
Abstract
This prospective longitudinal study compared the psychological development and patterns of attachment of 20 prematurely born children and 20 full-term children at 7 years of age. The School-age Assessment of Attachment (SAA) was used, and hypotheses and interpretation of the findings were drawn from the Dynamic-Maturational Model of Attachment and Adaptation (DMM). Significant differences between prematurely born and full-term children were found: 10% versus 0% at “high” risk, 55% versus 25% at “moderate” risk, and 35% versus 75% at “low” risk. There were no differences in the percentage of psychological trauma between samples, but there was a difference in the types of experiences leading to trauma. For prematurely born children, it was most often illness, whereas for full-term children, it was family problems. We discuss the implications for clinicians.
Introduction
Improvements in antenatal care and technological innovations in neonatal medicine have resulted in increased survival of low birth weight infants, especially very low birth weight (VLBW < 1500 g) and extremely low birth weight (ELBW < 1000 g). The psychological development and quality of life of these children and their families have been less extensively reviewed despite increasing importance. Our pilot study explored the psychological development, especially in terms of attachment strategies, of school-aged prematurely born children as compared to full-term children according to a functional analysis utilizing the School-age Assessment of Attachment (SAA, Crittenden, 2007; Crittenden & Kulbotton, 2007) to identify both the attachment strategies utilized by this population (strategies that can also be seen as an indicator of risk for maladaptation) and the presence of psychological trauma and modifiers of attachment strategies.
Attachment development in prematurely born children
Early parent–child interaction has been identified as an important factor in all infants’ development (Forcada-Guex, Pierrehumbert, Borghini, Moessinger, & Muller-Nix, 2006; Treyvaud et al., 2010). In several studies, mothers of premature infants have been described as less sensitive and more unresponsive and intrusive when interacting with their infants (Cassibba, Van IJzendoorn, & Coppola, 2012; Forcada-Guex et al., 2006; Muller-Nix et al., 2004). Additionally, fathers of premature born infants are described as less sensitive when compared with fathers of full-term born infants (Baldoni, Facondini, Landini, & Romeo, 2008; Baldoni et al., 2009). The infants themselves have been described as more passive, with less positive affect and less facial expression than full-term infants (Bozzette, 2007; Udry-Jørgensen et al., 2011). This would suggest a basis for the development of insecure attachment, but other studies have reported similar proportions of securely and insecurely attached premature and full-term infants (Cox, Hopkins, & Hans, 2000; Frodi & Thompson, 1985).
Similar attachment discrepancies persist into the preschool years, and have been fairly studied (Breslau, Chilcoat, Johnson, Andreski, & Lucia, 2000; Minde, 2000). At school age, studies have mainly focused on cognitive development and educational outcomes, highlighting an increased risk for reduced cognitive test scores and learning and language disabilities (Bhutta, Cleves, Casey, Cradock, & Anand, 2002; Grunau, Whitfield, & Davis, 2002; Msall & Tremont, 2002; Tideman, 2000). However, there are limited studies dedicated to attachment strategies (Tideman, Nilsson, Smith, & Stjernqvist, 2002), and no studies available regarding the dynamic maturation model of attachment and adaptation in prematurely born children at school age.
Increased risk of psychological distress and maladaptation
Recent reports on school-aged prematurely born children noted increased risk of depression, anxiety, feeding difficulties, behavioral and conduct disorders, and serious neurodevelopmental conditions (such as autism spectrum disorders, attention deficit and hyperactivity disorders, and learning disabilities) among prematurely born children, particularly low birth weight children, as compared with full-term children or children with normal birth weight (Aarnoudse-Moens, Weisglas-Kuperus, Van Goudoever, & Oosterlaan, 2009; Bhutta et al., 2002; Cerro, Zeunert, Simmer, & Daniels, 2002; Hack et al., 2009; Indredavik et al., 2010; Johnson & Marlow, 2011; Linnet et al., 2006; Lund et al., 2012; Potijk, De Winter, Bos, Kerstjens, & Reijneveld, 2012).
