
Abstract
Mental health stigma continues to be a significant barrier for psychiatric care in youth. Parental misperceptions regarding mental health may interfere with their child’s care and negatively influence their child’s view of mental health. For some children, their first experience with psychiatry occurs during medical hospitalization when they are seen by the Pediatric Consultation-Liaison (C/L) Psychiatry Service. Despite this unique role, there is sparse research on how to address mental health stigma with patients and families within the context of Pediatric C/L Psychiatry. This study explores the use of a brief educational video with messages from the Pediatric C/L Psychiatry team, families who have accessed mental health consultation in the hospital, and brief video interactions between family and the C/L team, to address mental health stigma. Common misconceptions are addressed during the video with the intent of reducing negative parental perceptions relating to mental health care. Families are given a survey highlighting these concerns, prior to and after watching the video. Pre- and post-intervention responses were compared using paired sample’s t-tests. Results indicated that the video did positively change parent’s confidence that psychiatry can be helpful, reduced their preconceived stigma regarding confidentiality, while alleviating concerns regarding psychotropic medication use in youth. Use of an educational video may be feasible, time efficient, and effective at reducing parental mental health stigma.
Introduction
Stigma is commonly defined as “an individual with an attribute” who is different from others in a less desirable way and is “thus reduced in our minds from a whole and usual person to a tainted, discounted one” (Goffman, 1963). Stigma continues to be a significant barrier to seeking mental health services. Mental health stigma in youth is often multifactorial and involves the perspectives of the child, caregivers, family, medical professionals, and their communities. Despite attempts to combat stigma, stigma remains a significant barrier to accessing mental health services among youth. This, along with limited psychiatric and psychotherapeutic resources in the community, has resulted in 64.1% of youth with major depression not receiving mental health treatment (Mental Health in America, 2018).
For some children, their first opportunity to see a pediatric psychiatrist arises when they are medically hospitalized and have comorbid psychiatric concerns impacting medical care. Inpatient Pediatric Consultation-Liaison (C/L) Psychiatry services are often a conduit to these services and have an important role in inpatient medical and psychiatric care. A nationwide study of discharged pediatric patients found that 10% were hospitalized for a primary mental health concern, while an additional 17–22% had a primary physical health diagnosis with a comorbid mental health diagnosis (Bardach et al., 2014). Nearly half of medically hospitalized youth have more than one comorbid psychiatric diagnosis (Bujoreanu, White, Gerber, & Ibeziako, 2015). Pediatric C/L Psychiatry interventions can reduce hospital length of stay, improve patient care, reduce polypharmacy, and reduce rate of hospital recidivism (Bourgeois, Kremen, Servis, Wegelin, & Hales, 2005; Bujoreanu et al., 2015; Hall & Frankel, 1996). Pediatric C/L Psychiatry services offer a unique way to reach vulnerable youth who require mental health care but may not have accessed care due to a variety of barriers, including stigma. Furthermore, youth with comorbid physical and psychiatric health concerns are at high risk of clinical decompensation and often experience poorer quality of life (Chen et al., 2009). Psychiatric consultation in pediatric medical settings offers a valuable opportunity to educate and care for the mental health needs of high-risk patients and families, while combating stigma.
Besides mental health stigma, many families have limited awareness that C/L psychiatric services exist, how to access these services, and what they entail. This limited understanding and awareness may be equally limiting in youth with medical and psychiatric comorbidity accessing mental health services during inpatient pediatric settings. The relative impact of mental health stigma and level of awareness of inpatient pediatric C/L psychiatric services is vastly understudied. The relative contribution of these factors toward accessing needed mental health services in the inpatient pediatric setting is not described in current literature. Regardless, both of these factors limiting access to pediatric C/L psychiatric service can be mitigated through psychoeducation, specifically the use of an educational video. Psychoeducation through the use of video has been shown to be effective in reducing stigma, improving attitudes, and enhancing behavioral intentions related to mental health in adolescents and adults (Corrigan, Morris, Michaels, Rafacz, & Rüsch, 2012). The demonstrated value of educational video use in other settings and with other populations, as well the ability of videos to improve caregiver awareness and understanding of mental health treatment choices, supported the use of video as a potential intervention in addressing parental stigma in pediatric C/L psychiatric care.
