
Abstract
Gender dysphoria in adolescence could be expected to be associated with delayed sexual development because of the distress related to the sexual characteristics of the body. However, identity challenges may also increase early and risk-taking sexual behaviours among adolescents with gender dysphoria. We studied sexual experiences among 101 adolescents, attending an adolescent gender identity service, desiring gender reassignment. Their experiences were compared to the sexual experiences of the same-aged population, evaluated in a large adolescent survey. A majority of adolescents with gender dysphoria had been in love or had a crush on somebody. Birth assigned females had experiences of romantic relationships twice as commonly as birth assigned males. Otherwise, there was no statistically significant difference in the adolescents’ sexual experiences. About half of the subjects had experiences of kissing, and about 40% had intimate (genital) sexual experiences with a partner. Compared to the general adolescent population, adolescents with gender dysphoria were less experienced. Autism spectrum disorder was associated with more delayed sexual development.
Introduction
Sexual maturation is one of the most essential developmental tasks of adolescence. Young people’s bodies, emotions and cognitions mature at this time, and this affects intrapersonal, interpersonal and societal interactions (Romeo & Kelley, 2009). The first steps in sexual encounters usually include practices such as kissing and petting. These typically precede first sexual intercourse or other intimate sexual practices by several years. In Western countries, 10% to 30% of adolescents first experience sexual intercourse by the age of 15 and the vast majority by age 20 (Madkour, Farhat, Halpern, Godeau, & Gabhainn, 2010; Savioja, Helminen, Fröjd, Marttunen, & Kaltiala-Heino, 2015). Onset of sexual activity at an early age has been associated with risky sexual behaviours, psychosocial difficulties, and emotional and behavioural disorders (Kaltiala-Heino, Marttunen, & Fröjd, 2015; Madkour et al., 2010; Savioja et al., 2015). In contrast, delay of initiation of sexual activity to the late stages of adolescence may suggest developmental difficulties.
Gender dysphoria (Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5)) refers to a condition in which an individual senses a marked discrepancy between the expressed or experienced gender and that individual’s biological sex (American Psychiatric Association, 2013), with clinically significant distress or impairment in important areas of functioning. In addition to the DSM-5 diagnostic term, gender dysphoria can also refer more broadly to anxiety and distress about gender features – bodily characteristics typically associated with being perceived as male or female – at large. Transsexualism (International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10); World Health Organization, 1992) refers to a persistent desire to live and be accepted as a member of the opposite sex. This is usually accompanied by a sense of discomfort with or the inappropriateness of one’s anatomical sex and a wish to undergo surgery and hormonal treatment to align the body with the experienced gender. Gender variance refers to a spectrum of gender experiences and gendered behaviours, such as perceiving and expressing oneself as male or female, somewhere in between or outside of the male–female continuum. The term ‘transgender’ is used as an umbrella term to refer to a variety of gender identities incongruent with one’s biological sex. Not all those identifying as transgender need to suffer from dysphoria. Cisgender refers to gender experience in agreement with one’s biological sex.
Gender dysphoria and/or transgender identification in adolescence could be expected to be associated with delayed sexual development given that it is the sexual characteristics of the body in particular that are the source of distress in gender dysphoria and that differing from the mainstream may increase the adolescent’s risk of experiencing difficulties in social relationships, including dating and sexual encounters (DeHaan, Kuper, Magee, Bigelow, & Mustanski, 2013). Gender-minority adolescents, as well as sexual minority adolescents, may have a reduced availability and increased challenges in finding potential partners when compared with their cisgender and heterosexual peers (Korchmaros, Ybarra, & Mitchell, 2015). Gender dysphoria is associated with increased likelihood of psychiatric disorders (Holt, Skagerberg, & Dunsford, 2016; Kaltiala-Heino, Sumia, Tyolajarvi, & Lindberg, 2015; Olson, Schrager, Belzer, Simons, & Clark, 2015). Psychiatric disorders have been associated with early and risk-taking sexual behaviour (Kaltiala-Heino, Marttunen, & Fröjd, 2015; Savioja et al., 2015; Savioja, Helminen, Frojd, Marttunen, & Kaltiala-Heino, 2017). It could be concluded that adolescents with gender variation may engage in risky sexual behaviours due to identity experiments or because the associated mental health problems could result in either the searching of comfort in intimacy or in impaired self-protection skills.
As far as we know, only one study has focused on the sexual experiences of treatment-seeking adolescents with gender dysphoria (Bungener, Steensma, Cohen-Kettenis, & de Vries, 2017). This study compared the sexual experiences of 137 transgender adolescents (M (standard deviation (SD)) age: 14.69 (2.2) years) in the Netherlands with those of a same-aged adolescent population. Transgender adolescents had fewer experiences of falling in love, dating, kissing, petting and intercourse than their general population peers. A majority of the transgender adolescents had nevertheless fallen in love, and about half had been involved in romantic relationships. One-fourth had experienced petting while undressed, and 5% had experienced sexual intercourse. The transgender adolescents did not rank sex as important as did the general population adolescents. Another study from the United States briefly commented on sexuality-related issues in a clinical sample of gender-referred adolescents (Olson et al., 2015). In this study, about half of the sample (M (SD) age: 19.2 (2.9) years) reported being sexually active. About half thus were not sexually active, which, given their age, may suggest delayed development in this domain compared to general adolescent population (Madkour et al., 2010; Savioja et al., 2015).
