
Abstract
Purpose:
Post-traumatic stress disorder (PTSD) rates among hospitalised adolescents are between 21% and 32%, and there is a lack of evidence-based interventions for this population. Trauma-focused cognitive behaviour therapy (TF-CBT) is an evidence-based intervention for children and adolescents with PTSD; however, it has not been implemented in an acute adolescent inpatient unit. This study examines the implementation of an intensive form of TF-CBT in an adolescent inpatient unit.
Method:
An uncontrolled open trail study was conducted where 15 adolescents diagnosed with PTSD were treated with an intensive form of TF-CBT. Measures used were the University of California, Los Angeles’ (UCLA) PTSD Reaction Index for Diagnostic and Statistical Manual of Mental Disorders (4th ed., Adolescent Version; DSM-IV-Adolescent Version), the National Stressful Events Survey PTSD Short Scale (NSESSS) and the Children’s Global Assessment Scale (CGAS)
Results:
Adolescents received an average of nine sessions of TF-CBT over a period of 28 days. The average NSESSS on admission was 23.73 and 8.27 at discharge; the CGAS average on admission was 19 and on discharge was 48.7; both were statistically significant changes.
Conclusion:
Preliminary findings support the use of an intensive form of TF-CBT to treat adolescents with PTSD admitted to acute adolescent inpatient units indicating the need for further research in this area.
Keywords
Introduction
Exposure to traumatic event/s results in the development of post-traumatic stress disorder (PTSD) in approximately 16% of children and adolescents (Alisic et al., 2014). Research of hospitalised adolescents indicates that more than 96% have been exposed to a potentially traumatic event (Havens et al., 2012), and the rate of PTSD in this population is between 21% and 32% (Allwood et al., 2008; Lipschitz et al., 1999). Harr et al. (2013) found that in one residential sample of youth, the average number of trauma prior to admission was 2.25 with the most common types being loss of parent, physical abuse, sexual abuse, and verbal abuse. Further to this, Allwood et al. (2008) found that compared with hospitalised adolescents without PTSD, those with PTSD had higher rates of co-morbid major depressive disorder (MDD), conduct disorder and suicidal ideation, and more frequent and longer hospital admissions. The diagnosis of PTSD among traumatised adolescents in inpatient settings is often challenging given the rates of comorbidities and varying expressions of emotional and behavioural difficulties. In addition, adolescents with PTSD may present to hospital due to other comorbidities and risk-related behaviour, making the impact of trauma challenging to identify (Zelechoski et al., 2013).
Trauma-focused psychotherapies are recommended as first-line treatments for adolescents experiencing PTSD (Cohen et al., 2010; National Institute for Clinical Excellence, 2005). Trauma-focused cognitive behavioural therapy (TF-CBT) has been identified as an empirically supported intervention for adolescents with PTSD (de Arellano et al., 2014; Gillies et al., 2012; Leenarts et al., 2013). While the majority of research on TF-CBT has been conducted in community settings (Cohen et al., 2004, 2011), TF-CBT has also been implemented in adolescent residential treatment facilities where the length of stay (LOS) varies between 4 months and 2 years (Cohen, Mannarino, & Navarro, 2012). In addition, the beneficial outcomes of TF-CBT have been demonstrated with adaptions such as reducing the number of sessions to eight (Deblinger et al., 2011) and adapting TF-CBT for adolescents with complex trauma (Cohen, Mannarino, et al., 2012).
Intensive interventions for PTSD have been conducted in community, residential settings and in individual and group formats. Two randomised controlled trials (McMullen et al., 2013; O’Callaghan et al., 2013) utilising TF-CBT with war-affected adolescents trialled a group TF-CBT programme providing three 2-hour sessions a week over a period of 5 weeks. Results in both studies indicated significant reductions in PTSD symptoms compared with wait-list control. Within a community sample, Ehlers et al. (2010) reported that intensive treatment (several sessions a week) for the adult mental health consumers with PTSD was as effective as the standard weekly cognitive treatment. Patients receiving the intensive treatment were seen to improve their daily functioning over a shorter period of time thus minimising the impact that PTSD has on their daily lives. Murphy et al. (2015) conducted an intensive 6-week residential programme for veterans diagnosed with PTSD, and this programme implemented three individual trauma-focused cognitive behavioural sessions a week in combination with the daily group programme. Findings indicated a reduction in PTSD symptoms which were maintained at 6-month follow-up. These studies add support for conducting PTSD treatment in an intensive way in a short time frame.
