
Abstract
Accumulating evidence indicates that psychological and neurophysiological processes interconnect and interact to activate the body’s stress system and to trigger and maintain functional somatic symptoms. This study used the Early Life Stress Questionnaire, Depression Anxiety Stress Scales and biological markers (heart rate, heart rate variability, skin conductance, C-reactive protein (CRP) titre, respiratory rate, and accuracy and reaction time in an emotion-face identification task), to examine childhood adversity, psychological distress and stress-system activation in 35 children and adolescents (23 girls and 12 boys, 9–17 years old) disabled by chronic pain (vs two groups of age- and sex-matched healthy controls). Patients reported more early-life stress (U = 798.5, p = .026) and more psychological distress (U = 978, p < .001). They showed activation of the autonomic system: elevated heart rate (U = 862.5, p = .003), elevated electrodermal activity (U = 804.5, p = .024) and lower heart rate variability in the time domain (U = 380.5, p = .007) and frequency domain (U = 409.5, p = .017). The group showed an upward shift of CRP titres (with 75th and 90th CRP percentiles of 4.5 and 10.5 mg/L, respectively), suggesting the activation of the immune–inflammatory system. Elevated CRP titres were associated with elevated heart rate (p = .028). There were no differences in respiratory rate or in accuracy and reaction time in the emotion-face identification task. The results indicate that interventions for children and adolescents with chronic pain need a multidisciplinary mind–body approach that concurrently addresses psychological distress, physical impairment and stress-system dysregulation.
Introduction
Accumulating evidence suggests that functional somatic symptoms emerge when there is hyperactivation, hypoactivation or dysregulation within the brain–body stress system – the hypothalamic–pituitary–adrenal (HPA) axis, autonomic nervous system, immune–inflammatory system and brain regions involved in arousal and emotion processing (Kozlowska, 2017; Pervanidou & Chrousos, 2018; Pick, Goldstein, Perez, & Nicholson, 2018; Vachon-Presseau et al., 2016). Chronic pain 1 is a common condition in childhood which is often accompanied by anxiety and depression (Zernikow et al., 2012). For a small subgroup, the pain is disabling and requires intensive multimodal inpatient rehabilitation (Friedrichsdorf et al., 2016; Hechler, Dobe, & Zernikow, 2010). At our hospital, this disabled group of children and adolescents is offered inpatient treatment in our multimodal inpatient rehabilitation programme, commonly known as the Mind–Body Program (Kozlowska, 2017). Within the Mind–Body Program, the clinical team use the Stress-System Model of Functional Somatic Symptoms (Kozlowska, English, Savage & Chudleigh, 2012) to inform treatment (see Figure 1). This model builds upon the work of the team’s research programme with children with functional neurological symptom disorder (FND) – where pain is comorbid in about half of the cases – the most frequent users of the Mind–Body Program. What we have found is that those children generally present for treatment in a brain–body state of increased arousal, with activation across multiple components of the stress system (Kozlowska, 2017). Accordingly, many of the programme’s treatment interventions focus on helping our patients downregulate their arousal and state of motor activation, thereby shifting the stress system towards a healthier, more regulated brain–body state that facilitates a return to health (Kozlowska, 2017). In this study, we investigate the pattern of stress-system dysregulation in children with chronic pain. We compare a group of children and adolescents with chronic pain against age- and sex-matched controls, and use biomarkers to examine stress-system function. The study will help inform the choice of multidisciplinary interventions needed to address the specific areas of dysfunction seen in children and adolescents with chronic pain. In this article, the terms child and children are used inclusively for both children and adolescents.
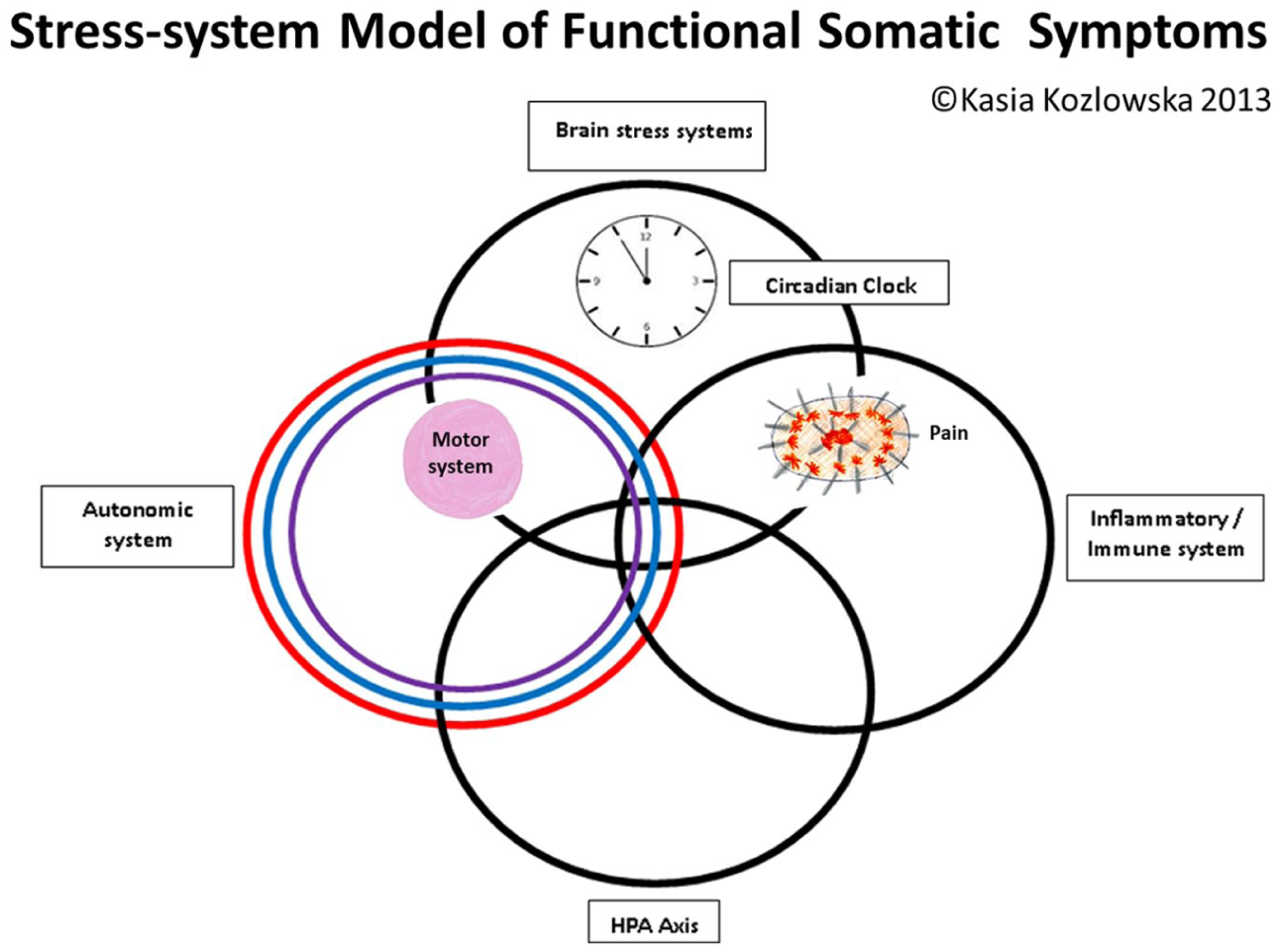
Circles metaphor of the stress system. The overlap between the different components of the stress system – the HPA axis, the autonomic nervous system, the immune inflammatory system and the brain stress systems – is presented by the overlap between the circles. The motor system, which includes central and peripheral components, is represented by the pink ball. The placement of the pink ball in the overlap between brain arousal systems and the autonomic system reflects that the activation of these systems can be accompanied by changes in motor function. For example, increases in autonomic arousal may be accompanied in the activation of the respiratory motor system (an increase in respiratory rate). The pain system, which also includes central and peripheral components, is represented by the spiky oval. The placement of pain in the overlap between brain arousal systems and the immune–inflammatory system reflects that the activation of these systems maintains chronic pain.
