
Abstract
The use of complementary and alternative interventions is growing and gaining popularity, both in the UK and internationally, with significant financial and emotional implications. Complementary and alternative interventions are often utilised by parents of children with Autistic Spectrum Disorders and research has investigated parental beliefs. There is, however, limited understanding regarding what professionals believe about the use of alternative treatments. In this paper we explore the opinions of a range of different professionals about alternative treatments and found that while some have an open-minded opinion, there was a tendency to hold beliefs that these treatments are ineffective, that they give false hope and have potential to harm the child. We discuss the implications for this in terms of the importance of an open dialogue between professionals and families and consider the importance of this in relation to the popularity of these interventions.
Introduction
Autistic Spectrum Disorder (ASD) is a complex lifelong neuro-developmental condition with no known cure and no universally accepted treatment (Sharpe & Baker, 2007). The causes of ASD are probably multi-factorial, although there is some evidence of genetic and neuro-anatomical differences in individuals (Happe, Ronald, & Plomin, 2006). As a consequence it requires chronic long-term management with treatments aimed at the core features and to maximise functional independence and quality of life while alleviating family distress (Myers & Johnson, 2007).
Treatments for children with ASD tend to be categorised into educational interventions, psychiatric interventions, psychological interventions and social interventions. These treatments are designed to promote socialisation, reduce maladaptive behaviours, address communication, social skills and daily living skills, and promote academic achievement (Myers & Johnson, 2007), which requires a multitude of different health care, social care and educational professionals. These can impose a significant cost to the state and the family (Knapp, Romeo, & Beecham, 2007). Parents of these children tend to expend considerable resources on maximising the potential of their child (Sharpe & Baker, 2007) and although treatments can be fairly extensive, there is limited evidence on their effectiveness.
In addition, having a child with ASD imposes considerable financial and emotional costs on families and carers (Sharpe & Baker, 2007) and the stress in these families is greater than that associated with other childhood disorders (Bromley, Hare, Davison, & Emerson, 2004). Over time parents become frustrated with conventional treatments and can, therefore, explore the use of complementary and alternative therapies for use with their children with the hope that the symptoms of ASD may be alleviated (Hanson et al., 2007; Wong & Smith, 2006). In addition to this children with autism tend to suffer from ancillary symptoms, such as gastric problems or sleep problems, and there are a range of complementary and alternative medicine (CAM) treatments that claim to just target these associated difficulties (Levy, Mandell, Merhar, Ittenbach, & Pinto-Martin, 2003).
Complementary and alternative medicine
CAM is a diverse array of practices not considered to be part of conventional medicine, but while grouped together under one rubric, they are heterogeneous in their ideology and practice (Kurtz, 2008). The use of CAM is particularly widespread in the UK with 10–20% of the population spending approximately £1.5–5 billion annually on these therapies and medicines (Tuson, 2005) and the market continues to grow (Zollman & Vickers, 1999). The rise of CAM interventions can be located within the wider societal trends that relate to changes in conceptualisations of health and illness (Sonitu, 2006). The increasing popularity of CAM thus can be understood within the wider context of cultural development and changes of attitude towards health care and services (Cartwright & Torr, 2005). The exact number of parents utilising CAM for their children with autism is unknown, with studies demonstrating a range of statistics, from 52% (Wong & Smith, 2006) up to 87% (Harrington, Patrick, Edwards, & Brand, 2006).
There are myriad CAM treatments available for children with autism, broadly categorised into five types: mind–body techniques, biologically based therapies, manipulative methods, energy therapies and body-based methods (National Center for Complementary and Alternative Medicine, n.d.). In reality the greater the functional difficulty the greater the likelihood of CAM use (Hanson et al., 2007). In mainstream medical practice there is an increasing reliance on evidence-based practice (Department of Health, 1999). The evidence for the effectiveness of CAM with ASD is, however, controversial with many treatments having not been systematically appraised, or their effectiveness assessed (Golnik & Ireland, 2009; Matson, 2007).