Foa et al. (2000) acknowledged that the research on the efficacy of inpatient treatment of PTSD is of a limited nature and only in relation to an adult population, predominantly veterans. Furthermore, current interventions for PTSD in acute settings largely focus on stabilisation, safety and improving coping skills (Foa et al., 2000). Gudiño et al. (2014) examined a group trauma-informed treatment for adolescents with PTSD in an inpatient setting which focused on skills training including psychoeducation, emotion regulation, communication and safety planning. This group programme was a brief version of the Skills Training in Affective and Interpersonal Regulation (Cloitre et al., 2006) programme adapted for adolescents (Brief STAIR-A) which targeted stabilisation, functioning, symptom reduction and safety. They found some reduction in PTSD symptoms at discharge compared with intake and increased coping efficacy at discharge, adding support to inpatient units providing trauma-specific interventions (Gudiño et al., 2014).
There is a significant need for adolescents with PTSD who are admitted to inpatient mental health units to receive specific targeted interventions that address their trauma-related symptoms. There is a high rate of PTSD among adolescents admitted to inpatient mental health units, yet there is a lack of research regarding empirically supported treatments for this population. This study builds on Gudiño et al. (2014) by exploring the implementation of an empirically supported treatment, TF-CBT, that includes an exposure component. As it is unknown that TF-CBT can be implemented in an adolescent inpatient unit, an uncontrolled open trial was conducted to explore this issue further. It is expected that the adolescents included in this study will experience a reduction in PTSD symptom severity following intensive TF-CBT intervention.
Methods
Study site and sample
Gna Ka Lun (GKL) is a 10-bed acute adolescent (11–17 years) tertiary Inpatient Unit, located in South Western Sydney Local Health District (SWSLHD), New South Wales (NSW), Australia. Referrals take place from emergency departments (ED) or outpatient community mental health services throughout NSW and Australian Capital Territory (ACT). Demand for service is high due to the number of ED and ambulatory presentations. Over 50% of GKL admissions are from the EDs and the rest from ambulatory services.
Procedure
All adolescents admitted to GKL between May 2015 and November 2016 were assessed by the multidisciplinary team (MDT) consisting of a senior child and adolescent psychiatrist, psychiatry registrar, clinical psychologist and senior nurse. Trauma screeners were administered at admission to screen for exposure to trauma. Assessments took place over two to three sessions, diagnoses were made using the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V; American Psychiatric Association, 2013) criteria. Adolescents whose primary diagnosis was PTSD formed the study sample. Adolescents with moderate to severe intellectual disability, comorbid schizophrenia and mania were not considered; however, those with autism spectrum disorder (ASD) and mild intellectual disability were included in this study.
The pre-test measures were administered – by either researcher 1 or researcher 2 who are both clinical psychologists, to the adolescents with a primary diagnosis of PTSD on admission. Following this, they underwent TF-CBT intervention to target their PTSD symptoms. Treatment was typically delivered in two to three sessions per week over a 3- to 4-week period. At discharge, the post-test measures were administered by either researcher 1 or researcher 2. The adolescent’s notes were reviewed in detail by two independent clinicians, a senior registered mental health nurse and a senior child psychiatrist not involved in their care and the Children Global Assessment Scale (CGAS) rating on admission and discharge was then scored. The CGAS evaluated the adolescent’s global impairment on a scale from 0 to 100 with higher scores indicating better functioning across domains. The CGAS has high interrater reliability (.84) and test–retest reliability (.85) and authors report good discriminant validity (Shaffer et al., 1983).