On the other hand, in an adolescent population study (Korchmaros et al., 2015), lesbian, gay, bi, trans and questioning (LGBTQ) adolescents were more experienced with romantic relationships and more active in initiating relationships both online and offline than their cisgender, heterosexual peers. Unfortunately, separate information on transgender adolescents was not presented. In a study of Canadian transgender-identifying adolescents (Veale, Watson, Adjei, & Saewyc, 2016), almost 5% reported a pregnancy experience in the past (had been pregnant/had impregnated a partner), about as commonly as same-aged general adolescent population peers. Studies have also suggested that transgender adolescents are more frequently subjected to negative experiences in the sexual domain, such as sexual harassment (Mitchell, Ybarra, & Korchmaros, 2014) and dating violence (Dank, Lachman, Zweig, & Yahner, 2014). Finally, a body of research focused on gender identity and risk of HIV and other sexually transmitted diseases. These studies have repeatedly found disproportionally high rates of these infections, especially among young adult transfemales (Poteat, Scheim, Xavier, Reisner, & Baral, 2016; Reisner et al., 2015), due to risky behaviours such as sex work and drug use (Brennan et al., 2012). Only one study on gender-referred adolescents has addressed sex work (Olson et al., 2015), finding that 6% of the referred adolescents reported engaging in the trading of sex for favours.
Thus, research to date suggests that gender dysphoria could be associated with both delayed and early sexual development as well as risky sexual behaviour, especially in the latter group. Empirical research on sexual development of adolescents with features of gender dysphoria, or on any other aspect of adolescent development, is scarce (Kaltiala-Heino, Bergman, Tyolajarvi, & Frisen, 2018). Hence, more knowledge is needed to better understand these processes in adolescents with gender identity issues and to develop services that best meet their needs in this realm. We also require information on the impact of early medical interventions on gender dysphoria on these same developmental processes. (Kaltiala-Heino, Bergman, et al., 2018; Shumer & Spack, 2015). Gender reassignment interventions likely have an impact on sexuality. Knowledge about sexual development of adolescents with features of gender dysphoria prior to medical interventions is needed if we want to evaluate the impact of treatment on it. The aim of this study is to describe the sexual experiences of adolescents attending a gender identity service for assessment in Finland, and to compare them with experiences reported by same-aged general adolescent population. More specifically we aim to
Describe the sexual experiences of clinically referred adolescents with features of gender dysphoria, and evaluate possible differences in sexual experiences between birth assigned males and females;
Analyse how age, pubertal timing, age at onset of gender dysphoria and mental disorders, all variables relevant for adolescent development, are related to sexual experiences among adolescents with features of gender dysphoria; and
Compare the sexual experiences of gender-referred adolescents with those of the same age in the general population to assess whether the gender-referred adolescents display similar, delayed or more advanced sexual experiences than same-aged peers at large.
Methods
Sample and procedure
The study is a retrospective chart review of adolescent sex reassignment (SR) applicants attending for assessment by one of the two adolescent gender identity services in Finland (Tampere University Hospital, Department of Adolescent Psychiatry) in the period 2011–2015. The assessments comprise structured and free form questionnaires, interviews by a multidisciplinary team and a review of the adolescent’s previous psychiatric and medical files. The initial assessment always includes an evaluation of psychosexual development. The first author (RK-H) and the second author (MT) were involved in the clinical assessments of all the gender-referred adolescents. The first author (RK-H), using a structured data collection form, collected the research data retrospectively from the case files using all information available after the clinical evaluations. For assessing sexual experiences, the data collection form included questions used in the adolescent population health survey in Finland (Kaltiala-Heino, Kosunen, & Rimpelä, 2003; Kaltiala-Heino, Savioja, Fröjd, & Marttunen, 2018). For the purpose of this study, supplemental questions, not in the population survey, on experiences of oral sex and sexual trauma were added. The study received approval from the ethics committee of Pirkanmaa Hospital District. In total, 107 adolescents were referred during the established study period 2011–2015. Their age range was 14 to 18 years. Of these, eight did not complete the assessments and are not included in the present study. Thus, the study includes 99 SR applicants, 84 birth assigned females and 15 birth assigned males. The mean (SD) age of both the birth assigned females and the birth assigned males is 16.9 (0.9) years.
