
Abstract
The study of attachment is a valuable theoretical framework to understand the influence of parents and friends on the evolution and development of adolescents. This study aimed to determine parents’ and peers’ attachment style, the relationship between parents’ and peers’ attachment and body dissatisfaction in adolescents with eating disorders (ED), and to compare it with a control group. The sample consisted of 260 adolescents (Mage = 15.35, SDage = 1.461): a control group consisting of 129 non-clinical subjects and an ED group composed by 131 adolescents diagnosed with ED who attended five ED units located in different regions of Spain. They completed the Body Shape Questionnaire (BSQ-34) and the Inventory of Parent and Peer Attachment (IPPA). Adolescents with ED have less trust with their parents, worse communication with their parents and peers, and greater alienation with fathers and peers. The results showed a statistically significant relationship between parents’ attachment and body dissatisfaction in both groups. In ED group, peers’ alienation was positively correlated to body dissatisfaction. Parental attachment and alienation feelings with peers could influence body dissatisfaction in ED adolescents.
Introduction
The study of attachment, an original construct of Bowlby’s (1969) theory, is a valuable theoretical framework to understand the influence of parents and friends on adolescent development and mental health problems such as eating disorders (ED). Recent studies have shown that a failure in the primary bond with the primary attachment figure constitutes both an etiopathogenic and a mental health risk factor for adolescents (Grzegorzewska & Farnicka, 2016). Studies on ED, considering the attachment theory, report that the insecure attachment is the most common parental style among adolescents with ED (Gander et al., 2015).
The review of attachment in adolescents with ED by Gander et al. (2015) highlights the lack of studies that analyse the possible differences in attachment between adolescents with and without ED. Orzolek-Kronner (2002) evaluated differences in parental bond among three groups: ED, clinical and non-clinical. Adolescents with ED, in comparison with the non-clinical group, showed worse communication and confidence in their parents, and greater alienation with them. Vega et al. (2011), in a study with females (aged 12–18), compared the association between attachment to mothers and peers in an ED sample and a control group. Regarding maternal attachment, they confirmed that these groups differed as regards the attachment to mothers, since adolescents with ED had an insecure mother attachment, and adolescents without ED showed better communication and trust in their mothers than adolescent girls with ED. Regarding the attachment to peers, adolescents without ED had secure attachment relationships, they trusted more and communicated a little better than adolescents with ED; these differences were minimal. They concluded that adolescents with ED showed some differences compared with a control group. These differences were much more relevant with respect to the maternal attachment than regarding the attachment with their peers. Nothing was said about alienation. On the other hand, at present, body dissatisfaction (BD) is a variable that deserves special attention in the scientific community since it is a relevant factor in the genesis, development and recovery of ED (Rohde et al., 2015). In addition, people with ED suffer from BD more often than other populations (Rabito-Alcón & Rodríguez-Molina, 2016).
A recent systematic review and meta-analysis about mediators which link insecure attachment with eating symptoms (Cortés-García et al., 2019a) revealed, in general, that the percentage of the total effect explained by the indirect effect was 58%. The pooled estimates of the indirect effect of BD were significant in studies with non-clinical population (72%) (Bäck, 2011; Koskina & Giovazolias, 2010). However, BD did not significantly mediate this relationship between insecure attachment and ED symptoms in two studies with clinical samples (Monteleone et al., 2017; Tasca et al., 2006); 26% of the total effect was explained by the indirect effect. These results did not support their expectations, and they explained them, at least partially, by the characteristics of two out of four included studies. Thus, the model tested by Tasca et al. (2006), specifically designed for patients with BN, was applied to a heterogeneous sample of women with ED, mostly AN. In addition, in this study the authors simultaneously analysed the negative affect which could have reduced the effect of BD. Moreover, another included work did not properly assess BD but the lived corporeality (Monteleone et al., 2017). In view of these considerations, they suggested future lines of research in order to study these relationships in clinical samples.