However, many of these findings were based on parental reporting (Singh, Kenney, Ghandour, Kogan, & Lu, 2013), criticized for the often substantial discrepancies between the different sources (parents vs teacher: Rescorla et al., 2014; parents vs adolescents: Rescorla et al., 2013; or standardized diagnostic interviews and clinical evaluations: Rettew et al., 2009)
Premature birth and post-traumatic symptoms
Premature births often involve painful and threatening events, often researched in terms of parental experience only, for example, the sudden interruption of a pregnancy, the early and sudden parental–child separation, long hospitalization, and the risk of death or disability. Intense feelings of anxiety and depression have been observed in the parents of prematurely born children. Most studies reveal parental stress in terms of post-traumatic stress disorder, especially in mothers of premature babies (Holditch-Davis, Bartlett, Blickman, & Miles, 2003), with long-term effects (Kersting et al., 2004; Muller-Nix et al., 2004; Pierrehumbert, Nicole, Muller-Nix, Forcada-Guex, & Ansermet, 2003; Stramrood et al., 2011). Additionally, recent studies highlighted high levels of salivary cortisol in both mothers and prematurely born children (Habersaat et al., 2014a, 2014b) and a correlation between post-traumatic stress disorder mothers’ symptoms and children cortisol levels (Habersaat et al., 2014a, 2014b). It would be interesting to investigate child’s psychological trauma associated with premature birth, from his perspective.
Dynamic-Maturational Model of Attachment and Adaptation
The Dynamic-Maturational Model of Attachment and Adaptation (DMM, Crittenden, 1995, 2000a, 2000b, 2008a, 2008b, 2015) conceptualizes patterns of attachment as adaptive strategies that infants, children, and adults utilize to cope with everyday challenges. The DMM conceptualizes danger, rather than safety, as the focus in the organization of attachment behavior. Thus, rather than describing distressed and troubled children as “disorganized,” the DMM interprets their behavior according to a set of organized self-protective strategies that function to maximize protection in threatening or dangerous conditions. This adaptation of behavior is a dynamic fit of strategy to the context, and the chosen strategies are learned from parental contingencies and contextual dangers (Crittenden, 2008). The learning process for these strategies results from both temporal information (termed “cognition”) and the intensity of stimulation (or “affect”), and these are processed in the brain. That is, information processing yields dispositional representations, which yields organized self-protective behavioral strategies.
The DMM model offers a large range of possible outcomes, including both the Ainsworth infant strategies outcomes (A1–2, B1–5, C1–2) and DMM categories (compulsive A+, coercive C+, and A/C with all the possible single grades in combination).
According to the DMM model, children using a Type A strategy rely more on “cognitive” information (based on temporal contingencies) to organize their behavior, whereas children with a Type C strategy depend more on “affective” information (based on intensity of stimulation). Type B reflects balanced integration and Type A/C alternation.
Children using compulsive A3–4 (A+) strategies mask negative affect (anger, fear, and desire for comfort) with the demonstration of false positive affect. Children using coercive C3–6 (C+) strategies employ false cognition in the form of self-deception and deception of others. These strategies have been associated with overprotective and unpredictable parenting. The extreme coercive C+ strategies were associated with parental warnings about invisible or unlikely dangers. C+ strategies are thought to be associated with particular difficulties: victimization, incompetence, peer rejection, academic underachievement, and psychosomatic illnesses (C4 “feigned helpless” and C6 “seductive strategies”) or with attention-seeking and acting out disorders, such as hyperactivity, attention problems, conduct and anxiety disorders (C3 “aggressive” and C5 “punitive strategies”) (Crittenden, 2000 a, 2000b, 2008a, 2008b, 2015; Crittenden, Dallos, Landini, & Kozlowska, 2014; Crittenden, Kozlowska, & Landini, 2010).
An individual child’s attachment strategy can be selectively modified by unresolved psychological trauma, rendering a behavioral strategy dysfunctional when a threat is associated with aspects of specific previous danger, or unselectively modified by modifiers, such as depression or somatic state expression, which convert an attachment strategy into a nonstrategy (Crittenden, 2007, 2008, 2015).