This study aims to determine if using an educational video regarding inpatient pediatric C/L psychiatric services with patient and family testimonials on their experience with the service can reduce stigma toward, and improve awareness of, Pediatric C/L Psychiatry during pediatric medical hospitalization. It is hypothesized that following the viewing of such a video, parental ratings of mental health stigma will be reduced with improved attitudes toward, and awareness of, Pediatric C/L Psychiatry and mental health care in this setting.
Methods
Study design
This is a single-center pilot study regarding the use of an educational video to address caregiver mental health stigma, and awareness of C/L psychiatric services, among pediatric patients admitted to an academic children’s hospital at any time prior to the study period. This pilot study will inform the feasibility and value of future study of video-based psychoeducation regarding C/L psychiatric services in the inpatient pediatric setting. This study involved surveying caregivers on their perceptions and beliefs regarding pediatric mental health care prior to and after watching a brief educational video. Preparatory work for the study, including literature review, survey development, video production, and elicited feedback on the video, occurred from August 2016 to October 2017. Data collection and study implementation began on November 6, 2017 and concluded on December 4, 2017. Pediatric patients were defined as any patient medically admitted to the academic pediatric hospital between the ages of 0 and 17, inclusive. Caregivers were defined as parents, or other primary caregivers, who provide primary support for a given pediatric patient’s care needs on a regular basis. The study was approved by the University of Michigan Health System Institutional Review Board.
Study site and C/L psychiatry service description
The Pediatric C/L Psychiatry service functions within a 221-bed children’s hospital, which is physically co-located with the larger academic health system. The hospital houses pediatric, neonatal, and cardiothoracic intensive care units, a pediatric emergency room, a co-located 16-bed child and adolescent inpatient psychiatric hospital, and access to all approved pediatric subspecialty services. There is an active child life service, pediatric psychology service, Pediatric C/L Psychiatry service, palliative care service, and adolescent medicine service. In the larger health system, there is access to a psychiatric emergency room that serves patients across the life span.
The Pediatric C/L Psychiatry service is composed of a 1.0 full-time equivalent (FTE) child and adolescent psychiatrist who is boarded in pediatrics, general psychiatry, and child and adolescent psychiatry, 1.0 FTE pediatric nurse practitioner, 0.5 FTE social worker, and a child and adolescent psychiatry fellow. Psychological services are provided through a separate service line by the Division of Pediatric Psychology within the Department of Pediatrics. These two service lines collaborate often and conduct shared care conferences and care coordination meetings. The Pediatric C/L Psychiatry service is primarily involved in guiding hospital-wide initiatives in mental health prevention efforts, education, screening, and consultations for evaluation and management of psychiatric concerns. The C/L Psychiatry service provides non-pharmacologic and pharmacologic intervention, and this is negotiated in advance with the Pediatric Psychology service if both services are involved in a given case. The C/L Psychiatry service consults exclusively to the inpatient pediatric setting with no ambulatory or Emergency Department consultation. On average, the C/L Psychiatry service sees 45 new consultations and 180 follow-up consultations per month.
Participants
Participants were recruited from the children’s hospital Patient- and Family-Centered Care Committee (PFCC) listserv. The PFCC consists of parents and other caregivers of youth who have been patients at any time at the children’s hospital with varying physical and mental health comorbidities. All e-mail addresses associated with the PFCC listserv were emailed a link to a simple survey created using Qualtrics. Qualtrics is a subscription software for collecting and analyzing data for research, customer satisfaction, product testing, and website feedback (Qualtrics, 2018).
Video design and development
The video was designed to introduce the members and services of Pediatric C/L Psychiatry and to address pediatric mental health stigma (video available on request). The video details the utility of mental health consultation in medically hospitalized youth, components of a typical consultation, and how the service can aid in the diagnostic evaluation and management within the hospital setting. Several common mental health stigmas are addressed as per the special section of the National Stigma Study–Children (NSS-C) (Pescosolido, 2007; Pescosolido, Perry, Martin, McLeod, & Jensen, 2007). Embedded throughout the video are live action shots of the Pediatric C/L Psychiatry service interacting with patients, families, and care team members. The video incorporates three caregiver testimonials on their interactions with the Pediatric C/L Psychiatry service. The video was reviewed by the University of Michigan Child and Adolescent Psychiatry Fellowship Program, several faculty and staff in the Department of Psychiatry, and the PFCC Advisory Board. The final video is approximately 8 minutes in duration. All participants shown in the video completed formal written consent to participate in the video and its dissemination.
