
Abstract
This mixed method systematic review appraises the individual, familial and systemic effect of 9/11 and the war on terror for majority and minority children and youth in North America. The results highlight the broad social consequences of the socio-political transformations associated with the terror context, which cannot be understood only through a trauma focus analysis. The social stereotypes transformed youth experiences of belonging and exclusion. The difference between the consequences for majority and minority youth suggests the need for a broader appraisal of this societal context to support the development of prevention and intervention intersectorial programs.
In the aftermath of 9/11, research has documented the magnitude of the consequences of terrorism on the mental health of adults, and to a lesser extent, of children. Early reviews emphasized the association between direct or indirect exposure to terrorist events and symptoms of post-traumatic stress disorder (PTSD) and other anxiety disorders in children (Fremont, 2004), highlighting the difficulties of studying these unpredictable events.
The World Trade Center (WTC) tragedy has been associated with rapid socio-political changes, locally and globally, as a result of the war on terror (WOT) (Ewing & Hoyler, 2008), officially launched by the American administration in the months after 9/11. These socio-political transformations include increased security measures in immigrant receiving countries, increased discrimination against Arab, Muslim and Middle Eastern minorities living in these countries and an escalation in international tensions (Pew Research Center, 2007; Rousseau, Hassan, Moreau, & Thombs, 2011). The impact of this social context on children and adolescents in Muslim immigrant communities is sometimes described as “collateral damage” (Balsano & Sirin, 2007).
Since 9/11, the medical and psychiatric literatures have widely documented the effects of this terrorist event on children’s and families’ symptomatology. In parallel, the social science literature has stressed a qualitative analysis of the transformation in children’s and youth’s social environment as a result of the WOT and its impact on their well-being, sense of identity and development. This apparent divide replicates, to a certain extent, the existing gap between medical studies of conflict and post-conflict trauma and social science research documenting the psychosocial antecedents and consequences of conflict within a social ecology framework (Miller & Rasmussen, 2010).
This mixed method systematic review (MMSR) aims at providing a comprehensive update on the present state of knowledge, building bridges between the medical and social sciences literatures in order to achieve an eco-systemic understanding of the impact of 9/11 and the WOT context on children and youth.
Definitions: Terrorism as an evolving concept
The concept of terrorism is defined officially by the U.S. Department of Defense (1996) as “the calculated use of violence or threat of violence to inoculate fear, intended to coerce and to intimidate governments and societies in the pursuit of goals that are generally political, religious or ideological.”
The fear associated with terrorism has different effects for different communities. In many Western countries, it elicits the majority’s fears and worries about social cohesion and the radicalization of Muslim minorities (Aly & Green, 2010). For these minority communities, the general population’s fear of terrorism and suspicions against those who might be terrorists is experienced as xenophobia and discrimination (Jamil & Rousseau, 2012; Pumariega & Rothe, 2010).
Razack (2008) proposes that the post-9/11 link between Muslims and terrorism should be understood within broader concerns about power relations and race thinking in Western society. Drawing upon Arendt’s work (Arendt, 1973), Razack argues that “race thinking” denies a common bond of humanity between groups based on European and non-European descent and divides the world between the “us” and “them”, projecting onto the “other” the violence associated with “inherent” inequalities of race, ethnicity and religion (Razack, 2008). The WOT thus exacerbates the tensions associated with religious, ethnic and racial attribution, which are markers of minority/majority status (Ajrouch & Kusow, 2007; Jamil, 2013). This has direct consequences for all children and youth, because identity construction is an important developmental task that is directly influenced by their social, political and cultural environment (Balsano & Sirin, 2007). In the case of immigrant children, the conflicts and tensions between the different social spaces that they inhabit (in particular home and school) can affect their well-being and social adjustment (Britto, 2008).
The 9/11 events themselves, although potentially traumatic and anxiety provoking, may be understood in very different ways depending on the youth, family and community environments (Rousseau & Jamil, 2008). In addition, majority–minority tensions associated with the WOT may also have significant mental health consequences due to the timing of terrorist attacks and the publicity given to counter-measures afterwards. In order to address the systemic effects of this context, we decided to review simultaneously studies about the 9/11 attacks and those addressing the WOT, hoping to overcome the implicit polarization that distinguishes them in the literature.
Method
Because of the absence of systematic mixed method reviews on the impact of 9/11 and the WOT on the mental health of children, we proceeded in two steps. Firstly, we undertook a preliminary mapping exercise to systematically gather lists of the existing literature to evaluate the number of studies, their methodological approaches, and to pilot the search strategy in order to formulate a comprehensive search strategy for papers that would meet the inclusion criteria.