Considering the complexity and diversity of CAM treatments available, it is inevitable that a certain proportion of carers will seek advice from professionals involved with their children. The nature of this relationship is based on their trust and belief that the professional will act in the best interest of the child, but will also have a knowledge and understanding of these alternative treatments. There is limited work on the perceptions and attitudes of practitioners about CAM, with only a small number of surveys in the US and a limited literature in the UK, with the literature on qualitative evidence being even sparser (Maha & Shaw, 2007). This is despite there being considerable value in investigating the attitudes of professionals, such as physicians, towards CAM (Milden & Stokols, 2004). It is, therefore, important that we gain greater depth of understanding of the views of professionals involved in the care of children with autism, as this will have a possible influence on the long-term relationship with families and the care that the child receives.
Aims of the paper
While there is growing research into CAM user perspectives (Hanson et al., 2007) and parental views on the use of CAM for their children with autism (Harrington et al., 2006), what is lacking is a good understanding of health care professionals’ viewpoints (Maha & Shaw, 2007). Maha and Shaw argue that in addition to recognising their views it is more important to explore the rationale behind them, which is addressed by qualitative inquiry. This paper aims to explore the views of professionals working with children with ASD regarding CAMs.
Methods
The data for this paper originates from a larger study on the perceptions of clinical and educational professionals on the diagnosis and management of ASD. This study explored the differences and similarities in diagnostic practice and the variation in management following diagnosis. This research utilised a qualitative approach to interview these professionals about their practice and understanding of ASD. The focus for this paper relates to questions regarding CAMs. The qualitative methodology allowed for an in-depth exploration of the experiences and opinions of professionals to build upon the limited quantitative available evidence. This approach provides an additional dimension to data that gives a ‘real-world’ feel to it.
Setting and sample
For this research, professionals from a National Health Service (NHS) organisation, a community children’s health provider and two Local Education Authorities (LEAs), who employ educational psychologists, were recruited. Although services for children with autism vary significantly throughout the country, this sample is fairly representative of the majority of professionals from these disciplines who see these children outside of a more specialised clinic environment. Most children in the UK do not routinely have access at present to specialist clinics. Furthermore, there is no specialist clinic locally.
Written consent was obtained from departmental managers to approach professional staff. It is acknowledged in the literature that research should have approximately 15 individual interviews and this should be increased according to the diversity of groups and categories represented in the data to reach saturation (Gaskell, 2000). We conducted 26 interviews; our sample included members representing 3 professional categories. These were child and adolescent psychiatrists, community paediatricians and educational psychologists (refer to Table 1). All consultant psychiatrists and paediatricians were invited individually by email and educational psychologists were identified by managers and selected email addresses provided. Although the proportions of individuals from each of the three sample groups were considerably different, this was not a factor that influenced the data collected. In accordance with qualitative quality guidelines (Spencer et al., 2003), recruitment continued until data saturation was achieved in each group (O’Reilly & Parker, in press). A larger sample group was available, but this methodology rendered this as unnecessary.
Recruitment of participants.