Survey design and implementation
General sociodemographic information about the caregiver and the identified patient was collected. Additional categorical information gathered included experience with mental health services, including therapy, psychotropic medication use, and previous mental health diagnosis, of both the caregiver and their children. Survey questions were adapted from two validated national scales used to address caregiver stigma to identify general caregiver attitudes toward pediatric psychiatry and stigma toward psychiatric care and psychotropic medication use (Pescosolido et al., 2007; Turner, 2012).(Tables 1 to 3). Participants were asked to rate their views along a 5-item Likert-type scale from strongly agree (1) to strongly disagree (5). Respondents completed these components of the survey prior to viewing the video and then subsequently after viewing the video. Although the C/L Psychiatry Service provides diagnostic assessment and non-pharmacologic intervention, this was a relatively small component of the survey given the desire to preserve the integrity of use of the validated surveys used in the study, as well as the significant overlap with the services provided by the Pediatric Psychology service at the study site.
Stigmatizing attitudes toward pediatric mental health (Adapted from PATPSI Study), N = 30 (Turner, 2012).
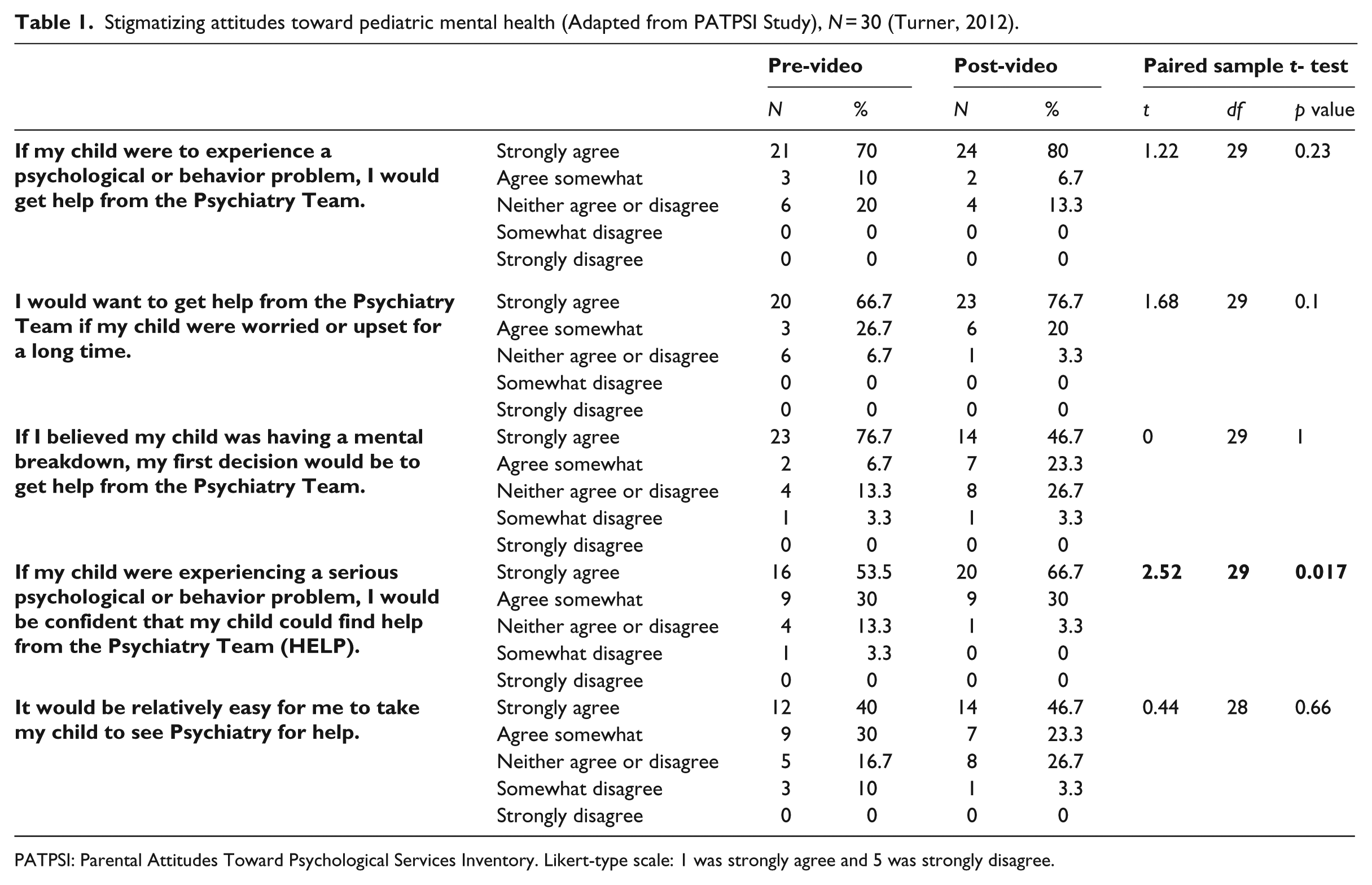
PATPSI: Parental Attitudes Toward Psychological Services Inventory. Likert-type scale: 1 was strongly agree and 5 was strongly disagree.
