
Abstract
Typically the social-emotional development or mental health of under 5-year-old Children in Care (CiC) is not routinely assessed and there are few published data in the UK on the prevalence of difficulties for these children. Our hypothesis was that there could be a significant level of unidentified and unmet need within this group. A screening procedure was developed and piloted in a 12-month study assessing both child factors and the developing relationships between children and their caregivers. Previous screening studies have shown that recommendations for interventions are not reliably expedited. An intervention component was incorporated to address this and minimise delay in the children and their carers receiving support. Close inter-agency collaboration was integral to the establishment, implementation and high level of participation in the study. The screening proved acceptable to the majority of birth parents and caregivers, with 94% uptake of participants. In the year prior to screening only 10% of under-fives coming into care were identified as having difficulties in contrast to 67% of children in the screening cohort. The brief interventions offered were taken up in three-quarters of cases, leading to increased referrals on and access to mental health services for these children.
Introduction
There is strong evidence that 70–80% of Children in Care (CiC) have extensive needs that require skilled professional help in order to achieve positive outcomes (Ward, Holmes, Soper & Olsen, 2008). Research to date has tended to focus on the emotional and behavioural disorders of school-age children, perhaps as it is harder to produce specific and reliable diagnoses for very young children. However, there is substantial evidence that early patterns of behaviour and functioning are established to a degree that they can have a long-term influence through childhood and into adult life (Anda et al, 2006; Keenan & Wakschlag, 2000) leading to experts in the field (Milburn, Lynch & Jackson, 2008; Sempik, Ward & Darker, 2008) to call for more research into the presentation and needs of the under-fives CiC group.
Where information is available on the difficulties that babies and very young looked-after children experience, it points to this group having multiple developmental risks at an early stage. These include risks from constitutional, prenatal adversity (e.g. maternal drug and alcohol misuse, domestic violence and stress in pregnancy), prematurity and birth complications, and high levels of postnatal neglect or abuse and early disrupted or disturbed care-giving experiences. These in turn can lead to infants and young children being harder to care for once they become CiC (Stovall & Dozier, 2000).
Sempik et al. (2008) reported from a retrospective study of Social Services case notes that 20% of children under five entering care in the UK showed emotional and behavioural problems. Jee et al. (2010) compared the identification rates of children’s social-emotional difficulties in a baseline period of routine assessment prior to, and then after, the introduction of a standardised screening tool. The authors reported that combining a standardised questionnaire with clinical assessment led to a six-fold increase in the identification of mental health difficulties (24%) in under-fives in foster care.
Access to mental health services for under 5s Children in Care
There are few published data on access to Child and Adolescent Mental Health Services (CAMHS) for CiC under 5 years of age in the UK, which may reflect a tendency not to refer among this age group. We know that needs remain unidentified in this group, but for CiC there are additional issues that may impede access to CAMHS that include temporary and/or uncertain placements, and that the child may often be placed out of borough, and/or subject to ongoing legal proceedings. In a comparable high-risk group of children in the US, Burns et al. (2004) reported that 32% of 2–5-year-olds who were in contact with child welfare services had emotional or behavioural problems, while only 6.6% had contact with any mental health services. Even with older children, many children’s needs are overlooked or not addressed in CAMHS (Whyte & Campbell, 2008).
Typically the social-emotional development and mental health of under 5-year-old CiC is not routinely assessed, and young children would only come to the notice of CAMHS when more severe behavioural difficulties occur in foster care or possibly at the point of a significant transition for the child, such as a placement breakdown or when moving from foster care to adoption. Observing the significant degree of distress and difficulty the children were experiencing when referred to our service raised questions of how long their problems had existed and whether they could have been alleviated at an earlier stage. This gave rise to our hypothesis that there could be a significant level of unidentified and unmet need within the under-five CiC group.
Since this project began, guidance has been drawn up by the National Institute for Health and Clinical Excellence (NICE) and the Social Care Institute for Excellence (SCIE) (2010), stating that services for looked-after children should ensure that “all babies and young children are assessed by a specialist child mental health worker to ensure the child does not exhibit signs of emotional distress (for example, children or babies who may exhibit passive, withdrawn or over-compliant behaviour)”. Furthermore, the guidance states that services should “offer early and preventive interventions for babies and young children to avoid placement breakdown and reduce the impact on a child’s potential to develop meaningful relationships in the longer term”.
The project area
The inner London borough where the project took place is a densely populated area with high levels of socio-economic and health difficulties: approximately one-third of dependent children live in poverty, and a similar proportion live in households reliant on workless benefits. The borough has one of the highest infant mortality rates in England and a higher than national average proportion of low birthweight babies (lower than 2500g).
The borough has a high number and proportion of CiC; in 2012 the proportion of CiC – 94.2/10,000 – was the highest in London. At any one time, there are around 115 CiC under the age of five, which represents approximately 20% of the total looked-after population. Approximately 75 babies and children come into care each year, and the majority of them remain in care for several weeks/months. The borough has a dedicated CAMHS CiC team with close working relationships with Social Services and Child Health, despite which early identification of difficulties remained low. In the year prior to the project, only eight children were referred to the service, 7% of the total under-fives CiC population.