The decision to opt for a MMSR was taken after the first mapping of the literature showed that the majority of studies on the mainstream community were quantitative, while studies on minorities were mostly qualitative. As indicated by the Cochrane collaboration, Campbell collaboration and the World Health Organization Measurement and Evidence Knowledge Network (Welch et al., 2010), a situation in which some social groups are not represented in the production of evidence can lead to inequity in reporting the health effects of a form of adversity. This working group recommended selecting criteria for study designs according to their “fitness for purpose” rather than to a strict adherence to the evidence hierarchy. To develop an appropriate search design, we were inspired by the systematic reviews on interventions for immigrants and refugees developed by the Canadian Collaboration for Immigrant and Refugee Health (Tugwell et al., 2010).
The results of the first mapping of the literature led to the following criteria. Firstly, the review should not be strictly centered on diagnosis or psychopathological categories to operationalize children’s reaction to 9/11 and the WOT (Fremont, 2004). It needed to also include outcomes linked to well-being, such as self-esteem, identity and agency, more frequently covered in the qualitative studies. Secondly, the exposure variable was defined to include both 9/11-induced direct and indirect trauma and the social context associated with the WOT. This methodological choice was based on the fact that the hurt and fear stemming from intercommunity tensions cannot be easily distinguished from the impact of direct or indirect exposure to 9/11.
Search strategies for the MMSR
We conceived separate quantitative and qualitative search strategies and opted for a scoring system that would concomitantly appraise qualitative, quantitative and mixed methods studies. We identified medical, psychological and social sciences databases that could contain relevant papers. The medical and psychological databases included Medline, CINAHL, ERIC, Embase, Cochrane, PsycInfo and PILOTS. The social sciences databases included Social Services Abstracts, International Bibliography of Social Sciences, Sociological Abstracts, Academic Search Complete, SocIndex, International Political Science Abstracts, ProQuest, PAIS International and ATLA Religion. We also searched the McGill World Catalogue for books published. Finally, in order to collect a wide array of gray literature on the topic, we individually searched websites of various agencies and organizations for relevant policy papers, studies and other publications, including European Union (EU) agencies, the Pew Center, independent survey institutes and community organizations. The search was defined by the following parameters.
Time frame: A 10-year period from 2001 to June 2011.
Target group: We included all studies about children and youth aged 0–20 years old. We opted for this age limit because of the number of college student studies and the importance of the transition period toward adulthood. Studies on pregnant women, parents and families were also included because of the importance of perinatal stress and the family environment.
Mental outcomes: We considered mental disorder/symptoms, (post-traumatic disorder and reaction, depression, anxiety behaviors, sleep and somatic problems, substance abuse) and positive mental health outcomes, such as well-being, social adjustment (agency, peer relations, self-esteem and identity) .
Two independent reviewers screened the eligible papers, documented their relevance to the MMSR and assigned them to the following categories:
quantitative research studies on children and youth (non-intervention) (including mixed method studies if mostly quantitative);
qualitative research studies on children and youth (including mixed method studies if mostly qualitative);