Bäck (2011), in a study with 80 high school students, found that the relationship between attachment and body/weight dissatisfaction only occurred in female students with their mothers. For females, secure maternal attachment was related to a more positive body image and self-perception of weight. Contrary, fearful maternal attachment was related to an increase in body and weight dissatisfaction. No correlations were found for males and for father attachment. Koskina and Giovazolias (2010) studied the effects of insecure attachment on the development of negative body image as a risk factor for the development of disturbed-eating patterns in male and female university students. In their study, BD fully mediated the relationship between attachment anxiety and disordered eating in women. BD mediated anxious attachment and dieting in men. In addition, attachment avoidance had a direct impact on eating behaviours for both genders, without the mediation of any variables.
In the scientific literature, most studies that analyse the relationship between attachment and BD in clinical samples of ED patients have been performed in adult population. Regarding the research conducted in adolescent population, there is a shortage of studies. In non-clinical samples, Wick et al. (2012) examined the association between attachment patterns, eating behaviour and satisfaction with one’s own figure for a nonclinical sample of adolescents (13- to 18-year-old) which included both sexes. They found a significant positive relationship between insecure attachment, development of ED, and BD. In another study, with an infant-juvenile sample of 5214 subjects (Szalai et al., 2017), it was found that parental dysfunctional attachment was associated with low BD mediated by the level of depression. However, to date we have not found scientific studies published that assess this relationship in adolescent clinical samples.
Most of the investigations mentioned so far have studied the relationship between BD and parental attachment. During adolescence a change of bonding style occurs from the parental-filial bonding towards one more relevant and stronger peer bonding, which in turn becomes more significant (Marion et al., 2013). Regarding BD, as our variable of interest, a study carried out with 216 adolescents, concluded that those who reported low-quality relationships with friends showed greater ED symptomatology and higher BD (Sharpe et al., 2014). In another investigation with adolescents, Schutz and Paxton (2007) found consistent relationships between BD, ED symptoms and negative qualities of friendship (conflict and alienation), but they did not observe this relationship with positive qualities of friendship such as communication, trust and acceptance. However, we have not found any studies that investigate the relationship between attachment and BD in adolescent clinical samples.
Considering the literature reviewed and the lack of studies that relate parental and peer attachment style and BD in clinical samples of adolescents with ED, we believe that this study might provide new data and relevant contributions focused on both prevention and treatment of adolescents with ED.
On the one hand, current best practices for ED treatment in adolescence include family-based interventions (Gorrell et al., 2019). Family-Based Treatment (FBT) is one of these (Le Grange et al., 2015). This approach considers the family, mainly parents, as a helpful and positive resource in bringing about recovery, and necessitates a good collaborative process between the parent-adolescent dyad (Forsberg & Lock, 2015). On the other hand, peers are a prominent source of support during adolescence (Sharpe et al., 2014). A good friendship could be a protective factor against ED. Therefore, we believe that addressing the improvement of the parent-child and peer-adolescent bonds could optimise treatment outcomes and achieve faster recovery in adolescents with ED.
The objectives and hypotheses of the current study are the following: (1) To find out if there are differences between parents’ and peers’ attachment in adolescents diagnosed with and without ED. It is hypothesised that adolescents without ED have better communication and trust, and less alienation with their parents and peers. (2) To study the possible relationship between parental and peer attachment and BD in adolescents diagnosed with and without ED. It is hypothesised that subjects with greater trust and communication with their parents and peers, and less alienation with them will present lower BD. (3) To determine if there are differences (ED group vs control group) with respect to the associations between attachment to parents and peers and BD. It is hypothesised that there will be differences between groups. Adolescents without ED will present a stronger correlation between attachment to parents and friends, and BD than adolescents with ED.
Method
Participants
The sample consisted of 260 subjects ranged between 13 and 17 years (Mage = 15.35, SDage = 1.461). Seventy percent (118/260) were female and 30% male (142/260). The ED group comprised 131 outpatients (50.39%) (90.1% (118/131) female and 9.9% (13/129) male) who met diagnostic criteria for ED according to ICD-10 (World Health Organisation [WHO], 1992): F50.0: Anorexia Nervosa (AN) (34.6%, 90/131) (87.8% (79/90) female) – characterised by significant weight loss, intense fear of gaining weight and body image alteration –, F50.2: Bulimia Nervosa (BN) (5%, 13/131) (100% (13/13) female) – characterised by binge eating and inappropriate compensatory behaviours –, and F50.9: ED not otherwise specified (EDNOS) (10.8%, 28/131) (92.9% (26/28) female) – not meeting all criteria for a specific diagnosis of ED. They received treatment as outpatients in five ED Units of five different regions of Spain (Andalusia, Aragon, Catalonia, Murcia and Navarra). The other sample (49.61%, 129/260) was a control group, comprising 49.6% (64/129) female and 50.4% (65/129) male, who had never attended mental health Units.