The screening process
Considerable thought was given to the structure of the screening process in order to maximise its acceptability to all the stakeholders (children, birth parents, carers and professionals). Our local paediatric colleagues played a key role in supporting the screening. There is also evidence that combining a social-emotional screen at the time of a paediatric review helps to facilitate access to a child mental health service, should that need arise (Briggs-Gowan, Horwitz, Schwab-Stone, Leventhal & Leaf, 2000).
The screening process was structured in order to capture information on the child’s development, physical and mental health needs, and to assess the quality of the child’s relationship and interaction with their caregiver(s). Zeanah, Berlin & Boris (2011) emphasise the importance of attachment theory when evaluating young children in foster care, and note that this may require practitioners to move from viewing difficulties as existing within an individual child to viewing them as existing between caregiver and child. Early patterns of attachment interaction are established in the first few days and weeks of a child being placed with a new foster or kinship carer (Stovall & Dozier, 2000) so assessment early on in the child’s life in care is important. Young children not only have a high level of dependency on their primary caregivers, but there is much evidence to indicate that social-emotional development itself is dependent upon the care-giving environment (Schore, 2001). Chambers, Saunders, New, Williams & Stachurska (2010) concluded that an assessment of the relationship between carer and child was crucial in gaining insight into the child’s individual difficulties along with their attachment and quality of relationship with others. We thought that examining all aspects of the child’s development and care experience together would provide an opportunity to understand better how the varying influences are inter-connected and would give clearer indicators for timely intervention.
Rationale for integrated intervention within project
Previous screening studies have found that recommendations from the screening have been put into practice in only a small proportion of cases. Burns et al. (2004) found that only 28% of recommendations for 0–2-year-olds were followed up, despite specific action having been advised after screening. Chambers et al. (2010) reported that only a small number of recommendations made after screening were followed up, with foster carer support being the least likely to be put in place 6 months later.
We therefore integrated an intervention arm into the project so that, when needs were identified, we could provide the follow-up, on a short-term basis at least, from within the project. This has several advantages, namely that the carers and professionals have continuity of contact with the same team; that the interventions can be carefully thought through with the first-hand detailed knowledge of the child’s needs; and that there is minimal delay between recommendations being made and the intervention being put into practice.
Aims
The overall aim of the project was to introduce a screening service that would provide earlier identification of the social and emotional difficulties of CiC aged under 5 years in a 12-month period and to gain a greater understanding of the level and type of needs among this population.
The screening would assess the children’s mental health and social-emotional functioning and provide a profile of their needs for further intervention and long-term planning, be that for adoption planning or returning home to birth parents. By providing timely and effective intervention, we aimed to reduce the impact of these difficulties for the child, and maximise healthy development and positive attachments with key caregivers. We wanted to improve access to CAMHS for children who had more significant mental health and social-emotional difficulties and refer children and families to appropriate community resources where they would be returning home to their birth family.
The project aimed to improve collaboration among professionals across health and social care in a position to positively influence the social and emotional development and mental health of CiC aged under five.
Hereafter the term foster carer will be used to refer to both foster and kinship carers unless specific points about either group are made.
Method
Ethical approval
Ethical clearance for the study was given by the South East London Research Ethics Committee in June 2010.
Sample
Children were recruited in a 12-month period between September 2010 and August 2011. All children who were under 60 months old when they entered care were eligible to take part in the screening (two children were 63 and 65 months by the time the screening questionnaire was administered). We were notified of 77 children in this time period. Children who returned home before an Initial Health Assessment (IHA) with a paediatrician was arranged (n=6) were not included.
Measures
The Greenspan Social and Emotional Growth Chart (SEGC) (Greenspan, 2004) is a brief questionnaire that assesses acquisition of social and emotional milestones in children from birth to 42 months of age. Each item is scored on a five-point scale indicating how often the child shows that behaviour (none, some, half, most, or all of the time). The summed score is translated into a scaled score, which is comparable across age groups. The SEGC was used with children in our sample who were under 3 months of age.
The Ages and Stages Questionnaire: Social and Emotional (ASQ-SE) (Squires, Bricker & Twombly, 2003) assesses the social and emotional behaviour of children aged from 3–65 months. Seven behavioural areas of self-regulation, compliance, communication, adaptive, autonomy, affective functioning, and interaction with people are addressed in separate questionnaires for children at 6, 12, 18, 24, 30, 36, 48, and 60 months of age. The number of questions ranges from 21 at 6 months to 30 at 24–65 months, each taking about 10–15 minutes to complete. The carer is asked to rate how often the child shows a specific response or behaviour to items listed on the questionnaire. The three choices are: ‘Most of the time’, ‘Sometimes’, or ‘Rarely or never’, scoring 10, 5, and 0 points, respectively. The total score is calculated and may then be compared with the standardised clinical cut-off score for each age band. The ASQ-SE was used with children in our sample who were aged between 3 months and 65 months.