Data about stress-system dysregulation in children with chronic pain are slowly emerging. Researchers have used measures of salivary cortisol to assess the HPA function. A prospective study of 2230 Dutch adolescents – the TRAILS (Tracking Adolescents’ Individual Lives Survey) study – showed that adolescents within the headache and gastrointestinal symptom cluster had low cortisol levels during stress exposure (a social stress task), and adolescents within the overtiredness, dizziness and musculoskeletal pain symptom cluster had low cortisol levels after awakening in the morning (Janssens et al., 2012). Along the same lines, many – but not all – small studies of children with functional abdominal pain also showed HPA axis dysregulation (Gulewitsch et al., 2017).
Researchers have used measures of C-reactive protein (CRP), a nonspecific systemic marker of inflammation, to assess activation of the immune–inflammatory system. In the TRAILS study, adolescents with functional somatic symptoms had higher CRP levels than their healthy counterparts – a finding that was stronger in adolescents within the headache and gastrointestinal symptom cluster (Jonker, Schoevers, Klein, & Rosmalen, 2017).
Researchers have used measures of heart function – heart rate (HR) and heart rate variability (HRV) – derived from the electrocardiogram (ECG) to assess autonomic system function. Elevated HR is a biomarker of autonomic system activation (withdrawal of the restorative component of the vagal nerve, part of the parasympathetic system ± sympathetic activation). 2 High HRV – the constant change in HR from one beat to the next – is a biomarker of the activity of the restorative component of the vagal nerve. High HRV is associated with better physical and mental health (Grippo, 2017). Evans et al. (2013) found that children with chronic pain had lower HRV than healthy controls and that the children were unable to further lower their HRV during an acute experimental pain task, meaning that their autonomic systems had lost their capacity to respond to further stress (Evans et al., 2013). In another study – a follow-up, 8 years after initial presentation, of children with functional abdominal pain – Walker et al. (2017) showed that young women with ongoing pain, as well young men with ongoing pain or in remission, showed lower HRV than pain-free, healthy controls (Walker et al., 2017). In a study looking at pain responses in children with chronic pain, Tsao, Evans, Seidman and Zeltzer (2012) showed that children with chronic pain exhibited a trend towards higher baseline and post-session HR than controls (elevated HR reflects lower vagal activity and greater activation of the sympathetic system). In clinical practice, clinicians have begun to use HRV biofeedback as both a pain management strategy and an arousal regulation strategy with children with chronic pain (Chudleigh et al., 2019; Yetwin, Marks, Bell, & Gold, 2012).
Researchers have used functional imaging to look at the pattern of activation in brain regions involved in arousal and emotion processing. Whereas the adult research literature is substantial (Vachon-Presseau et al., 2016), data from studies with children are only now beginning to emerge. In a study of chronic pain patients (children with chronic regional pain syndrome (CRPS)) before and after rehabilitation treatment, Simons et al. (2014) used resting-state functional magnetic resonance imaging (fMRI) to look at functional connectivity between the amygdala (an arousal and emotion processing region) and cortical and subcortical regions (Simons et al., 2014). In comparison to healthy controls, patients initially showed enhanced functional connectivity from the left amygdala to multiple cortical, subcortical and cerebellar regions. Following multimodal rehabilitation, the patients showed dampened hyperconnectivity from the left amygdala to the motor cortex, parietal lobe and cingulate cortex. The study also showed that, prior to rehabilitation, patients showed enhanced functional connectivity to several regions key to fear circuitry (prefrontal cortex, bilateral middle temporal lobe, bilateral cingulate, hippocampus) and that the level of connectivity correlated with higher pain-related fear scores. Following multimodal rehabilitation, there was a decrease in pain-related fear and this decrease was associated with a decreased level of connectivity between the amygdala and the motor and somatosensory cortex, cingulate and frontal areas. In another study, using fMRI during a fearful-faces paradigm, Simons (2016) showed that children with chronic pain (also CRPS in this instance), compared to healthy controls, displayed a diminished response to fearful faces in regions associated with emotion processing (in the striatum, amygdala, insula and dorsolateral prefrontal cortex) (Simons et al., 2016). They also found an association between increased pain-related fear levels and decreased activity in a number of brain regions (right amygdala, insula, putamen and caudate). Interestingly, they found no difference in self-reported emotional valence and arousal between the two groups. These data highlight that engagement and activation of brain regions involved in arousal and emotion processing – the brain component of the stress system – are important in the neurobiology of chronic pain.
Finally, another body of work has used proxy measures of brain function – measures of reaction time, attention or somatosensory evoked potentials – to look at brain function during pain-related tasks or to examine differences between children with chronic pain and control groups on a range of standardized tasks. The outcome from this body work is inconclusive. For example, one study – using a dot-probe paradigm – found that children with chronic pain (vs children with eating disorders) had overall slower reaction times to correctly identify angry, sad and neutral faces (Hughes-Scalise & Connell, 2014). An earlier study – using the emotion-identification task (as used in this study) – found no significant differences between underweight adolescents with an eating disorder and healthy controls in emotion-identification accuracy or in the reaction time for correctly or incorrectly identified emotions (Hatch et al., 2009). Because the studies used different tasks, it is not possible to infer that children with pain have slower reaction times to emotion faces. A recent review of studies examining attention biases showed that healthy children without chronic pain do not show interpretation or attention biases towards pain-related stimuli, and found only weak evidence for the presence of attention biases, characterized by vigilance towards pain-related stimuli, and of pain-related interpretation biases in children with chronic pain (vs those without) (Brookes, Sharpe, & Kozlowska, 2018).
In this study, we used self-report measures to document early-life stress and psychological distress, and biological markers – HR, HRV, electrodermal activity (EDA) amplitude, CRP titres, respiratory rate (RR) and face recognition reaction times – to examine whether children disabled by chronic pain, versus healthy controls, display differences in function within the autonomic nervous system, immune–inflammatory system, respiratory motor system and brain systems underlying vigilance and motor readiness. We hypothesized that the patients would report more adverse life events, experience more psychological distress and show activation of the autonomic system (increased arousal reflected in increased HR, lower HRV and increased EDA amplitude) and activation of the immune–inflammatory system (a shift towards a proinflammatory state, as reflected by CRP median percentiles). We also investigated whether increases in arousal were accompanied by the activation of the motor respiratory system (increased respiration rate in the resting-state condition) and increases in vigilance and motor readiness to emotion faces (face recognition reaction times).
Methods
Participants
A total of 35 patients (23 girls and 12 boys) aged 9–17 years with chronic pain and significant functional impairment were recruited (October 2010 and January 2014) from consecutive referrals to the mind–body multimodal inpatient rehabilitation programme for children and adolescents with functional somatic symptoms at our tertiary care hospital. All patients had been fully examined and investigated, including blood work, by one or more paediatricians, who had made the diagnosis of chronic pain. Potential participants were excluded if they had a developmental disability or if medical perpetuating factors for their pain had not been appropriately investigated or treated. Five families declined participation. Because most children with chronic pain presenting to the hospital are treated via the outpatient Pain Clinic or via the day programme run by the Pain Clinic, the number referred to the Mind–Body Program is small.
Two healthy control groups of 35 participants each – matched on age, sex and body mass index (BMI) to the pain group – were recruited from the Brain Resource International Database (BRID; Gordon, 2003). Control group A had completed the study protocol with the exception of the EDA component, and control group B had completed the study protocol with the exception of the facial emotion-identification task. Controls were excluded if they had a current or previously diagnosed mental disorder as per Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2000) or if they had an immediate family member with a current or previously diagnosed mental disorder. Other exclusion criteria for controls included the diagnosis of a chronic medical illness (including any severe physical impairment), a history of previous brain injury or head injury causing loss of consciousness within the last 5 years or insufficient English proficiency to understand the consent process and laboratory study. Because inclusion as a healthy control required that the child be doing well, all controls had Global Assessment of Functioning (GAF) scores of ⩾80 (doing alright or doing well). Two control groups were used because we were unable to source a cohort from the BRID who had completed exactly the same combination of tasks as our chronic pain cohort.
Ethical approval for this study was granted by the Sydney Children’s Hospitals Network Human Research Ethics Committee. Participants and their guardians provided written informed consent in accordance with National Health and Medical Research Council guidelines.
Procedure
Children with chronic pain – and their families – were provided information about the study and invited to participate after they had completed routine psychiatric family assessments that confirmed the diagnosis of chronic pain, using DSM-IV-TR criteria for Pain Disorder.