The sexual experiences among the clinical gender dysphoria sample were compared to those in a population sample of 90,953 boys and 91,746 girls aged 14 to 18 who participated in the School Health Promotion Study (SHPS) in 2010–2011. The SHPS is an anonymous classroom survey on adolescents’ health and health behaviours run by the National Institute of Health and Welfare. The survey has been carried out annually since 1995, since 2008 among both secondary school students (aged 14–16 years old) and upper secondary and vocational school students (aged 16–20 years old). Until 2011, the study was carried out in alternate years in certain parts of Finland. Then the results of 2 consecutive years were combined to represent the whole country. The SHPS was granted approval by the ethics committee of the National Institute for Health and Welfare in Finland. These data have been described in more detail elsewhere (Savioja et al., 2015, 2017). Both the boys and the girls in the SHPS 2010–2011 comparison data used in the present study had a mean (SD) age of 16.3 (1.2) years.
Measures
In the SHPS, sexual experiences were elicited by asking if the respondent had experienced kissing on the mouth (yes/no), light petting (fondling on top of clothes, yes/no), heavy petting (fondling under clothes or naked, yes/no) or sexual intercourse (yes/no). The same information was collected from the case files of the clinical sample adolescents. These experiences were compared between the clinical sample and the population data, except for light petting, which was inconsistently recorded in the case files and therefore not used in the analyses. Because intercourse may be less central to the sexual practices of adolescents with diverse gender identifications, we completed the items in the clinical sample by adding experiences of oral sex (similarly rated yes/no). A variable describing intimate sexual experiences with a partner was then formed, comprising petting under clothes or while naked, intercourse or oral sex. Experiences of any intimate sexual practice (heavy petting, intercourse or oral sex) were then compared between the clinical and the population data. From the case files of the gender dysphoric adolescents, we also recorded whether they had been in love or had a crush on somebody (yes/no), and whether they had romantic relationships (yes/yes but just online/no). Furthermore, experiences of sexual abuse (yes/no) and any other negative sexual experiences (yes/no) were recorded from the case files. These topics are routinely discussed with the SR applicants.
Age (continuous variable) and sex (sex assigned at birth among the SR applicants, sex indicated in the survey response by the population adolescents) were recorded in clinical and population samples.
Further variables used in the analyses in the clinical sample were pubertal timing (early vs. normative or late), age at onset of gender dysphoria (less than 12 vs. 12 or more) and current or previous specialist-level psychiatric treatment history (yes/no) as well as the reasons for the psychiatric treatment as recorded in the case files (depression, anxiety, suicidality/self-harm, psychotic symptoms or psychosis, conduct problems, substance abuse, autism spectrum disorder, attention deficit hyperactivity disorder (ADHD); each yes/no). The distribution of these characteristics among the clinical sample is presented as sex assigned at birth in Table 1.
Age, pubertal timing, age of onset of gender dysphoria and psychiatric treatment contact as well as reasons for it among clinically referred adolescents with features of gender dysphoria.
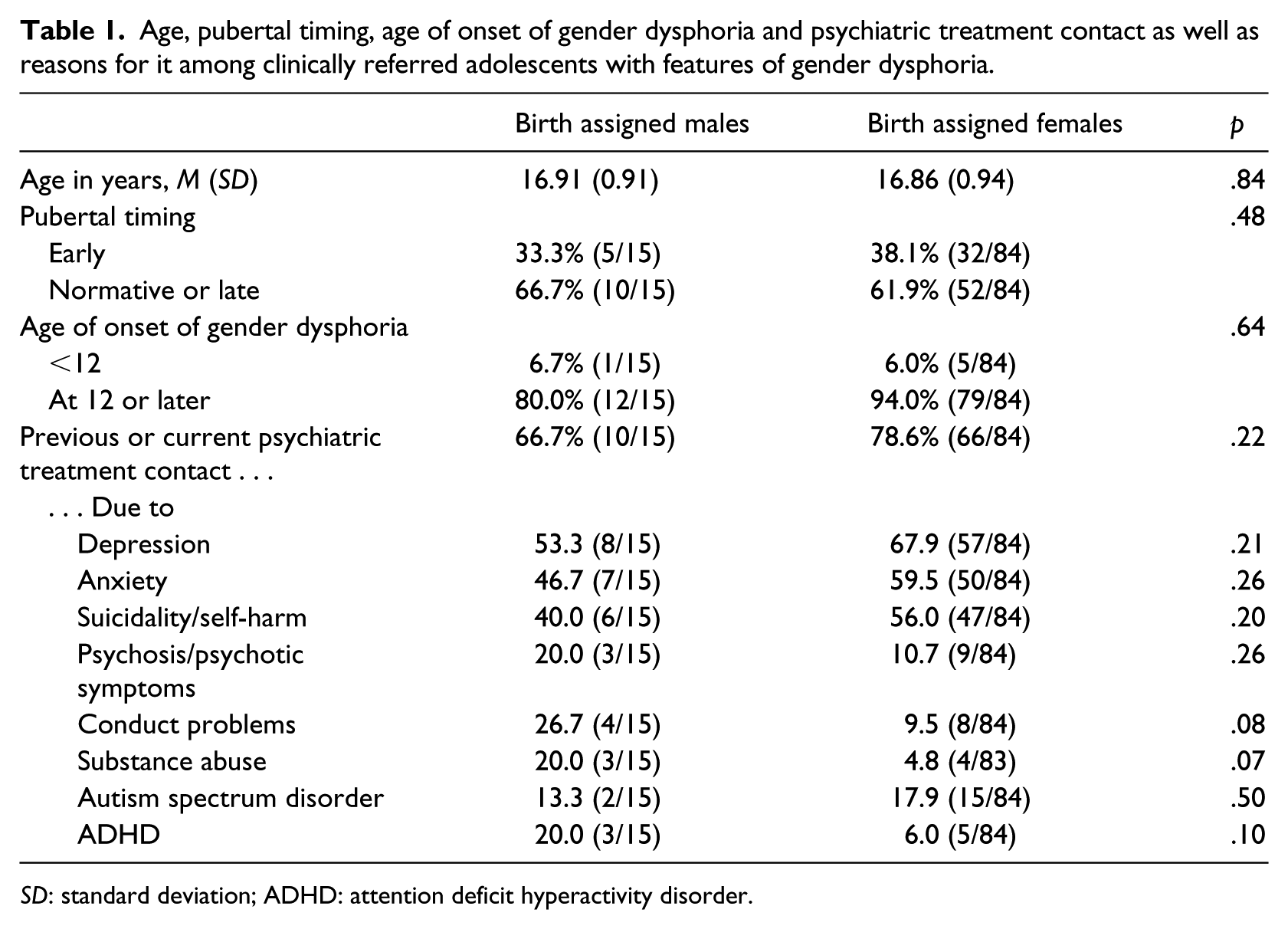
SD: standard deviation; ADHD: attention deficit hyperactivity disorder.