The Parent Caregiver Involvement Scale (PCIS) (Farran, Kasari, Comfort & Jay,1986) assesses the caregiver’s behaviour while interacting with the child during a 20-minute observation of free play with the child. The focus is on actions that (a) are appropriate to the child’s emotional needs and developmental level and (b) promote developmental competence. Eleven behaviours are assessed for amount, quality, and appropriateness using a five-point rating scale: physical involvement, verbal involvement, responsiveness, playful interaction, teaching behaviour, control over child’s activities, directives, relationship among activities, positive statements, negative statements or discipline, and goal setting. In addition, an ‘overall observer impression’ score is given, made up of individual scores for: availability, acceptance, atmosphere, enjoyment, and learning environment. In this study we rated behaviours on the following scales: physical involvement, verbal involvement, responsiveness and directives, as well as a rating of overall observer impression.
Informal observations
Each child was observed in the IHA and in the foster carer’s home when possible. In each situation observations were recorded on a proforma under the headings of: social/communication behaviours of child; attachment behaviours; facilitation of child in IHA by carer &/or birth parent. Each of these categories were divided into observations with birth parent and with carer. We also recorded potential stressors for the child, such as the carer leaving the room during the observation. In addition, any behaviour differences in the child between the IHA and home observation were noted; for example, if the child was noticeably more relaxed/ alert/ vocal between settings.
Procedure
The local authority provided a list of children newly received into care each week and who were due to have an IHA with a community paediatrician. Once an IHA was scheduled, an information sheet was sent out to the birth parent, foster carer, child’s social worker and supervising social worker, letting them know that we could be joining the IHA to start the screening process, unless the birth parents exercised their right to opt out of the study.
The carer and/or birth parent was asked to complete the SEGC or ASQ-SE. Questionnaires were administered with foster carers as a semi-structured interview. This gave the opportunity for the carer to expand on specific questions, giving examples of the child’s responses in different situations.
Information about the child’s health and development was discussed with the paediatrician after the IHA. A home visit was arranged after the IHA to complete the PCIS.
The information from the IHA, screening questionnaires, observations, developmental and health information from the paediatricians, and background information were integrated into a summary compiled by a CAMHS Clinical Specialist, which included a formulation and recommendations for the child’s social and emotional development. The summary was distributed to the child’s social worker, foster carer, paediatrician and independent reviewing officer (IRO), if possible in time for the next Looked-after Child Review meeting (LAC Review), in order that the information could be incorporated in the consideration and discussion of the child’s needs. (LAC reviews take place at 1 and 4 months following a child entering care, thereafter every 6 months, and are key decision-making forums focussing on the specific needs and well-being of the child.)
Where we considered that an intervention or advice to the foster carer or network was indicated from the screening findings for a child or their carer, we had a follow-up discussion with the child’s social worker, the fostering social worker and foster carer for the child to agree an intervention plan.
The intervention package typically included one or more of the following: liaison with professionals; network meeting including foster carer to discuss screening assessment; advice on social-emotional needs of child to foster carer; direct guidance and support to foster carer; advice to network professionals; and direct carer–child work.
The guiding principles underpinning all interventions were twofold: that the individual child’s social-emotional needs along with the quality of carer–child interaction would be the primary focus for informing the intensity and type of the intervention; and that the caregiver–child relationship is the main agent for change and that all interventions would focus on maximising this relationship in order to best meet the child’s needs.
We hoped the intervention would provide more in-depth information to the network of professionals, especially the child’s social worker, of the nature of the child’s needs and developmental change over time in order to help inform care planning.
After each screening a feedback questionnaire was sent to the child’s social worker, foster carer, paediatrician and IRO asking for their feedback on the screening summary and, in the case of the foster carers, their experience of the screening process. In the cases where an intervention was recommended and agreed, we sent out the feedback questionnaire following the end of the intervention period. Non-responders were contacted by phone after 2 weeks and respondents given the option to complete the questionnaire over the telephone or return it electronically.
After 6 months, children who remained in care received a review health assessment (RHA) by the paediatrician. Where possible a repeat of the initial screening was completed at the RHA, including observation of the child during the assessment and completion of the ASQ-SE with the foster carer.
Data analyses
A Pearson’s correlation was used to examine the relationship between child age and PCIS scores, and analysis of variance with Bonferroni post hoc comparisons were used to test for differences between child gender and child age groups in PCIS scores. t-tests were used to compare PCIS scores of boys and girls and of children who were and were not recommended an intervention. Chi-square tests were used to test for associations between age and likelihood of referral and between year of referral and the identification of difficulties.
Results
Sample
In total, 67 children aged under five came into care by the local authority between September 2010 and August 2011, and remained CiC long enough to have an IHA; 63 (94%) of the eligible population were screened. The other four (6%) children were not included as their birth parents opted out of the project.