Demographic information and clinical characteristics of the pain group were collected during the routine psychiatric assessment and using self- and clinician-reported measures. Information collected during the psychiatric assessment included the number and location of pain sites, other somatic symptoms, family history of mental disorder and the child’s story of the symptoms, including antecedent stressors. Children with chronic pain also rated the average and maximal intensities of their pain – in the previous week – at assessment using the visual Likert-type scale (0–10). Following the clinical assessment, and to document the child’s global level of function, clinicians completed the Royal Alexandra Hospital for Children Global Assessment of Function, the DSM-IV-TR (American Psychiatric Association, 2000) GAF was modified to account for impairment from chronic pain, FND or other chronic illness.
All children with chronic pain underwent laboratory assessments, which took place during their inpatient rehabilitation admissions, at which point they were experiencing significant levels of pain. At the laboratory, an ECG yielded measures of HR, HRV and RR, and an EDA measure of peak amplitude was acquired while the child was sitting quietly with eyes open (for details regarding methodology, see (Kozlowska et al., 2015)). Participants also participated in the facial emotion-identification task, a well-established emotion-faces paradigm in neuroscience research (Gur et al., 2002; Kozlowska, Brown, Palmer, & Williams, 2013; Palmer, 2009). They were shown a series of 48 standardized faces displaying basic expressions of emotion: happiness, fear, sadness, anger, disgust and a neutral expression presented for 2 seconds (2000 ms). Using a touch-screen computer, they were required to select the label corresponding to the emotion displayed out of the six available options, with standardized instructions emphasizing the importance of both speed (reaction time) and accuracy (correct identification).
At the end of the laboratory assessment, children with chronic pain completed the Depression Anxiety and Stress Scales (DASS), which are a validated measure of perceived stress in paediatric populations (Lovibond & Lovibond, 1995; Patrick, Dyck, & Bramston, 2010) and the Early Life Stress Questionnaire (ELSQ), a checklist of 19 stress items – and an option for elaboration – based on the Child Abuse and Trauma Scale (Cohen et al., 2006). Of the 19 items, 12 pertained to relational stressors, including bullying, physical abuse, sexual abuse, emotional abuse, neglect, parental separation, loss by separation, loss by death, family conflict, severe illness of a family member, domestic violence and other. Additional items pertain to birth complications, life-threatening/severe illness, war trauma and natural disasters. Participants record if they have or have not experienced the given stressor and, if so, the age period during which the stressor has been experienced.
CRP titres (a nonspecific marker of inflammation) and white blood cell count (WCC; a marker of infection) were included if the blood panel testing had been performed through our hospital laboratory. Serum CRP was measured by a commercial reflectance spectrometry enzyme-linked immunoassay (Ortho-Clinical Diagnostics, Rochester, NY), which utilizes a monoclonal mouse anti-CRP antibody conjugated to horseradish peroxidase. The sensitivity of the assay (limit of blank) is 2.03 mg/L, equivalent to the concentration above which CRP may reliably be ascertained to be present in the sample. The assay has a coefficient of variation of 12% at a concentration of 7.3 mg/L. A CRP reference interval of ⩾10 mg/L is reported by the laboratory as indicating inflammation or infection. The WCC calculations were performed using a Beckman Coulter UniCel DxH 800 cell counter.
All healthy controls attended the laboratory assessment and completed the same battery of laboratory tests, with the exception of the EDA measure (control group A) and the face recognition task (control group B). None of the controls provided blood samples.
Measures and data analysis
HR was measured in beats per minute. HRV indices of the vagal activity were measured in two different ways: using the time-domain measure of HRV, RMSSD (root mean squared successive differences of the interbeat intervals measured in ms2 (RMSSD-HRV)), and using the frequency-domain measure of HRV (high-frequency power measured in Hz (HFP-HRV)). The EDA measure of sympathetic activity was measured from the peak amplitude of the increase in skin conductance in microsiemens (μs). RRs were reported as breaths per minute. Reaction times to emotion faces were measured in milliseconds. Accuracy was measured as the percentage of correctly identified emotion faces.
Before all analyses, outliers beyond 2.5 SDs were removed from the lab-acquired data, and all missing values (8% for the pain group, 5% for control group A and 8% for control group B) were replaced with the mean, determined separately for children younger than 12 years and children 12 years or older (Palmer, 2009). For the blood panel data (for pain subjects only), CRP titres were missing for seven children and WCCs for four; missing values were not replaced.
Data analysis included examination of demographic characteristics of the pain group versus control groups A and B; face recognition reaction times (and accuracy) of the pain group versus control group A; and autonomic data and RR of the pain group versus control group B. Student’s t-tests were used to compare groups on variables when test assumptions were satisfied. When assumptions were violated (such as normal distribution), the nonparametric Mann–Whitney U test was used instead. Two-way 2 (group: pain or control) × 6 (emotion: happy, sad, fear, anger, disgust, neutral) mixed analyses of variance (ANOVAs) with repeated measures for emotion (accuracy and reaction time) were performed. Due to CRP data being censored below 2 mg/L, Tobit censored regression models 3 were used to assess whether CRP levels were associated with any demographic or clinical measures (Austin, Escobar, & Kopec, 2000). Pearson and Spearman correlations were used to examine the pattern of relationship between self-reported measures and relevant biomarkers of stress-system activation in the pain cohort.
Normal reference ranges were used to consider BMI percentiles, CRP titres and WCCs. For comparative reference ranges for BMI percentiles, we used data from Centers for Disease Control and Prevention. BMI percentile cutoffs were as follows: underweight (<5), healthy (5 to <85), overweight (85 to <95) and obese (⩾95) (Centers for Disease Control and Prevention, n.d.). For comparative reference ranges for the CRP data, we used published data from the TRAILS study, with its 2230 16-year-old adolescents (Jonker, Rosmalen, & Schoevers, 2017) and a cohort of 468 healthy young adult volunteer blood donors (Shine, de Beer, & Pepys, 1981). The adult study had shown that, in healthy young adults, the median concentration of CRP was 0.8 mg/L, the 90th percentile was 3.0 mg/L and the 99th percentile was 10 mg/L, indicating that values > 10 mg/L were strongly suggestive of a pathological process. The TRAILS study had shown a similar pattern of findings: the median concentration of CRP was 0.4 mg/L, the 25th percentile was 0.2 mg/L, the 75th percentile was 1.0 mg/L and the 90th percentile was 3.13 mg/L. In our hospital, the clinical cutoff of >10 mg/L is used by clinicians in day-to-day clinical practice to signal potential systemic inflammation. WCCs were deemed to be elevated if they exceeded the normal clinical WCC range (4.5–13.5 × 109/L) used by clinicians in the hospital.
Results
The study involved 35 patients (23 girls and 12 boys) aged 9.88–17.07 years (M = 13.60, SD = 2.09) experiencing chronic pain with significant functional impairment and two control groups of 35 age-, sex- and BMI-matched controls (control group A: age range = 9.83–17.84, M = 12.91, SD = 2.05 and control group B: age range = 9.16–17.11, M = 13.10, SD = 2.18). Referrals to the programme came from general paediatrics (40%), the neurology department (29%), the chronic pain clinic (20%), rheumatology (6%) and orthopaedic specialists (6%).
Clinical characteristics of children/adolescents with chronic pain
The children and adolescents with chronic pain reported high baseline intensity of pain, with a mean of 7.22 (range 4–10) and high maximal pain intensity, with a mean of 9.4 (range = 7–10) on a 10-point Likert-type scale. In total, 49% of patients (n = 17) had pain in one site, 23% (n = 8) had pain in two sites, 26% (n = 9) had pain in three sites and 3% (n = 1) had pain in four or more sites. The most common sites for pain were the head (46%, n = 16), back (26%, n = 9), abdomen (23%, n = 8), both legs (14%, n = 5) and right leg (14%, n = 5).
Levels of functional impairment were high. Mobility was impaired for almost half of the cohort, with 17% (n = 6) needing crutches to mobilize, 6% (n = 2) being restricted to a wheelchair and 17% (n = 6) effectively bedbound. And 54% (n = 19) of the cohort were unable to attend school (because of their pain), and the median length of school missed was 6 weeks (range = 1–83 weeks). GAF scores ranged from 11 to 65 (M = 38.4) indicating that the majority of children/adolescents had major impairment in several areas of functioning. With regard to BMI percentiles, patients fell across the four groups: underweight (n = 2, 6%), healthy weight (n = 18, 51%), overweight (n = 9, 26%) and obese (n = 6, 17%).
