
Abstract
This paper presents case examples that document the preliminary clinical utility of using electronic monitoring (EM) feedback to tailor empirically validated adherence-promoting interventions, delivered in standard clinical practice. Challenges of utilizing EM in standard clinical practice as well as future directions are also discussed. Two adolescents referred for behavioral adherence promotion intervention are described. Each youth was provided a MEMS® bottle and one oral medication was chosen jointly by the therapist, family, and medical provider for adherence monitoring. Graphical MEMS® feedback was provided to families during intervention visits and subsequently used to tailor adherence interventions to target each family’s unique needs. EM feedback was a feasible and clinically rich supplement to adherence-promoting interventions. EM facilitated identification of adherence barriers and successes, and open and non-adversarial discussions regarding adherence between patients, families, and clinicians, and provided real-time representations of patients’ medication administration. These case presentations suggest that EM feedback can be a clinically useful tool when used as a supplement to an empirically supported intervention delivered in standard psychological practice aimed at adherence promotion among chronically ill youth.
Introduction
Adherence in pediatric populations
Nonadherence to treatment regimens is a significant problem within pediatrics. While prevalence of nonadherence varies by disease population, complexity of treatment regimen, and how adherence is assessed (Quittner, Espelage, Ievers-Landis, & Drotar, 2000; Rapoff & Barnard, 1991), extant literature suggests that approximately 50 percent of pediatric chronic illness patients are nonadherent to prescribed treatment regimens (Lemanek, Kamps, & Chung, 2001; Rapoff & Barnard, 1991). Poor adherence to pediatric medical regimens carries considerable implications for patient quality of life, health outcomes, and disease management decisions by healthcare providers (DiMatteo, Giordani, Lepper, & Croghan, 2002; Rapoff, 1999). Treatment cost- effectiveness is also impacted; it is estimated that nonadherence in the US costs between $100 and $300 billion yearly (Berg, Dischler, Wagner, Raia, & Palmer-Shevlin, 1993; DiMatteo, 2004).
Adherence monitoring and promotion in clinical care
Despite the extraordinary negative consequences of poor adherence in pediatrics, little is documented in the broad pediatric literature on adherence monitoring in standard clinical care. What is documented, however, often takes place as part of randomized controlled trials (Kahana, Drotar, & Frazier, 2008; Lemanek et al., 2001), not clinical practice. Unfortunately, youth and families that participate in clinical trial research are often vastly different from those seen by pediatric psychologists in clinical practice. For example, youth with complex medical and comorbid psychological profiles are typically excluded from participation in research studies (Drotar, 2009). As such, interventions used in randomized clinical trials are limited in terms of generalizability.
Alternatively, clinical case presentations offer an opportunity to highlight youth typically seen in practice, describe challenging clinical populations, and inform clinical practice (Drotar, 2009). Case presentations also offer an arena for the description of novel treatment methods, an increasingly important area as public health needs continue to move toward efficiency in care. Electronic monitoring (EM) is one example of novel methodology with great promise of improving treatment adherence in chronically ill youth in standard care. To our knowledge, this paper is the first to report case presentations systematically using EM feedback to tailor adherence-promoting intervention in outpatient pediatric clinical practice, using case presentations to do so. These case examples represent a first step toward documenting the clinical utility and feasibility of EM feedback and highlight common challenges incurred by using MEMS® bottles with pediatric patients receiving outpatient intervention for poor medical treatment adherence.
Adherence measurement
In the face of healthcare reform and its emphasis on increasing health management efficiency and minimizing healthcare costs, objective adherence assessment and adherence promotion are highly salient within pediatric care. A recent review of evidence-based assessments in pediatric psychology highlighted a general consensus that adherence assessments should not only be integrated into standard clinical practice but their clinical applicability evaluated (Cohen et al., 2008; McQuaid, 2008).
However, measuring adherence to medical treatment regimen is a complicated process for clinicians. Several methodologies are available (see Drotar, 2000; Rapoff, 1999 for a review) and each presents unique advantages and disadvantages. Self-report measures are perhaps the most frequently used method because they are easy to administer, inexpensive, and can evaluate multiple aspects of adherence (e.g., barriers to adherence, understanding of treatment regimen, allocation of treatment responsibility; La Greca & Bearman, 2003). However, self-report is subject to social desirability and individuals often provide overestimates of their adherence compared to objective adherence measures. In fact, Riekert and Rand document average self-reported adherence rates above 85 percent compared to electronic monitoring rates below 70 percent (2002). Self-report measures are further limited by reliance on respondent recall of their adherence during a specific period of time, poor feasibility with very young children, and the fact that data may need to be collected from multiple respondents who participate in disease management (Quittner, Modi, Lemanek, Ievers-Landis & Rapoff, 2008; Rapoff, 1999). All of these factors may make it difficult for clinicians to accurately capture adherence rates as part of standard psychological care. Given these limitations, EM may be a more clinically useful and accurate assessment tool.
Current uses of electronic monitoring: What’s being done?