The DMM has a validated assessment for attachment strategies and psychological traumas (Farnfield, Hautamäki, Nørbech, & Sahhar, 2010; Kozlowska & Elliott, 2014). The SAA (Crittenden, 2007a; Crittenden & Kulbotton, 2007) is a functional analysis suitable for 7- to 8-year-old school-age children analyzing the morphology of speech of the child instead of relying on parental reporting. The assessment identifies attachment strategies, provides information about the child’s memory system/information processing, and explores traumatic experiences and the clinical implications of the attachment strategies. The strategies are classified into groups based on the theoretically expected psychological risk (see Crittenden, Kozlowska, & Landini, 2010): “low risk” (B, A1–2, C1–2), “moderate risk” (A3–4, C3–4) and “high risk” (pre A5–6, C5–6, A/C).
Our research was designed to investigate attachment strategies among prematurely born children compared with a control group of full-term born children, at 7–8 years old, specifically investigating the strategies most at risk of maladaptation (A+ and C+). Additionally, the research investigated evidence of psychological trauma or modifiers of the strategies among the groups.
Hypotheses
We hypothesized that compared to full-term school-aged children, prematurely born children would have
Higher rates of A3–4 and C3–6 attachment strategies and lower rates of A1–2, B, and C1–2 attachment strategies;
Increased risk of psychological distress and maladaptation;
Higher rates of psychological trauma or loss related to illness or perinatal experience;
Higher rates of modifiers of attachment strategies, in particular depression and expression of somatic state;
Correlation between their psychopathological risk and their severity of perinatal problems;
Correlations between psychopathological risk and hospitalization days in the neonatal unit.
Method
This pilot study was approved by the Ethics Committee of Reggio Emilia Arcispedale Santa Maria Nuova (ASMN), and informed parental consent to participate in the study was obtained by all parents.
Participants
Inclusion criteria included premature birth, defined as either ⩽32 weeks of gestation and <1500-g birth weight, or birth at full term (⩾38 weeks of gestation). Exclusion criteria included restricted native language skills, and a range of complex medical conditions (infant cerebral palsy, infant malformations, chromosomal abnormalities, fetopathy, intraventricular hemorrhage > grade II, periventricular leukomalacia–cystic ⩾ 2, retinopathy of prematurity ⩾ III, neonatal withdrawal syndrome).
For the prematurely born children sample, all 62 prematurely born children, born between 2006 and 2007 at this institution, were considered for the study. All families were approached by telephone. Of the 62 children, 24 were untraceable, 12 refused to participate in the study, and 6 were excluded according to the exclusion criteria.
The control group was composed of 20 full-term children, randomly selected for the current study from a larger undergoing study, characterized by the voluntary involvement of three school classes from the same geographical area as this institution. A total of 60 parents were invited to participate through an informative note, written by the school headmistress.
Assessments
The Perinatal Risk Inventory (PERI) (Scheiner & Sexton, 1991) was used to describe the severity of perinatal problems for the prematurely born group. It is an 18-item inventory based on several perinatal factors such as Apgar index, gestational age, weight, head growth, electroencephalography (EEG), ultrasound, and ventilation. Each item is scored 0–3 on an ordinal scale; the higher the score, the higher the risk of later problems. The total score of the PERI demonstrated a significant correlation with the infants’ last score on the Bayley and Stanford–Binet (Scheiner & Sexton, 1991). A clinical cutoff point (⩾5) was used (Pierrehumbert et al., 2003) to separate low-risk, few medical complications, and high-risk newborn infants, associated with negative developmental outcomes. Studies have highlighted these outcomes specifically for those with PERI of ⩾10 at 9 and 18 months (Scheiner & Sexton, 1991; Zaramella et al., 2008). In fact, using a score of 10 on the PERI, Scheiner and Sexton (1991) provided a sensitivity of .76, specificity of .79, positive predictive value of .475, and negative predictive value of .929 in identifying infants who were developmentally disabled.