Mental disorders were strongly comorbid in the pain group. These included anxiety (51%, n = 18), depression (46%, n = 16), eating disorder (6%, n = 2), bipolar disorder (3%, n = 1) and disruptive behaviour disorder not otherwise specified (NOS; 3%, n = 1). Nonspecific somatic symptoms, which were also common in this group, included fatigue (69%, n = 24), nausea (54%, n = 19), dizziness (43%, n = 15), breathlessness (29%, n = 10) and sensation of the heart pounding (14%, n = 5).
The majority of the cohort (86%, n = 30) were prescribed psychotropic medications for comorbid anxiety or depression. In total, 63% (n = 22) were prescribed a selective serotonin reuptake inhibitor (SSRI), most commonly fluoxetine or sertraline. Medication to address sleep-phase disturbance or disrupted circadian rhythm included melatonin 3–9 mg nocte (20%, n = 7), low-dose quetiapine 6.25–12.5 mg nocte (37%, n = 13) or clonidine 25–75 µg nocte (3%, n = 1). Gabapentin was prescribed for pain having a possible neuropathic component (14%, n = 5), as was amitriptyline 25 mg nocte (3%, n = 1). On the day of laboratory testing, 80% (n = 28) of patients had taken their morning medication prior to testing: SSRIs (63%, n = 22), mirtazapine (6%, n = 2), carbamazepine (3%, n = 1) and gabapentin (14%, n = 5).
Antecedent life events and early-life stress
Antecedent stressors were commonly reported by children with chronic pain and their families at the psychiatric family assessment (range = 1–11, M = 5; see Table 1). More than half of the cohort had a medical event preceding the onset of pain, including injury or accident (37%, n = 13), medical illness (23%, n = 8) or a surgical procedure (6%, n = 2). The other most common antecedent events were family conflict, bullying and parental mental health disorder. Six children (12.5%) had a parent with a chronic pain condition. On the ELSQ, children with chronic pain (vs controls) reported an increased number of early-life stressors (see Table 2).
Antecedent life events experienced by children/adolescents with chronic pain.
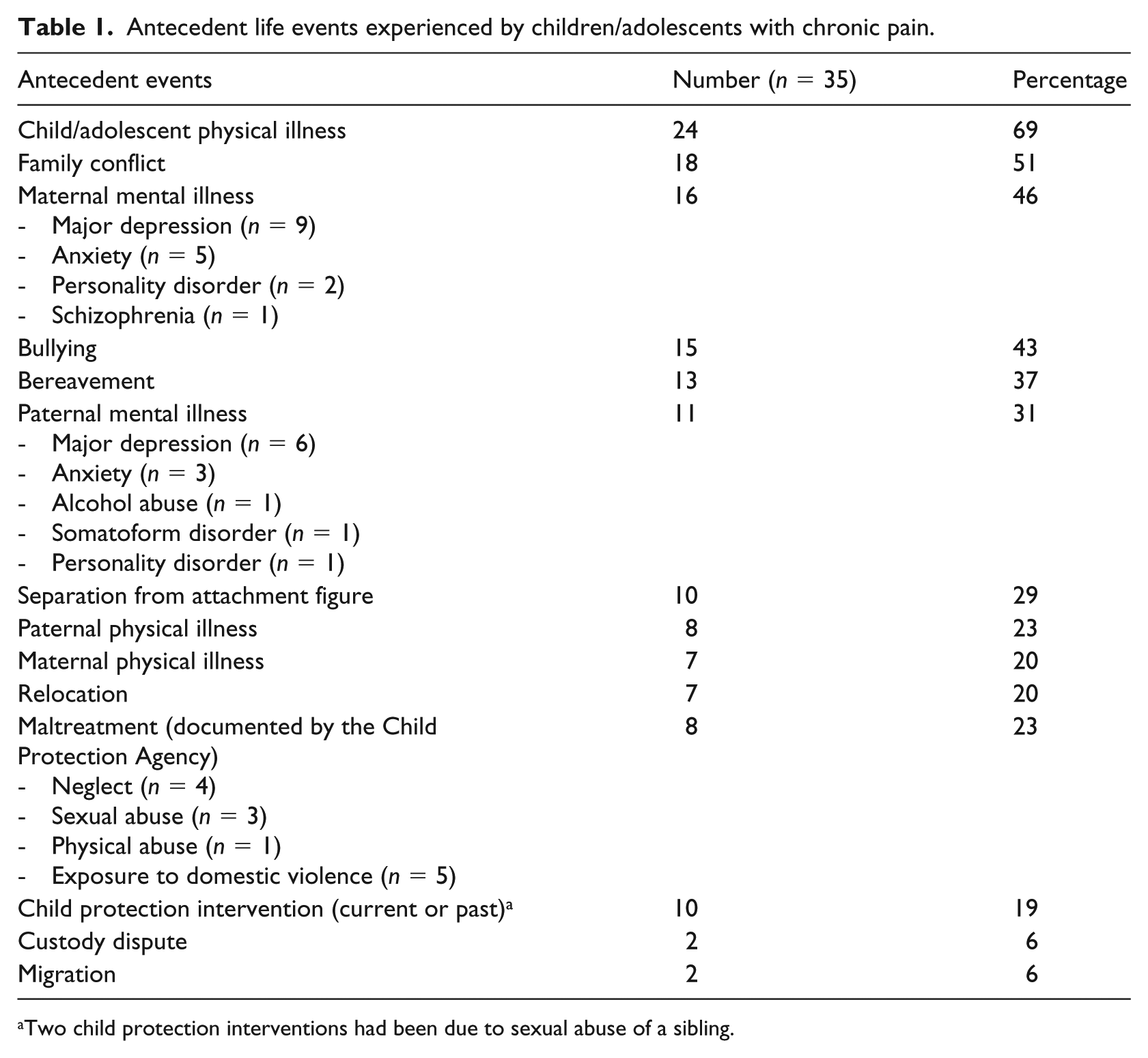
Two child protection interventions had been due to sexual abuse of a sibling.
Demographics, BMI and self-report measures in children with chronic pain and healthy controls.
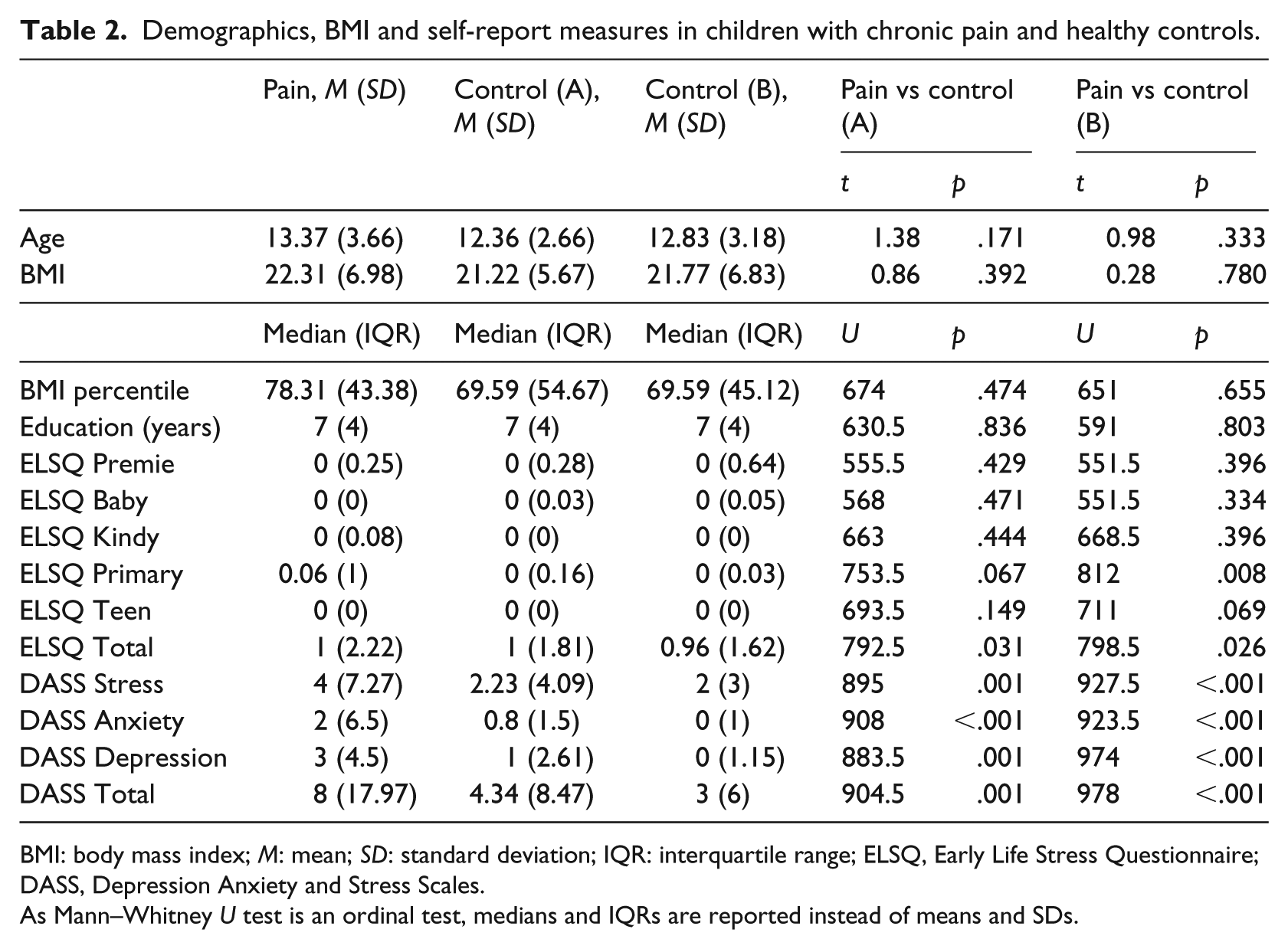
BMI: body mass index; M: mean; SD: standard deviation; IQR: interquartile range; ELSQ, Early Life Stress Questionnaire; DASS, Depression Anxiety and Stress Scales.