Of the 63 children screened, 37 were boys and 26 were girls; age at screening ranged from 6 weeks to 65 months (mean 19.6; SD 19.43). At screening questionnaire completion, the time the child had been with their carer ranged from 2 weeks to 21 weeks, with the mean time being 8.13 weeks. In 43% of cases, the screening questionnaire was completed within 6 weeks of the child becoming looked after. Figure 1 shows the age of children when the screening questionnaire was completed.
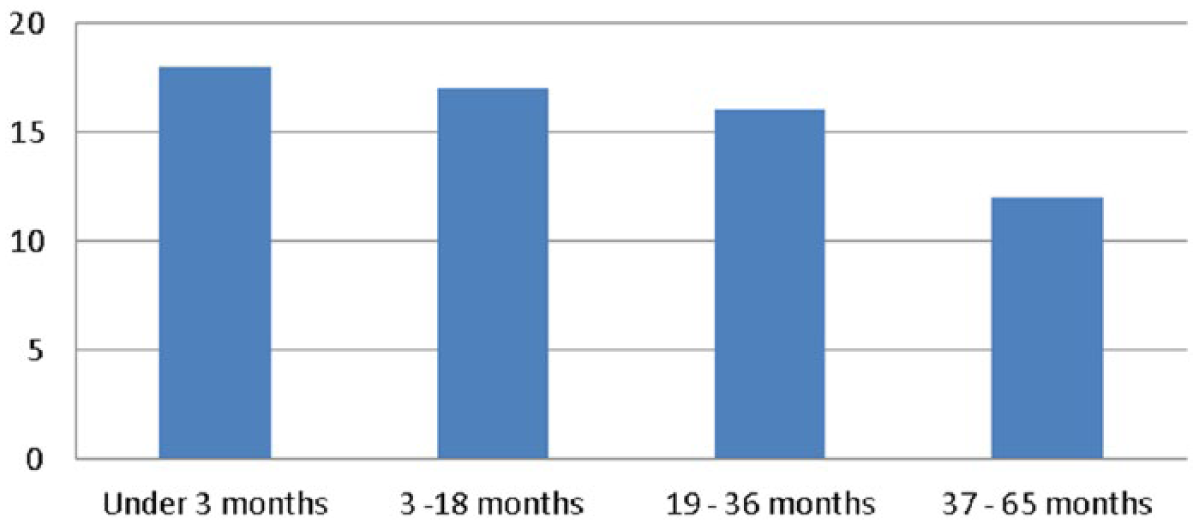
Age of children when questionnaire completed.
The placement status of the children included: 70% with Social Services foster carers; 14% in kinship placements; 10% in mother/baby assessment centres; 3% with independent agency foster carers; and 3% in mother/baby foster placements. Two-thirds of the sample was from Black and Minority Ethnic groups and one-third were White British.
Level and type of social-emotional difficulties in the screened population
Social Emotional Growth Chart
The Social Emotional Growth Chart (SEGC) was completed by 19 carers of babies under the age of 3 months and 11 birth parents. In this <3 month age band we had the highest level of parent participation, as parents were more likely to attend the IHA when the babies were very young.
According to foster or kinship carer’s ratings, five children (25%) were on the 25th percentile or below, nine children (50%) were between the 25–75th percentile and five children were on the 75th (25%) percentile or above.
Parents’ ratings resulted in one child being on the 25th percentile, five children on the 37th percentile, two children on the 50th percentile and three on the 99th percentile. For the seven children where the SEGC was filled in by both parent and carer, in two cases mother and carer (maternal grandmother) scored the same, in four cases the parent(s) scored the child lower than the carer, and only one parent scored their child higher than the child’s foster carer.
Ages and Stages Questionnaire: Social and Emotional
The ASQ-SE was completed by 44 carers. Of these, three children had profound developmental disorders and were excluded from the analysis. A further child was excluded because her score was more than 3 standard deviations above the mean. Of the remaining 40 children 11 (28%) scored above the clinical cut-off point, with a further five children (13%) within 10 points of this value.
Children in the 19–36 month age group had greater difficulties than both younger (3–18 months) and older (37–65 months) children, based on the ASQ-SE scores alone and boys were rated as having more difficulties than girls and were more affected by increasing age.
To examine the type of difficulties identified from the ASQ-SE, the specific questions where children scored 5 (some difficulty) or 10 (significant difficulty) points were examined. The most prevalent difficulties shown by children whose score was approaching or above the ASQ-SE recommended cut-off score included: being too friendly with strangers (69%); not doing what is asked of them (80%); showing no concern for others’ feelings (75%); not using any words for feelings (67%); not indicating their needs at all to carer (59%), and eating problems (59%).