The SAA (Crittenden, 2007; Crittenden & Kulbotton, 2007) was selected as the analysis methodology because it is designed to identify school-age attachment strategies and provide information about the child’s memory system and information processing, both through direct verbal speech and through the relationship with the interviewer. It is important to note that it assesses implicit memory systems (somatic, procedural, imaged), as well as explicit memory systems (body-talk, semantic, connotative language), and reflective integration (episodic memory and reflective integration adapted to concrete thinking of school-age children). The SAA analysis emphasizes information processing through children’s discourse, particularly dysfluence. This permits coders to access information not subject to the child’s conscious control. The SAA’s concurrent clinical validity has been previously demonstrated (Crittenden, Kozlowska, & Landini, 2010; Kwako, Noll, Putnam, & Trickett, 2010).
The children were shown a series of seven picture cards depicting commonly exposed school-age threats such as going out alone, rejection from peers, moving house, bullying, or the mother transported to hospital. The children were asked first to tell an imagined story about the card’s theme, and then a real episode about their own experience. Afterwards, specific questions were asked inquiring cognition, affect, theory of mind, and reflective integration. The procedure ended with a request for the child to imagine a happy time with his or her family.
The transcripts were coded, using the SAA manual (Crittenden, 2007), by a reliable SAA coder (“level 1” of coder reliability with a concordance of ⩾.80, suitable for all applications, both clinical and research one) who was blind to information on both the study and the children (apart from what was mentioned in the assessment itself). The coder assigned each SAA protocol to one of 13 DMM classifications and, when indicated, also assigned lack of resolution of trauma/loss or modifiers. In this study, psychological traumas were also classified in relation to danger experiences, as family events (including parental separation), illness (including the condition of the prematurity itself), or other. When children described their premature birth as their own experience, a trauma was assigned, and when children spoke semantically about their birth but explained that they could not remember the experience, a trauma was not assigned.
For the purpose of exploring clinical implications of the attachment strategies, groups based on the theoretically expected psychological risk for maladaptation were created (see Crittenden, Kozlowska, & Landini, 2010), as low- (B, A1–2, C1–2), moderate- (A3–4, C3–4), and high- (pre A5–6, C5–6, A/C) risk.
Data collection
Demographic and clinical data were collected for the prematurely born children group from the patient files. Demographic and medical clinical status data of the control group were obtained directly by the school from a dedicated form compiled by the parents. Family demographic information was also collected. The SAA was administered to each child during an individual 1-hour interview, audio recorded, and subsequently transcribed.
Study design
The study is a prospective comparison between premature- and full-term born children. The comparison between variables in two independent samples was performed using chi-square test and represented through Cramer’s V. In cases of very small cell sizes, Fischer’s exact method was used.
Results
Of the 20 prematurely born children enrolled, 11 were male with an average age of 7.3 years, of age and gestational age of 30 weeks (range: 27–32), and mean birth weight of 1294 g (range: 749–1500). The mean PERI score was 6.9 (range: 2–23), and the neonatal unit hospitalization days mean was 54.6 days (range: 25–98). The control group included 9 males, mean age of 7.2 years. All the children spoke Italian and did not have the medical conditions listed above.
Distribution of the attachment strategies
The Type C attachment strategy was predominant in the entire sample of 40 children: 23% were classified as C1–2 and 30% as C3–4. Type A strategy was observed in 20% (12.5% A1–2 and 7.5% A3–4), Type B in 15%, and the combined A/C strategies in 12.5%.
Hypothesis 1. Higher rates of A3–4 and C3–6 attachment strategies and lower rates of A1–2, B, and C1–2 attachment strategies in prematurely born children.
The 6-way (A3–4, A1–2, B, C1–2, C3–6, and A/C) distributions illustrated a trend toward this hypothesis, but statistical significance was not reached (χ2(3) = 5.7, p = .1). The coercive Type C strategy was used most frequently by both groups (35% full-term and 70% prematurely born), but in the full-term group, the strategies were more normally distributed (see Table 1).
Distribution of the SAA subclassifications (strategies) by referral group.