As Mann–Whitney U test is an ordinal test, medians and IQRs are reported instead of means and SDs.
Self-report measures of subjective depression, anxiety and distress
On the DASS, children with chronic pain (vs controls) reported higher subjective anxiety, depression and distress (see Table 2).
Biological markers of stress-system activation
Autonomic nervous system
Children with chronic pain showed increased arousal in the resting state as evidenced by cardiac and EDA measures of autonomic function – increased HR, decreased RMSSD-HRV, decreased HFP-HRV and increased EDA amplitude (see Table 3).
Differences in autonomic system measures and respiratory rate during eyes-open resting state.
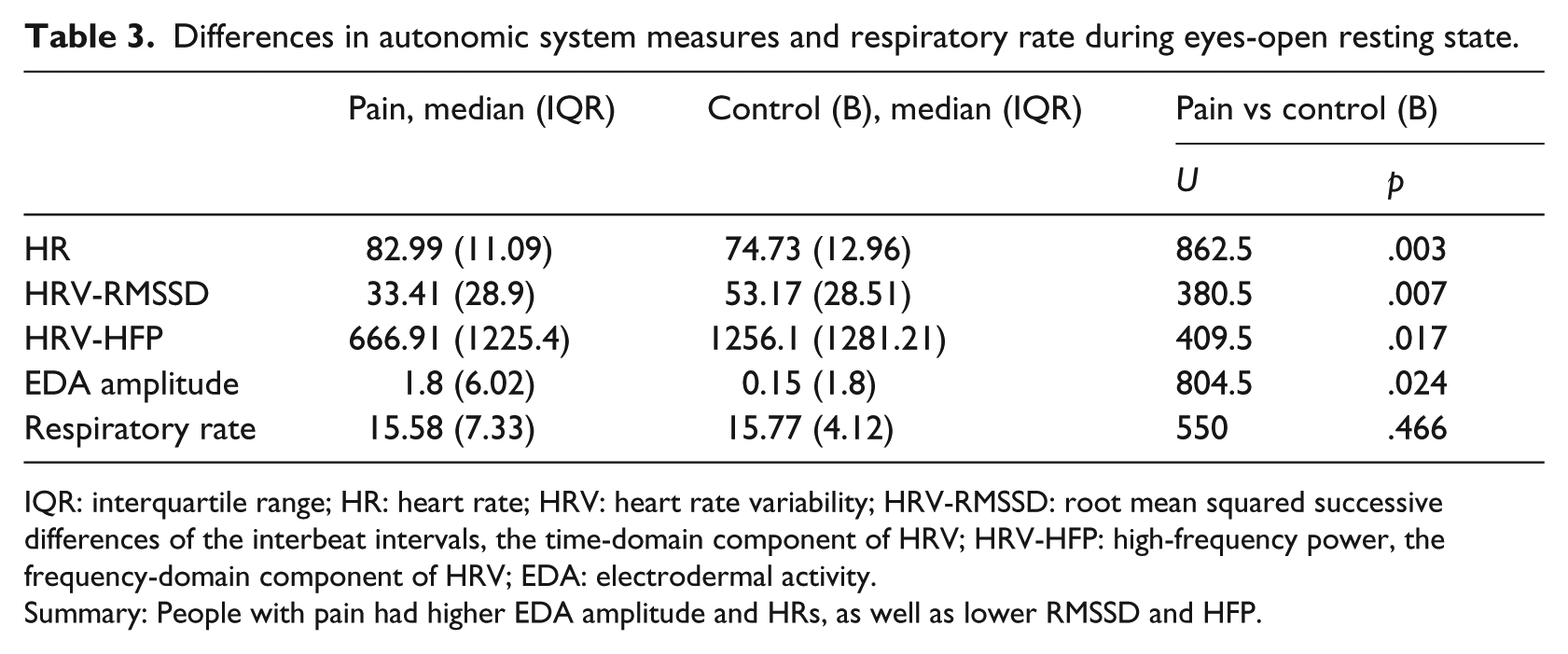
IQR: interquartile range; HR: heart rate; HRV: heart rate variability; HRV-RMSSD: root mean squared successive differences of the interbeat intervals, the time-domain component of HRV; HRV-HFP: high-frequency power, the frequency-domain component of HRV; EDA: electrodermal activity.
Summary: People with pain had higher EDA amplitude and HRs, as well as lower RMSSD and HFP.
Immune–inflammatory system
In the 28 children with CRP titres, the distribution of CRP titres – as indicated by the 75th and 90th percentiles – was higher than the reference ranges reported previously in a Dutch population sample of 16-year-old adolescents and a UK sample of healthy young adult blood donors (see Figure 2; Jonker, Schoevers, et al., 2017; Shine et al., 1981). In total, 29% (n = 8/28) of children had elevated CRP titres (⩾2 mg/L) and the remainder (n = 20/28) had normative titres (<2 mg/L; see Table 4). With the exception of one patient (2.9%) who had an elevated WCC of 20.5 × 109/L, all other WCCs fell within the normative reference range.
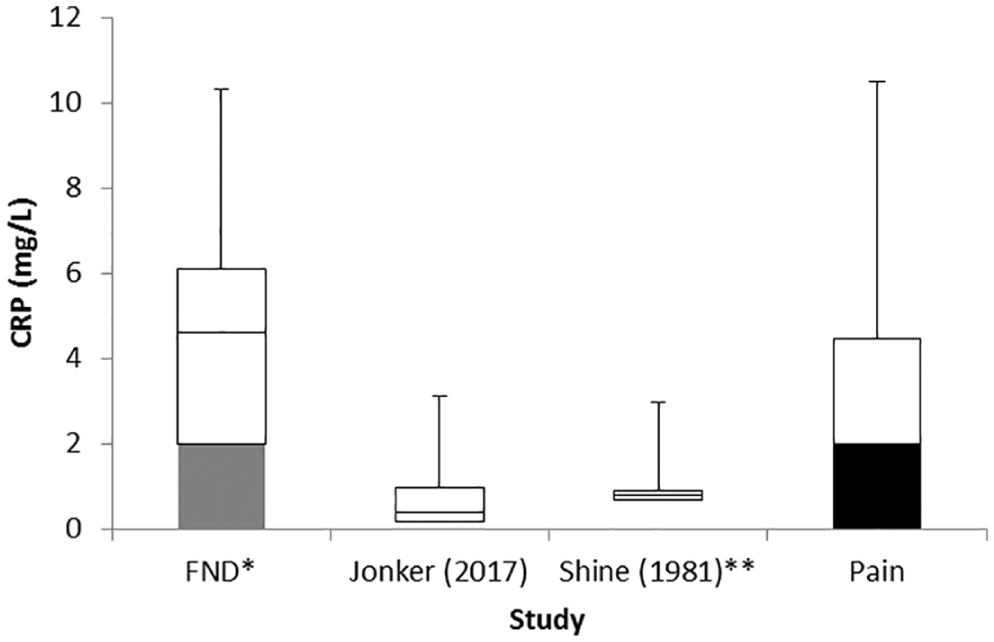
Comparison of CRP distribution with previous studies. Box indicates the 25th, median and 75th centiles. Upper whiskers indicate the 90th centile. The median for the pain cohort from this study is somewhere in the <2 range, but the 75th and 90th centiles are much higher than for the Jonker and Shine healthy cohorts (Jonker, Rosmalen, & Schoevers, 2017; Shine et al., 1981).