research studies (all methods) on parents or families;
research studies (all methods) on intervention subdivided into three categories: clinical interventions, community interventions, and intervention directed toward involved professionals;
non-research papers (theoretical-analytical) that could provide background information;
policy-oriented papers and documents;
literature review papers.
Subsequently, the quality of the research papers (quantitative and qualitative) and the intervention studies was appraised using the scoring system for mixed studies reviews proposed by Pluye et al. (2009). Figure 1 presents the resulting flow chart.
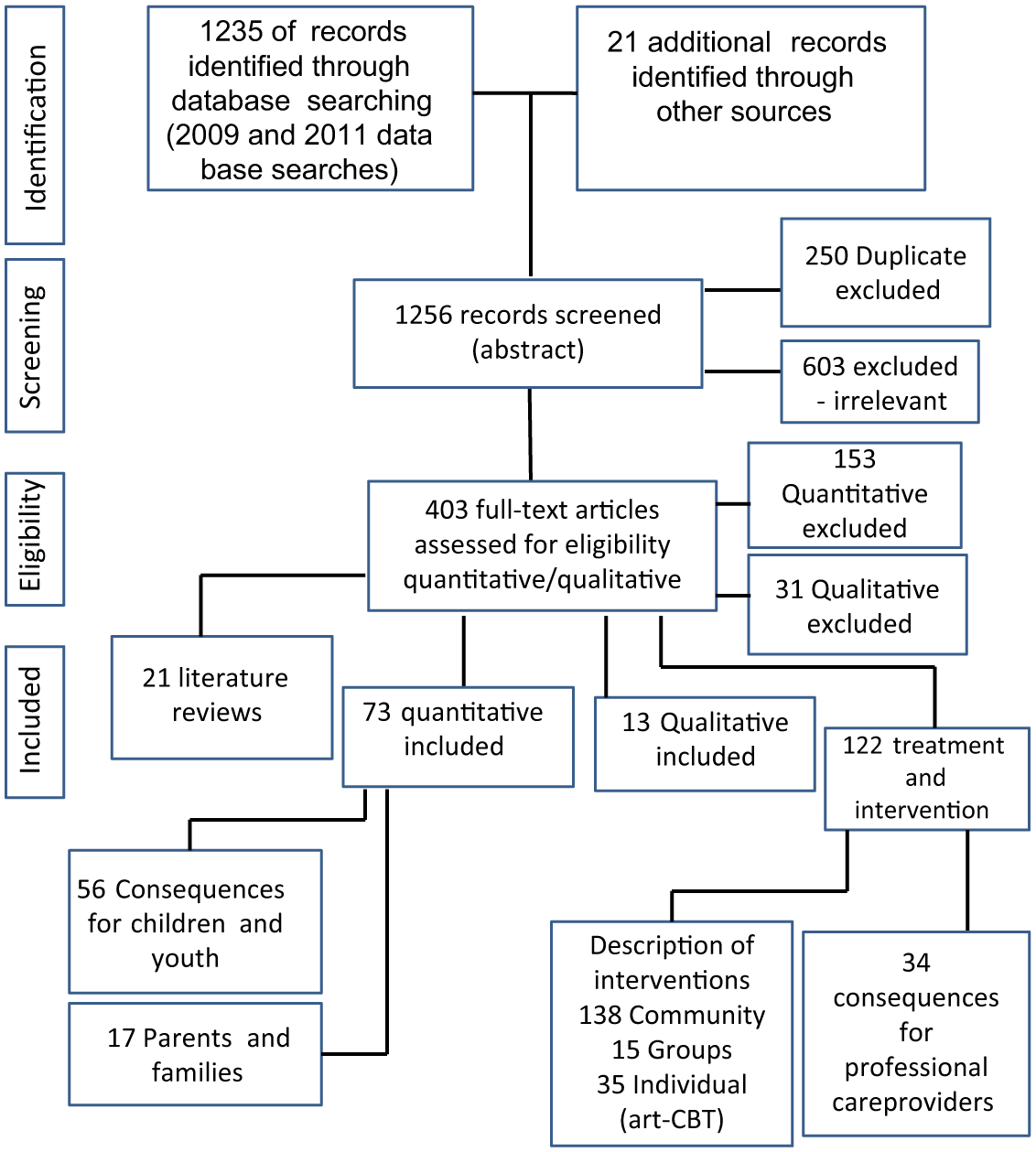
Search and selection flow sheet 2001–2011.
Results
Consequences of 9/11 and the WOT on symptoms and psychopathology
Children’s reactions to 9/11 are strongly related to exposure. Following 9/11, numerous studies have documented the impact of direct exposure for children and youth in New York City (NYC) Masten & Osofsky, 2010). Direct exposure varied as a function of proximity from the WTC, including direct life threat, associated smoke, city turmoil, involvement of family members or people known to the children as victims or as first responders. Indirect exposure through the media and family reactions has also been scrutinized, although the significance of its short- and long-term effects is a subject of controversy (Pine, Costello, & Masten, 2005). In both direct and indirect exposure, the impact of cumulative trauma related to past community and family violence (Mullett-Hume, Anshel, Guevara, & Cloitre, 2008) has a greater impact on the severity of long-term symptoms than high-dose exposure to a single event.
In Western migrant receiving countries, the sense of safety in the public domain and the shattering of cultural and political symbols after 9/11 profoundly challenged the social fabric. They were associated with polarization between “us” and “them” and with the emergence of identities categorized in moral terms of good/bad (Jackson, 2005). Attack-related economic problems were also part of these wide ripple effects that disrupted children’s lives and were directly associated with child psychopathology (Comer et al., 2010).
In addition to the distinction between event versus context adversity, one of the main methodological challenges is linked to the unpredictability of terrorist events, which are, of necessity, studied retrospectively. In the immediate aftermath of 9/11, large, nationally representative surveys documented the first reactions of adults and children in the US. Schuster et al. (2001) described substantial symptoms of stress across the country, with 35% of children presenting with at least one stress symptom and 47% with safety worries. Schlenger et al. (2002), however, reported that overall distress levels were in the normal range, except in the New York area where 60% of adults reported that one or more of their children were upset by the attack. These discrepancies may be associated with methodological issues and, in particular, with the emotional expression elicited by the research topic. In a study on 171 adolescents, Whalen, Henker, King, Jamner, and Levine (2004) found elevated levels of negative affect when adolescents were asked directly about 9/11, while no mood changes were detected when they were asked about their daily activities before and after 9/11. They emphasized the need to distinguish attentional focus generated by the question-asking process (focused distress) from significant clinical distress (ambient distress).
In the following sections, we summarize the quantitative studies on the topic, distinguishing the consequences for children and youth according to their developmental stage (Table 1) and emphasizing, when available, studies based on a comparison with pre-9/11 data. Subsequently, we address associated family and social factors.
Quantitative studies by developmental stage.