Instruments
Hollingshead’s social position index (Hollingshead, 1975). This instrument evaluates parental social classes, based on two indicators: academic degree and profession. It provides a global index that allows individuals to be classified into five classes: low class (level V), medium-low (level IV), medium (level III), medium-high (level II) and high (level I).
Body Shape Questionnaire (BSQ-34) by Cooper et al. (1987). The Spanish version was used (Raich et al., 1996). It is a self-reported questionnaire. It comprises four subscales (BD, fear of gaining weight, appearance-related low esteem and desire to lose weight) and consists of 34 items that are answered by a standard six-point Likert scale ranging from ‘never’ to ‘always’. The total score ranges between 34 and 204. The cut-off point is usually established at 105, higher scores indicating greater BD. The reliability of this questionnaire in Spanish version (Raich et al., 1996) has been reported adequate, with high levels of internal consistency (Cronbach’s alpha of .95–.97).
Inventory of Parent and Peer Attachment (IPPA) by Armsden and Greenberg (1989). It was adapted to the Spanish population by Delgado et al. (2016). It has been specifically designed for adolescents from 12 to 19 years old. It evaluates the perception of the quality of parent- adolescent relationships as well as the quality of the relationships between adolescents and friends. The questionnaire has 75 items. Each evaluation of the perception of the attachment relationship with mothers, fathers and friends yields a total score, which is calculated by combining the scores of the three subscales (trust, communication and alienation). The items of the instrument are rated by means of a four-point Likert scale: 1 (almost never or never), 2 (sometimes), 3 (often) and 4 (almost always or always). The test-retest reliability was 0.93 for parental attachment and 0.86 for peer attachment. In Spanish inventory validation (Delgado et al., 2016), an adequate internal consistency (ω ⩾ 0.68) for each of the scales of the three forms of the questionnaire was obtained.
Design and procedure
It is an observational, analytical and retrospective design carried out between 2016 and 2018.
In order to obtain the clinical sample, an intentional non-probabilistic sampling was used. A psychologist was responsible for recruiting the study participants in each ED Unit according to the following inclusion criteria: (1) Patients between 13 and 17 years old, (2) Meeting diagnostic criteria of the ICD-10 (WHO, 1992) for the diagnostic category of ED, (3) Not having a comorbid clinical diagnosis and (4) Receiving psychological and / or psychiatric treatment in each of the ED Units. When a patient attended the ED Unit and met the inclusion criteria, the psychologist explained verbally the purpose of the investigation and invited him to participate voluntarily in it. In addition, he gave the patient an information sheet that indicated the objectives of the investigation, the instructions for completing the questionnaires, the risks and inconveniences, benefits, voluntariness and the confidentiality criteria. The research project was previously approved by the Clinical Research Ethics Committee of each ED Unit. After having been informed of the research project, the informed consent was signed by the patients or by the mothers, fathers or legal guardians in case of patients under legal age. Then the patients fulfilled the questionnaires. The diagnosis according to ICD-10 (WHO, 1992), which is established by the psychiatrist or the clinical psychologist of each ED Unit through a structured interview, was collected from the patient’s medical history.
Regarding the control group, two Secondary Schools were contacted in two of the five regions participating in the study. After obtaining the appropriate permission from the Schools’ directors, a professor from each school centre, collaborating with the research, selected entire classes of students between 13 and 17 years old, and explained to the members of each class the objective of the research by inviting them to participate in it. This collaborator was in charge of informing, delivering and collecting the questionnaires completed by the students, after signing the informed consent. It was established as an exclusion criterion that participants had received or were receiving psychological/psychiatric treatment in order to avoid the possible effect that the symptomatology could have on the parental bond. For this reason, 26 subjects did not participate in the study. All the information obtained was treated in accordance with the provisions of the Spanish Organic Law 3/2018, on the protection of personal data, and the Law 41/02 on Patient Autonomy.