To classify pubertal timing, age at menarche/oigarche was recorded. Pubertal timing was classified as early if the adolescent had experienced menarche or oigarche at age 11 or earlier. If this exact information was not available, perceived pubertal timing in relation to same-aged peers (pubertal changes started earlier/at the same time/later than in most of the same-aged peers) was used. Of the birth assigned females, 94% (79/84) recalled age at menarche, whereas of the birth assigned males, only 26.7% (4/15) recalled age at oigarche, but when perceived timing as compared to same-aged peers was added, estimate of pubertal timing was available for all in the clinical sample.
These variables were used because of their potential relevance for the issues studied. Early pubertal timing is associated with earlier and risk-taking sexual experiences in adolescence (Downing & Bellis, 2009; Kaltiala-Heino, Fröjd, & Marttunen, 2015), and early pubertal timing is also more common among adolescents with clinical gender dysphoria than in same-aged population (Sumia, Lindberg, Tyolajarvi, & Kaltiala-Heino, 2016). Age at onset of gender dysphoria is important because virtually no empirical studies have been presented concerning adolescent-onset gender dysphoria (Kaltiala-Heino, Bergman, et al., 2018). Psychiatric disorders have an impact on sexual development (Kaltiala-Heino, Fröjd, & Marttunen, 2015; Savioja et al., 2015, 2017).
Statistical analyses
Sexual experiences in the clinical sample are presented for birth assigned males and birth assigned females. Comparisons of all studied sexual experience items between birth assigned males and birth assigned females were made using cross-tabulations with chi-square statistics/Fisher’s exact test, where appropriate.
Proportions of having engaged in intimate sexual experiences with a partner were compared between birth assigned males and birth assigned females, between those with and without psychiatric treatment history, those with and without early pubertal timing and those with childhood (<12) versus adolescent (12 and older) onset gender dysphoria using cross-tabulations with chi-square statistics/Fisher’s exact test, where appropriate.
Multivariate associations were studied using logistic regression, entering intimate sexual experiences with a partner as the dependent variable and sex assigned at birth, age, pubertal timing, psychiatric treatment history and onset of gender dysphoria as independent variables. Odds ratios (ORs) with 95% confidence intervals (CIs) are given.
To study the role of psychiatric comorbidities in greater detail, bivariate (cross-tabulation with chi-square/Fisher’s exact test statistics) and multivariate analyses (as described above) were carried out using kissing and intimate sexual experiences as outcome variables and each reason for psychiatric treatment in turn as the explanatory variable.
Sexual experiences of the clinical sample were finally compared with those in the general population, first using cross-tabulations with chi-square statistics. Next, differences between the clinical sample and the population were studied using logistic regression controlling for age and sex (as previously defined for each group).
Missing data
For the purpose of this study, if patients’ various sexual experiences were documented in the file, they were then recorded as yes. However, as comments were not systematically made on sexual behaviours the adolescent had not experienced, then behaviours not mentioned were recorded as no.
In the population data, 1.3% had skipped the item concerning kissing, 1.7% light petting, 2.1% heavy petting and 2.7% intercourse. Given the large size of the data, this is unlikely to bias the representativeness of the information collected.