Measures
Exposure to traumatic event
The initial screener (Questions 1–13) of the University of California, Los Angeles (UCLA) PTSD Reaction Index for Diagnostic and Statistical Manual of Mental Disorders (4th ed., Adolescent Version; DSM-IV-Adolescent Version; Steinberg et al., 2004) was used to screen for exposure to traumatic events at admission. The symptom severity component of the UCLA was not used given the timeframe of exploring symptom severity over a 30-day period, a timeframe which was deemed too lengthy for repeated use in an acute inpatient setting.
Severity of post-traumatic stress symptoms
The National Stressful Events Survey PTSD Short Scale (NSESSS) is a nine-item self-report measure which assesses the severity of PTSD symptoms in children aged 11–17 and has high validity (.84) and reliability (α = .91; Kilpatrick et al., 2013). Adolescents rate the intensity of symptoms over the last 7 days on a 5-point Likert-type scale. Adolescents reporting multiple traumas were asked to identify the trauma causing them most impairment and this was targeted for treatment. The NSESSS was chosen for use in the inpatient setting as it allowed for repeated use after a 7-day period and as such would be valid and reliable for the shorter LOS. The NSESSS was administered pre and post TF-CBT treatment.
Intervention
TF-CBT is an evidence-based treatment for children and adolescents with PTSD, typically conducted over a 12- to 16-week period with one session conducted per week and is used frequently in community settings with children and adolescents aged between 3 and 18 years of age (Cohen et al., 2017). The primary components of TF-CBT are referred to by the acronym ‘PRACTICE’: Psychoeducation/Parenting Skills, Relaxation, Affective Modulation, Cognitive Coping, Trauma Narrative and In Vivo Exposure to decrease trauma reminders, Cognitive Processing, Conjoint Child–Parent sessions and Enhancing Safety. Its use in an acute adolescent inpatient unit has not been described. As the historical average LOS at GKL was approximately 22 days, the standard TF-CBT programme was adapted to provide two to three TF-CBT sessions a week, as opposed to once per week as conducted in community settings. TF-CBT was identified as an intervention which is consistent with the broader Trauma Informed Care framework of which the unit operates.
Following completion of the measures, TF-CBT was delivered by a clinical psychologist. Both clinicians completed online and face-to-face training in TF-CBT. In addition, researcher 1 completed the Supervisors Training and Master Class. During the course of this study, the clinicians engaged in weekly peer supervision. Researcher 1 also engaged in group supervision sessions from an accredited TF-CBT trainer and consultant via phone from the United States. As using TF-CBT in an acute inpatient setting is a novel approach, fidelity to the content of the model was considered essential. The only modification made was condensing the programme delivery into 2–3 weekly sessions over an average of 4 weeks, instead of weekly over 12–16 weeks to complete the TF-CBT package during the course of admission. This adaptation of TF-CBT reduced the length of the programme by 75% on average while preserving the integrity of the model by retaining the ‘PRACTICE’ components implementation.
Two to three TF-CBT sessions were conducted per week. Initial symptom severity measure was completed as part of the adolescent’s first TF-CBT session. Typically, the entirety of TF-CBT as implemented in this study involved the following: each individual component of PRAC was provided in one session; the Trauma Narrative was processed over one to three sessions; Cognitive processing over one to two sessions; finally, one session was spent on Enhancing Safety completing post measures. As such, between 8 and 10 TFCBT sessions were averaged over a 3- to 4-week period, although in some cases this varied based on individual circumstances.
Although including parent/caregiver in the conjoint, trauma narrative session is usually recommended (Cohen, Mannarino, et al., 2012; Cohen, Mannarino, & Navarro, 2012); however research conducted by Deblinger et al. (1996) indicates that TF-CBT improves PTSD symptoms when conducted with children only.
In this study, parents/caregivers were included in psychoeducation which included discussion of the trauma events and its impact on the adolescent and their wellbeing. Parents were also included in parenting components to help increase support and attachment. In regard to sharing, the Trauma Narrative adolescents refused to include their parents in the reading of their narrative for a number of reasons, which included the nature of the traumatic event and/or the non-offending parent was also a victim of the trauma event. However, a session with parents/caregivers was still conducted to provide an overview of the Trauma Narrative to give context about the trauma event and to coach parents/caregivers on how to respond to the adolescent regarding their courage in completing the Trauma Narrative. The last session involved families and their adolescent in discussing ways of enhancing future safety.