Data analysis
With respect to the statistical analyses, the tests were selected according to the objectives of this study, considering the nature and distribution of the variables studied.
To achieve the first objective, the differences between groups (the ED group vs the control group) in attachment to mothers, fathers and peers were examined by one-way ANOVA.
For the second objective, Pearson’s correlations were calculated to find out the relationship between attachment to parents/peers and BD in both groups.
Finally, in order to determine the third objective, the Pearson correlations were compared between the study variables in the ED group and without ED, by means of the Zou (2007) method. This method, based on confidence intervals, allowed us to examine the differences between two independent correlations. The premise is that the confidence interval reports the magnitude and accuracy of the relationship, while the standard hypothesis test mixes these two characteristics (Zou, 2007). We use the COMPCOR statistical program (Silver et al., 2015) that requires the sample size, the correlations of each group and the percentage of the confidence interval (95%). A level of significance of 5% was considered (p < .05).
Results
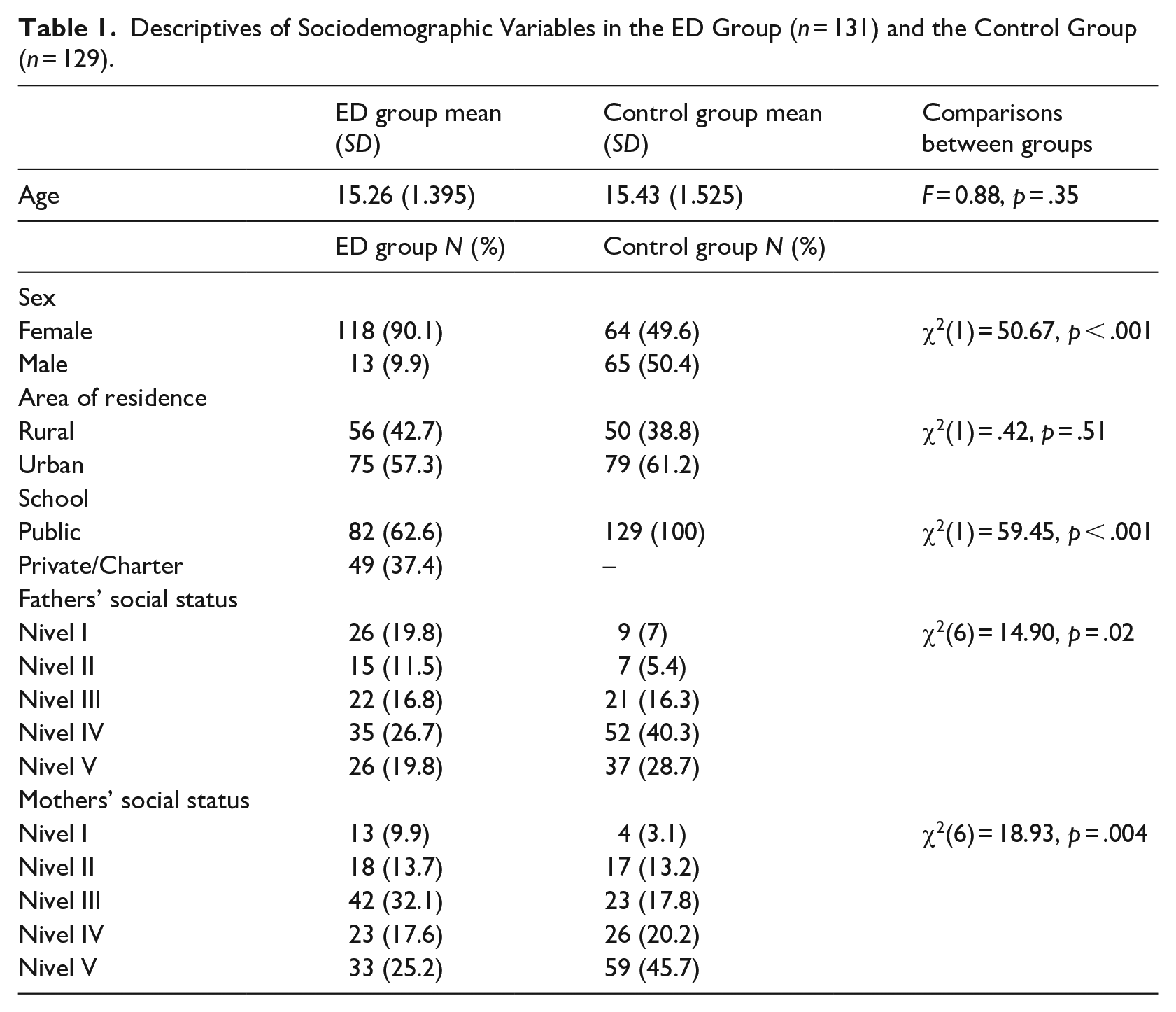
Preliminarily, we carried out a descriptive study of the study sample. There were more girls in the control group than in the ED group. In addition, parental social class was significantly higher in the ED group. See Table 1.