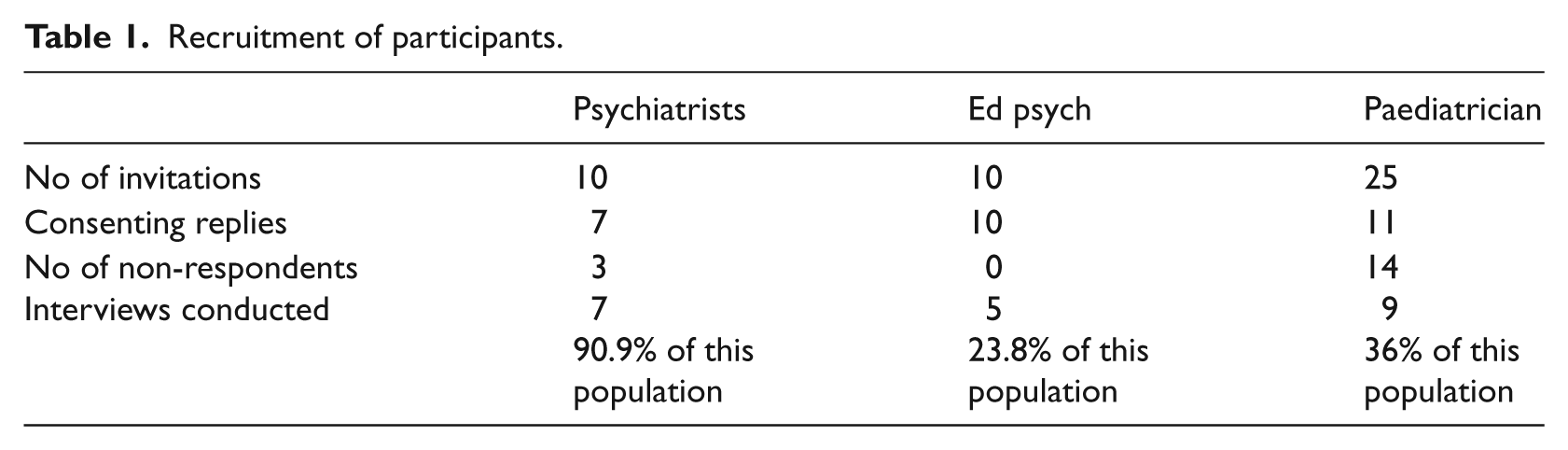
These participants were mostly female ranging in age from early 20s up to early 50s. In this area there is no specialist ASD clinic, so patients are seen by generic clinicians and educational psychologists and thus the numbers of cases vary significantly. For example, in Child and Adolescent Mental Health Services approximately 25% of the workload relates to autism. These groups were recruited because of their close involvement in the diagnosis and management of these children and the data collection process is a reflection of what happens in routine practice. Although the diagnosis and management of children with ASD does include a number of other professional groups, inclusion of all groups was beyond the scope of this research. Although Leicestershire is a multicultural county, the majority of children identified as having ASD are from the White British population.
Data collection and analysis
We utilised semi-structured interviewing to explore professional perceptions of CAM. The semi-structured approach to interviewing allows for a flexibility in the schedule and allows the research to be more participant led (Kvale, 1996). The data for this paper was taken from questions directly related to CAM from a larger interview schedule regarding the diagnosis and management of ASD in routine practice.
We subjected our data corpus to an in-depth thematic analysis due to its theoretical flexibility and meaning-making direction (Braun & Clark, 2006). Thematic analysis allows the research team to draw meaning from the data, allowing the emergence of patterns and the identification of salient issues (Boyatzis, 1998). The data were subjected to verbatim transcription processes and NVivo software was utilised to facilitate the first- and second-order coding process. Through coding, NVivo enhances the identification of salient themes that emerge from the qualitative data (Bryman, 2008). To improve and ensure inter-coder reliability, multiple readings of the transcripts were undertaken by several members of the research team (Boyatzis, 1998).
Ethics
Ethical approval was obtained from the National Research Ethics Service (NRES) in the UK, as some data was obtained from practitioners working within the NHS. The Economic Social Research Council framework for social research ethics was used for guidance.
Analysis
A number of emergent themes were identified. Firstly, some professionals were accepting of CAM and presented an open-minded opinion. Secondly, there is reference to the acceptability of some interventions and not others. Thirdly, there is a general negative perception of CAM, such as false hope, expense of CAM and lack of evidence base. Finally, many professionals reported that they would not actively recommend CAM treatments.
This spectrum of opinions was expressed within each professional group. However, we found that generally psychiatrists tended to be more negative of the concept of CAM, while paediatricians appeared more pragmatic. Educational psychologists had a similar range of views to the psychiatrists, except that some felt unable to comment.
Mainstream treatments were described by respondents during the interview process, but while this is important, it is beyond the remit of this paper. In this locality, there is no agreed treatment package, which is fairly representative of many UK regions. In general there were agreements that particular modes of intervention, such as psycho-education for parents, educational interventions and speech and language therapy, were important. However, there was significant variation in the overall treatment package advocated.