In addition to receiving TF-CBT which included individual and family sessions, all adolescents were provided with pharmacotherapy, family meetings with treating team to discuss the progress of treatment, group therapy which focused on coping skills, educational support and remediation during their stay at GKL. Other than TF-CBT, none of the aforementioned interventions addressed trauma specifically. On discharge, a handover of treatment and progress was provided to the local community child and adolescent mental health service of all adolescents, including those in the study, which is standard practice for adolescents discharged from the unit. The role of the local community child and adolescent mental health service is to provide ongoing support of adolescents and their families/care givers.
Participants
The sociodemographic and clinical variables are detailed in Table 1. The average age of the participants was 14.66 years with an overwhelming majority of them being female (87%). Sexual and/or physical abuse accounted for 80% of the identified traumatic event leading to PTSD. MDD was the most-common comorbidity (87%). All participants were admitted to GKL from the ED due to a number of reasons, primarily relating to self-harm or suicide. Other reasons included deterioration in functioning, aggression and homicidal ideation. Given the multiple comorbidities and admission to the unit due to risk-related issues, the identification of PTSD as the primary problem was often not recognised until comprehensive assessment was conducted.
Demographic information (N = 15).
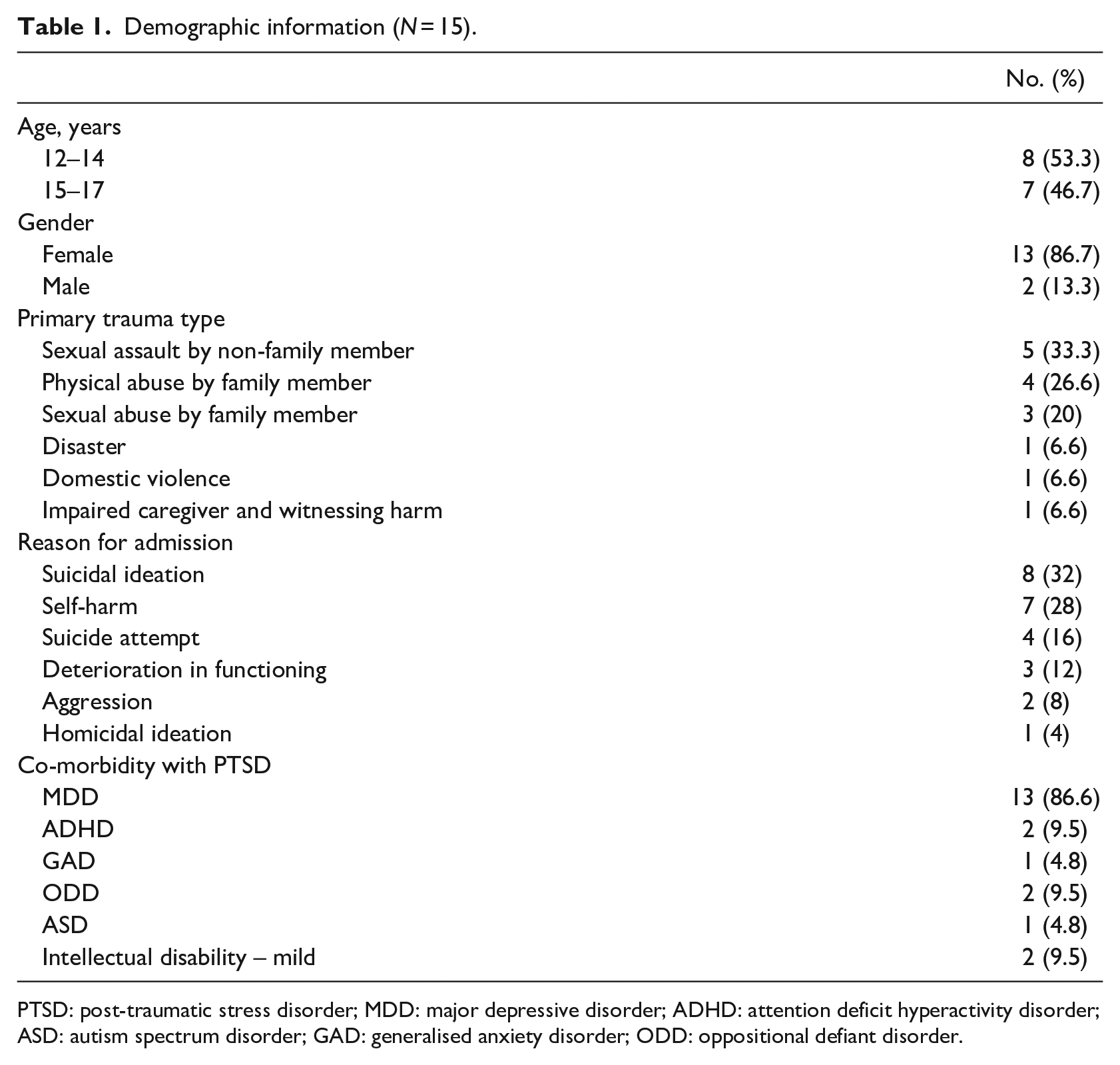
PTSD: post-traumatic stress disorder; MDD: major depressive disorder; ADHD: attention deficit hyperactivity disorder; ASD: autism spectrum disorder; GAD: generalised anxiety disorder; ODD: oppositional defiant disorder.
Ethical considerations
Ethics for this was part of a larger study examining the overall experience of adolescents accessing GKL. TF-CBT was part of the suite of interventions offered to all admitted adolescents depending on their need. Approval was granted by SWSLHD Human Research Ethics Committee. All participants gave signed consent to engage in treatment as prescribed.
Analyses
The data were collected on a semi-structured format designed for the study and analysed using SPSS version 25. Paired t-tests were used to test the effectiveness of TF-CBT in this study.
Results
Out of 120 adolescents admitted between May 2015 and November 2016, 41 (34%) had diagnoses of PTSD. Fifteen of them were considered eligible for the study as they had a primary diagnosis of PTSD and had a LOS greater than 5 days. The LOS for the 15 participants included in the study ranged from 25 to 81 days (M = 48.3; SD = 15.6) with a length of treatment ranging from 16 to 46 days (M = 27.8; SD = 8.98) with session frequency of two to three sessions per week with a mean of 9.1 sessions (SD = 1.58). Psychosocial factors, primarily accommodation, contributed to the increased LOS for some adolescents in this treatment group. Factors influencing length of treatment included transition to school, integration back into the community and in one case transition from male to female therapist during the narrative phase.