Results
Sexual experiences among the clinical sample with features of gender dysphoria
Of adolescents attending gender identity service, 83.3% had been in love with or had a crush on someone else, and 63.6% had experiences of going steady. Experiences of kissing were reported by 61.6%, 38.4% had experienced heavy petting, 19.2% intercourse and 14.1% oral sex. Any intimate sexual experiences with a partner (heavy petting, intercourse, oral sex) were reported by 39.4% and 49.5% had experiences of solo sex. Birth assigned males had fewer experiences of going steady than birth assigned females, but otherwise no differences were detected according to sex assigned at birth (Table 2).
Sexual experiences among adolescents attending gender identity service in Finland (% (n/N).
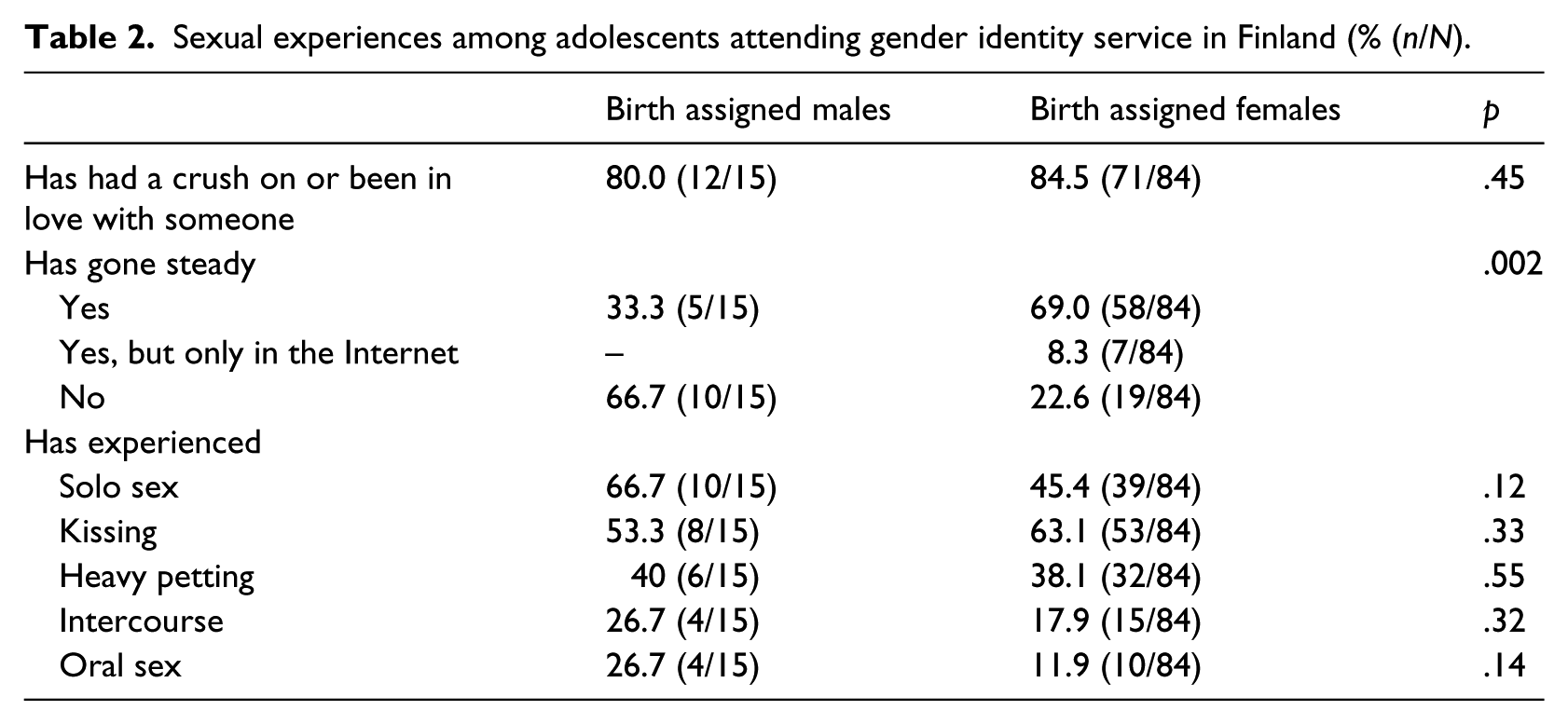
Of the gender-referred adolescents, 5.2% reported experiences of sexual abuse and 6.4% other distressing and negative sexual experiences, with no statistically significant difference between birth assigned males and birth assigned females.
Of the birth assigned males, 40% (6/15) reported intimate sexual experiences with a partner (heavy petting, intercourse or oral sex), of the birth assigned females, 39.3% (33/84) (p = .59). Those who had intimate sexual experiences with a partner were slightly older than those who had not (17.2 (0.8) vs. 16.7 (1.0) years, p = .004). Intimate sexual experiences were less common among those with early pubertal timing than among those with normative or late timing (24.3% (9/37) vs. 48.4% (30/62), p = .02). Age at onset of gender dysphoria (<12 vs. 12 or later) and specialist-level psychiatric treatment history were not associated with intimate sexual experiences with a partner. When these variables were entered simultaneously as independent variables in logistic regression, increasing age (continuous) was associated with increased OR for having intimate sexual experiences with a partner (OR = 2.1, 95% CI = [1.1, 3.7]), and early pubertal timing with decreased OR (0.29, 95% CI = [0.08, 0.87]).