Theme 1: Open-minded opinion
Some professionals reported an open-minded opinion related to the concept and practice of CAM. Although these reports appear relatively neutral, there is some implication that they see some value in these interventions.
1. I don’t have a problem with it [CAM for ASD] and certainly some families find it useful. (Participant 1 – Consultant Psychiatrist) 2. Um I’m always open to new ideas and I think it is good to read around. (Participant 27 – Senior educational psychologist)
In these extracts the professionals report that some families consider CAM interventions useful, and while not directly endorsing this value, they do present an open-minded opinion it. In extract 1 the consultant psychiatrist acknowledges that families can find CAM interventions useful, but qualifies the number with ‘some’, suggesting there are criteria for usefulness. What this indicates is that this professional has had some experience of parents reporting back usefulness of some of the CAM interventions. In extract 2 the professional takes a slightly different approach, arguing that they are ‘open to new ideas’ but still does not assert a positive view of CAM, directly marking it necessary to ‘read around’. This suggests that professionals ought to have knowledge about these alternatives.
Theme 2: Harm to children
A significant issue proposed by the professionals was related to the concept of harm. This interest is inherent in the conceptual framework for the statutory sector in terms of working in the best interest of the child and causing no harm.
As long as it causes no harm
While not directly positively appraising or promoting CAM interventions, these professionals accepted an intervention that would not cause any harm to the child. Parental responsibility usually dictates a non-harmful approach to CAM, as families reported considering safety and side effects when choosing CAM (Hanson et al., 2007).
3. If that’s an avenue they want to go down as long as it’s not going to cause harm to the child I’m okay with it. (Participant 1 – consultant psychiatrist) 4. In a nutshell I think as long as it’s not doing any harm or detriment to the children and the families using it will go along with it. (Participant 16 – consultant community paediatrician) 5. I don’t have problems with complementary and alternative therapy provided first it’s not um going to contradict or be a problem with current treatment the child’s having and secondly it’s not something which is potentially dangerous. (Participant 45 – community paediatrician)
Again these professionals do not actively promote the use of CAM interventions but they show a passive acceptance of the use of such treatments, provided that there is no evidence of distress or harm to the child. Extract 3 claims to be ‘okay with it’ rather than positively promoting or believing in the effectiveness. It is more of a passive acceptance formulated as something that parents engage in to be ‘gone along with’ by orthodox professionals. This is a viewpoint shared by extracts 4 and 5, whereby both paediatricians showed they are prepared to accept the use of CAM for these children but would become more active if they considered something to be ‘potentially dangerous’.
CAM interventions can cause harm
Problematically it is recognised that CAM interventions may have the potential to be harmful and Levy et al. (2003) found that as many as 9% of their sample were engaged in harmful CAM treatments. This is despite the view that CAM use is often associated with a belief that natural remedies and therapies are safer than conventional medicines (O’Callaghan & Jordan, 2003).
6. I think the only advice I would give is that if they’re on any particular medication or any supplement they need to be very careful and thorough about understanding what the drug does and possible complications of the side effects if they are reported. (Participant 5 – consultant psychiatrist) 7. …but there could also be unknown consequences (.) side effects (.) especially if it involves ingesting tablets or being injected. (Participant 6 – consultant psychiatrist) 8. My only caution would be about some of the you know things like for example you know severe dietary restriction um I would caution parents about that because I think it could be damaging to the child’s development so if I thought there was a terrible risk to the child you know I would I would point that out. (Participant 9 – consultant psychiatrist)
In extracts 6–8 the professionals discussed their views of CAM remedies by demonstrating a caution and concern about the possible damage that various ingested versions of CAM can cause to their patients. They proposed the possibility that CAM interventions can cause harm to the child with autism and therefore argued that parents need to express care if using these. These professionals do position themselves as having a responsibility to the child to communicate to the parents about the possible dangers of using CAM interventions. Smith (2005) argues that many CAM treatments can do more harm than good and give false hope to families, and service providers need to make careful judgements to ascertain whether a CAM remedy is plausible.