Descriptives of Sociodemographic Variables in the ED Group (n = 131) and the Control Group (n = 129).
For the first objective, one-way ANOVA was performed to determine if there were any differences between the ED group and the control group in IPPA scores. As shown in Table 2, adolescents with ED have less confidence with their parents, worse communication with their parents and peers, and greater alienation with fathers and friends. In addition, the ED group had a higher BD than control group, being the difference statistically significant (p < .05).
Descriptives and Comparisons Between Groups and Scores on IPPA and BSQ in the ED Group (n = 131) and the Control Group (n = 129).
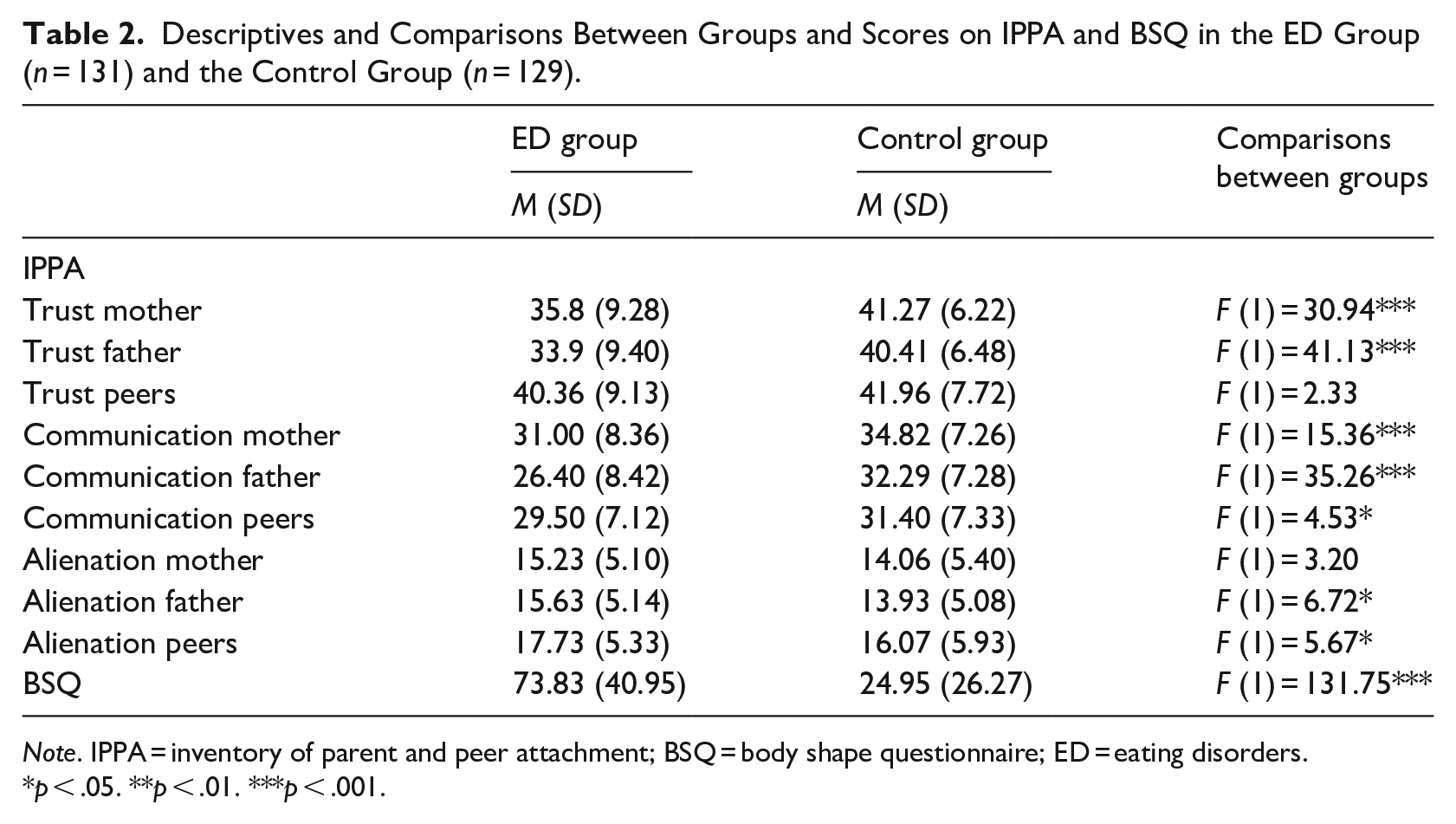
Note. IPPA = inventory of parent and peer attachment; BSQ = body shape questionnaire; ED = eating disorders.