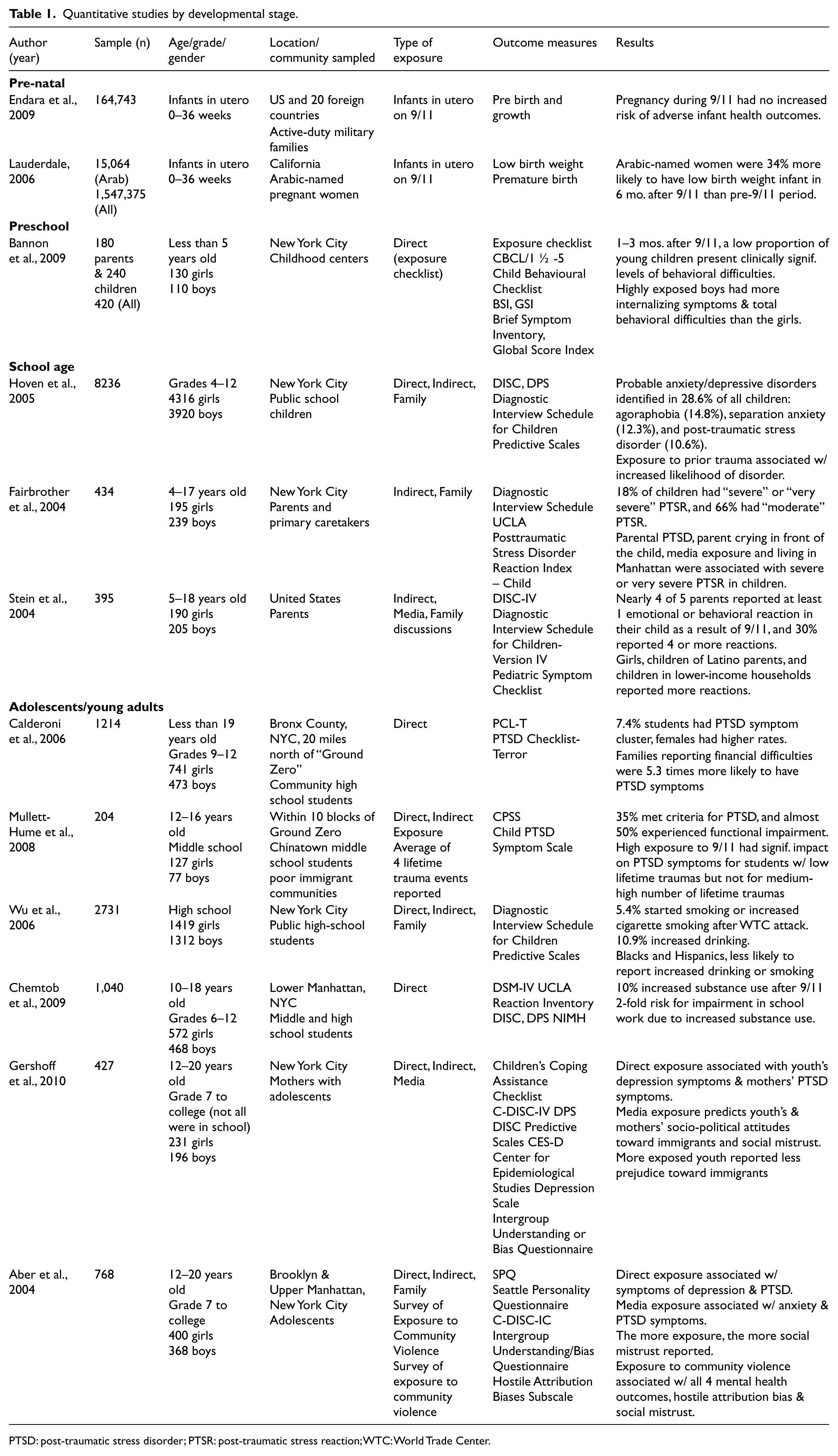
PTSD: post-traumatic stress disorder; PTSR: post-traumatic stress reaction; WTC: World Trade Center.
Prenatal consequences
After 9/11, studies have produced contradictory results about the association between maternal stress and negative infant health outcomes. The examination of a large cohort (n = 164,743) of infants, comparing infants exposed in utero to 9/11 to infants gestating in the preceding and following years, suggest no increased risk for infant health (growth and pre-term birth outcomes) (Endara et al., 2009). In contrast, a well-designed study in the New York area (Eskenazi, Marks, Catalano, Bruckner, & Toniolo, 2007) describes an association between 9/11-related stress and low birth weight. Similarly, a state-wide study in California reports an elevated risk of poor birth outcomes (pre-term birth and low birth weight) for women with Arab names who gave birth in the six months following 9/11 (Lauderdale, 2006). The results confirmed the authors’ hypothesis about the relationship between an increase in discrimination, maternal stress and infant health outcomes, highlighting the impact of terrorism on the social context.