EM is considered by some to be the “gold standard” of adherence measurement (Cramer, 1995). The Medication Event Monitoring System (MEMS®; AARDEX Ltd, Zug, Switzerland) is the most extensively used electronic medication monitor, with hundreds of research studies in both adult and pediatric samples (Maikranz, Steele, Dreyer, Stratman, & Bovaird, 2007; Modi et al., 2006; Rapoff, Belmont, Lindsley, & Olson, 2005). MEMS® mimics a traditional pill bottle in both appearance and utility, and tracks the date and time of each bottle opening. MEMS® bottles store information in real time that can be quickly downloaded for analysis (Cramer, 1995). Unlike other measures of adherence, EM is currently the only method available to objectively identify administration patterns (e.g., whether patients are taking too much or too little medication, whether medication is taken at the prescribed time of day, and so on) (Rapoff, 1999). However, EM is not without limits. EM devices such as MEMS® bottles merely serve as a proxy for adherence, indicating only whether or not the electronic container was opened, not whether medication was consumed. Electronic monitors can also malfunction, are expensive, and cannot accommodate every type and size of medication (e.g., liquid or powder suspension) (Quittner et al., 2008). Yet the fact that previous research indicates EM reveals more accurate and reliable adherence rates compared to patient, caregiver, or physician self-reports, pill counts, and pharmacy records (Rapoff & Barnard, 1991; Riekert & Rand, 2002) outweighs these limitations and enhances the clinical utility of EM.
Feasibility of electronic monitoring in clinical care
Previous intervention research provides preliminary evidence for the clinical utility of MEMS® feedback by patients and providers alike. In a study of EM and counseling for adult diabetes patients, Rosen and colleagues (Rosen, Rigsby, Salahi, Ryan, & Cramer, 2004) found that providing feedback about MEMS® data not only facilitated a non-adversarial discussion of adherence, but was welcomed by patients. Moreover, MEMS® bottles have the benefit of allowing clinicians to monitor patient adherence in their natural environments without disrupting patients’ daily medication-taking routines (Schmitz, Sayre, Stotts, Rothfleisch, & Mooney, 2005). In pediatric care, previous research suggests EM can provide objective evidence to aid in determining the level of parental involvement needed for optimal health outcomes (Riekert & Rand, 2002). EM data revealing a high level of adherence to medication may persuade parents that their child or adolescent is capable of adhering to medication without a high level of parental monitoring. On the other hand, electronic data that reveals poor adherence may encourage parents to assume greater responsibility and monitoring of their child’s pill-taking behavior.
However, pediatric adherence promotion efforts utilizing feedback from EM data have yet to be empirically tested. A limited number of previously published RCT interventions using EM feedback as a key component to increase patient adherence provide preliminary evidence for the clinical utility of MEMS® feedback, but this research is overwhelmingly adult focused. In each of these studies, patients receiving MEMS® feedback demonstrated significantly greater improvements in adherence that maintained over time compared to individuals in the “no feedback” condition (e.g., Cramer and Rosenheck, 1999; de Bruin et al., 2010; Mooney, Sayre, Hokanson, Stotts, & Schmitz, 2007; Nides et al., 1993; Schmitz et al., 2005). Only one study provided EM feedback to children for adherence promotion; results demonstrated significantly higher adherence among asthmatic children who received feedback compared to controls (Otsuki et al., 2009). Given the supporting evidence for the utility of EM data, incorporating EM feedback into adherence promotion interventions may be a promising avenue for clinical care with pediatric patients. To our knowledge though, feedback from MEMS® data has not been routinely incorporated into standard clinical care to promote treatment adherence among chronically ill children and adolescents.
Adherence Center clinical service: Incorporating MEMS® into clinical care
The Center for the Promotion of Treatment Adherence and Self-Management at Cincinnati Children’s Hospital Medical Center (CCHMC) is devoted to the development and implementation of clinical services for youth who present with salient problems in adherence to prescribed medical treatment regimens. Currently, the Center routinely utilizes MEMS® bottles as a part of standard outpatient clinical psychology practice for adherence promotion among pediatric patients with a chronic illness. Incorporating EM feedback into standard clinical practice aimed at adherence promotion at CCHMC affords an opportunity to evaluate the clinical utility of this novel treatment mechanism. At the start of outpatient clinical care, all patients taking oral medication for the treatment of a pediatric medical condition are provided a MEMS® bottle and one oral medication is chosen jointly by the therapist, family, and medical provider for adherence monitoring. Medication monitoring is unique to each patient and chosen on the basis of treatment complexity, assay levels revealing subtherapeutic drug levels, and importance of a particular medication for health outcomes. During follow-up visits, data from the MEMS® bottle is downloaded, feedback (verbal and graphical) is provided to families in session, and barriers or challenges to adherence are discussed and targeted directly during the session. Typical adherence promotion strategies used in combination with EM feedback include empirically supported interventions such as behavior management (e.g., behavioral contracting and reinforcement contingencies) and guided problem solving, as well as education regarding illness and treatment and motivational interviewing strategies (Drotar, 2006; Graves, Roberts, Rapoff, & Boyer, 2010; Kahana et al., 2008).