Theme 3: Negative perceptions of CAM
Data reveals that there was considerable negative commentary regarding CAM. Professionals reported that CAM often fails to work, gives false hope, can be expensive and there is limited evidence regarding its effectiveness.
False hope
Problematically, CAM can be introduced as a treatment and some propose to cure autism (Hanson et al., 2007). Levy and Hyman (2005) report that families often hope there is an external reason for the ASD that may be reversed by alternative treatments that will ameliorate the symptoms in their chid.
9. These are desperate families and if somebody promises them a cure in return for a substantial sum of money many of them feel compelled to make big sacrifices in the hope that this therapy would work. (Participant 6 – consultant psychiatrist) 10. I think there’s a lot of charlatans out there who are exploiting anxious parents. (Participant 11 – educational psychologist) 11. Parents shouldn’t have to be going off to see quacks and told to abandon all this mainstream stuff and just take my quack medicine or do this weird programme and the child will be better you know that’s cruel. (Participant 11 – educational psychologist)
Dawkins (2003) shows that CAM interventions still carry some negative connotations and are referred to by some as quackery, or at least unconventional and unorthodox. In these extracts the professionals recognised some of the feelings that parents experience following diagnosis and report that parents are ‘desperate’ and ‘anxious’. Professionals appear to thus correlate the vulnerability of parents with the CAM practitioners by positioning them as ‘charlatans’ and ‘quacks’. In extract 11 these CAM practitioners are construed as being ‘cruel’. This works to imply a contrast with orthodox medicine, which is described as being ‘mainstream’.
Cost of CAM
A key concern that professionals have relates to the expense of CAM interventions that parents have to find. CAM has a considerable cost to its consumers, but despite this has grown in popularity (Cartwright & Torr, 2005). The time, effort and financial resources that families put into CAM potentially create an additional burden on families (Myers & Johnson, 2007).
12. Um some families get fleeced I must say by the complementary therapists. (Participant 1 – consultant psychiatrist) 13. I guess that the concern is that there are I’m aware of some organisations that sell therapy programmes at a vast expense um with very little evidence that they’re actually suitable for autism. (Participant 3 – consultant psychiatrist) 14. I saw a family recently who paid several hundred pounds to see this private therapist which said they’re going to do another therapy which involved injecting the child with different chemicals. (Participant 6 – consultant psychiatrist)
The extracts show that professionals believed that families were being unfairly exploited financially. This is consistent with the view expressed by doctors that vulnerable patients require protection from expensive ineffective treatments (Maha & Shaw, 2007). All three professionals here used extreme terms to highlight their concerns regarding these exploitations. In extract 12 the psychiatrist employed the term ‘fleeced’ as a way of considering CAM as defrauding families. Similarly, in extract 13 the psychiatrist proposed CAM interventions as being of ‘vast expense’. What this does is position the intervention in a negative way. In extract 14 the psychiatrist provided a particular case as an example of how parents get taken advantage of by CAM representatives.
Lack of evidence
Mainstream therapies are generally grounded in an evidence base and their clinical effectiveness has been subject to peer review, scientific research and strict regulations (Myers & Johnson, 2007). Problematically, the evidence base for many CAM interventions is anecdotal at best, consisting of single case studies, testimonies from parents and one-off cited reports. The evidence is mostly subjective, with potential placebo effects (Smith, 2005).
15. The way I respond to these situations is that I I don’t prevent the family from going and having these therapies but I emphasise the fact that these therapies have a very limited evidence base. (Participant 6 – consultant psychiatrist) 16. I (.) to be honest I didn’t think there was any clear cut research to show to show that it made a difference. (Participant 13 – educational psychologist) 17. I don’t think there’s enough evidence base in most aspects of this for it to be endorsed by health officials. (Participant 16 – community paediatrician)
The professionals in our data corpus showed considerable concern about the limited evidence base for CAM interventions and most of the participants interviewed commented on this issue. In extract 15 the consultant psychiatrist demonstrated an emphasis on this limited evidence base when communicating with families. This is a view supported by the educational psychologist and the paediatrician in extracts 16 and 17, who demonstrated that there is not enough evidence for CAM interventions.