Consequences for preschoolers and school-age children
The impact of 9/11 on preschoolers was largely mediated by family reactions and by the principal caregiver’s emotional availability (Coates & Schechter, 2004). Their reactions are related to exposure (Wang et al., 2006) and gender and may be expressed through internalizing and behavioral problems. Young children also present re-enactment behaviors and patterns of traumatic play (Cohen, Chazan, Lerner, & Maimon, 2010).
Geographical proximity appears to play a key role in school-age children’s reactions to terrorism. According to Fairbrother, Stuber, Galea, Pfefferbaum, and Fleischman (2004), 18% of NYC children reported severe or very severe post-traumatic stress reaction (PTSR), while most of them had at least moderate PTSR. According to Stein et al. (2004), 30% of parents reported more than four emotional or behavioral reactions in their children. Latino parents and low-income households reported significantly more terror-related reactions in children, suggesting an uneven impact across society. Parents’ emotional reactions and television exposure were associated with an increased risk. Older children and boys who were more exposed to the media presented more PTSD symptoms (Saylor, Cowart, Lipovsky, Jackson, & Finch, 2003). Media-inspired intrusive images were strongly associated with the persistence of symptoms (Holmes, Creswell, & O’Connor, 2007).
A few studies based on pre-existing longitudinal research compare pre- and post-9/11 outcomes. In children who were directly exposed to the 9/11 attacks, Lengua, Long, Smith, and Meltzoff (2005) confirmed the increase in post-traumatic stress symptoms at levels comparable to those in children directly exposed to disasters. The authors highlighted differences according to ethnicity, with African American children being more upset than white, Euro-American children. Pre-attack stress load, pre-existing anxiety and maternal worry predicted children’s reactions (Hock, Hart, Kang, & Lutz, 2004; Lengua et al., 2005). However, some studies did not find any differences in children’s psychopathology before and after 9/11 (Henry, Tolan, & Gorman-Smith, 2004). One documented a temporary decrease in behavior problems 4 months after the attack, with a return to the baseline levels 6 months after (Stuber et al., 2005). This supports the idea that children’s reaction to stress may be linked in complex ways to the appraisal of danger and their maturational processes (Pynoos et al., 2009).
Adolescents and young adults’ reactions
There is a large body of literature on the psychological reactions of adolescents and young adults to 9/11. Some discrepancies are important to highlight. Some studies underlined the heavy toll of 9/11 on youth mental health, provoking an immediate psychological distress that subsided after several months (Matt & Vázquez Valverde, 2008). Others emphasized that the majority of youth reported no increased problems (Gould, Munfakh, Kleinman, Lubell, & Provenzano, 2004). Proximity stood out as an important factor for anxiety-related symptoms in adolescents (Blanchard, Rowell, Kuhn, Rogers, & Wittrock, 2005; Callahan, Hilsenroth, Yonai, & Waehler, 2005). Some longitudinal studies suggested that the exposure to terrorism may have a prolonged effect either on this age group as a whole (Blanchard et al., 2005), or on a restricted group of vulnerable individuals (Callahan et al., 2005; Gould et al., 2004). Others indicated that anxiety and depression symptoms were mild, transitory and not clinically significant (Matt & Vázquez Valverde, 2008).
Overall, females had more psychological distress than males (Ford, Udry, Gleiter, & Chantala, 2003; Ray & Malhi, 2005). They also tended to use more emotion-based strategies, while males reported higher levels of disengagement responses. The latter was associated with poor outcomes, but only for females (Wadsworth et al., 2004). Exposure to terrorism was also associated with increased substance use, which affected adolescents’ school work, academic performance and behavior (Chemtob, Nomura, Josephson, Adams, & Sederer, 2009; Wu et al., 2006). Adolescents who were vulnerable because of previous exposure to violence and trauma (Mullett-Hume et al., 2008; Nixon & Nishith, 2005) or a pre-existing anxiety disorder were more likely to have significant anxiety and depressive symptoms and to be at risk for PTSD.
The protective role of parents and families
Families play a key role in modulating children’s reaction to terrorism because they are their primary life milieu. Parents’ personal characteristics and previous mental health problems (depression and PTSD) were associated with children’s symptoms, particularly in preschoolers (Chemtob et al., 2010; Nomura & Chemtob, 2009). The 9/11 context also affected parenting, with different consequences according to the child’s developmental stages (Mowder, Guttman, Rubinson, & Sossin, 2006). In young children, the assistance of parents to cope with media exposure and parents’ emotional openness played an important role (Lutz, Hock, & Kang, 2007; Phillips, Prince, & Schiebelhut, 2004). In adolescents, parental unavailability to discuss the events and parent–adolescent conflict was associated with more psychological distress (Gil-Rivas, Holman, & Silver, 2004; Gil-Rivas, Silver, Holman, McIntosh, & Poulin, 2007).