p < .05. **p < .01. ***p < .001.
Second, to study the possible relationship between parental and peer attachment and BD in adolescents diagnosed with and without ED, Pearson’s correlations between IPPA and BSQ scores in the ED group and the control group were analysed. As it is shown in Table 3, in the ED group and the control group there are statistically significant correlations between communication, trust and parental alienation (IPPA) and BD (BSQ). That was not the case with respect to peers, where only in the ED group alienation with peers correlates positively with BD (BSQ).
Confidence Limits (95%), Correlations Between BSQ and IPPA Scores in the ED Group (n = 131) and in the Control Group (n = 129).
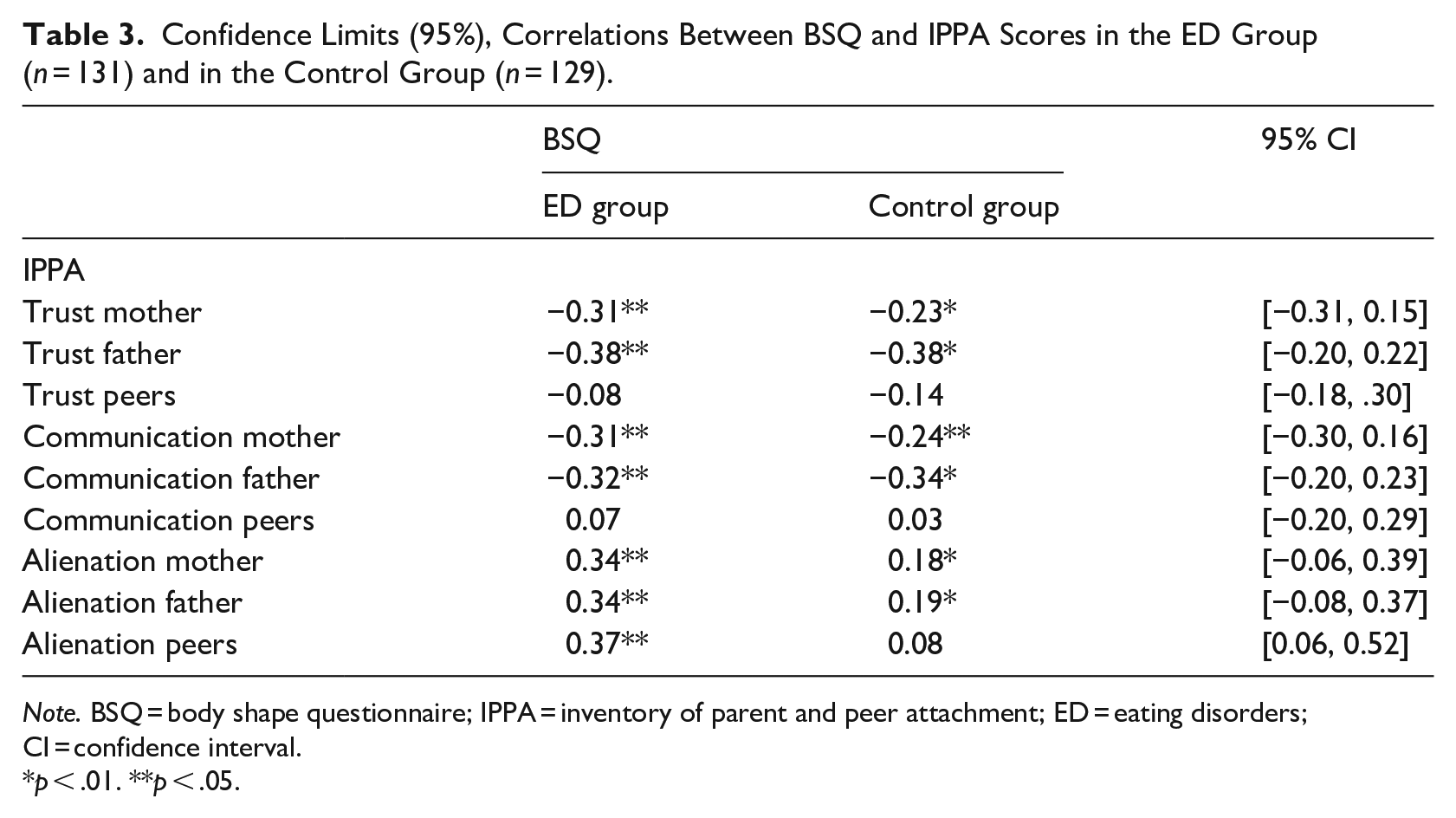
Note. BSQ = body shape questionnaire; IPPA = inventory of parent and peer attachment; ED = eating disorders; CI = confidence interval.
p < .01. **p < .05.
Finally, to determine the third objective, we examined if there were any differences between the correlations studied in the two independent groups (the ED group and the control group) through the confidence intervals (95%). As it is shown in Table 3, there are only significant differences between groups in peers’ alienation (p < .05).
Additionally, we analysed possible differences regarding parental social class, attachment subscales (IPPA) and BD (BSQ). The results show that there are no significant differences (p > .05).
Discussion
The first objective of this research was to examine if there were any differences between parental and peer attachment in adolescents with and without ED. Our starting hypothesis is partially met. In our study, adolescents with ED have less trust with their parents, worse communication with their parents and peers, and greater alienation with fathers and peers. The results are in line with the study conducted by Vega et al. (2011) and present some differences regarding the study by Orzolek-Kronner (2002). In our study, adolescents with ED do not have a greater alienation with mothers, compared with their peers without ED. It seems that the lack of positive aspects of the relationship, such as communication and trust, have greater weight in the way the bonding is established between parents and adolescents with ED.