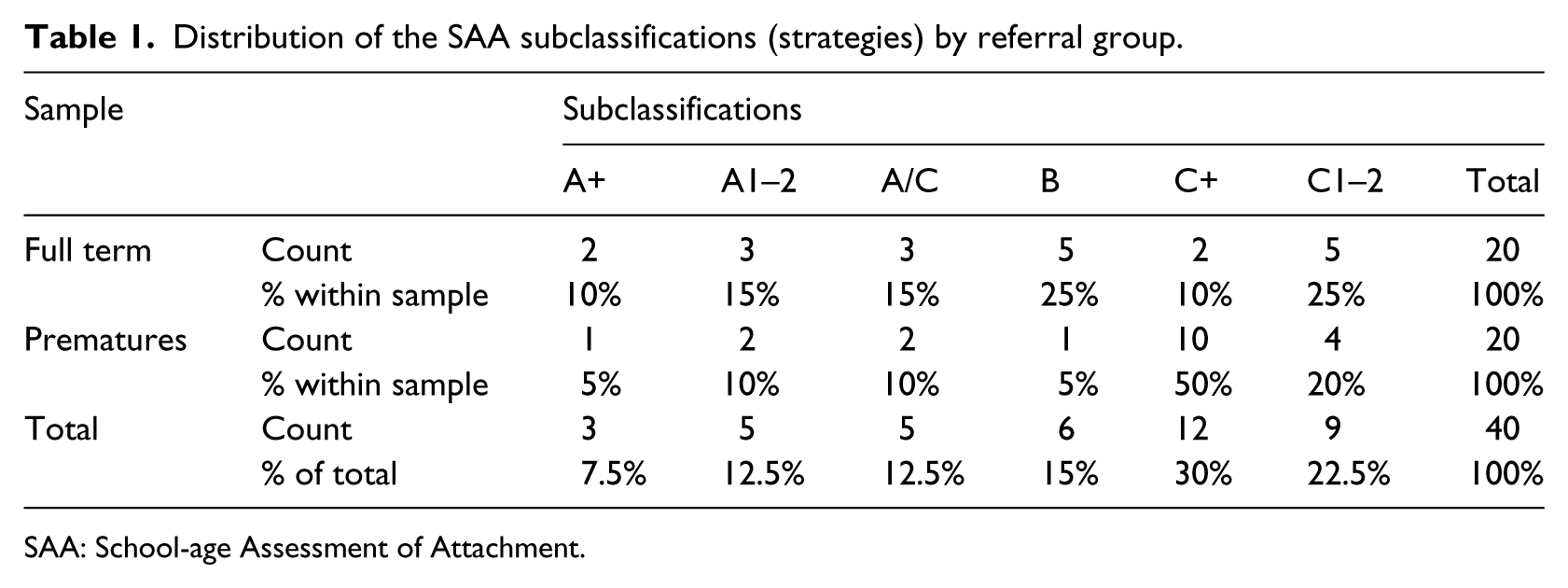
SAA: School-age Assessment of Attachment.
A statistically significant difference between the two groups was observed according to the rates of C3–6 strategies, most frequently noted in prematurely born children (10% full-term and 50% prematurely born) (Fisher’s exact test, p = .01), but not for the rates of the A3–4 strategies (10% full-term and 5% prematurely born) (Fisher’s exact test, p > .05). A statistically significant difference was also observed for the low-risk strategies group (B, A1–2, and C1–2), more frequently observed in the control group (65%) compared to prematurely born children (35%, χ2(1)= 6.4, p < .05).
Hypothesis 2. Increased risk of psychological distress and maladaptation in prematurely born children.