The terrorism-related social context is particularly difficult in the case of family grief (Abbott, 2009; Chemtob et al., 2007; Possick, Sadeh, & Shamai, 2008). A small study reports the hidden grief of South Asian families who lost a relative in the WTC attacks (Inman, Yeh, Madan-Bahel, & Nath, 2007). The simultaneous experience of discrimination, because they were perceived as potential aggressors in their neighborhoods, interfered with their mourning process.
Social factors and their consequences for psychological distress
A relatively marginal, yet significant, set of studies emphasizes the social heterogeneity in the consequences of 9/11 on American youth. Socioeconomic precariousness, with its associated poverty and violence in inner cities, may be a risk factor for PTSD in adolescents after terrorist events (Calderoni, Alderman, Silver, & Bauman, 2006). Ethnicity also influences youth reactions to terrorism, particularly in the causal explanations of the event (Walker & Chestnut, 2003). Negative and positive outcomes linked to the event varied among ethnic groups as a function of their feelings of personal and collective threat (Milam, Ritt-Olson, Tan, Unger, & Nezami, 2005). The 9/11 context also had an impact on minority–majority relations, youth social development, stress symptoms associated with increased hostile attribution bias and social mistrust (Aber, Gershoff, Ware, & Kotler, 2004).
Other Western immigrant receiving countries also reported negative consequences of increased community tensions on youth. In Europe, post-9/11 Islamophobia was linked with an upsurge in verbal and physical discrimination and associated with increased vulnerability for minority youth (Ramberg, 2005). A large comparative study of Muslim and non-Muslim youth in three European countries showed a strong correlation between discrimination and feelings of alienation (Fundamental Rights Agency (FRA), 2010).
Social consequences of 9/11 and the WOT for children and youth
Although the consequences of 9/11 for mainstream children and youth are mainly assessed through a psychological framework, the social impact of the WOT on minorities and in particular in Arab and/or Muslim communities is mostly represented in qualitative studies in terms of issues of identity negotiation, belonging and social relations between them and the host society. Three major themes emerge from the literature: (1) increased negative stereotyping, discrimination and marginalization; (2) the challenges of identity negotiation as youth; and (3) the coping strategies of individuals and communities to live within this socio-political context.
Discrimination and marginalization
Uniformly, in all studies, subjects felt there was increased negative stereotyping, bias, suspicion and discrimination towards them as Arabs, Muslims or being associated with Middle Eastern countries. Although negative social perceptions about these communities were present in American society before 9/11 (Cainkar, 2009), often overlaid with racial bias (Jamal & Naber, 2008), after the terrorist attacks, the dominant discourse connecting them with violence and terrorism intensified. Evidenced by the number of American studies in this literature review, the effects were felt very strongly by American Muslim youth, living in a country that was the site of the 9/11 terrorist attacks.
The social consequences affecting children and youth played out in schools and on campuses in different communities. Among children, Kromidas (2004) described how fourth graders in a NYC school stigmatized South Asian and Muslim classmates through their construction of a racialized enemy. Among college-age Muslim youth, many felt they were under increased pressure, leading to feelings of social exclusion, alienation and marginalization. Racial and religious-based discrimination seem to be intertwined in the experiences of Muslim youth (Hopkins, 2004; Sporton, Valentine, & Nielsen, 2006).
Identity negotiation
The WOT context has called into question on their identities as American and Muslim and the sense of belonging of immigrant youth. The existing challenges of negotiating identity and belonging between family, peers and community, which are part of the process of growing up, were intensified for young people as they come of age in this socio-political context (Naber, 2005). For second-generation on immigrant youth, their position also creates an additional tension in their process of identity negotiation (Sirin & Fine, 2007). The literature highlights the fracturing and polarizing effects for some teens and college-age Muslim youth of both sexes. Sarroub (2005) found that Yemeni American Muslim schoolgirls in Michigan felt they were failing at all three of their identities. Sirin and Fine (2007) reported that Muslim boys (ages 12–18) were more likely to feel the divisions between constructions of “us” and “them” as Americans and Muslims than the girls in their focus groups. Other studies highlighted the fluidity and malleability of the youth identities as part of a negotiation process (Ewing & Hoyler, 2008; Zaal, Salah, & Fine, 2007). While some distanced themselves from their identity as Americans in favor of renewed self-affirmation as Muslims (Ewing & Hoyler, 2008; Peek, 2003), others renegotiated their American identities to include their critique of American foreign policy (Zaal et al., 2007).
This identity negotiation has transnational implications because of the ways that Muslim immigrant youth identity is connected to wars in other parts of the world (Sporton et al., 2006). For example, the suffering of Afghanis and Iraqis in their respective countries was a source of empathy and identification for some Muslim youth in Bradford as part of a shared position of marginalization and suffering of Muslims globally (Güney, 2010).