The Adherence Center at CCHMC is also concurrently conducting effectiveness research aimed at evaluating components of behavioral interventions for adherence promotion and institutional review board approval was obtained before initiating the study. Following a baseline assessment of treatment adherence, families are referred for behavioral adherence promotion intervention conducted by pediatric psychologists separate from medical visits. Those that meet certain inclusion criteria (i.e., ages 2−18 years, diagnosed with a chronic medical condition that requires adherence to ongoing medical treatment, referred for adherence promotion intervention) are also then recruited to participate in the research study. Families that choose to participate are then re-evaluated at two follow-up assessments; 4−6 months and 12 months. Families are provided a MEMS® bottle following baseline evaluation and this data is downloaded during intervention visits and targeted based on each family’s unique needs. Families that opt out of the research study also receive MEMS® bottles and feedback is provided for the duration of treatment.
Case presentations
The patients presented here were referred to the Center’s clinical service and recruited to participate in the Center’s research study. They were chosen for presentation here not based on treatment outcome, but rather, because (1) poor adherence was highly salient to their clinical presentation, (2) adherence was a crucial focus of adherence-promoting outpatient therapy, (3) EM served as a primary intervention component, and (4) they presented with complex clinical profiles and comorbidities typically seen in youth referred to the Adherence Center for adherence promotion. Both families were provided a MEMS® bottle following intake and a joint decision was made with the family and medical providers regarding which medication to track. Each family was told how the MEMS® bottle would be used during the course of treatment (e.g., “This bottle gives us a graph each week that tells us how often you’ve taken your medicine over the past week. We’re going to be looking at this graph every week and it will help us talk about how you’re doing, what successes you experience with your medicine, and also identify any problems or difficulties you may be having, and why”). Each family brought the MEMS® bottle to therapy visits and adherence data was quickly downloaded at the start of each session. This was done by placing the MEMS® bottle onto a reader plugged into the USB port of a computer and transferring the dosing history data from the MEMS® bottle onto the computer. Within seconds, data was downloaded into a software program that read, displayed, and printed adherence information (e.g., date/time of all bottle openings, frequency of missed doses). All families were provided education on how to interpret downloaded MEMS® adherence data (see Figure 1 for a standard MEMS® calendar plot; “This shows you how many times your bottle was opened each day: 0 = bottle was never opened, 1 = bottle was opened once, 2 = bottle was opened twice”). At each session’s start, adherence data since the last session was presented to each family and trends (e.g., missed doses, no missed doses, doses taken outside prescribed time interval) in adherence were discussed. To ensure that MEMS® data was not punitive, the clinician highlighted both positive and negative adherence patterns at each session. Strategies that contributed to positive adherence behaviors were also used in problem-solving around negative behaviors (e.g., “It looks like there were a couple of days where you took your medicine each time you were supposed to…great job! What made it easy to take your medicine on those days? There were also a couple of days where the bottle was only opened once instead of twice…what made it difficult to take all your medicine on those days? What is usually happening during the time that dose is supposed to be taken? What made it easier to take all your medicine on day X compared to day Y?”). In addition, adherence difficulties were normalized (e.g., “It’s just a fact of life – doses are missed. There are a lot of things that get in the way of taking your medicine, like sports, hanging out with friends, etc…but all of these things can be overcome with some planning and teamwork”).