Distribution of CRP titres in the 19 children with pain with CRP data.
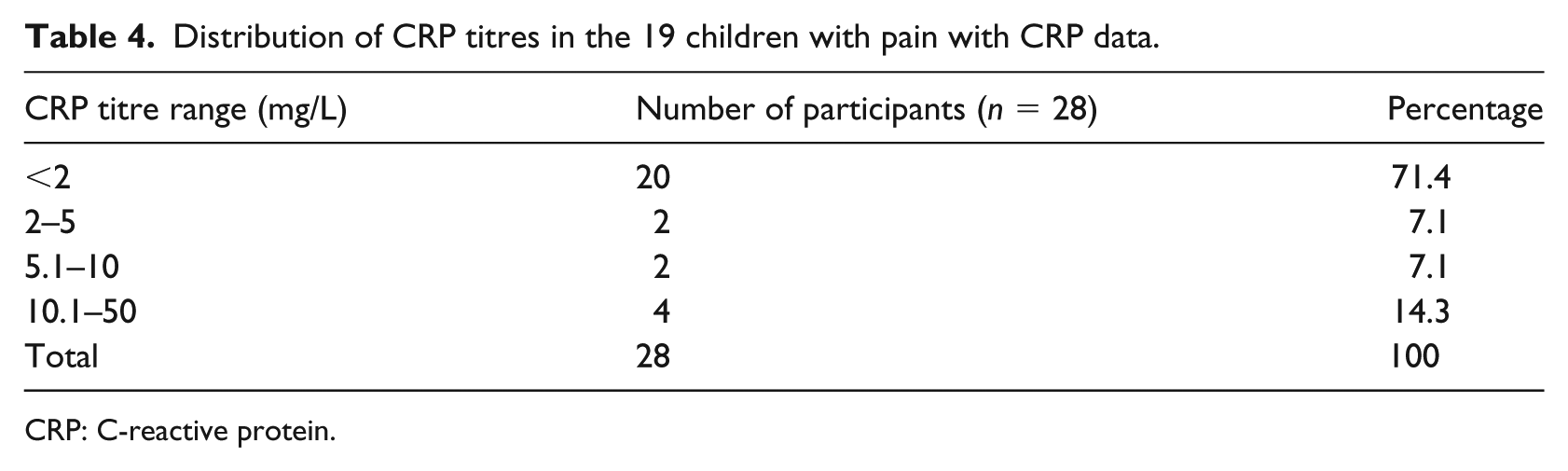
CRP: C-reactive protein.
The Tobit analysis confirmed that elevated CRP titres were not explained by BMI percentile, antecedent illness/injury or other confounding factors, and suggested that CRP titre levels were strongly associated with elevated HR (see Table 5).
Tobit regression analysis for censored data.

CI: confidence interval; BMI: body mass index; DASS: Depression Anxiety and Stress Scales; ELSQ: Early Life Stress; EDA: electrodermal activity; HR: heart rate; HRV: heart rate variability; HRV-RMSSD: root mean squared successive differences of the interbeat intervals, the time-domain component of HRV; HRV-HFP: high-frequency power, the frequency-domain component of HRV; RR: respiratory rate.
Respiratory motor system
There were no differences between children with chronic pain and controls in resting-state RR (see Table 3).
Vigilance and motor readiness to emotion faces
There were no differences between children with chronic pain and controls in overall reaction times (F(5, 340) = 1.01, p = .417), in overall accuracy (F(5, 340) = 0.44, p = .793) on the emotion-face identification task (Greenhouse–Geisser corrected) and in reaction and accuracy times for each emotion (see Table 6).
Raw scores for accuracy and reaction time for individual emotions in the emotion-identification task.
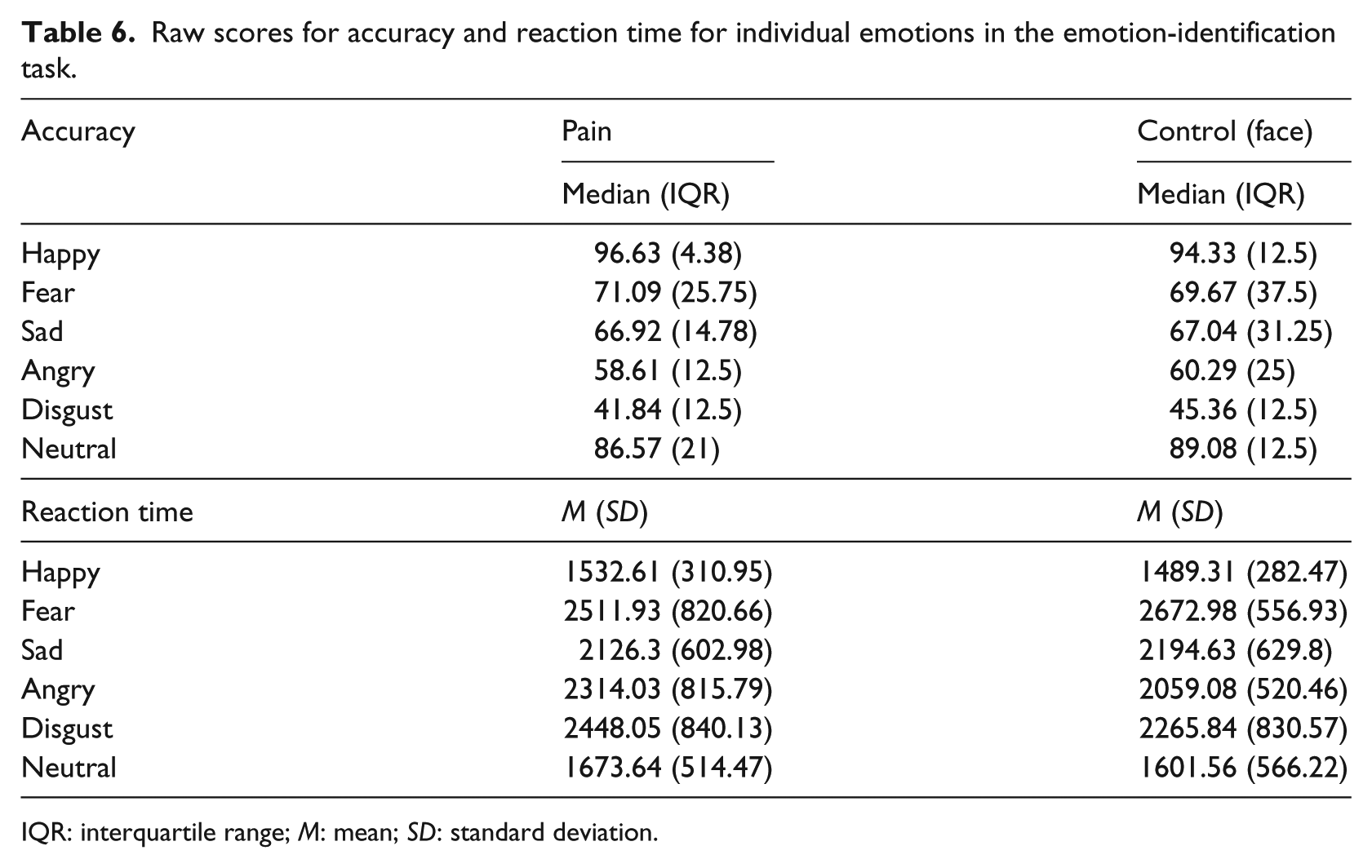
IQR: interquartile range; M: mean; SD: standard deviation.
Post hoc analyses
BMI percentile and DASS Total were negatively correlated with both HRV-RMSSD and HRV-HFP (see Table 7). EDA was positively correlated with HR and negatively correlated with RR. HR was negatively correlated with all HRV measures, while all HRVs were positively correlated with each other.
Correlations between self-reported measures and biological markers.