Participants completed part 1 of the survey, which included questions regarding general demographic information, as well as caregiver stigmatizing attitudes and beliefs about psychiatric care. Participants were then instructed to watch an embedded video in the survey. They could not move to part 2 without watching the video. After the video concluded, participants filled out part 2 of the survey, which included identical measures of caregivers’ stigmatizing attitudes and beliefs about psychiatric care. Results were recorded anonymously, and data were de-identified. Respondents could only respond once to the survey given unique identifiers embedded in the survey link. The survey was non-incentivized.
As the PFCC does not maintain an active listserv, a convenience sample from the PFCC was taken. The survey was emailed to a contact list of caregivers at weekly intervals over a 1-month period. 45 participants accessed the survey and 30 of those participants completed the survey in its entirety. Data were analyzed only for those 30 respondents who completed the survey in its entirety during the study period.
Data analysis
Analyses were conducted using IBM SPSS Statistics 24. A series of paired samples t-tests were conducted to compare pre-intervention (1) to post-intervention (2) responses on the 13 individual stigma-related questions.
Results
Of the 30 survey respondents, 90% were female and 97% were Caucasian. Most respondents were 45–54 years of age (50%), followed by 35–44 (26.7%), 55 or older (13%), and 25–34 (10%). All respondents had at least a high school education. Two-thirds of the respondents had themselves received mental health care in the past and 13.3% were currently receiving some type of mental health care. Half of respondents had a child who had previously been seen by psychiatry and 76.7% had children who had participated in psychotherapy, predominantly for anxiety (23.3%) or depression (13.3%).
Video effects on caregiver attitudes
There was a statistically significant increase in response to the individual question of “confident my child could find help from the psychiatry team” (t(29) = 2.52, p = .017) (Table 1). There were no significant differences in the other four individual questions regarding caregiver attitudes.