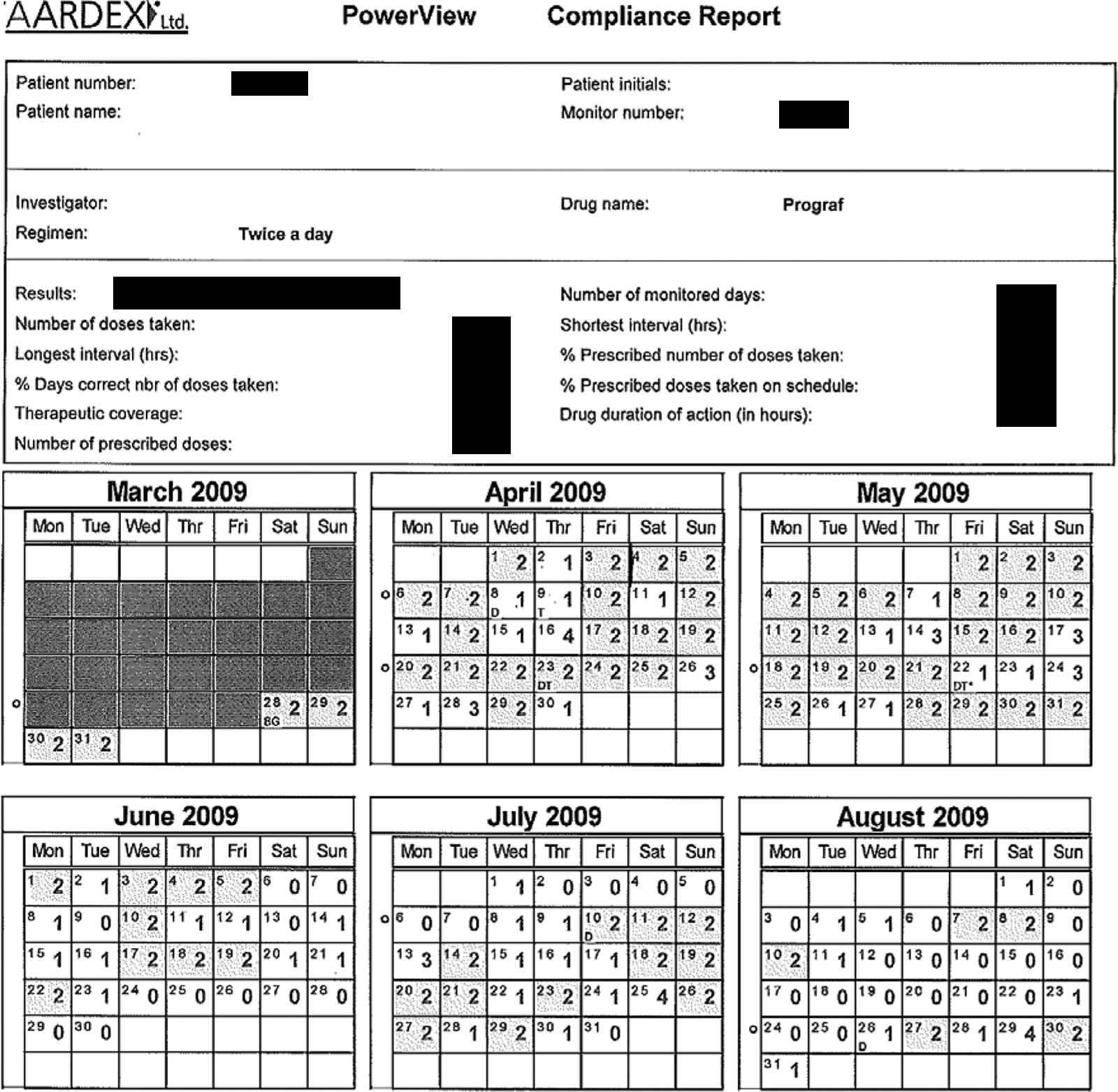
Standard MEMS® bottle calendar plot.
Week to week, adherence promotion treatment was individually tailored to each family’s needs based on family report as well as MEMS® adherence data, and was often comprised of (1) education: purpose and mode of action of medication, the link between adherence and health outcomes; (2) reallocation of treatment responsibility; and (3) guided problem-solving: identifying a barrier to adherence, identifying possible solutions, testing possible solutions, and evaluating the effectiveness of possible solutions. The decision of which treatment component to begin with, as well as which components to utilize during future visits, was based entirely on each family’s specific adherence needs. As a result, the type, number, and order of treatment components varied across each family. The aim of treatment was movement towards greater independence in disease management, sustained adherence of at least 80 percent of all prescribed doses (DiMatteo et al., 2002; Rapoff, 1999), discontinuation of MEMS® bottle, and continued monitoring by medical providers. Treatment termination was planned jointly by the therapist, patient, and family.
Case example 1
“JD” is a 14-year-old African-American male with a diagnosis of focal segmental glomerulosclerosis (FSGS) for which he underwent kidney transplantation at the age of 12. He was referred to a pediatric psychologist at the age of 13 by the nephrology team due to ongoing concerns with the patient’s self-care and the family’s adherence to oral medication. JD’s prescribed treatment regimen consisted of anti-rejection medication (twice daily, 12 hours apart), steroids (taken every 48 hours), antifungal medication (once daily), hypertensive medication (once daily), and aspirin (once daily). At the start of outpatient clinical care for adherence promotion, JD’s mother, a single parent of five children, assumed responsibility for all aspects of disease management. At baseline, JD’s adherence to oral medication was approximately 25 percent, due in part to poor organization of medication (e.g., medication dispersed throughout the house, individual pill containers misplaced) and little understanding regarding the purpose of medication and consequences of nonadherence. The family also identified ongoing disease management strain between JD and his mother and heightened parenting stress as contributing factors to adherence difficulties.
Near the beginning of treatment a joint decision was made with the family and medical providers to electronically monitor Prograf®, one of JD’s anti-rejection medications. Based on the aforementioned barriers to adherence, during 7 outpatient therapy visits spanning 3.5 months, JD and his mother were provided with education regarding FSGS as well as how his specific medications worked to target his illness. Reallocation of treatment responsibility was also provided to identify disease management tasks that JD could practice at home and eventually relieve his mother of primary treatment responsibilities. Guided problem solving targeted JD’s poor organization of medication; he suggested “keeping all medication together” and “using a pill box” as possible solutions and subsequently put these solutions into action. To target inconsistent behavior management by JD’s mother, parent training was provided and focused on developing and implementing an adherence contract, with clear goals (e.g., “taking my Prograf with dinner 4 out of 7 days”) and rewards (e.g., movie night). EM was incorporated alongside these treatment components, in order to promote better adherence. During therapy visits, MEMS® data was downloaded and the family provided with adherence feedback and a printout of JD’s adherence since treatment initiation (see Figure 1 for an example of the actual format of adherence data presented to families). JD, his mother, and the therapist jointly reviewed patterns in improvement in adherence and/or challenges experienced, and treatment was subsequently tailored based on the family’s need.