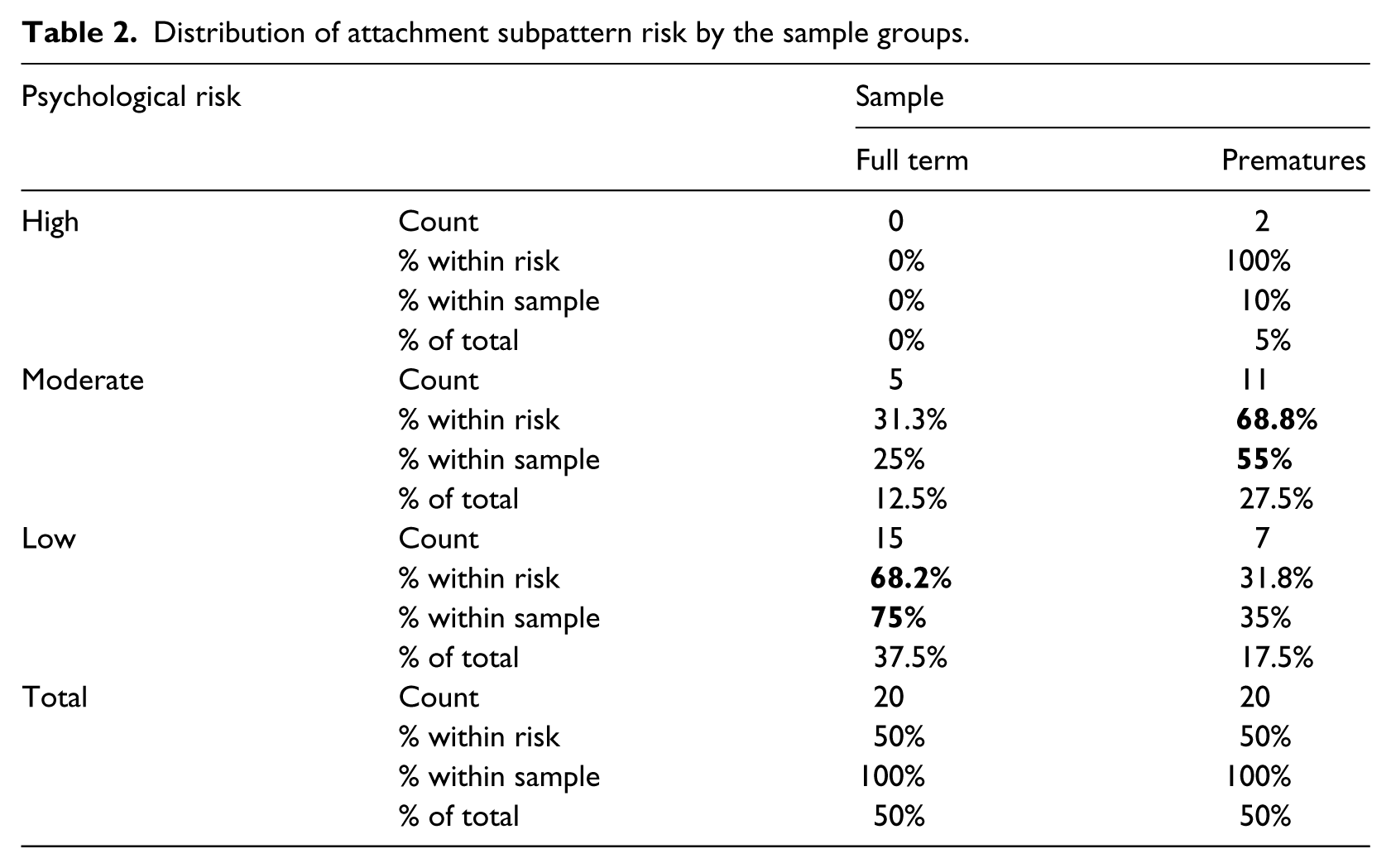
As hypothesized, the incidence of high risk for maladaptation (pre A5–6, C5–6, A/C) was more common in the prematurely born group (10%) compared to the control group (0%) (Fisher’s exact test, p = .033). Rates of low risk (B, A1–2, C1–2) were more common in the control group (75%) than prematurely born children (35%) (see Table 2).
Distribution of attachment subpattern risk by the sample groups.
Hypothesis 3. Higher rates of psychological trauma or loss related to illness or perinatal experience in prematurely born children.
Although psychological traumas were less often assigned to prematurely born children (20%) than to the control group (30%), a statistically significant difference was not found. There was, however, a difference in the basis for the psychological traumas; the control group recorded significantly more family-related traumas (primarily parental separation), and the prematurely born children reported more illness-related events (Fisher’s exact test, p = .003).
Hypothesis 4. Higher rates of modifiers of attachment strategies, in particular depression and expression of somatic state, in prematurely born children.