The second objective of this study was to explore the possible relationship between parental and peer attachment, and BD, in adolescents with and without ED. In the ED group, an attachment based on greater trust and communication and less alienation with parents correlated negatively with BD. Peer alienation correlated positively with BD. In the control group, only parental attachment was related to BD. Regarding these data it is noteworthy that peer attachment style established by adolescents with ED seems to be crucial for their body image development, which is in accordance with other studies based on non-clinical samples (Wick et al., 2012; Szalai et al., 2017) regarding parental attachment. In addition, these results are similar to those obtained by Schutz and Paxton (2007) with adolescents regarding peer attachment, BD, and ED symptoms, since they did not find association between communication, trust and several study variables.
From our study it can be deduced that parental attachment is related to BD in both adolescents with and without ED. 2. On the other hand, peer attachment does not seem to be relevant for adolescents without eating disturbances. Nevertheless, the perception of peer alienation by adolescents with ED could influence their body appreciation. This could be explained by the greater influence that peers have in the body image development in adolescents with ED (Hosseini et al., 2017). The experience with peers provides an important social context, in which the standards of appearance and ideals are communicated, modelled and reinforced and, therefore, may have significant consequences for the body image development (Rodgers et al., 2015). In this context, a relationship with peers based on alienation and isolation along with the recognition of their need for closeness, which at the same time shows feelings of anger and emotional involvement, could affect the body image development in adolescents with ED.