A time-series model (auto-regressive moving average; ARIMA) was used to examine JD’s medication adherence over time. Time series models are more robust than other parametric tests (e.g., independent t-tests, repeated measures t-test, general linear modeling) in comparing during-treatment to post-treatment changes because they allow data to be modeled across time as opposed to looking at mean differences between two or more time points (Borckardt et al., 2008). Due to scheduling constraints on the part of JD’s family, EM did not begin until approximately 1.5 months post treatment initiation, 12 days prior to the fifth session. Thus, we compared differences in treatment adherence during-treatment and post-treatment. There were 56 days of EM data available during treatment (the family abruptly discontinued treatment due to time constraints after session 7 or day 57 of EM), which were compared to post-treatment adherence (314 days available). JD’s mean percentage adherence to Prograf® during treatment was 95.53% (SD = 29.04%) and decreased to 52.07% (SD = 44.55%) post-treatment (see Figure 2). This decrease in medication adherence was statistically significant as evidenced by ARIMA, t = 3.97, p <.01. Overall, JD’s MEMS® data revealed significant improvements in adherence with participation in adherence-promoting treatment, and immediate declines in adherence with premature termination of this treatment (due to parent-reported caregiver burden and family stress unrelated to treatment). Of note, JD and his mother were also recruited into the Center’s research study and continued to participate after attrition from therapy; as a result, MEMS® data remained available after the family dropped out of outpatient adherence promotion treatment.
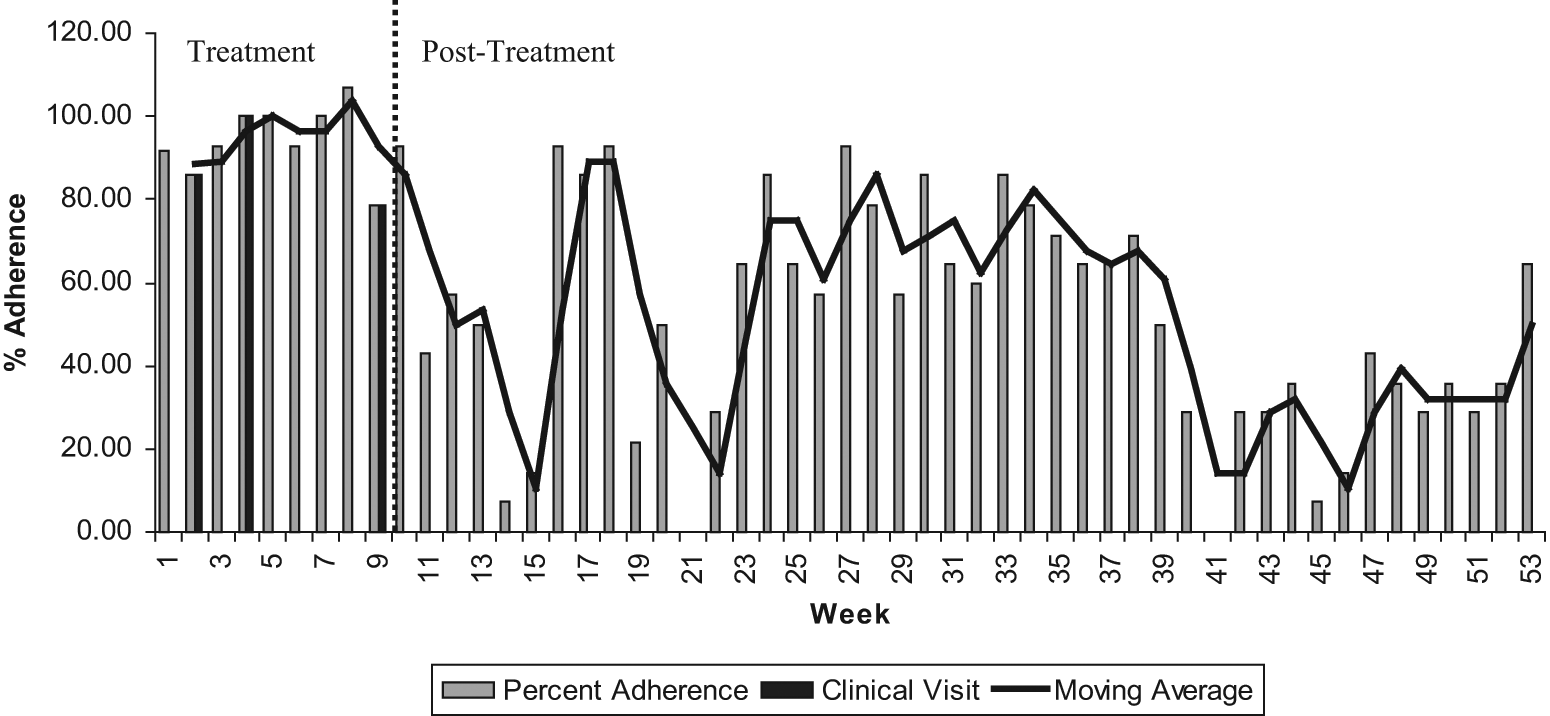
Case example 1: Adherence (%) as a function of adherence promotion clinical visits.