Prematurely born children presented with depressed strategies more often than the full-term children (20% vs 0%), although this difference was not statistically significant (Fisher’s exact test, p > .05).
Hypothesis 5. Correlation between psychopathological risk and severity of perinatal problems in prematurely born children.
A relationship between the severity of perinatal problems and the risk for psychological maladaptation was found among the prematurely born children (r = .5, p < .05); 85% of prematurely born children with low psychological risk (B, A1–2, C1–2) had low PERI scores (⩾5). Furthermore, 100% of prematurely born children with high PERI scores (>5) were categorized at moderate psychological risk.
Hypothesis 6. Correlations between psychopathological risk and hospitalization days in the neonatal unit in prematurely born children.
The hypothesis was supported with statistical significance (r = .5, p < .05). Of the prematurely born children classified at high psychological risk (pre A5–6, C5–6, A/C), 100% were hospitalized in the neonatal unit for >2 months. Conversely, 57% classified at low psychological risk were hospitalized in the neonatal unit for <1 month.
Discussion
The current pilot study explores and assesses aspects of the psychological development of school-age prematurely born children, without severe health issues, compared to children born at full term, specifically analyzing types of attachment strategies, psychological trauma, and modifiers of attachment strategies. Data available in literature are currently restricted to attachment strategies of prematurely born children at young ages (first months to preschool age) and rely often on parental reporting.
Distribution of attachment strategies
The study highlights a predominance of the coercive Type C strategies by both prematurely born and full-term children. The authors suggest that this finding may reflect a cultural aspect of adaptation in Italy, and requires confirmation from future studies. The prematurely born infant has been described as more passive and disorganized, rendering parenting more difficult as the interactive signals are more complex to decipher. Additionally, parents of prematurely born children have been described as less sensitive than other parents (Baldoni et al., 2009; Cassibba et al., 2012; Forcada-Guex et al., 2006; Muller-Nix et al., 2004) and may in part determine their children’s attachment strategies. Further research is required to explore the reasons for the mothers’ less sensitive interaction, exploring their attachment representations.
Passivity and low parents sensitivity are compatible with the school-age C+ strategies, prevalent in the current sample of prematurely born children. These children can be described as having serious problems in finding predictable contingencies in their parents’ behavior and being, therefore, forced to use affective information to stand their ground and make family matters clearer for them.
Neurocognitive development of VLBW children is often characterized by uncertain outcomes: is this an unspeakable danger for parents? Can this uncertainty influence parental behavior, creating an unpredictable alternation between overprotection for their fragile infant, and anger or frustration for their children’s problems? It is commonly accepted in literature that the parents, and especially mothers, of prematurely born children are more concerned for their child’s health compared to parents of children born full term (Allen et al., 2004; Singer et al., 2007).
Is this unpredictability of the parents connected with the concern for their child’s health, or with further aspects (e.g. parental history)? Direct observations of the parents’ protective strategies could clarify the parents’ contribution to children’s strategic patterning.
Distribution of psychological risk of maladaptation: higher risk for prematurely born children
Unlike studies that used parents’ reports about their children (Bhutta et al., 2002; Cerro et al., 2002; Lund et al., 2012), this study assesses psychological risk through direct assessment of the children. The higher psychological risk shown by prematurely born children in this study is consistent with the higher rates of psychological disorder for this group as reported in literature (Bhutta et al., 2002; Indredavik et al., 2010; Johnson & Marlow, 2011; Lund et al., 2012; Potijk et al., 2012). The percentage of moderate risk of psychological maladaptation in this study for the control group was 25%, consistent with epidemiological findings suggesting that 20% of normative children have psychological disorder (Roberts, Attkisson, & Rosenblatt, 1998). However, discrepancies for Italy may exist, with an Italian study reporting only 9.8% of preadolescents (10–14) diagnosed with a Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, (DSM-IV) disorder (Frigerio et al., 2009). Considering these results, along with information of increased permanent psychological problems during adolescence, including lower rates of secure attachment (Hall et al., 2008; Hallin, Bengtsson, Frostell, & Stjernqvist, 2012; Tideman, 2000), the organization of care of prematurely born children appears to deserve careful thought. In our sample, psychological issues were substantial by school-age children, including uncertainty about sources of danger and fear, vicarious or personal, about their experience of illness. In other words, it may be important to harmonize the needs for an early diagnosis of potential neurodevelopmental problems with the risk of alarming the families of prematurely born children, in order to avoid inadvertently sending them messages about “fragile” children, who need higher generic protection without specifying the nature of their child’s risk.