To study the role of psychiatric comorbidities in more detail, we further analysed kissing and intimate sexual experiences with a partner by each of the recorded reasons for psychiatric treatment. Adolescents who had a treatment history due to autism spectrum disorder had these experiences less common in both bivariate and multivariate analyses. Of those treated for autism, 23.5% (4/17) had experiences of kissing, of those never treated for autism, 69.5% (57/82), p < .001. Of those currently or previously treated for autism spectrum disorder, 11.8% (2/17) had intimate sexual experiences, compared to 45.1% (37/82) of those without treatment for autism (p = .008). In logistic regression model controlling for sex, age, age of onset of gender dysphoria and pubertal timing, treatment due to autism spectrum disorder persisted as associated with fewer experiences of kissing (OR = 0.11, 95% CI = [0.03, 0.49]) and less commonly having intimate sexual experiences with a partner (OR = 0.1, 95% CI = [0.01, 0.9]).
Comparison to adolescent general population
Adolescents in the clinical sample had less commonly experienced kissing (61.6% vs. 71.5%, p < .02), borderline less commonly heavy petting (38.4% vs. 46.6%, p = .06) and less commonly intercourse (19.0% vs. 34.9%, p < .001). Combining the intimate, genital experiences (heavy petting and/or intercourse and/or oral sex), the difference between groups diminished to a tendency in bivariate analyses: of the clinical gender dysphoric sample, 39.0%, and of the general population adolescents, 46.8%, reported at least one of these (p = .07).
Because the adolescents in the population data were slightly younger than the SR applicants and the sex distribution was more even among them, group differences were adjusted for age and sex. After controlling for age and sex, the adolescents in the clinical sample were less likely to have experienced kissing (OR = 0.44, 95% CI = [0.29, 0.67]), intercourse (OR = 0.27, 95% CI = [0.16, 0.45]) or any intimate sexual practices with a partner (OR = 0.47, 95% CI = [0.31, 0.70]).
Discussion
The aim of this study was, first, to describe sexual experiences of adolescents clinically referred due to features of gender dysphoria and compare these experiences between birth assigned males and females. Second, our aim was to evaluate the role of age, pubertal timing, age of onset of gender dysphoria and mental disorders on sexual experiences in this group. A third aim was to compare the experiences of the gender-referred adolescents with those of the same-aged peers. A majority of the gender-referred adolescents had been in love and gone steady as well as experienced kissing. Almost 40% had intimate sexual experiences with a partner and about a half had tried solo sex. Differences between birth assigned males and females were few. Sexual experiences were more common among older adolescents and, unexpectedly, less common among those with early pubertal timing. Adolescents with a diagnosis of autism spectrum disorder had fewer sexual experiences than those without autism spectrum disorder. Gender-referred adolescents had less sexual experiences than reported by same-aged population.
Sexual experiences of gender-referred adolescents
A majority of the gender-referred adolescents in our clinic had experiences of being in love, going steady and kissing, and about a half had experienced solo sex. Intimate sexual experiences with a partner were somewhat less common. These findings are in line with another North European study by Bungener et al. (2017) from the Netherlands, except that in our sample experiences of intercourse were more common than in the corresponding Dutch sample. In both ours and in the Dutch study, sexual experiences became more common and intimate among older subjects, as is normative during adolescence (Dalenberg, Timmerman, & van Geert, 2018; Madkour et al., 2010). These findings suggest that sexual experiences advance among adolescents with gender dysphoria in a similar way as among adolescents at large, even if distress related to sexual characteristics of the body could also result in discontinuities in sexual development. In a study by Olson et al. (2015) in the United States, on the other hand, only a half of clinically referred adolescents with features of gender dysphoria were sexually active even if they were on average a couple of years older than our subjects. More research is needed for understanding possible cultural influences on sexual behaviour and experiences of gender dysphoric adolescents.
Among the gender-referred adolescents, birth assigned females had more common experiences of romantic relationships than birth assigned males. Femininity in boys is less accepted than masculinity in girls (Ristori & Steensma, 2016), which may contribute to this finding: gender-nonconforming boys may face more peer rejection and difficulties in finding romantic partners than corresponding girls. Otherwise, sex differences were not seen in sexual experiences of gender-referred adolescents. The small number of birth assigned males in our sample may have limited the power of our study to detect statistically significant gender differences in the sexual experiences of the adolescents with gender dysphoria, but, on the other hand, sex differences were not detected in the comparable Dutch study, either (Bungener et al., 2017).