Video effects on caregiver stigma related to pediatric mental health
Among the questions regarding caregiver stigma, concerns regarding mental health confidentiality for their child decreased significantly following viewing of the video (t(29) = –3.75, p = .001) (Table 2). There were no significant differences in the other three questions regarding caregiver stigma relating to pediatric mental health.
Stigmatizing perceptions pertaining to mental health treatment for youth (Adapted from Special Section, National Stigma Study–Children), N = 30 (Pescosolido, 2007; Pescosolido et al., 2007).
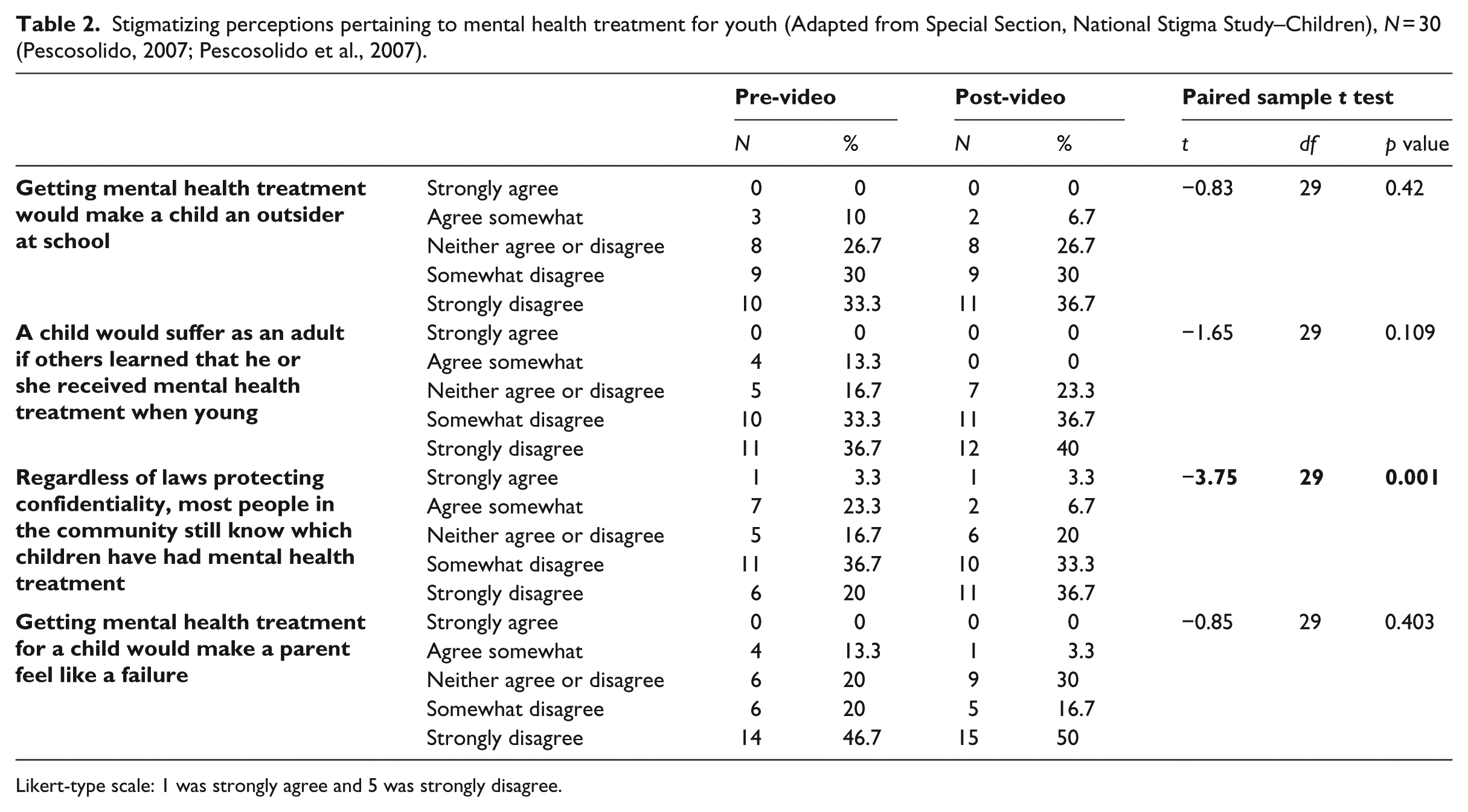
Likert-type scale: 1 was strongly agree and 5 was strongly disagree.
Video effects on caregiver stigma related to psychotropics
There were statistically significant improvements in caregiver stigma relating to overmedication (t(29) = –2.5, p = .018) and long-term negative effects of psychotropic medication use in youth (t(29) = –2.07, p = .048) (Table 3).
Stigmatizing attitudes regarding psychotropic use in youth (Adapted from Special Section, National Stigma Study–Children), N = 30 (Pescosolido, 2007; Pescosolido et al., 2007).
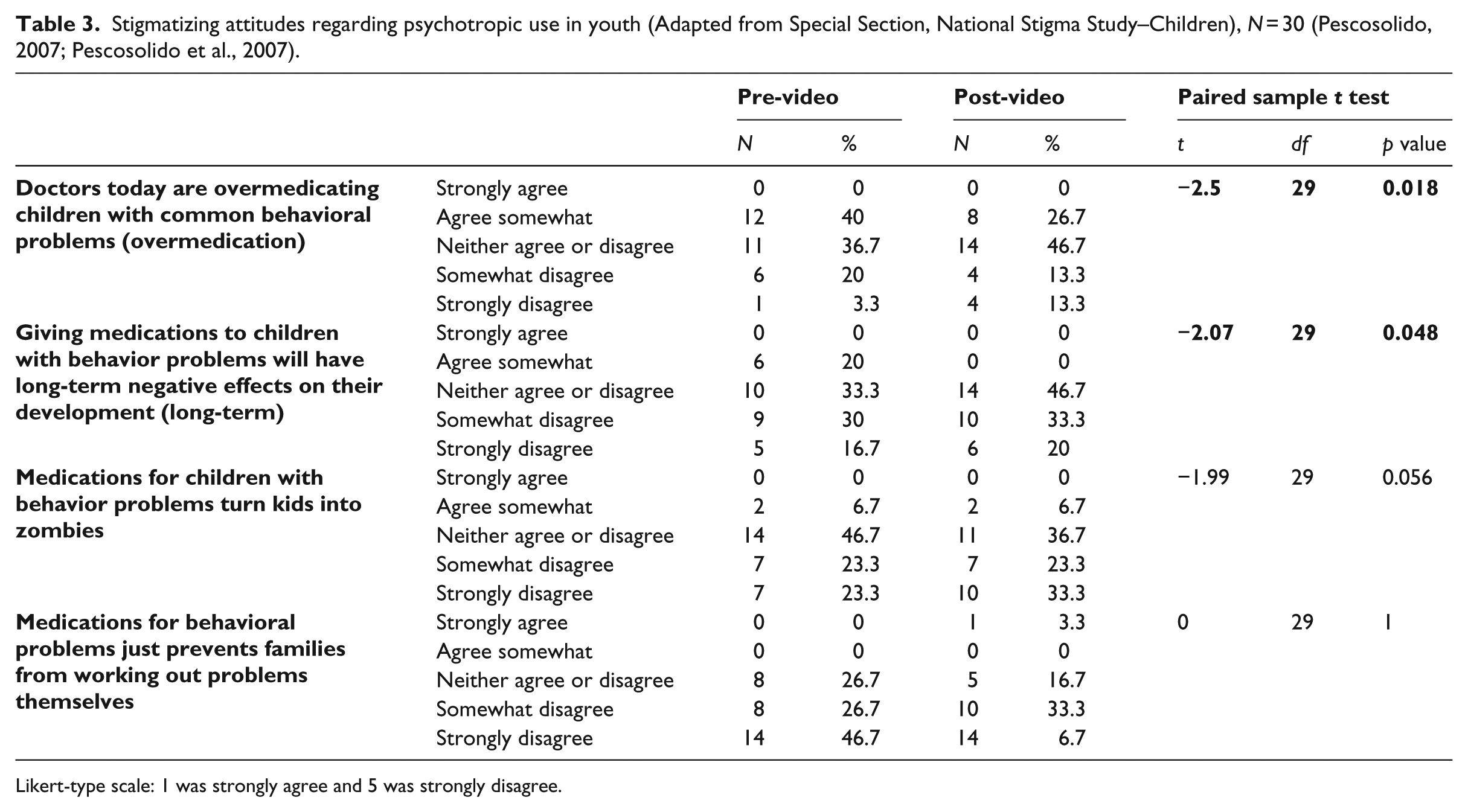
Likert-type scale: 1 was strongly agree and 5 was strongly disagree.
Discussion
This pilot study aimed to assess caregiver stigma relating to pediatric mental health and the Pediatric C/L Psychiatry service among caregivers of youth with medical and potential psychiatric comorbidities previously served by a large academic pediatric medical hospital. The study explored the use of a brief educational video, including caregiver and provider informed content, to address caregiver mental health stigma, a significant factor in accessing and engaging potentially necessary mental health services in the medical setting. The study demonstrated that the use of a brief educational video could significantly impact caregiver attitudes and stigma regarding pediatric mental health care. These findings suggest the use of a brief educational video is a promising intervention to reduce