Case example 2
“Sarah” is a 13-year-old white female with a complex medical history since infancy that includes diagnoses of a neurogenic bladder (i.e., a medical condition where the bladder does not empty properly), congenital abnormalities of the intestine, and end-stage renal disease (ESRD). She was referred to a pediatric psychologist at the age of 12 by the nephrology and urology teams due to ongoing concerns with the patient’s self-care and the family’s adherence to oral medication, dressing changes, diet restrictions, and home catheterization. Sarah’s home treatment regimen consists of hypertensive medication (once daily), antibiotics (every 48 hours), phosphate/phosphorus binders (taken with each meal/snack), antispasmodic/anticholinergic medication (once daily), folic acid (once daily), vitamin D (once every 4 weeks), and iron (once daily). To monitor medication taken during lunch on schooldays, Sarah takes medication in the presence of the school nurse. These adherence concerns persisted since early childhood and were contributing factors to Sarah’s worsening kidney disease and poor treatment responsiveness. A kidney transplant was pending and contingent on improvements in disease management and treatment adherence. At the start of outpatient clinical care for adherence promotion, Sarah assumed primary responsibility for all disease management tasks, with minimal parental involvement, despite longstanding poor adherence; per physician and family report, she took approximately one-third of all prescribed medication doses, infrequently changed dressings and catheterized at home, and did not adhere to a prescribed low-potassium diet. Sarah’s poor organization, poor understanding regarding the purpose of medication and consequences of nonadherence, poor allocation of treatment responsibility between herself and her parents, and parenting stress, were all identified as contributing factors to her difficulties meeting chronic illness demands and poor adherence.
The family was provided a MEMS® bottle at the start of outpatient therapy; a joint decision was made with the family and Sarah’s nephrologist to monitor one of her phosphate/phosphorus binders. MEMS® data was utilized in a manner similar to JD. Of note, Sarah and her family were also recruited into the Adherence Center’s research study. Based on the aforementioned barriers to adherence, Sarah and her family were provided education on ESRD and how her medications work to target her illness during weekly or biweekly outpatient therapy visits spanning 1.5 years. 1 Reallocation of treatment responsibility was also targeted; caregiver burden resulting from Sarah’s chronic medical condition made it difficult for parents to participate in disease management, and thus Sarah assumed primary responsibility for self-care and treatment tasks. As such, parenting stress was targeted (e.g., identifying sources of social support and stress relief, seeking mental health treatment) in order to attain greater parental involvement in disease management and achieve better balance between tasks that could be assumed by Sarah versus her family. This also involved identifying other caregivers (e.g., babysitter, aunt, stepfather), enlisting their participation in the therapy process, assigning disease management tasks to each individual, and consulting with Sarah’s school nurse to implement an adherence log for lunchtime medication. Guided problem-solving focused predominantly on Sarah’s forgetfulness in the context of taking evening medication, and caregiver disorganization. The family suggested putting up visual reminders (“Take your medicine with dinner”), placing all evening medication on the dinner table, and close parental monitoring, as strategies to improve adherence. Parent training of behavior management was also provided and focused on developing and implementing an adherence contract (e.g., “taking binders with every evening meal”) with consequences (e.g., losing a favorite item of clothing or accessory). Based on EM data, adherence contracts were strong motivators for Sarah to be adherent to medication. The longstanding nature of Sarah’s health problems was a significant burden and hindrance on Sarah’s quality of life, and she developed a heightened sense of hopelessness towards following prescribed treatment regimen and doctor recommendations. She perceived missed doses as “no big deal” and candidly voiced her frustrations (“I’m sick and tired of doing this!”; “I wish doctors would get off my back!”). Cognitive-behavioral approaches including modifying Sarah’s negative cognitions, identifying pros and cons of taking medication, and taking steps towards increasing Sarah’s involvement in “normal” social activities, were targeted during sessions. Of note, during the course of outpatient therapy, Sarah underwent several extended hospitalizations during which MEMS® bottle use was restricted. Because the AARDEX system enables users to create “non-monitored periods” when a MEMS® bottle is not being used, adherence rates were not affected (see Figure 3).