The role of pubertal timing, age of onset of gender dysphoria and mental disorders
Early pubertal timing has, in adolescent general population studies, been associated with earlier onset of intimate sexual behaviours (Downing & Bellis, 2009; Kaltiala-Heino, Fröjd, & Marttunen, 2015). Early pubertal timing has also been associated with a number of mental health complaints (Kaltiala-Heino, Koivisto, Marttunen, & Fröjd, 2011) and likewise with gender dysphoria in adolescence (Sumia et al., 2016). In the present sample of adolescents clinically referred due to features of gender dysphoria, early pubertal timing, however, was associated with less sexual experiences. This was unexpected, and the topic needs to be assessed further in future studies.
Age at onset of gender dysphoria had in our data no associations with indicators of sexual development, but as the number of childhood onset cases was very small, conclusions need to be drawn with caution. Clinical guidelines for the treatment of gender dysphoria among adolescents are nevertheless informed mainly by knowledge gained from childhood onset gender dysphoria intensifying in puberty (Cohen-Kettenis & Klink, 2015). There is little empirical research on adolescent-onset gender dysphoria, particularly among birth assigned females, which seems to be increasing across the Western world (Aitken et al., 2015; Kaltiala-Heino, Bergman, et al., 2018; Marchiano, 2017; Wood et al., 2013). Comprising mainly subjects with adolescent-onset gender dysphoria, all our findings provide novel information of this little researched group.
Psychiatric disorders could both delay the onset of sexual behaviours, for example, because of lower self-esteem, deficits in social skills and negative appraisals of social interactions, and advance the initiation of sexual contacts through a desire to seek comfort in intimacy, through deficient skills in protecting oneself or through disinhibition (Kaltiala-Heino, Fröjd, & Marttunen, 2015; Savioja et al., 2015, 2017). Thus, psychiatric treatment history may comprise influences that contradict each other. Gender-referred adolescents also display psychiatric disorders at disproportionately high frequency (Kaltiala-Heino, Bergman et al., 2018). However, among the gender-referred adolescents, sexual experiences were not associated with having a psychiatric treatment history in general. In more detailed analyses, having a treatment history due to autism spectrum disorder was associated with fewer sexual experiences. Difficulties in reciprocal social interaction, both in understanding and in communicating, are core features of autism spectrum disorder (American Psychiatric Association, 2013). It is thus understandable that autistic disorders delay such delicate and complex interactions as romantic and erotic relationships. Autism spectrum adolescents with gender identity issues likely face excessive challenges in the romantic/erotic life domain. As has also been noted earlier, autism was vastly overrepresented in our sample of gender-referred adolescents (Van Der Miesen, Hurley, & De Vries, 2016).
Reported prevalence of sexual abuse and other negative sexual experiences was unexpectedly low in this sample, given that, for example, sexual harassment and dating violence have been reported to be particularly common among gender diverse adolescents (Dank et al., 2014; Mitchell et al., 2014). Trauma history is always a part of the assessments in the study unit. Reported prevalence of sexual abuse and other negative sexual experiences was also unexpectedly low given that the psychiatric disorders were common in our subjects, and sexual trauma is an important risk factor for psychiatric morbidity (Chen et al., 2010). This does not suggest that sexual trauma would be an important link between gender dysphoria and psychiatric disorders.
Sexual experiences of the gender-referred adolescents compared with those of the same-aged peers in the population
Fourteen- to eighteen-year-old adolescents clinically referred due to features of gender dysphoria were sexually less experienced than their same-aged peers in the general population. It is understandable that gender dysphoria is associated with delays in sexual development because it is the sexual characteristic of the body that is perceived as the source of distress in gender dysphoria. This may inhibit engagement in sexual encounters. Similar difference to the general adolescent population was seen in the study of Bungener et al. (2017) in the Netherlands. Sexual experiences nevertheless became more common with increasing age, as is developmentally appropriate. The gender-referred adolescents had also experienced falling in love as commonly as has been reported in adolescent population of same age (Kaltiala-Heino, Lindberg, Fröjd, Haravuori, & Marttunen, 2018). In the emotional level of sexual development, the clinical sample adolescents thus did not display slower rate than same-aged peers at large.
Studies in different contexts, such as population surveys, or in young urban transgender communities found the same or increased level of sexual activity in sexual and gender minority youth compared to sexual and gender majorities, and focused on significant sexual risk taking such as sex work in HIV risk (Brennan et al., 2012; Korchmaros et al., 2015; Poteat et al., 2016; Reisner et al., 2015; Veale et al., 2016). Our sample of clinically referred adolescents seeking gender reassignment was different. Cultural and social factors may also play a role here, given that the above adolescent studies were all carried out in North America and ours in Northern Europe. It can also be that adolescents with features of gender dysphoria who seek contact to gender identity services are an essentially different group from transgender-identifying youth in the community.
Early and risk-taking sexual behaviour in adolescence has been associated with a variety of difficulties between adolescents and their parents among adolescents at large (Kotchick, Shaffer, Forehand, & Miller, 2001; Wight, Williamson, & Henderson, 2006) and in gender minority adolescents (Ryan, Huebner, Diaz, & Sanchez, 2009; Wilson, Iverson, Garofalo, & Belzer, 2012). Parental hostile reactions and rejection are often discussed in the literature concerning gender variance among adolescents (Mayer, Garofalo, & Makadon, 2014) and have been associated with social marginalization and, for example, sex work (Brennan et al., 2012). In our data, there were no cases of parental rejection or physical abuse towards the gender dysphoric adolescents. This may be a factor protective of early and risk-taking sexual behaviour in our sample. If such problems emerged, the child welfare services, which are very strong in Finland, would be available to support the adolescent as needed. Sex work was not an issue in the present sample.