caregiver stigma toward mental health services in a high-risk pediatric population and therefore impact a key barrier to accessing consultative mental health services in the inpatient medical setting. In addition, the use of an education video enhances awareness of C/L psychiatric services when knowledge and awareness is not readily present on pediatric medical admission. This is the first study to explore the issue of mental health stigma in inpatient pediatric care settings and the first study to measure how a brief educational intervention can impact stigma, awareness, and access to psychiatric consultation in caregivers of medically ill youth.
This study has many similarities, and a few notable differences, to the few existing national studies exploring caregiver stigma toward pediatric mental health care. Existing national studies on mental health stigma have not been conducted on inpatient pediatric units and therefore direct comparison is limited. The NSS-C examined parental beliefs and attitudes toward pediatric mental health care (Pescosolido, 2007; Pescosolido et al., 2007). Compared to the NSS-C study, this study demonstrated lower stigma ratings at baseline for the study population. For example, in this study only 10% of respondents agreed that pursuing mental health treatment would “make a child an outsider at school.” In the NSS-C study, nearly half of respondents agreed with this statement (Pescosolido et al., 2007). This trend was also observed in response to confidentiality and the belief that psychotropics were an impediment to solving behavioral problems non-pharmacologically (Pescosolido et al., 2007). Other findings in this study were in line with the NSS-C study. The Parental Attitudes Toward Psychological Services Inventory (PATPSI) study showed that parents with previous experience with child mental health services have less stigma and more positive attitudes toward child mental health services than those with no previous experience (Turner, 2012). As over 75% caregivers in this study had previous experience with child mental health services, this could account for some of the differences noted with the NSS-C (Turner, 2012).