Psychologically traumatic experiences: the perinatal experience as traumatic for both parents and children
Based on analysis of the child’s SAA discourse, prematurely born children had psychological traumatic experiences less often than children born full term (20% vs 30%). This does not mean that prematurely born children face less dangerous experiences: in fact, their strategic organizations are overall more extreme (as discussed regarding their higher psychological risk), and only in a proportion of cases, their psychological response to danger is considered traumatically unresolved. Nevertheless, we found an interesting difference in the basis for the psychological traumas: full-term children more often recounted family-related traumatic events and prematurely born children recounted illness-related ones. These data may suggest that the family faced with potential health issues of a prematurely born child focuses more attention on health issues at the expense of other family issues. In our sample, only full-term children were traumatized by family issues, such as parental separation. The literature also highlights an increased risk of post-traumatic disorders in mothers of prematurely born children (Holditch-Davis et al., 2003; Kersting et al., 2004; Muller-Nix et al., 2004), and in the prematurely born neonates themselves, cortisol, a stress indicator, higher than the average has been underlined (Habersaat et al., 2014a, 2014b). More investigation regarding the maternal disorder and the trauma it can incur on the children is needed.
Severity of perinatal problems and psychological risk
Our SAA-based findings of psychological risk are coherent with other studies (Fuertes et al., 2006; Udry-Jørgensen et al., 2011) and underline an association between increased psychological risk and more severe perinatal problems and longer hospital stay. Based on the overall PERI score, our sample should be considered at high risk of negative developmental outcomes (Scheiner & Sexton, 1991; Zaramella et al., 2008).
Medical risk and the long postnatal hospitalizations, rather than prematurity itself, may influence both infant self-regulation and parental stress (Bonifacio et al., 2010; Miceli et al., 2000). It is well known that these factors can affect the neurocognitive development (Bonifacio et al., 2010; Miceli et al., 2000) and the quality of the early dyadic interaction, which in turn affects children’s psychological development (Fuertes et al., 2006; Habersaat et al., 2014a; Muller-Nix et al., 2004; Pierrehumbert et al., 2003; Stramrood et al., 2011).
Limitations and directions for future research
This pilot study has inherent limitations associated with a small sample size, and caution should be taken when interpreting the results. The study design lacks the analysis of the parental attachment strategies, and therefore correlations between multiple parental representations and children self-protective strategies could not be made. Additionally, an analysis of the children’s cognitive ability was not performed, and should have been controlled for, as studies show that the IQ of prematurely born children is usually lower than children born full term. However, the study offers valuable information into the psychological well-being of the prematurely born child compared with a control group, and offers insight into a possible link between the parental trauma, associated with the birth and the uncertainty of their child’s health, and the child’s psychological development, and should be considered for future research.
In conclusion, if this pilot study is replicated and expanded, especially to include the analysis of parental attachment strategies, it suggests some clinical applications. First, the SAA may yield clinically relevant information for medical professions without further sensitizing the families to medical fragility, as could be the case with ordinary medical and psychological assessments. The SAA may move the focus of attention to emotive variables, and may hint toward the possible negative impact of considering the prematurely born child as fragile. Additionally, the SAA could be a valid mechanism for understanding better the children’s trauma associated with prematurity. And finally, the study points to possible advantages of professionals being alert to C+ strategies, in order to improve parental consultancy (supporting their awareness of child behavioral strategy) and children assessment, considering how their behavioral strategy influences their own performance (e.g. cognitive performance or academic achievements). In particular, children with C+ strategies can emphasize their incompetence (C4 feigned helpless strategy) or can struggle with the therapist (C3 “aggressive” strategy) during the assessment session; in both cases, the result may be worse performance.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.