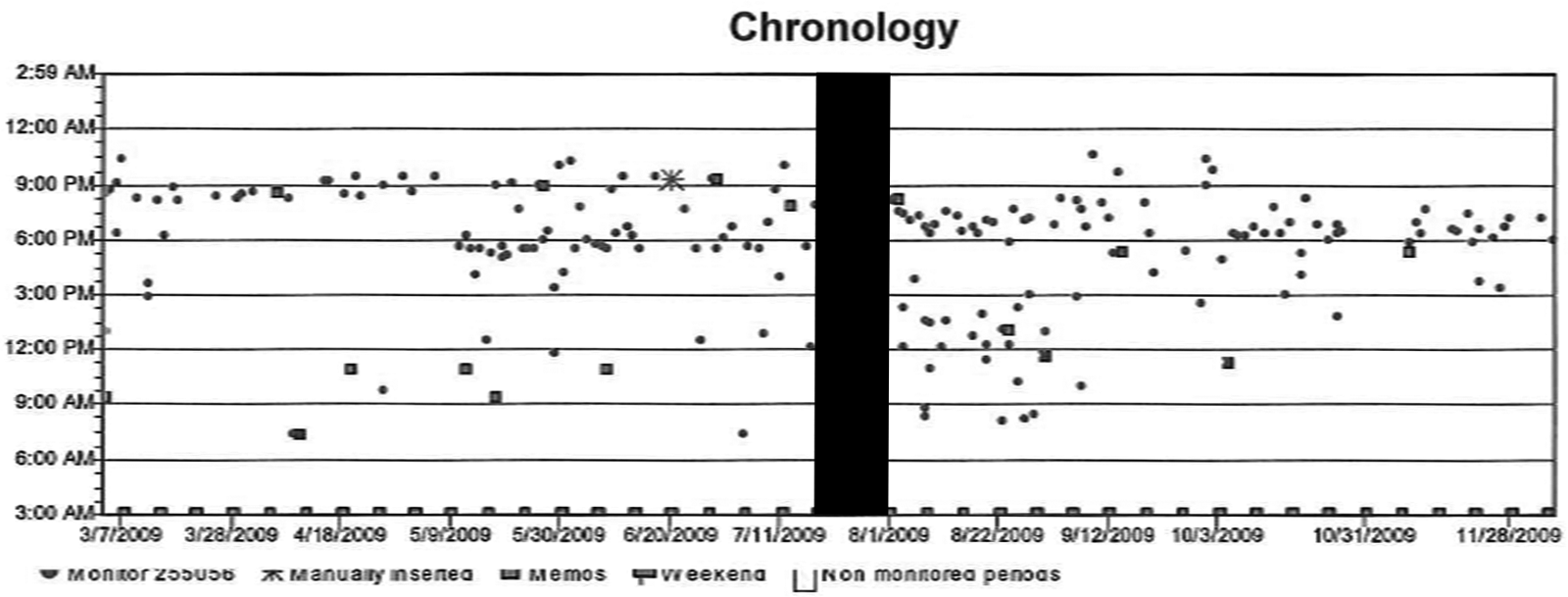
Case example 2: Dose timing scatterplot.
ARIMA was used to examine Sarah’s medication adherence over time. Of note, “non-monitored periods” are treated as missing data, which is accounted for in ARIMA analyses. Also, since Sarah’s treatment is ongoing and comparisons cannot be made between during-treatment and after-treatment periods, adherence trends over time were modeled. There were 512 days of EM data available during treatment; Sarah’s mean percentage adherence to Renagel® over the course of treatment was 39.65% (SD = 28.23%). Mean percentage adherence to Renagel® during the first week of monitoring was 38.89% and 57.14% at the last EM download (week 77). Medication adherence changed significantly over time as evidenced by ARIMA, t = 28.88, p <.01, and a polynomial trend reflects increased adherence over the course of treatment. Overall, although Sarah’s EM data revealed chronic low adherence, over the course of treatment she demonstrated significant improvements in her adherence to oral medication.
Discussion
Lessons learned
Each case presentation highlights many of the benefits of incorporating MEMS® bottles feedback into clinical practice, in combination with other adherence-promoting treatment strategies. First, EM downloads were quick and simple, requiring no more than 5 minutes of the clinic visit. Second, EM feedback enabled active discussions and problem-solving between the child, parent, and therapist that were specifically tailored to the family’s unique adherence barriers and challenges. Third, the presence of objective adherence data facilitated open and non-adversarial discussions regarding adherence. For example, both JD and Sarah endorsed feeling frustrated by physicians’ frequent “check-in” regarding adherence and consequent “talks” about the need for improved adherence and consequences of poor disease management. In contrast, both adolescents found MEMS® feedback non-intrusive and non-confrontational, thereby facilitating their active involvement in their adherence promotion. Families were also highly engaged during MEMS® feedback and enthusiastic about gauging their adherence progress and/or setbacks. Fourth, MEMS® data provided real-time representations of JD’s and Sarah’s medication administration, including the time and date medication was taken, without relying on potentially biased parent/child report. Fifth, graphical representation of MEMS® data was a useful clinical tool for identifying treatment components that were most effective in promoting adherence, or that impaired adherence, thereby making it possible for the clinician to further tailor the intervention to each patient’s unique needs. EM data was interpreted in relation to treatment strategies implemented during prior sessions, thereby allowing the clinician to determine the clinical usefulness of those strategies. For example, the implementation of a pill box did not reveal any improvements in JD’s adherence to oral medication based on EM data; this was confirmed by family report and subsequently discontinued. In contrast, initiating adherence contracts with Sarah was associated with improved adherence per MEMS® data, and this tool remained an asset to Sarah’s self-care and disease management. MEMS® was able to be modified to account for extended hospitalizations or time periods during which the MEMS® bottle was not used; this ensured adherence rates accuracy. Lastly, EM provided objective data that facilitated teamwork and collaborative problem solving with JD and Sarah’s medical providers. For example, when Sarah’s blood work revealed elevated potassium levels, medical providers consulted with the pediatric psychologist to determine whether Sarah’s levels reflected poor adherence to oral binder medication (available per EM data), poor adherence to a low potassium diet, or perhaps, issues related to poor response to medication.