Coping responses
Despite the negative impact of the WOT context for many minority Muslim and Arab communities, the literature highlights the emergence of positive coping strategies. Among college-age youth, there was an increased sense of community cohesion in their local Muslim communities (Ewing & Hoyler, 2008) and positive outreach and efforts to raise awareness of Muslims on their campus (Peek, 2003) and in society. This may in part be a gendered response, as young Muslim women felt a strong moral responsibility to both present a positive image of themselves and their communities to the external host society and to protect their families from knowledge of the discrimination they have experienced (Zaal et al., 2007). In a different study, younger teenage Muslim girls (ages 12–18) believed more strongly in the value of positive outreach efforts to dispel negative stereotypes than Muslim boys (Sirin & Fine, 2007).
Another important source for coping strategies is at the family level. Rousseau & Jamil’s (2010) family-based study with South Asian Muslim parents and their children (ages 8–12) and youth (13–18) explored how family communication and coping strategies were mirrored between parents and children. Parents who felt a greater sense of agency and expressed a complex view of the wars in Afghanistan and Iraq had children who were likely to exhibit the same types of responses. Conversely, the children of parents who felt more helpless in coping with the wars and preferred to avoid discussing the current conflicts with their children also displayed avoidant responses and feelings of helplessness.
Interventions: From the child to the community
The WTC catastrophe mobilized mental health professionals who have developed and implemented an impressive array of interventions addressing children and family needs. A number of these initiatives have been described, but very few have been evaluated and numerous questions remain unanswered about their effectiveness.
Overall, community-level mental health service use increased after 9/11 (Boscarino, Adams, & Figley, 2011). Help-seeking for children was related to direct exposure (DeVoe, Bannon Jr, & Klein, 2006) and to parental distress (Stuber et al., 2002a). Approximately 10% of New York children received some form of counseling, mostly through schools (Stuber et al., 2002b). The gap between needs and service use was emphasized by different authors (Ford, 2004) in the direct aftermath of 9/11, but unmet needs were not further mentioned in the following period. It is thus difficult to appraise whether or not this resource mobilization was effective or insufficient.
Different models of bio-psycho-social assessments of the needs of children confronted with terrorism were proposed (Demaria, Barrett, Kerasiotis, Rohlih, & Chemtob, 2006; Paasivirta et al., 2010). Koplewicz, Cloitre, Reyes, and Kessler (2004) identify key elements to plan effective mental health services for children affected by terrorism: awareness of the parenting response, context sensitivity and, in particular, feasibility and acceptability to the community as well as flexibility and diversity in the development of programs intended to maximize community and family engagement.
The largest treatment initiative was organized by New York State, which created a consortium to provide evidence-based treatment to 700 of the most affected children (CATS Consortium, 2007). The consortium trained and supervised 174 clinicians to deliver trauma-focused cognitive behavioral therapy (CBT), primarily to Latinos (65%) and children from low-income backgrounds (58%) (Hoagwood et al., 2007). Six months after the intervention, both the children who received trauma-focused therapy and those who received the brief CBT skills had improved (CATS Consortium, 2010). Because of the naturalistic design, however, it is not possible to know the outcomes for children with similar levels of trauma who did not receive treatment. Universal interventions were offered to all children irrespective of symptomatology, using mainly elements of expressive therapy, body-oriented strategies and parental involvement (Berger, Pat-Horenczyk, & Gelkopf, 2007).
Because of the extent of community exposure to terrorism and of the collective nature of trauma, group therapy for children, youth or parents was widely implemented (Burlingame & Layne, 2001; Maccoll, 2007). Group therapy, mainly trauma focused, was used alone or in synergy with individual treatment (Phillips, 2009). Developmental issues, which interact with traumatic reactions, were at the forefront of adolescent group therapy (Aronson, 2005; Holmes, 2005).
Diverse school-based programs were developed to alleviate psychological distress and traumatic symptoms associated with a terrorism context (Weist et al., 2002). A first set of programs was trauma focused and targeted children presenting symptoms, as in the case of the CATS consortiums and others (Brown & Bobrow, 2004). A second set of programs consisted of universal interventions offered to all children irrespective of symptomatology, using mainly elements of expressive therapy, body-oriented strategies and parental involvement (Berger et al., 2007). A third set of school programs addressed the intercommunity tensions associated with the WOT in multiethnic communities (Auger, Seymour, & Roberts, 2004; Baum, 2005; Felix et al., 2010). These school-based programs promoted a respectful understanding of the multiplicity of meanings associated with this context (Rousseau & Machouf, 2005) and encouraged a respectful awareness of the Other (Hassim & Cole-Adams, 2009).
Community interventions
Community intervention through public education campaigns and the mobilization of all institutional and community instances were an important part of the reestablishment of a safe and supporting environment for children after 9/11 (Koplewicz et al., 2004; Walsh, 2007). Few studies have evaluated the impact of community interventions. There are, however, preliminary indications of an association between a positive emotional climate in the community and an increase in social support and post-traumatic growth at the individual level (Vázquez & Hervás, 2010).