Many of the children who scored below the recommended cut-off, suggesting no concern in their overall social-emotional development, had some concerning behaviours highlighted through the questionnaire and discussion with the foster carer. For example, 33% of the children did not use words for feelings, 33% did not indicate any needs to their carer, 33% showed no concern for others feelings, 38% had no awareness of danger and 38% were unable to stay awake for an hour at any one time in the day/night. The overriding impression given by the foster carers was that these babies and children were very easy to care for, yet some carers appeared to feel intuitively concerned and questioned the significance of behaviours such as those mentioned above.
Parent Caregiver Involvement Scale (PCIS) and observations of Carer–Child relationship
Home visits were made with 56 children and their carers and the PCIS was completed with 54 children and carers. It was not possible to complete the PCIS for six children who were placed in mother and baby assessment centres, two newborn babies who were sleeping at the home visit and a further child who had severe developmental disabilities. The two children excluded from previous analysis owing to developmental disability have been excluded for continuity, giving a total of 52 PCIS results.
There were no significant differences between boys and girls for any of the PCIS scores. Correlations between child age and PCIS scores indicated that carers used more directives (r=0.49, p<001) and showed less physical involvement (r=0.55, p<001) acceptance (r=0.32, p=0.023) and enjoyment (r=0.28, p=0.049) with older children.
ANOVA showed that physical involvement mean scores decreased (F (3, 48)=5.489, p=0.003) and directives mean scores increased (F (3, 48)=12.370, p<0.001) across age bands. Correlations between scores indicated that the higher the directives score the lower the score on quality (r=−0.337, p=0.027) and appropriateness (r=−0.307, p=0.045) of directives.
Level of interventions needed from overall assessment of child’s needs
As described earlier, decisions around the need for interventions were based on the clinical analysis of all the information collected for the child, rather than solely on the results of the ASQ-SE or SEGC questionnaires. The observations of the child’s interaction with their foster carer, using both standardised PCIS measures and informal observations, as well as the carer’s qualitative descriptions of the child’s responses, gave important insights into how the child responded to the care available to them as well as the kind of specific responses the child evoked in the foster carer. Common examples of this were when the child hurt themselves, was tired or distressed and the foster carer responded by believing that the child was not in need of or did not want their care. Other concerns related to observations of low levels of vocalisations and reciprocity between babies and carers in cases where developmental delay was present. This resulted in a number of children being identified as having needs requiring input in the clinical formulation who had not scored highly on the questionnaires.
For the following analysis all children are included, including those with developmental disorders.
From the 63 children who completed the screening, a meeting and /or direct work was recommended for 40 children, with a further two cases being recommended a specific advice sheet, resulting in 67% of the screened group receiving a recommendation for an intervention. For a further two children it was recommended that they were re-screened before the 6-month review date.
Older children were more likely to be recommended an intervention (χ2(3, 63)=24.95, p<0.001).
The relationship between the PCIS and recommendations/referrals
We had set out to explore the quality of the carer–child relationship alongside any specific child difficulties in order to inform the focus for the intervention. These findings indicate some of the ways in which relationships between foster carers and children were affected.
Children who were recommended an intervention scored significantly lower on physical involvement (t(3,48)=3.06, p=0.004) and overall observer impression scores (t(3,48)=2.053, p=0.046) on the PCIS than those not recommended an intervention.
In the youngest age group, those recommended an intervention scored significantly lower on the overall observer impression score (t(1,8)=5.6, p<0.001) and on the verbal score (t(1,8)=4.48, p=0.002). No other significant differences were found, although the numbers in the ‘no intervention’ group are small.
Those that went on to be recommended a referral to CAMHS scored significantly lower on physical involvement (t(1,52)=-2.0, p=0.047) and lower on overall observer impression score (t(1,52)=-2.69, p=0.01.
The children who were recommended a referral to CAMHS were also compared with those who were recommended an intervention within the project but no further involvement after the project intervention: they scored significantly lower on enjoyment on the PCIS (t(1,34)=-3.18, p=0.003)
Uptake of project interventions
Overall 73% of the children and carers that were recommended an intervention went on to take this up. For a further two newborn babies it was recommended that they were re-screened early.
The reasons for interventions not being taken up were: three children returned home immediately after the screening; another eight children were recommended an intervention but there was minimal contact from the social worker to discuss the child’s needs; in only one of these eight cases the social worker/IRO expressed the view that the intervention was unnecessary. In five cases of the remaining seven children, the CiC CAMHS has since been approached to discuss concerns about the child or to make a referral.
Children referred to CAMHS
Of the 63 children in the project, two children were referred to CiC CAMHS at the time the screening was taking place (these were both older children, aged 5 years and 4 years 3 months) and 14 were referred to CAMHS on advice from the project team as ongoing mental health needs were identified. We recommended that a further three children were referred to CAMHS but this had not taken place by the end of the project. This total of 19 children is 30% of the screened population.
Information from feedback audit
Feedback questionnaires were sent to all social workers, IROs, foster carers and kinship carers. We asked specific questions regarding their experiences of the different stages of the screening process including the intervention, and how useful the screening summary was in adding to their understanding of the child. We also asked professionals to rate how much the screening contributed to care planning.