The PTSD severity as measured by NSESSS ranged from 13 to 35 at admission (M = 23.9; SD = 6.78) and from 0 to 19 at discharge (M = 8.1; SD = 6.1). Level of functioning as measured by CGAS ranged from 10 to 28 at admission (M = 19; SD = 4.8) and from 38 to 55 at discharge (M = 48.7; SD = 5.7). To test the effectiveness of TF-CBT as a treatment intervention for PTSD in adolescents, pre-intervention measures of the CGAS and NSESSS were compared with post-intervention measures of the CGAS and NSESSS, using two separate paired t-tests (as the current data set met the assumptions of a paired t-test). While two outliers were more than 1.5 box lengths from the edge of the box in the box plot, inspection of their values did not indicate them to be extreme, and thus, they were kept in the analysis. Furthermore, the difference in scores for the pre- and post-test CGAS and NSESSS were normally distributed, as assessed by visual inspection of the histograms and the Shapiro–Wilk’s test (p = .193, p = .556 respectively). As preliminary analysis of the data indicated that the difference in scores on both the CGAS and NSESSS did not significantly vary with age or treatment length ps > .05, these variables were not included in the analysis. Clinical relevance of the change in global functioning and severity of PTSD symptoms before and after intervention are explained in terms of clinical classifiers within the measures. At the time of admission and before TF-CBT intervention, on average, patients fell within the second lowest functional range on the CGAS, that is, Very Severely Impaired – Considerable supervision is required for safety (average score of 19.00 on the CGAS). Following treatment, on average, patients had improved in global functioning such that they moved up three clinical classifiers to the functional range: Obvious Problems – Moderate impairment in most areas or severe in one area (average score of 48.73 on the CGAS). Furthermore, at the time of admission and before TF-CBT intervention, on average, patients fell within the Moderate to Severe range on the NSESSS (average score of 2.64 on the NSESSS/total score of 23.73 on the NSESSS). Following treatment, on average, patients had improved in PTSD symptom severity such that they fell within the None to Mild range for PTSD symptom severity as measured by the NSESSS (average score of 0.92 on the NSESSS/total score of 8.27 on the NSESSS (Table 2).