The issue of stigma is particularly important in consultative mental health services within pediatric medical settings as the youth served are at greater risk of psychopathology and are less likely to seek sustained mental health services compared to the general population (Bardach et al., 2014). The risk of psychopathology in youth with acute medical illness is related to the distress and discomfort of physical disease, disruptions to daily routine and functionality, and the bidirectional relationship between physical disease and psychiatric disease, namely depression and anxiety (Maneta & DeMaso, 2017). Pediatric C/L Psychiatry can facilitate access to needed mental health services in a less stigmatizing fashion (Bardach et al., 2014).
Although stigma serves as a significant barrier to psychiatric consultation, the need for pediatric psychiatry consultation continues to rise rapidly (Shaw, Pao, Holland, & DeMaso, 2016). Pediatric C/L Psychiatry has the unique role of providing mental health consultation to youth who have not accessed mental health due to a variety of reasons including avoidance, past negative experiences, and stigma. A psychiatric consultation can dramatically impact the emotional, cognitive, functional, and physical well-being of youth and significantly improve quality of life and both psychiatric and medical outcomes (Hall & Frankel, 1996; Merikangas et al., 2010). Not only does engaging Pediatric C/L Psychiatry reduce distress and offer an opportunity to dispel misconception but also consulting psychiatry 10% sooner can reduce hospital length of stay, as well as cost, by 7.9% each (Bujoreanu et al., 2015). Therefore, family engagement with Pediatric C/L Psychiatry services may have far-reaching immediate and downstream effects on patient and family perceptions, involvement in care, cost, and clinical outcomes. Ultimately, future study is needed to determine how stigma impacts engagement with mental health services in the inpatient pediatric setting and whether addressing stigma prior to psychiatry consultation has direct effects on clinical outcomes or cost.
This important opportunity for engaging mental health services highlights the critical importance of addressing caregiver stigma as a barrier to accessing Pediatric C/L Psychiatry services. This study highlights a low-cost and well-accepted intervention that has the potential to reduce stigma and misconceptions regarding pediatric mental health. This, in turn, can potentially obviate one of the biggest barriers to accessing and engaging mental health services in the pediatric hospital setting. Establishing a positive perception and interaction with Pediatric C/L Psychiatry early can foster a better understanding and experience with pediatric mental health services. Future study is needed to understand the durability of the study findings and whether use of a brief educational video results in tangible increased use of mental health services, both in the acute inpatient setting and beyond the inpatient setting. Furthermore, further investigation is needed to look at other modalities of addressing stigma that are well accepted, feasible, and can be provided longitudinally.
Limitations
There were several limitations to this study that are important to consider. Given that no previous studies have explored the level of stigma toward mental health consultation in inpatient pediatric settings, there are no pre-existing data to determine how prevalent and pervasive stigma may be in this setting compared to other settings. The high level of stigma was extrapolated from studies of traditional outpatient and inpatient psychiatric settings and primary care settings, and it is unclear if this same level of stigma exists in inpatient pediatric settings. On the one hand, the inpatient setting may be more conducive to mental health engagement due to the consolidation of services and acuity of need. However, most patients and families admitted to inpatient medical settings may be focused primarily on medical need and may not be mentally or emotionally prepared to be asked to have their child seek a mental health provider as that is not a common expectation on admission to an inpatient pediatric setting. In the future study of psychoeducation regarding C/L psychiatric services in inpatient pediatric settings, a more appropriate first step would have been to administer a survey to a representative group of caregivers on inpatient pediatric care settings to obtain baseline perceptions and attitudes to inform interpretation of post-intervention responses to an educational video.