Theme 4: Professional recommendations
The overall theme running through the analysis is that professionals would not generally recommend CAM interventions to families. The data demonstrates that the professionals who work with children with ASD and their families have a range of opinions regarding the use of CAM interventions, but the general consensus amongst them is the expense, potential harm and limited evidence base lead them to the conclusions that they would be unlikely to actively recommend CAM interventions to families.
18. There’s no specific thing that I would recommend my parents that I’ve heard of. (Participant 5 – consultant psychiatrist) 19. Interviewer: Is there anything that you would recommend to the parents that’s complimentary or alternative? Respondent: No. (Participant 43 – community paediatrician)
In these examples the consultant psychiatrist and the community paediatrician from extracts 18 and 19, respectively, are clear and assertive about their reluctance to recommend CAM interventions to families. In extract 18 the psychiatrist argued that there is no ‘specific thing’ that they would recommend to families demonstrating a lack of belief in the effectiveness of CAM treatments and in extract 19 the community paediatrician answers the interviewer’s question with a clear and succinct ‘no’, the absence of a rationale or account making the assertion stand out strongly. While the assertion from the psychiatrist in extract 18 is softer than the others, there is still a clear message that there would be no active recommendations due to the ‘doubt’ regarding the effectiveness.
Discussion
When considering the nature of ASD it is inevitable that families will encounter a number of services and professionals from whom they will seek advice and treatments for their children. Parents often acknowledge that ASD is a complex condition, but often their physicians underestimate how desperate some parents feel about the lack of treatment options (Harrington et al., 2006). In reality, there are a number of treatment options available to ameliorate the impact of ASD on the individual’s quality of life. An adapted cognitive behavioural therapy model, a psychological intervention, has been shown to improve the symptoms of anxiety (Wood et al., 2009) and a number of other interventions have proved useful in social development. However, no treatment can provide a cure, they remain sporadic in availability and can be difficult to implement. CAM proposes to fill the gap in conventional medicine. In reality families may combine traditional interventions with CAM treatments, but this could pose certain risks (Smith, 2005). This emphasises the need for professionals to recognise and be aware of all treatments utilised by families.
Generally professionals are cautious of CAM treatments. While some appear to be open minded and adopt a pragmatic approach, others express much more negative opinions and reservations, a finding demonstrated within all the professional groups. Negative opinions include concerns around potential harm, the limited evidence base for treatments and the creation of false hope for the families. This false hope can result in an economic strain as families attempt to improve their child’s health. While the evidence for some CAM interventions is available, there can be others that may result in serious adverse effects and therefore families need to be correctly informed (Zollman & Vickers, 1999). The difficulty is that although mainstream treatments were considered preferable to CAM, the evidence for the long-term effectiveness of these interventions also remains limited. It is interesting, therefore, that professionals place a higher emphasis on the need for evidence in CAM, which may be a reflection of their professional background.
The general consensus is, however, that CAM offers little therapeutic or physical benefit to children with autism. Some, however, argue that families should be encouraged to explore all possibilities, thus the clinician needs to be armed with information and knowledge to provide support and advise these families (Golnik & Ireland, 2009). Milden and Stokols (2004) found that 76% of patients asked their physicians about CAM and yet 61% of professionals tended to discourage its use, although 81% of physicians claimed to want more information about it. Parents have reported that often the clinician did not ask about CAM use and some parents were concerned that the clinician did not understand or have much knowledge of it (Wong & Smith, 2006). Internationally, physicians may recommend CAM interventions, but there is a significant variation in the advice they provide for families. Interventions such as multi-vitamins and dietary changes are often actively encouraged whereas more controversial treatments, such as delaying immunisations and chelation therapy, tend to be discouraged (Golnik & Ireland, 2009).