Outcome measures.
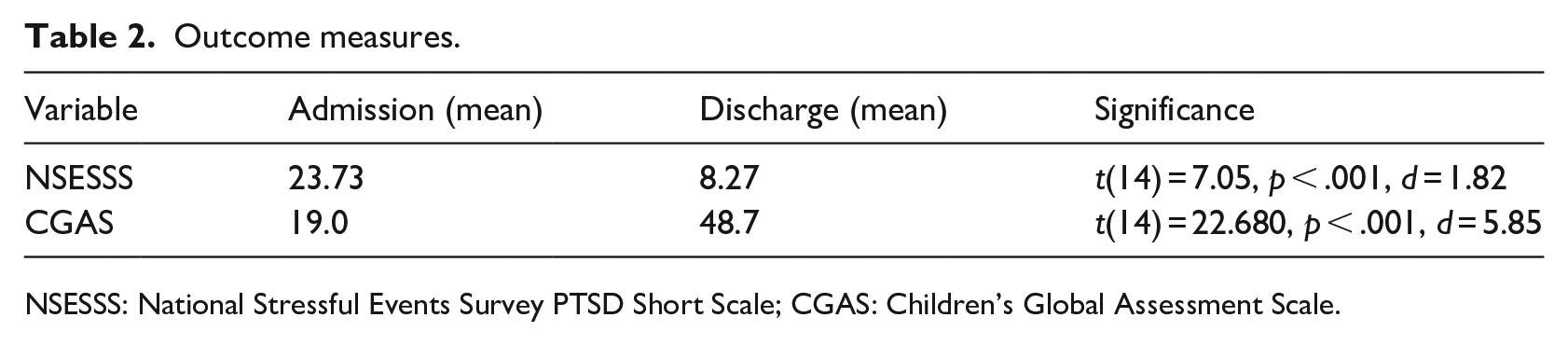
NSESSS: National Stressful Events Survey PTSD Short Scale; CGAS: Children’s Global Assessment Scale.
Intervention impact as tested by pre- and post-test difference
Following the TF-CBT intervention, patients demonstrated a significant reduction in symptom severity as rated by the NSESS (mean difference = 15.47, SD = 8.49; t(14) = 7.05, p < .001, d = 1.82) and a significant improvement in global functioning on the CGAS (mean difference = 29.73, SD = 5.08; t(14) = 22.680, p < .001, d = 5.85). These results indicated, that within a typical inpatient treatment setting, that TF-CBT intervention had a small effect size on patients with PTSD symptoms and a medium effect size on their global functioning.
Discussion
The findings of this uncontrolled open trial suggests that an intensive form of TF-CBT for adolescents in an acute inpatient setting is associated with a significant decrease in symptoms of PTSD and a notable increase in the level of functioning among participants.
This novel modification of an effective treatment is potentially a recommended addition to the therapeutic repertoire of all acute inpatient units for those adolescents with PTSD. These early findings demonstrate that interventions within an inpatient setting can be structured and intensive rather than focusing only on containment and stabilisation. Adolescent inpatient mental health settings may benefit from having TF-CBT as a specific approach incorporated within the broader framework of Trauma Informed Care. Further research would be beneficial to explore potential applications of intensive psychological interventions for their use in inpatient settings.
In line with previous TF-CBT research (de Arellano et al., 2014; Gillies et al., 2012; Leenarts et al., 2013), this study resulted in a reduction of PTSD symptoms. The findings of this study regarding the reduction in severity of PTSD symptoms are similar to those of other studies in community setting (Cohen et al., 2004, 2011) and of modified versions of TF-CBT, such as a study conducted with war-affected adolescents (McMullen et al., 2013; O’Callaghan et al., 2013). Similar findings were also found in intensive adult interventions both in community (Ehlers et al., 2010) and residential programmes (Murphy et al., 2015).
