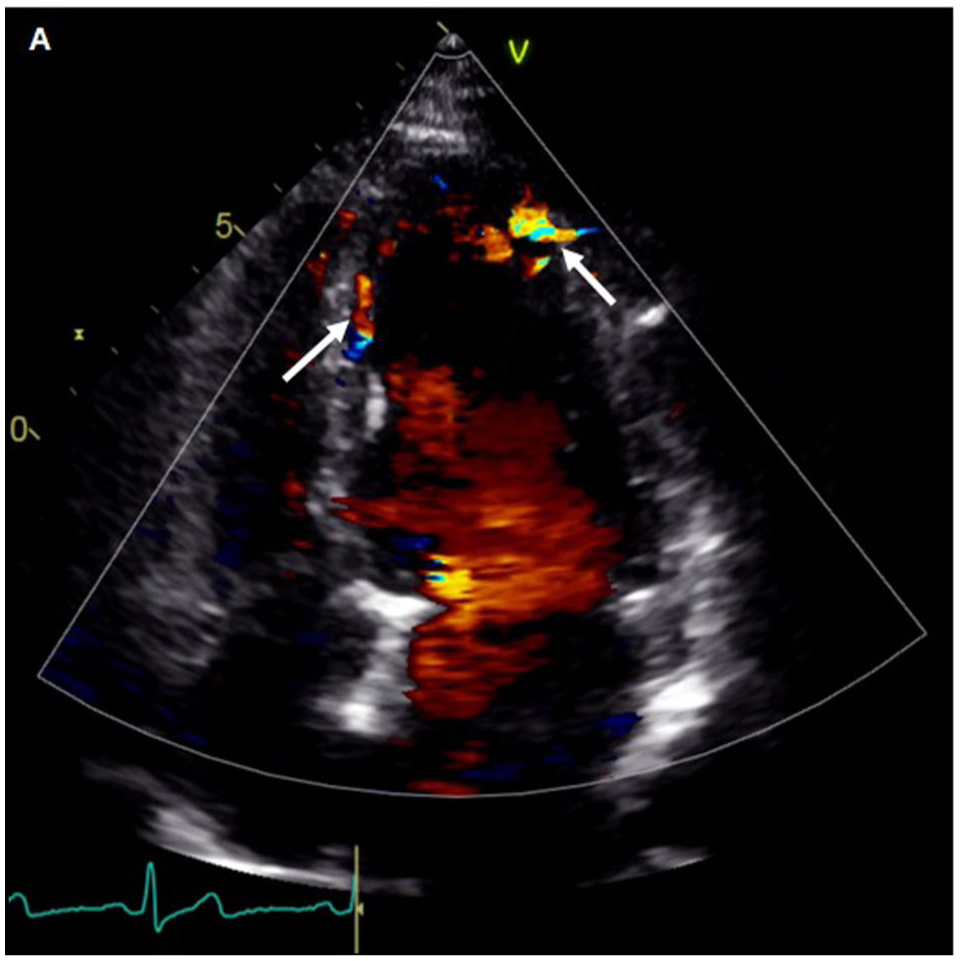
A 59-year-old woman with no relevant medical or family history was evaluated due to 3 months of progressive dyspnea on exertion. The physical examination and electrocardiogram were unremarkable. Transthoracic echocardiography revealed mild left ventricle dilation with preserved biventricular systolic function, in addition to diastolic and continuous flow signals within the ventricular wall (Panel A, arrows), consistent with the presence of tortuous and enlarged coronary arteries (see also: Supplemental Video A, available online).