The perceptions of parents tends to view CAM treatments as being divided into those that have the potential to ‘cure’ a condition and those that seek to ameliorate the symptoms (Kemper, 2001). In addition, treatments can be used as a replacement for more traditional interventions or as an adjunct to them. This has been seen in a variety of childhood conditions, both mental and physical (Chan, 2002; Kelly, 2004). The illness profile appears to determine how CAM is utilised. For example, in Attention Deficit Hyperactivity Disorder, often viewed as a behavioural problem, treatments are used in both ways (Chan, 2002), while in a life-threatening illness, such as cancer, CAM is used to complement traditional treatments (Kelly, 2004). This compares with autism, which has no specific treatment, is a lifelong condition and parents are frustrated by a lack of cure. The limited nature of the literature on professionals’ attitudes towards CAM (Maha & Shaw, 2007) makes it difficult to compare the attitudes regarding CAM for ASD with other conditions. It does appear, however, that these attitudes are fairly consistent and tend to err on the negative side.
The attitudes of professionals to the use of CAM is a complex issue and may be multi-factorial in nature, reflecting social, cultural, educational and professional beliefs, with personal experience of CAM potentially being very significant. Personal experience of using alternative treatments may influence a professionals’ readiness to support or oppose a family’s use of such treatment, particularly if they have personal experience of autism in a family member. Professionals’ beliefs about CAM cannot be treated in isolation from societal trends. CAM usage is greater in the younger age groups (O’Callaghan & Jordan, 2003; Thomas et al., 2001), has a significant gender difference, with women being more likely to use and recommend it (Kronenberg, Cushman, Wade, Kalmus, & Chao, 2006; Sikand & Laken, 1998), and has cultural differences (Kronenberg et al., 2006; Wong 2009). Some cultures advocate CAM procedures (Wong, 2009) to a greater degree than Western medical philosophy, while some cultural groups have been reported to have a reduced uptake (MacKenzie, Taylor, Bloom, Hufford, & Johnson, 2003). Social trends have reflected a decline in the belief in biomedicine and increase in the significance of the patient’s own experiences and perceptions (Sonitu, 2006). The influence of the media and readily accessible information is difficult to assess but is fairly pervasive (Schmidt & Ernst, 2004).
This can be reflected in the polarised view of CAM and its role in the NHS, with some doctors advocating that it ought to have more priority, with others being against its integration (Maha & Shaw, 2007). Respondents in Maha and Shaw’s (2007) study expressed some concern about raising the profile of CAM and affording it more credibility, and it was felt that there was a need for further quality evidence. It is noted that when professionals have an interest in CAM they are more likely to take initiative to learn more about it (Milden & Stokols, 2004). While general influences from society may influence practice, there are also differences between professional groups, which may reflect differences in training or perceived remit of professional practice. Educational psychologists may often view their role as advisory and, while this may also be present in the medical profession, the asymmetrical relationship can often lead staff to feel more protective of their patients. The societal influences are significant when considering the professional/service user interaction. While in addition to the above factors, professionals will also be influenced significantly by other professionals and the evidence-based practice environment, the service user, however, may be more affected by these factors.
The views of mainstream professionals may contrast with the views of CAM practitioners. CAM practitioners generally hold a positive view of conventional medicine and are able to see the value of traditional treatments and do not hold the position that CAM ought to replace orthodox medicine, but rather that it should be integrated with CAM approaches (Barrett et al., 2004). CAM practitioners report that a key aim of their work is to empower patients and provide them with the mechanisms for them to take responsibility for their own health (Barrett et al., 2004; Kurtz, 2008), which may be seen as one of the important tenets of managing a long-term condition such as autism. The diversity of CAM approaches, however, means that some treatments have potential to be more effective than others, and although CAM tends to be constructed as a homogenous group of interventions, this is not necessarily correct.
In order for professionals to serve the needs of children and their families it is important that they understand the parents’ beliefs about the disorder (Harrington et al., 2006) and have an open dialogue to ensure the best treatment for the child, as parents are less likely to admit to trying CAM methods if they feel judged or get a negative evaluation from the clinician (Levy & Hyman, 2005). This does not mean that professionals need to condone or agree with the use of CAM, but that they need to be sensitive to the patients’ beliefs and sensible in the advice given.