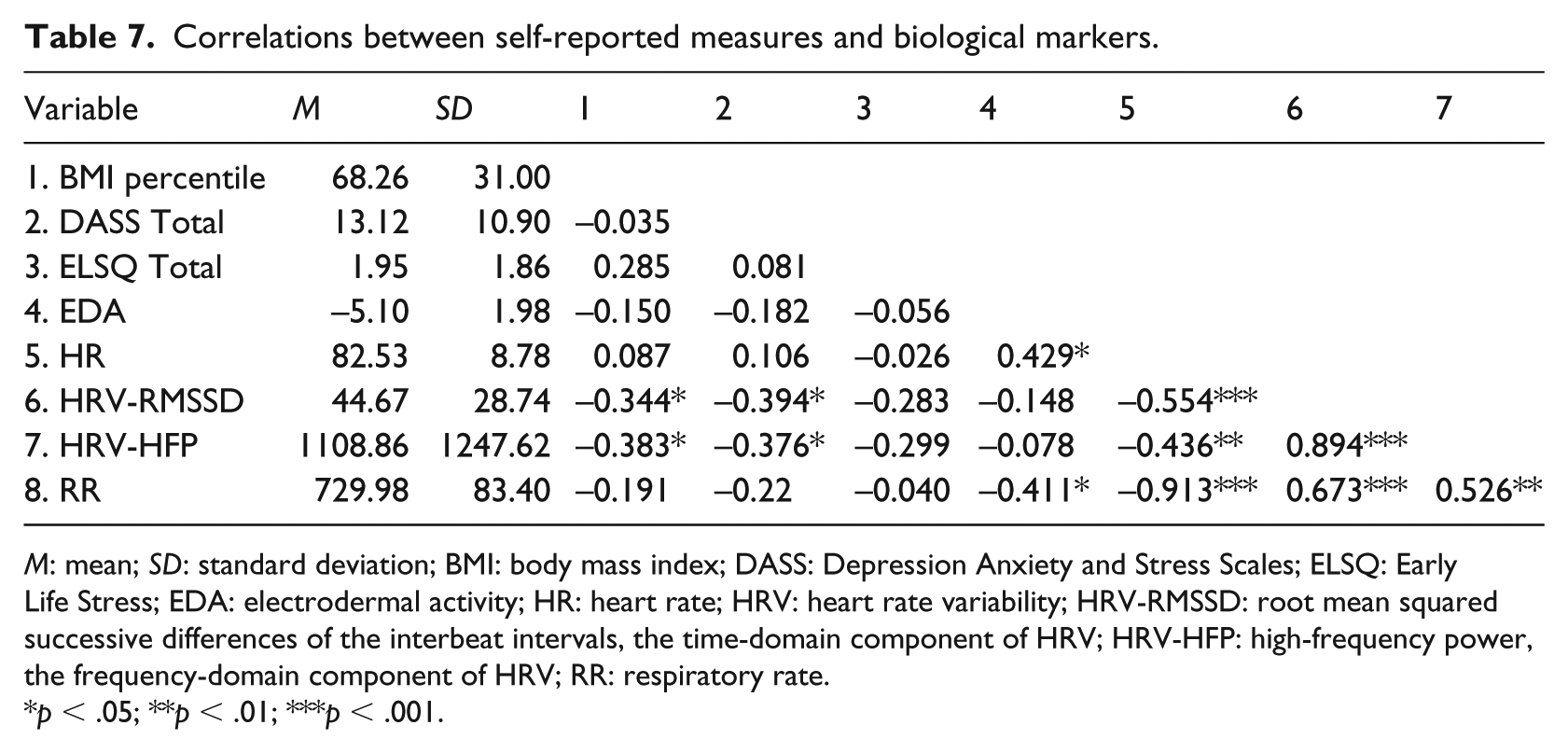
M: mean; SD: standard deviation; BMI: body mass index; DASS: Depression Anxiety and Stress Scales; ELSQ: Early Life Stress; EDA: electrodermal activity; HR: heart rate; HRV: heart rate variability; HRV-RMSSD: root mean squared successive differences of the interbeat intervals, the time-domain component of HRV; HRV-HFP: high-frequency power, the frequency-domain component of HRV; RR: respiratory rate.
p < .05; **p < .01; ***p < .001.
Discussion
In this study, we used biological markers of stress-system function – HR, HRV, EDA, CRP titres, RR and face recognition reaction times – to examine whether children and adolescents with chronic pain (vs controls) showed activation of one or more components of the stress system. Alongside the biomarkers, we also used self-report measures of adverse life events across development and subjective anxiety, depression and distress. Compared to controls, patients reported more adverse life events and higher depression, anxiety and distress. Alongside the pain and psychological distress, patients showed activation of the autonomic system – both decreased vagal activation and increased sympathetic activation – as reflected by lower HRV, elevated HR and elevated skin conductance in the resting state. As a group, patients also showed a shift towards a proinflammatory state, as reflected by median percentiles that were demonstrably higher than the reference ranges reported previously in population studies or healthy controls. More than a quarter of patients showed elevated CRP titres (⩾2 mg/L), falling in the low-grade inflammation (2–15 mg) range. Our study adds to a growing literature suggesting that psychological distress in children and adolescents with chronic pain occurs together with stress-system activation and dysregulation. The results affirm that interventions for children and adolescents with chronic pain need a multidisciplinary mind–body approach (Hechler et al., 2010), one that concurrently addresses physical impairment, stress-system dysregulation and psychological distress.
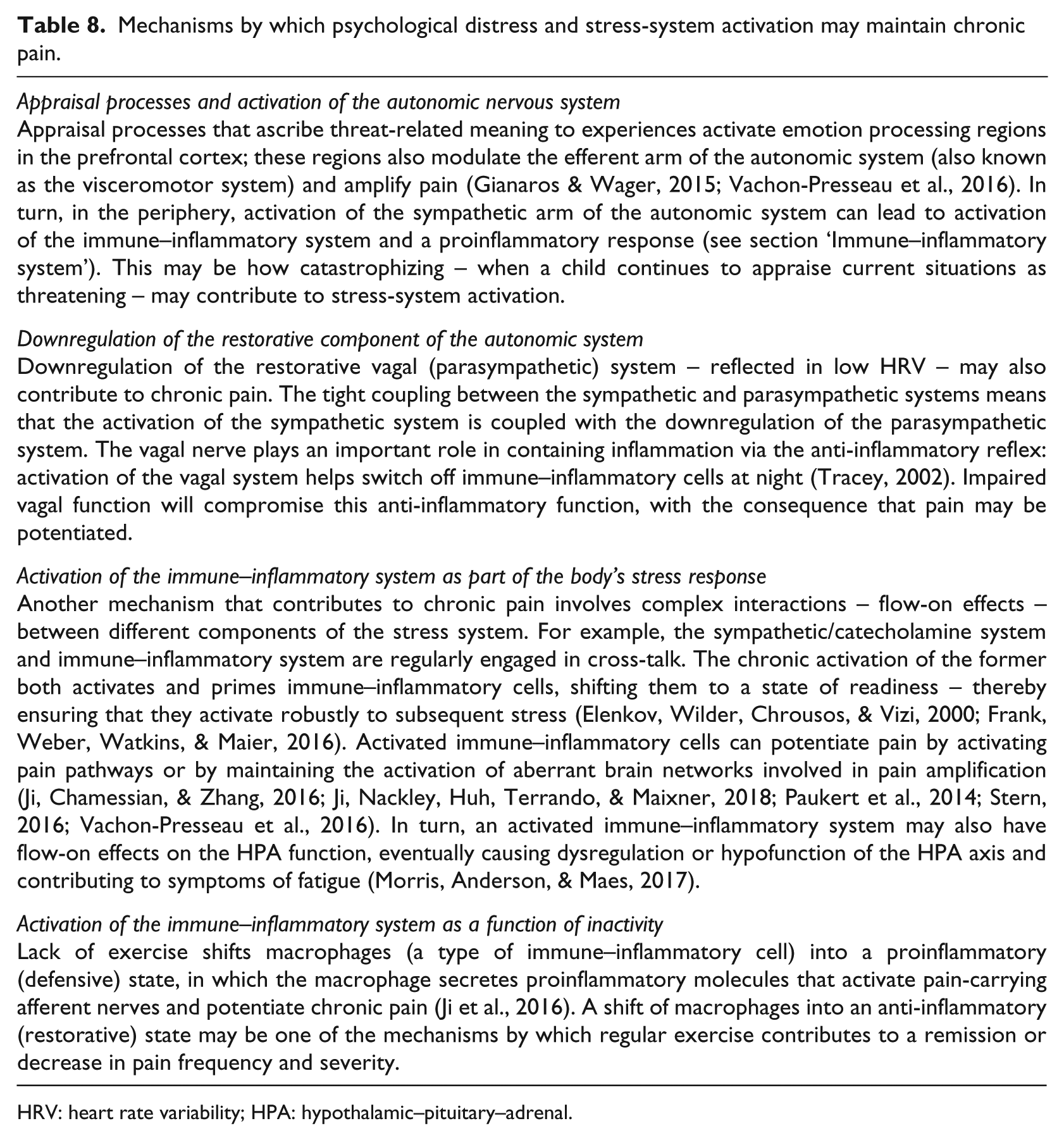
Over the last 20 years, a large body of research has found that adverse childhood experiences play a role in the development of chronic physical illnesses, mental health disorders and functional somatic symptoms, including chronic pain, later in life (Felitti et al., 1998; Fischer, Lemmer, Gollwitzer, & Nater, 2014; Flaherty et al., 2009; Nelson, Simons, & Logan, 2018). Against this background, neuroscientists have been trying to understand how adverse life events during development are biologically embedded in the body and, in particular, how adverse life events ‘alter physiological systems to produce a chronic stress burden’ (McEwen, 2012, p. 17180) that affects health and wellbeing and increases the risk of stress-related disorders over the lifespan (Chrousos, 2009; Hertzman, 1999; McEwen, 2012). In this study, our patients with chronic pain reported more adverse life events and more psychological distress than their healthy peers. These results are in line with previous findings (Friedrichsdorf et al., 2016; Mulvaney, Lambert, Garber, & Walker, 2006; Nelson et al., 2018; Simons, 2016). Alongside the psychological distress, our patients with chronic pain showed increased activation of the stress system. Whereas previous studies have emphasized the importance of psychological distress in the maintenance of chronic pain – measuring constructs such as pain catastrophizing, fear of pain, attention to pain, lower perceived self-worth and increased rates of comorbid anxiety and depression (Friedrichsdorf et al., 2016; Simons, 2016) – our results suggest that activation and dysregulation of the stress system occurs alongside psychological distress. In this context, it seems that psychological and neurophysiological processes interconnect and interact together to trigger and maintain chronic pain. In Table 8, we summarize some of the neurobiological mechanisms by which psychological distress and stress-system activation may maintain chronic pain.