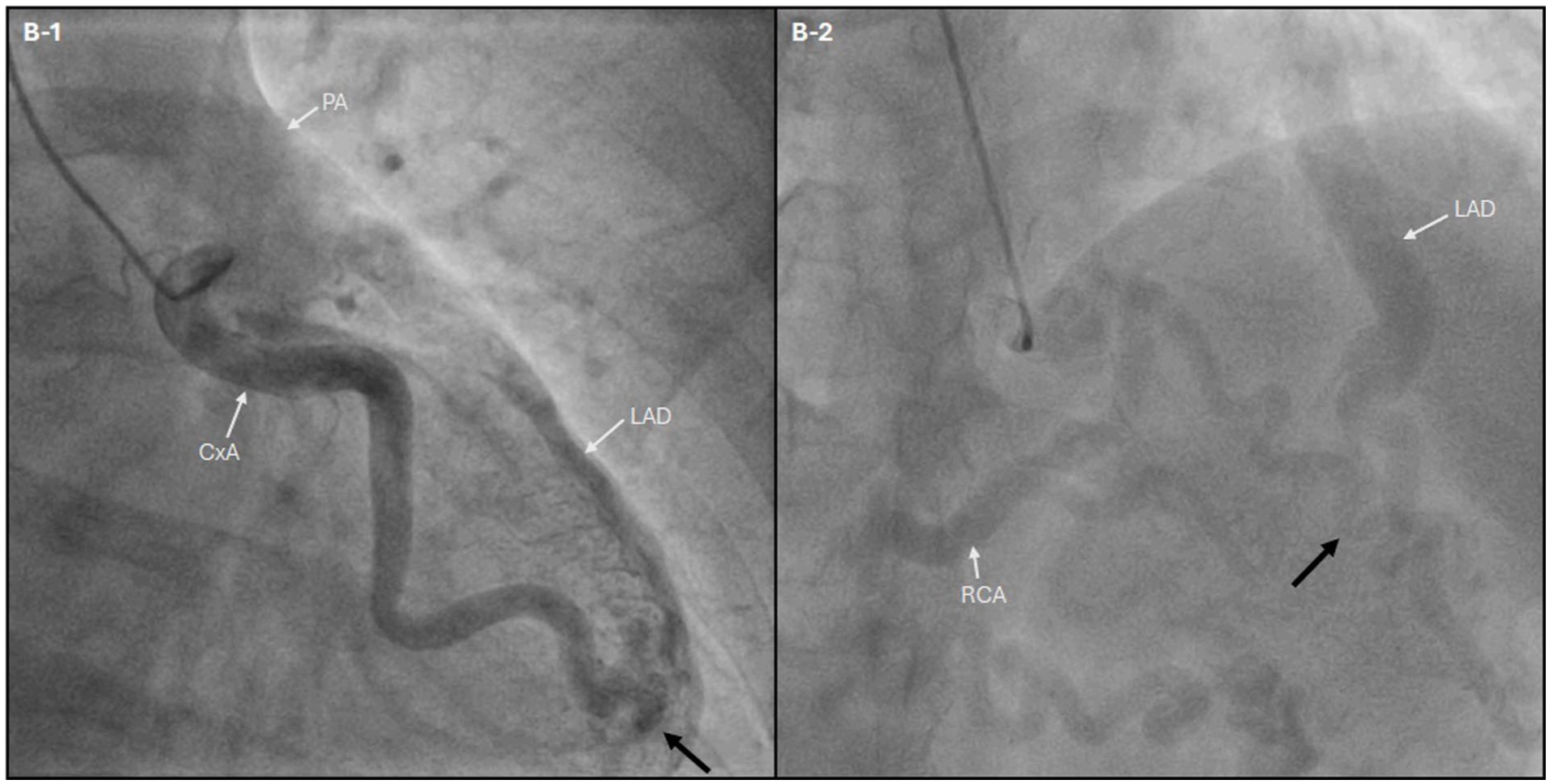
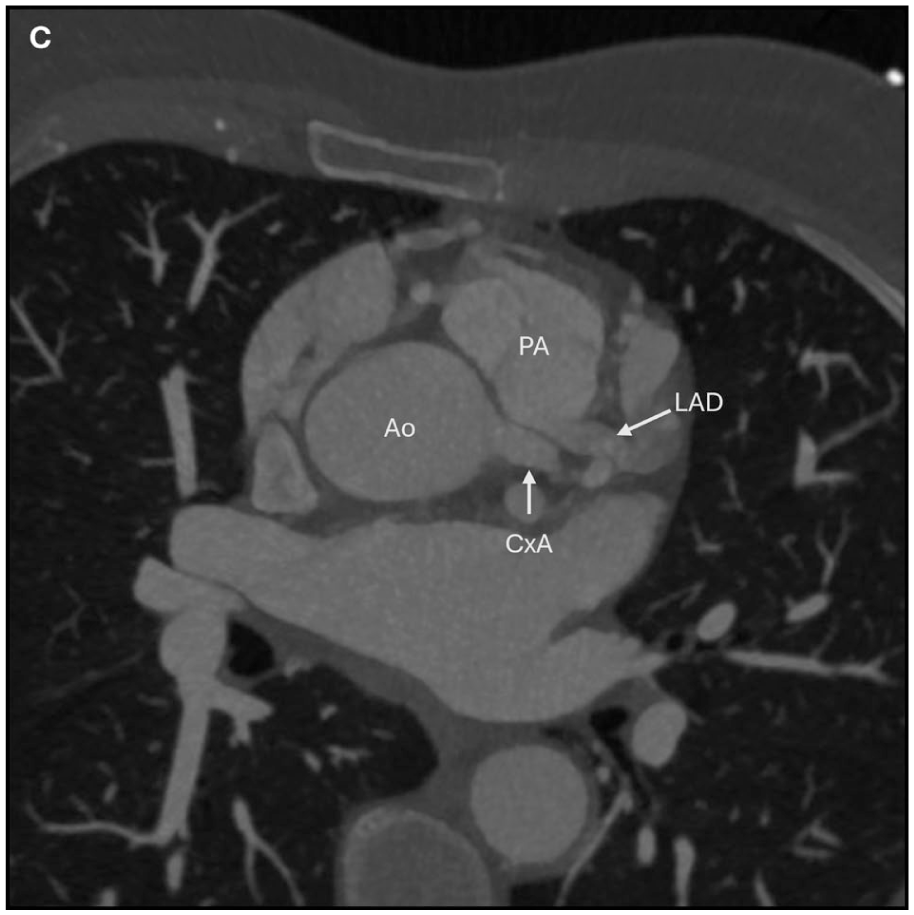
A coronary angiography demonstrated markedly ectatic coronary arteries. The left anterior descending (LAD) artery originated anomalously (Panel B and Supplemental Video B) from the pulmonary artery (PA) with retrograde perfusion via collaterals (Panels B-1 and B-2: green arrows) from the circumflex artery (CxA) and right coronary artery (RCA). This finding was consistent with the diagnosis of an anomalous origin of the left anterior descending artery from the pulmonary artery (ALADAPA). Circumflex and right coronary arteries demonstrated normal aortic (Ao) origin. A coronary computed tomography (CT) angiography confirmed the anomalous origin of the LAD and the presence of diffuse ectatic coronary arteries, with no evidence of atherosclerotic coronary artery disease (Panel C).
To assess functional impact and myocardial viability, a myocardial perfusion scintigraphy was performed and demonstrated moderate-to-severe reversible ischemia in the anterior myocardial territory. To re-establish physiological antegrade perfusion, the patient was referred for surgical correction.
Anomalous origin of the left anterior descending artery from the pulmonary artery (ALADAPA) is exceptionally rare with only 52 cases reported in the literature and a systematic review.1,2 It may remain undetected until adulthood due to extensive enlarged collateral development. Early recognition with multimodality imaging is essential, as surgical reimplantation of the anomalous artery into the aorta is the definitive treatment to prevent myocardial ischemia, ventricular dysfunction, and sudden cardiac death. 3
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental videos for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.