The study population was a convenience sample of caregivers, namely all parents, who had a previously medically hospitalized child. This limits the generalizability of our findings to the active clinical setting, where caregivers may have stronger emotions and thoughts regarding the care of their child that may impact stigma and perception of utilization of Pediatric C/L Psychiatry service. The caregivers completing the survey, by virtue of being members of a committee focused on patient/family-centered care and its volunteer nature, are likely not representative of the typical caregiver whose child is hospitalized in an inpatient medical setting. It is more likely that caregivers involved in such a committee have less stigma and more awareness of C/L psychiatric services. However, the fact that viewing the educational video changed their perceptions and attitudes about C/L psychiatric service is encouraging given these limitations and further supports a broader study of the psychoeducational intervention. A natural next step would be to pursue a similar study design for caregivers whose children are actively medically admitted. However, this was challenging in this unfunded pilot study where a dedicated team was not available to implement the study. Study implementation by the consultation service was both not feasible and would introduce bias.
The study sample size was also small and fairly homogeneous, again limiting generalizability. Half of the caregivers identified that their children had been seen by psychiatry in the past, and over three-fourths had participated in some form of psychotherapy indicating that many participating families were already familiar with some type of mental health care. The majority of patients identified in the study were seen for anxiety (23.3%) or depression (13.3%), which is comparable to lifetime rates of anxiety (31.9 %) and depression (11.8%) in adolescents (Merikangas et al., 2010). Despite this, there were no differences in the responses between those previously exposed to mental health services and those that were naïve to mental health services, but our sample size was likely too small to identify a significant difference. Respondents were also predominantly female and Caucasian, which is similar to the hospital caregiver population served in the hospital and may limit generalizability in males and in ethnically diverse populations.
The video itself was constructed without dedicated funding or professional video editing. Video production quality was noted to be the biggest concern when eliciting feedback from caregivers. The intent is to take these pilot study findings and pursue funding to develop a professionally designed and edited video with the necessary components and feedback from caregivers and other health professionals gathered in this study. It is unclear from this study whether the effects of the video are durable and whether repeated viewing has an additive impact on stigma over time. This study did not explore operationalization of the video in the busy inpatient medical setting. This would be important to consider as to the practical dissemination of the video and how this could influence caregiver stigma. At this institution, there are a series of educational videos for families included in a “Get Well Network” that nurses, staff, and physicians can access and offer to families. The goal would be to include an educational video on Pediatric C/L Psychiatry as part of this video series and have it readily accessible to show prior to Pediatric C/L Psychiatry consultation. Inclusion of a psychoeducational video on C/L psychiatric services, along with other health-related educational videos, further destigmatizes mental health and normalizes discussions relating to child and adolescent mental health needs in the inpatient pediatric setting.
Direct comparison between this study and the NSS-C study is challenging due to this study’s option of a neutral response. Future studies should eliminate the option of a neutral response and require respondents to take a non-neutral stance on statements provided to replicate the NSS-C study. Furthermore, this study’s sample size was significantly smaller and less diverse as compared to the more ethnically diverse and gender-balanced NSS-C study (41% male vs. 10% in this study) (Pescosolido et al., 2007). This is an important consideration since ethnically diverse populations and males both tend to have higher rates of stigmatization against pediatric mental health care compared to Caucasian females (Pescosolido et al., 2007). In addition, participants’ involvement in the PFCC, which is designed to improve patient safety, quality, and care, including mental health care, may have fewer stigmatizing attitudes at baseline. In the future, it would be helpful to capture a larger sample of respondents and potentially sample respondents whose children were actively hospitalized at the time before consultation rather than assessing stigma retrospectively.
Conclusion
Caregiver stigma regarding pediatric mental health care is a significant barrier to accessing needed mental health services for youth and continues to be a challenging topic that has been minimally studied. Pediatric C/L Psychiatry is an important service that can have a significant impact on physical and mental health, cost, and clinical outcomes. Pediatric C/L Psychiatry provides service to a particularly vulnerable population with complex medical and psychiatric comorbidities and offers a unique opportunity to address caregiver mental health stigma. In this study, we demonstrate that the use of a brief educational video introducing the Pediatric C/L Psychiatry service and addressing common mental health misconceptions can have a tangible effect in improving caregiver attitudes regarding pediatric mental health. It can also reduce caregiver stigma regarding pediatric mental health and psychotropic use. The use of such a video represents a potentially feasible, sustainable, time-sensitive, and promising intervention that may reduce caregiver stigma and therefore reduce a critical barrier to accessing Pediatric C/L Psychiatry services in an inpatient pediatric care setting.
Footnotes
Acknowledgements
The authors listed above have contributed to the conceptualization and design of the study, collection of data, data analysis, writing of the manuscript, and editing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.