Mechanisms by which psychological distress and stress-system activation may maintain chronic pain.
HRV: heart rate variability; HPA: hypothalamic–pituitary–adrenal.
The pattern of relationship between various biomarkers in the pain group – that is, a positive association between HR and EDA (two different branches of the sympathetic system) and between HRV-RMSSD and HRV-HFP (HRV in the time and frequency domains, respectively) and a negative association between HR and HRV – was consistent with known associations. The findings of a relationship between HR and CRP titres ties in with the broader literature suggesting that there are complex interactions between autonomic system activation, immune–inflammatory system activation and chronic pain (see Table 8). Likewise, the finding that BMI percentile and DASS Total were negatively correlated with both measures of HRV suggests a complex relationship between subjective distress and body systems involved in energy regulation and arousal. An association between BMI and HRV in both young women (Sheema & Malipatil, 2015) and young men (Yadav et al., 2017) has recently been reported, and the relationships between stress and autonomic function and between stress and weight increases in children are areas of current research (Elbers, Rovnaghi, Golianu, & Anand, 2017; Pervanidou & Chrousos, 2018).
Our patients’ mobility was also significantly compromised, and our patients were significantly deconditioned (see mobility status described in section ‘Results’). Persisting immobility is related to a proinflammatory (defensive) state that functions to potentiate chronic pain and that can be reversed with regular exercise (see Table 8). In turn, for approximately half of the sample, the loss of mobility was associated with an unhealthy BMI in the overweight or obese range, increasing risk for future health problems.
Surprisingly, markers of motor activation – RR and reaction times to emotion faces – were not increased in children with chronic pain. These findings are in stark contrast to children presenting with nonepileptic seizures, many of whom show an increase in resting RR (Kozlowska et al., 2017), and to patients with functional neurological symptoms in general, who as a group show faster reaction times to emotion stimuli, suggesting the activation of motor systems alongside the stress system (Kozlowska, Brown, Palmer, & Williams, 2013). 4 It is possible that aberrant activation and engagement of motor regions play a central role in relation to functional neurological symptoms, where motor symptoms are the key feature of the clinical presentation.
Clinical implications
Our findings of stress-system activation suggest that interventions that downregulate the body’s stress system – or any component of the stress system – will help move the stress system towards more healthy function and are therefore an important component of any multidisciplinary treatment programme for chronic pain. Downregulating the autonomic system to a less activated state may act as a circuit breaker within the stress system. HRV biofeedback and slow-breathing exercises (HRV is maximal at slower breathing rates) are powerful interventions for upregulating the vagal function and downregulating the sympathetic function (Gevirtz, 2000; Paccione & Jacobsen, 2019). Likewise, regular exercise, for example, is a powerful intervention that helps change stress-system function at multiple system levels. Exercise targets autonomic nervous system dysregulation by helping re-establish autonomic regulation through daily activation and deactivation of the stress system. Exercise also targets immune–inflammatory system activation by helping macrophage cells shift to an anti-inflammatory (restorative) state (Ji, Chamessian, & Zhang, 2016; see Table 8). Exercise also facilitates re-establishment of healthy set-points within the stress system because of its role in brain plasticity and new learning (Saraulli, Costanzi, Mastrorilli, & Farioli-Vecchioli, 2017), presumably helping to reverse some of the functional and brain plasticity changes that maintain chronic pain. Other mind–body interventions – mindfulness, regulation exercises using imagery and hypnosis – help the child or adolescent downregulate brain arousal systems and help modulate stress-system regulation (Creswell, Lindsay, Villalba, & Chin, 2019; Jiang, White, Greicius, Waelde, & Spiegel, 2017). Finally, because stress affects the brain–gut axis and the gut is involved in the modulation of the immune–inflammatory system, simple dietary interventions that help maintain the health of that system – promoting an anti-inflammatory effect and helping decrease rates of comorbid anxiety and depression – may emerge as an important component of interventions for chronic pain (Chatterton et al., 2018).
Limitations
This study has a number of limitations. First, the study sample is small. Second, the children who participated in this study were severely disabled by chronic pain. In this context, it is possible that children with less pain-associated disability would not demonstrate the degree of stress-system activation/dysregulation found here. That said, our findings cohere with those from other studies (Evans et al., 2013; Jonker, Schoevers, et al., 2017; Tsao et al., 2012; Walker et al., 2017). Third, the laboratory assay used to measure CRP in our cohort had a coefficient of variation of 12% at 7.3 mg/L, with a limit of blank of 2.1 mg/L. Consequently, CRP titres less than 2 mg/L could not be measured. Because of this, we do not know if the children with CRP levels of <2 mg/L also showed an upward shift in CRP levels compared to controls, as shown by Jonker, Schoevers, et al. (2017). In future studies, the use of CRP assays with lower limits of detection (high-sensitivity CRP) will be able to better measure subtle changes in systemic inflammation (at lower CRP levels). Fourth, because of the severity of the participants’ medical conditions, we were unable to withdraw them from their psychotropic medications prior to the laboratory visit. The majority of our patients were treated with SSRIs, and the clinical literature suggests that SSRIs may accelerate motor reaction times (Dumont, de Visser, Cohen, van Gerven, & Biomarker Working Group of the German Association for Applied Human, 2005) – a result that we did not find. It is possible, however, that without the use of SSRIs, the reaction times to emotion faces in the children with chronic pain (vs controls) may have been slower.
Conclusion
Our study has significant implications for the treatment of children and adolescents disabled by chronic pain. It adds to a growing literature indicating that psychological and neurophysiological processes interconnect and interact to activate the body’s stress system and to trigger and maintain chronic pain. This study also highlights that interventions for children and adolescents with chronic pain need to address stress-system dysregulation, alongside physical impairment and psychological distress. Interventions need to address both body and mind.
Footnotes
Authors’ note
Peter M McInnis is also affiliated with Rivendell Child Adolescent and Family Mental Health Service, Sydney Local Health District, Australia.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: T.B. reports stock, stock options and a salary from Total Brain, Australia (owner of the rights to the Brain Resource International Database) outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.