Mean feedback scores can be seen in Table 1.
Mean feedback scores 1 from independent reviewing officers, social workers and foster carers.
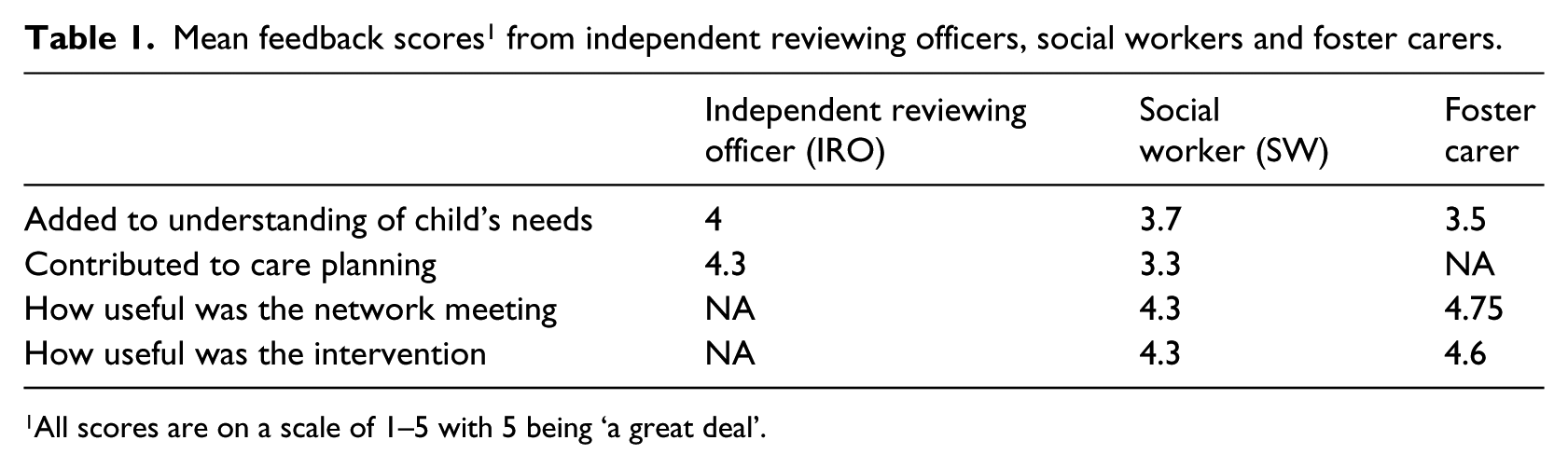
All scores are on a scale of 1–5 with 5 being ‘a great deal’.
Comparison between screening and routine paediatric assessment in the identification of difficulties
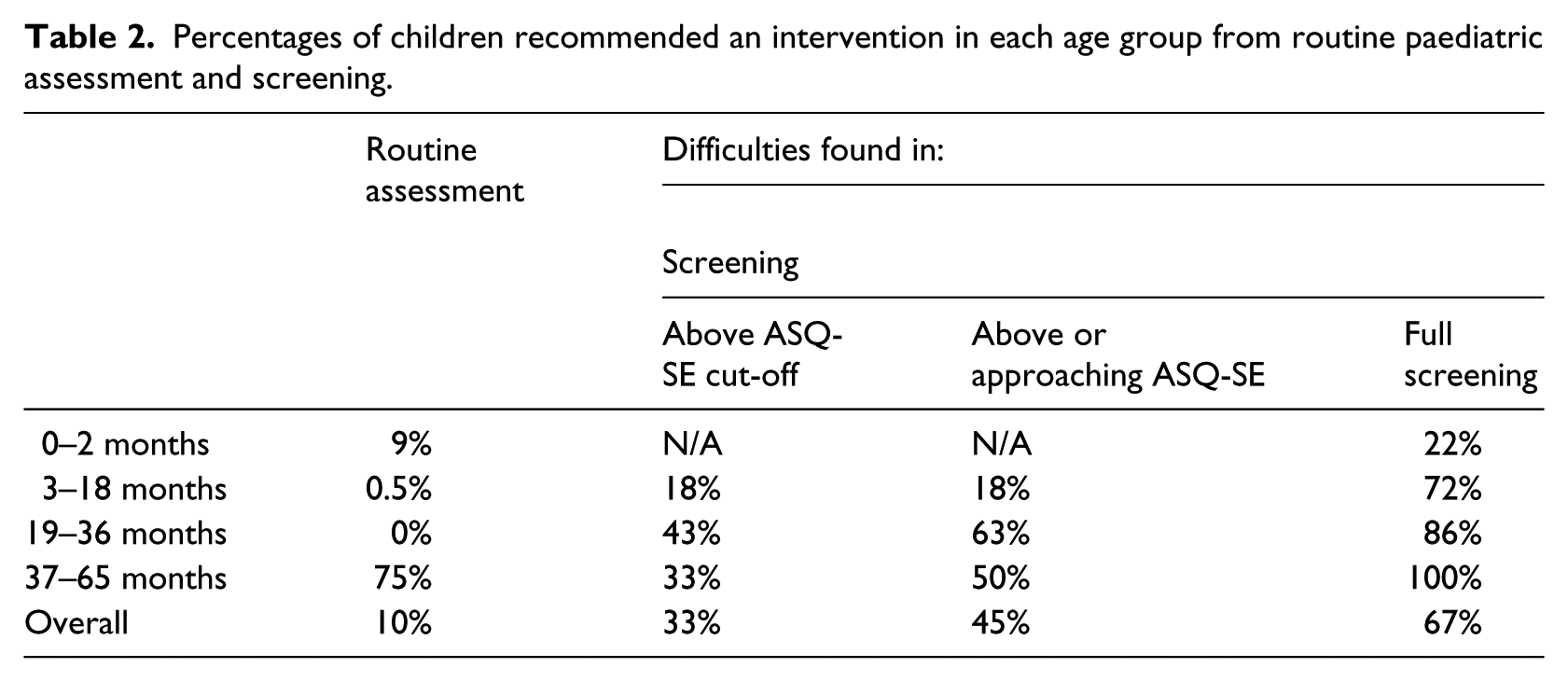
Paediatrician records were used to assess how many social-emotional difficulties and concerns had been identified at routine health assessments in under-fives CiC in the previous year. A concern was considered to have been identified when the paediatrician recorded an action point relating to an emotional or behavioural concern. In the 12 months before the screening began paediatricians identified concerns in six out of the 61 children seen (Table 2). In the study period a significantly greater proportion of children were identified who were above or approaching the ASQ-SE clinical cut-off point (χ2(1, N=63)=8.451, p=0.003) or who were identified as having difficulties after the complete screening (χ2(1, N=124)=38.23, p<0.001).
Percentages of children recommended an intervention in each age group from routine paediatric assessment and screening.
Discussion
Early identification of social and emotional difficulties
This project set out to investigate the hypothesis that there was a significant degree of unidentified and unmet need in relation to both the social-emotional well-being and mental health of very young CiC, aged 0–4 years. Our findings confirm our hypothesis that the proportion of babies and children identified with significant levels of social-emotional concerns was higher than the proportion of children identified through the routine paediatric assessment carried out previously (67% in this screening study compared with 10% in the year before). In addition, we found that the full screening procedure identified a greater degree of difficulty than using the ASQ-SE screening questionnaires alone (67% compared with 33%), strongly suggesting the need to combine CAMHS clinical assessment expertise and standardised measures to identify and formulate the social-emotional and mental health needs of the 0–4 CiC population.
Type and levels of social-emotional difficulties identified
The type and level of children’s difficulties that we identified from the screening procedure were varied. The evaluation provided some insights into the nature and context of the most common problems the children experienced.