Patients like Sarah also highlight some of the complexities involved in using EM data, particularly in the context of a complex medication regimen. Sarah was required to take her phosphorus/phosphate binders with meals; however, the number of meals she consumed daily varied greatly. In addition, her lunchtime medication was being monitored by the school nurse, not her MEMS® bottle. Both of these issues required reliance on self-report; that is, nurse report for periods not monitored electronically (e.g., lunchtime) and Sarah’s report of the number of meals she consumed daily. This is a commonly used method in patient care, yet self-report is subjective and prone to problems with accurate recall. While MEMS® software is capable of creating different treatment phases based on fluctuations in dosing, patients like Sarah who experience daily fluctuations present a heightened level of complexity in calculating and interpreting adherence data. Finally, it is likely that young patients referred for nonadherence experience difficulty across several medications, not just one. This may require more than one medication to be monitored and, thus, a separate MEMS® bottle for each medication being monitored. This may become burdensome for families and impede, rather than facilitate, adherence.
Limitations of electronic monitoring
Several limitations inherent to EM should be considered. First, MEMS® bottles have been deemed cost prohibitive due to their cost of $110 each. Yet, relative to other routine medical tests and devices frequently used in healthcare, the prohibitive nature of MEMS® bottles lies not in the actual cost, but rather that this technology is not reimbursed by insurance companies. As a result, its use in clinical care has thus far been limited. Use of electronic pill bottles by clinicians also necessitates training to download MEMS® data during clinic visits and organize data for each patient. In the case of the X Clinical Service, research staff provided additional support; however, clinicians were able to download and manage data when research staff were unavailable. In those cases, clinician management of data did not require any additional time. Lastly, EM provides a proxy of adherence and measures “presumptive” dosing (Rapoff, 1999); JD’s and Sarah’s bottle openings do not confirm that medication was actually ingested at the time of each opening. Falsification is a potential shortcoming inherent to all methods of adherence measurement (Rapoff, 1999).
Implications and future directions
We strongly believe that EM feedback can be beneficial to a wide range of pediatric patients referred to standard clinical practice for adherence promotion. To address cost as a potential obstacle to incorporating EM into standard clinical practice, coverage from insurance or pharmaceutical companies may be essential. Continuous glucose monitors (CGMs) in juvenile diabetes provide a useful model for reimbursement of novel medical assessment and intervention. While reimbursement for CGMs by insurance or government organizations remains limited, many health plans are increasing CGM coverage in response to emerging evidence for their clinical effectiveness (Juvenile Diabetes Research Foundation International, 2007; Klonoff, 2005). Future research is therefore needed to replicate findings on the clinical utility of EM feedback in standard pediatric clinical practice. Research that can demonstrate clinically significant improvements in adherence among chronically ill pediatric patients due to EM feedback will be instrumental in providing evidence to insurance companies regarding the clinical effectiveness of EM devices, and subsequent need for coverage of these devices. Future research is also needed to evaluate the differential adherence-promoting effects of providing feedback based on EM, self-report measures, and other objective measures of adherence (e.g., bioassays).
The case studies presented here represent an integral first step in establishing the clinical utility of EM feedback in psychological practice aimed at adherence promotion. Experience in a clinical setting suggests this new technology can be an unbiased and objective tool to facilitate non-adversarial discussions around adherence and complement empirically supported treatment components shown to be effective in promoting adherence among youth. Incorporating EM feedback into treatment aimed at improving adherence among chronically ill children and adolescents is a promising avenue for clinical care that warrants further attention. Additional research delineating the validity of EM feedback in standard clinical practice is needed. Moreover, effectiveness studies documenting the integration of EM feedback with empirically supported treatments could be useful in demonstrating the value of psychology in promoting health behavior change. As healthcare reform moves forward, psychologists have a unique opportunity to contribute to health management and outcomes. Electronic monitoring may prove to be an essential tool in this endeavor.