Advice may be sought from the multitude of professionals involved with the families and, while the study was not comprehensive, the three groups sampled represent a broad area of expertise that is highly likely to be consulted for this type of advice. The absence of a specialist local clinic does make the opinions of the varied professional groups more clinically significant. We interviewed a representative sample from each category, ensuring that saturation in each group was achieved. Although caution is essential in interpreting findings due to the non-responders, the nature of the methodology, particularly through achieving saturation, reduces the overall effect on the data and its robustness.
In contrast to some of the larger scale survey designs in this area, the sample size ostensibly appears to be quite small. The use of qualitative methodology does, however, negate much of this discrepancy by allowing a more in-depth, rich exploration of the individual views, which in turn allows for a transferability of findings to broader issues. We acknowledge that our sample was recruited from a limited geographical area, yet we expect these findings are representative due to the diversity of skills and international training and experience of the professionals. These issues were not specifically explored in this study and it may be useful to consider this in future research.
Although this data is based on the professionals’ perceptions of their interactions with families, it would be useful to ascertain what is occurring in actual practice. Possible routes for exploration may include audit of services or interviewing families on their experiences of professional consultations. A difficulty with this area remains retrospective recall of events and, therefore, audio or video recordings of practice would add significantly to both research quality and professional practice. A wider inclusion of the professional groups involved in children with ASD, such as speech and language therapists, clinical psychologists, occupational therapists and teachers, would also be enlightening.
The growing field of autism research and practice, together with increasing numbers of individuals diagnosed with the condition, does raise the question whether children should be seen by all professionals or by specialists. It may be impossible for all professionals to have an in-depth knowledge of all aspects of ASD, including CAM. While it may be possible to educate professionals in the area of CAM as an intervention, it is questionable whether professionals would be engaged and whether this is cost effective.
While professionals may be unhappy with the concept and existence of CAM treatments, in reality the popularity of CAM continues to grow. As such, the increasing popularity of CAM can be understood within the wider context of cultural development and changes of attitude towards health care and services (Cartwright & Torr, 2005). In the era of the health care consumer it is essential that professionals educate themselves concerning the various treatment modalities, both mainstream and alternative, thus enabling them to offer the best available care for their service users.
Due to this growing popularity it is becoming essential that the use of CAM in autism and also other conditions receives further attention from the research community. It is important that families can make informed choices regarding treatments, with access to a rigorous evidence base that explores the effectiveness and value of the treatment options. Ethically, this is potentially quite difficult. While some CAM treatments appear fairly benign, for example, the use of fish oils or pro-biotics, other CAM treatments require significant monitoring or are potentially harmful, for example IV chelation therapy. This poses the challenge of obtaining an adequate evidence base while protecting these children.
Collectively, these factors are significant in commissioning the availability of CAM treatments within the NHS, particularly in this current economic climate. However, families will continue to seek these treatments, which may pose increasing economic burden on families.
Concluding remarks
It is argued that there is a push/pull culture in health care (Cartwright & Torr, 2005). Cartwright and Torr (2005) note that people are pushed away from traditional medical care because of dissatisfaction with services and ineffective treatments for chronic conditions and are pulled towards CAM for a greater autonomy and control over health. This is particularly important with ASD, which is a complex condition with an uncertain outcome. It is important the health professionals who work with this population understand the range of interventions that parents may use and assist families in their choices of treatments and systematically monitor their efficacy (Goin-Kochel, Myers, & Mackintosh, 2007). This will encourage better communication between professionals and families and confidence in their ongoing care. It is essential that professionals develop a trusting relationship with families and are able to give a balanced view of therapy. The medical profession has struggled with the emergence of CAM and, while it dismissed it as quackery in the first instance, it has struggled to reconceptualise its ideas and condemnation to come to terms with its growing popularity (Winnick, 2005).
Footnotes
Acknowledgements
We would like to extend our thanks to Panos Vostanis for his comments on earlier drafts of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
None declared.