A considerable number of babies were aged 6 weeks or under when they came into care. We did not find the brief SEGC provided sufficiently detailed information to contribute appreciably to our understanding of the infant’s social-emotional functioning. This, along with a number of babies being described at least initially, as ‘easy to care for’, may have affected the overall level of needs identified in this screening cohort. The SEGC did give a snapshot of the carer’s (birth parent or foster carer) view of the child. It was also useful in flagging up differences in the foster carer and birth parent’s view of the baby.
The full screening procedure included the clinical analysis of all the information collected for the child, rather than the ASQ-SE or SEGC questionnaire scores alone, and this informed the decisions about the need for interventions. Children in the older age group (37–65 months) were assessed as having the highest level of difficulty from the full screening and were recommended interventions in 100% of cases, in comparison with 86% of children in the 19–36 months group and 72% in the 3–18 months group. However, the carers rated children in the 19–36 month age group as having the greatest difficulty from the ASQ-SE alone, suggesting that they found the behaviours of this age group more challenging.
The clinical formulation was significantly informed by the PCIS findings and clinical observations of the interaction and relationship between caregiver and child. The PCIS findings revealed correlations between the age of the child and certain scores: that the older the child the lower the physical involvement score and the higher the directives score. When the directives scores were examined in terms of their sub-scores for quality and appropriateness, it was found that the higher the directive score, the lower the quality and appropriateness of the directives. This suggests that when the relationship between carer and child may become didactic, with many directives being given to the child, there is a negative impact on the quality of the interaction. In addition, the older the child the lower the carer scored on the acceptance and enjoyment sub-scores of the overall observer impression score.
Although it is understandable that babies will receive more physical care and contact than 4–5-year-olds, it is apparent that the level of physical involvement between carers and young children can be quite low. An explanation for this could be that many young toddlers and 3–5-year-olds presented with behaviours that did not convey their needs or distress directly to the carer and therefore did not elicit nurturing responses. In addition, some children would communicate distress or frustration but then reject their carers’ attempts to help or comfort them. Carers tended to feel that they should wait for the child to signal readiness for closer contact, but as avoidant responses were so clearly ingrained in many children, it was observed how a pattern of distant relating between carer and child could become an established norm.