Methodological considerations
A limitation of the present study is the moderate sample size of gender-referred adolescents. However, our sample included all who completed the assessments in one of the two specialized adolescent gender identity services in the country, and thus the sample is well representative of the target population. The data size allowed nevertheless meaningful comparisons with population data. A strength of the study is that we could take the population data into account and collect corresponding information from the case files.
Structured surveys during assessments could have improved data quality by ensuring systematic elicitation of all details in the same way as in the SHPS, but, on the other hand, this information was elicited by experienced clinical staff, which increases the likelihood that the adolescents disclosed their experiences. In our clinic, sexual experiences are always elicited from all adolescent psychiatric patients, including those referred due to gender identity issues, because sexual development is such a central aspect of adolescent development, and the stage and progression of adolescent development are central factors for planning developmentally sensitive treatment in adolescent psychiatry. We always ask about sexual experiences and their emotional meaning, about aspects of safe sex and responsibility and about possible traumatic experiences on the sexual domain. We find this a very important topic to discuss with the gender-referred adolescents. The discussion about sexuality-related topics takes place in free format, as it needs to be adjusted according to the adolescent’s age, developmental level, cognitive capacity, personality and ease/difficulty to talk about these topics, but the aim is to form a comprehensive picture of the adolescent’s sexual development and needs in this domain. Consequently, information such as that elicited in School Health Promotion Survey is easy to collect from case files.
First intercourse is often discussed as sexual debut in adolescent sexual health research. Practices such as kissing and petting usually precede intercourse by several years (Dalenberg et al., 2018; Madkour et al., 2010). In sexual and gender minority youth, intercourse may not be an important aspect of sex life in any developmental phase. In sexual minority youth, oral sex or genital petting may rather represent sexual initiation (Goldberg & Halpern, 2017). We therefore focused more on comparing any intimate sexual experiences than experiences of intercourse. In the SHPS survey, the presentation of questions on sexual experiences may appear heteronormative, as if suggesting intercourse as a self-evident final step, but with the gender-referred adolescents, the topic was of course discussed in a more diversity-sensitive way. It is, however, noticeable that a considerable minority of gender-referred adolescents, particularly of birth assigned males, had experienced (heterosexual) intercourse. Therefore, discussing contraception and prevention of sexually transmitted diseases (STIs) also needs to be addressed. Assuming that intercourse is not relevant for gender dysphoric adolescents would also be prejudiced.
We were able to analyse the role of different psychiatric disorders for sexual experiences in the gender-referred group, which is a strength, but a limitation is that the validity of the diagnoses in previous psychiatric contacts needs to be considered with a certain caution. The files obtained from previous treating agents were not always complete and did not provide diagnoses according to ICD-10, and we were not able to check in the databases of the previous treatment providers what ICD diagnoses were recorded there. Thus, we recorded reasons for previous treatment based on verbalizations in the referrals and available copies of previous files. This only allowed a rough descriptive classification of problems related to anxiety, depression, suicidal behaviours, conduct problems, autism spectrum–related problems, substance abuse, psychotic symptoms and others. We only recorded these problems if the adolescent had a psychiatric treatment contact. The data give a picture of the primary problems in previous psychiatric treatment contacts but not of all possible symptoms. Therefore, our figures for problems related to anxiety, depression and so on are likely underestimates (Kaltiala-Heino, Sumia, et al., 2015).
Sexual orientation and gender identity are different entities, and transgender people present with a variety of sexual orientations. Nevertheless, sexual orientation has long been used to subtype Gender Dysphoria/Transsexualism (Lawrence, 2010). During adolescence, the different facets of sexual orientation – attraction, behaviour and identity – may still be developing (Saewyc et al., 2004), and there may be changes over time in all of them (Diamond, 2000; Savin-Williams & Cohen, 2015). Therefore, we find it more important to determine whether adolescents with gender dysphoria or transgender identity display developmentally appropriate and favourable involvement in romantic and erotic relationships than to focus on orientation. Therefore, we did not systematically collect data on sexual orientation, which may, however, be seen as a limitation in the present study.
Conclusion
Adolescents with features of gender dysphoria that warrant clinical attention display a delayed sexual development compared with same-aged general population, but many nevertheless have age-appropriate erotic experiences. Autism, overrepresented in gender-referred adolescents, is in this group particularly associated with delayed sexual development. Clinicians working with adolescents with features of gender dysphoria need to discuss sexuality and sexual health issues with them. Aspects of contraception and safe sex may need attention, as may on the other hand uncertainties and perceived obstacles for seeking age-appropriate romantic and erotic contact.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.