Psycho-education was been a major response to terror-related community reactions (Howard & Goelitz, 2004). However, a review of the different materials revealed discrepancies in what is recommended to parents and teachers. Many parents’ guides assume community homogeneity (Shapiro, 2002). For example, although the American Academy of Child and Adolescent Psychiatry (AACAP) recommended teaching tolerance and avoiding stereotyping, they advocated for coordination between home and school (AACAP, 2003) and a “moral clarity” position that may not acknowledge the wide gaps between majority and minority families’ experiences (Rousseau & Machouf, 2005). This raises important, but as yet unanswered, questions about the kind of messages that can simultaneously be reassuring for all children, while protecting the social fabric from further polarization.
Helping and supporting professionals
Taking care of terror-related reactions can be a difficult task for professional caretakers. Numerous papers address the reactions of social workers, psychologists, pediatricians, nurses and psychoanalysts, among other service providers (Lindy & Lindy, 2004). The powerful collective meanings attached to terrorism raise issues of therapeutic neutrality (Tummala, 2005). They may introduce a particular proximity between the patient and the therapist because of the “shared” trauma (Tosone, 2006) or provoke uncertainties and fears when the clinical encounter becomes a space in which similarities and differences evoking terror are re-enacted (Brothers, 2003).
Discussion
Overall, this MMSR confirms the importance of 9/11 and the associated context of the WOT for children and adolescent mental health, while highlighting empirical gaps between studies on majority and minority groups and disciplinary gaps between clinical/medical and social science approaches to understanding the effects on mental health. In the epidemiological literature, the emphasis on psychological distress and trauma-related symptoms, although important, is phenomenological and does not address meaning or processes leading to hurt or dysfunction. However, it is often built on underlying assumptions that associate symptomatic manifestations with direct or indirect exposure to the event (9/11). The social sciences literature reveals that the path to distress can be quite different for minority and majority children and youth. It highlights the way in which the WOT affects the identity construction of minority youth and their sense of belonging to the host country. In both cases, for minorities and the majority, the terrorist attacks shattered the sense of safety of children and youth, provoking or reactivating anxiety and anger, and transforming their vision of themselves, the “other” and the future. The long-term psychological and social consequences of this are still being played out, often in dramatic ways, in terms of minority–majority relations in North America and other immigrant receiving countries.
At the intervention level, these results suggest that there is a need to widen the assessment frame of terror-related problems and to broaden the scope of interventions to address them. Clinical and community assessments of the mental health impact of terrorism and the WOT should take into account three main factors.
Terrorism events and the WOT are man-made traumas that are embedded within strong collective ideological networks of meaning and their inhumanity may shatter basic trust. In the case of terrorism, the unpredictable nature of the danger and the nebulous profile of the “enemy” introduce a high degree of uncertainty that may further decrease children’s sense of safety, either because they fear being a potential target or because they become the object of suspicion and exclusion.
There is some evidence that vulnerable children and families are more affected by terrorism and the WOT. This vulnerability may come from constitutional factors (previous mental health disorder), familial factors (conflict) or social and cultural factors (socioeconomic precarity, minority status).
In immigrant receiving countries, the consequences for minority children and youth may be more difficult to address within mainstream health and education services because of the avoidance of the families and the prejudices of the host countries’ institutions. In the local context, clinicians need to be aware of the impact of intercommunity tensions on children, such as exclusion or bullying, and not assume that discrimination experiences will be reported.
The review also suggests that immigrant receiving countries should broaden the scope of their interventions. Although there is certainly a role for trauma-focused interventions after terrorist events, a resilience building emphasis seems to be promising. When applied in multiethnic societies, these types of interventions need to go beyond a strong condemnation of violence and integrate in a thoughtful way the diversity of meanings associated with the events and their consequences for children. Although the promotion of strong cohesion around a unified ideological meaning may be protective in the short term for children, it may further aggravate social divisions. Psycho-educational interventions, which are commonly used, need to represent social diversity and foster a culture of solidarity and peace, which go beyond political correctness and encourage moral complexity and awareness of the other (Rousseau & Machouf, 2005).
At the research level, attention needs to be paid to the specific impact of the terror context on children and youth and, in particular, to the role of psychological development, gender, social and cultural variables. Indirect effect should not only be conceptualized as media exposure. Rather, the complex interactive effect of terrorism and the WOT on children’s family and local social environments needs to be better understood. The homogeneity of communities should not be assumed. At the methodological level, caution should be given to the contamination of results by the emotional/ideological dimension of the topic, which may result in exaggerating or minimizing the impact of events and of the context. While anxiety disorder and PTSD should be considered, functioning and social outcomes should also be given more importance. When little is known about specific communities, mixed methods may provide valid data and uncover some of the existing blind spots. Finally, more interventions addressing the wide range of consequences of this context need to be developed and vigorously evaluated.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.