There are many challenges to the development of the relationship between carer and foster child. With acceptance and enjoyment scores also showing a significant decline as the child’s age increased, carers needed support to acknowledge difficulties in developing a close emotional relationship at times. Conflict may arise between the carers and agencies’ expectations of the carers’ competency, skills and role, on the one hand, with the emotional impact of the child’s demands, or absence of demands, on the other. We thought that this played a role in many cases where the children’s difficulties were minimised by the carers in their response to the initial screening questionnaire but came to light in subsequent conversations or direct observations.
The specific child behaviour difficulties that were most prevalent across the age bands in children both above and below the ASQ-SE cut-off were: highly indiscriminate behaviour towards adult strangers, inability to express even basic needs to their carers or to seek comfort from them when hurt /distressed, difficulty with peer relationships and eating difficulties.
Combining screening with intervention provision
Findings from other screening studies that recommendations for interventions following screening were not expedited is unsurprising to the authors in some respects, as we have become more aware of the enormous pressures on carers and professionals alike in meeting the wide range of demands of high-level contact schedules, and tasks from procedural, training and legal processes. The engagement of the carers and professionals in creating a thinking space for the emotional/mental health needs of the children starts within the screening process, and providing continuity of workers into the intervention stage helped to maintain engagement of carers and their uptake of the intervention offered. The integrated screening and intervention approach resulted in 73% of children recommended an intervention actually receiving help following the screening.
The interventions offered were individually tailored to the context for each child and carer, but whether advice-based or involving direct work they all specifically targeted the caregiver–child relationship as the main agent for change. It was important to translate the screening information into both practical action as well as a deeper emotional understanding of the child’s needs and presentation.
Introduction of a new service and interdisciplinary collaboration in a multi-agency setting
Introducing a new service and way of thinking into a multi-agency setting requires both confidence and a willingness to try new working practices from both senior management and professional practitioners. In this London borough there was positive support and inter-agency cooperation from within CAMHS, Social Care and Child Health, which made it possible to introduce the project in the first instance and is likely to have influenced the high rates of participation. Overall, the screening was accepted by the majority of birth parents, with only four out of 67 birth parents opting out of the screening, a 94% uptake rate of the initial screening stage.
At each stage of the screening and intervention process there was close and growing communication, collaboration and joint working between professionals in the project and the partner agencies. There was overall a very positive response to the screening reports in terms of their usefulness in adding to the understanding of the child’s needs and in how much they impacted on care planning. The highest degree of satisfaction came from foster carers and social workers in their view of the usefulness of the intervention. Awareness that the focus of the screening is not only on the child but also on the carer does create challenges in finding a balanced but sufficiently thorough shared formulation to inform the child’s network.
Access to CAMHS
Lastly, we wanted to investigate whether the project would increase access to CAMHS for under 5-year-old CiC. Within the screened group 16 children were referred to either the CiC CAMHS team or other local community CAMHS. In addition, there were many more referrals to our CiC CAMHS during the project from social workers, IROs and paediatricians for under-fives who had already been in care some time and so were ineligible for screening. This resulted in 24 children in total being referred to CiC CAMHS during a 12-month period in the project, a significant increase in referral rate compared with the previous year when only eight under-fives had been referred. In addition, four further referrals of children seen in the project were made to CiC CAMHS soon after completion of the project.
Limitations
The main limitations of the project were the short-term nature of both the interventions that could be offered and the short timeframe in which we could follow up the children for reviews, which led to less than half being seen at 6 month review. The short timeframe for data collection limited the size of the sample obtained and thus the extent to which the data could be interrogated.
It was clear that some children had very established difficulties and patterns of behaviour requiring a longer period of treatment for them and their foster carers to make changes. The evidence-based treatments for high-risk CiC in this age group, for example Attachment and Biobehavioural Catch-up (Bick & Dozier, 2013), have treatment packages that deliver at least 10 sessions, with the recognition that attachment behaviours can take time to change, especially if the child continues to live with uncertainty and the stress this inevitably brings.
A future study has been developed to trial screening babies from 3 months and over, to implement a longer intervention with reviews at 6 and 12 months to explore outcomes over time. This new study will start in early 2014.
Conclusion
This project tested the feasibility of screening babies and very young CiC with a comprehensive but accessible social-emotional screening on first entering care, and found a significant degree of previously unrecognised and unmet need. A short-term intervention was well received and a need for development of further specific CAMHS input and review over a longer period is indicated for some of this vulnerable group of children to help them make meaningful and healthy attachments and relationships to others.
Footnotes
Acknowledgements
The authors wish to thank Chris Saunders (Southwark Children’s Social Care), John Simmonds (British Association of Fostering & Adoption), and Dr Danya Glaser (Great Ormond Street Hospital) for their support of this study.
Funding
This work was supported by Guy’s and St Thomas’ Charity (G091012).