Additional benefits to shortening the length of treatment is the decrease in the period of distress for the adolescent leading to a timely return to improved functioning, which was maintained at discharge and hopefully generalised to the home and school environment. Other potential uses of these findings could be that other current structured treatment programmes could be adjusted for shorter inpatient care.
Community mental health teams could refer adolescents with PTSD for an intensive form of TF-CBT within an inpatient setting if the adolescent’s level of functioning and risk mean that they cannot be managed safely in the community. The safety and supervision inherent within an inpatient environment perhaps provides the therapeutic containment that facilitates the adolescent’s engagement with the intervention without further decompensation.
Ordinarily, parents/carers are encouraged to be involved in all parts of the adolescent’s treatment journey. In this open trial, families were involved in the treatment process; however, adolescents did not consent to their parent/carer being included in the conjoint trauma narrative session as such an overview of the Narrative was shared with the non-offending parent/carer to contextualise the trauma for them. As noted by Cohen, Mannarino, and Navarro (2012), if adolescents decide not to share their trauma narrative with their caregiver, it should be respected, as not doing so may impact therapeutic relationship and progress (Deblinger et al., 1996)
This uncontrolled open trial explored the applicability of an intensive form of TF-CBT in an acute inpatient environment. As such, it was beneficial to keep the number of participants low with the view to conduct a larger study. Future studies will include a control group and a larger sample size. As there were no control groups, it was difficult to isolate what part of treatment was most effective as all participants also received treatment as usual including pharmacotherapy, group therapy and family meetings. In addition, the protocol did not measure any possible side effects or harm associated with the intervention. Given the preliminary nature of the research, post-discharge symptoms and functioning to ascertain the maintenance of improvement were not evaluated. Also, the absence of measures that specifically identify and track comorbidities makes it difficult to ascertain the role TF-CBT in reducing symptomology of co-morbid disorders.
Although we did not have a qualitative component, some spontaneous feedback from the adolescents and their families was pleasing. This included ‘When I think of how much I have accomplished, I am filled with so much hope and faith in the years to come’, and ‘Thank you for saving my daughter’s life’.
We recommend that the next research step is to compare the effectiveness of adding TF-CBT to usual care in a randomised controlled trial (RCT) in the inpatient setting, that is, TF-CBT plus usual care vs. usual care alone. Including larger sample sizes, incorporating assessment of co-morbidities and long-term follow-ups are further steps. Follow-up will assist in identifying whether the gains from an intensive form of TF-CBT are maintained over time. It would be beneficial for future studies to assess the impact of an intensive form of TF-CBT on readmission rates and length of follow-up treatment. It will also be worthwhile to measure functional gains of adolescents on the unit who are not engaged in TF-CBT to ascertain how therapeutic the unit is non-specifically. In addition, screening for PTSD/trauma experience and effects should be routine for adolescents presenting to any part of mental health services as we now have effective evidence-based treatments for them across settings. Furthermore, these findings can be easily generalised and feasibly implemented in any acute adolescent mental health unit, as the study site was a mainstream public hospital inpatient setting (with minimal exclusion criteria) and no additional funding or increase in staff required (besides training investment).
Conclusion
The preliminary findings from this uncontrolled open trial support the use of an intensive form of TF-CBT intervention for adolescents with PTSD in an adolescent acute inpatient setting. Further research in this area with a larger sample size and control group to examine the effectiveness of an intensive form of TF-CBT in an acute adolescent inpatient population is recommended.
Footnotes
Acknowledgements
We wish to acknowledge all the adolescents and their families who participated in the study; in addition all clinical staff at Gna Ka Lun who provided treatment for them at their time of crisis. Special acknowledgements also to Dr Mukesh Prabhuswamy who helped rate the CGAS of all adolescents in the study who were primarily treated by the senior child psychiatrist, and to Dr Laura Murray for her supervision and support in TF-CBT.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.