The third objective of the study was to determine if there were any differences between the ED group and the control group with respect to the relation established between attachment and BD. The results indicate that there are differences between groups, specifically regarding peer alienation. Nevertheless, adolescents without ED did not present a stronger correlation between attachment to parents and peers, and BD than adolescents with ED. In both groups a statistically significant relationship is established between parental attachment and BD, however, the association with peer attachment differs. In our study, no association was observed between peer attachment and BD in adolescents without ED. Against previous expectations, our study indicates that the relationship between parental attachment and BD occurs in both clinical and non-clinical samples. These data do not support our initial starting hypothesis and seem to be against the results of a recent systematic review and meta-analysis (Cortés-García et al., 2019a) in which some differences in the relationship established between BD, attachment and eating symptomatology (in both clinical and non-clinical samples) are found. This could be explained by the limitations that the authors themselves acknowledged in their meta-analysis (Cortés-García et al., 2019a).
On the other hand, the results highlight the importance of parental attachment in BD. From this perspective, adolescents with insecure attachment can internalise certain aesthetic standards, such as thinness in women or more muscle mass in men, aiming acceptance and social approval (Ferreiro et al., 2014). When these objectives are not achieved, BD increases, which in turn intensifies the risk for ED (Rohde et al., 2015).
First of all, as a novelty, this study contributes to deepen the understanding of the relationships of interest in adolescents diagnosed with ED. Secondly, to highlight the role of the father, since there is a shortage of literature on the attachment between fathers and sons/daughters with ED (Gander et al., 2015). Most of the studies on attachment have focused mainly on the mother-daughter bond. Third, this study examine the role of peers, since they acquire special relevance during adolescence, leaving the parents relegated in order to acquire the autonomy and independence necessary for their personal development. And finally, it must be noted the multicentric nature of our study since it has been developed in five different communities in the same country, which facilitates the generalisation of results.
One of the clinical implications of the findings for adolescent attachment with ED, and specifically with BD, is to help clinicians in the process of evaluation, cases formulation and treatment of patients. On the one hand, it would be interesting to include the evaluation of parents and peer attachment in adolescents who come to Mental Health Units. The understanding of the relationships that adolescents establish with their parents and peers might be helpful in any psychotherapeutic intervention. A secure bond established between parents and children, and between adolescents with their peers, can be a good prognostic factor to consider when starting a specific ED treatment. In addition, programs aimed at improving communication and trust in the relationship with parents might be promising in the prevention of ED. On the other hand, considering the evaluation of BD at the beginning of the psychological and/or psychiatric intervention with adolescents, especially when suspected ED, could determine an early intervention to improve the adolescents’ body image.
This work invites to include, as a psychotherapeutic objective in the interventions with adolescents suffering from ED, the intervention on attachment, emphasising the improvement of communication and trust between parents and children, since this could affect the adolescent body satisfaction. This intervention might contribute to reduce eating psychopathology. Also, this study proposes to manage with feelings of peer alienation that adolescents with ED usually suffer, focusing the therapeutic work in the interpersonal relationship’s improvement.
However, our study has a number of limitations to be considered. The sample has not been selected randomly, it is not an experimental study and the relationships between the variables could be affected by the effect of uncontrolled variables.
Three of the most important limitations of the study refer to sample selection. Firstly, the racial or ethnic variables of the study participants have not been considered. Secondly, we did not collect information about the degree of malnutrition in the ED sample, which could affect their cognitive status. Finally, the only exclusion criteria for selecting the control sample was that the student was receiving psychiatric/psychological treatment. Thus, we excluded adolescents who had mental disorders that would have required psychological/psychiatric attention both in the past and in the present. However, there was not a clinical psychologist in charge of conducting a structured interview to determine if participants met clinical criteria for eating disorders and to exclude them from the control group. That is why, there could be some adolescent who were suffering from an eating pathology at the time of completing the questionnaires. However, we estimate they were the minimum and this would not invalidate the results. Another aspect to be noted is that we have obtained the control sample in public schools. It would have been interesting to have included participants from charter or private schools.
Another limitation of the study is the self-reported measure to assess attachment. This measure directly evaluates the conscious perceptions of other people’s emotions and behaviours but it would not consider the defensive processes that usually occur when the participants talk about their attachment experiences.
Regarding future lines of intervention, we suggest that it would be interesting to evaluate the impact of a specific intervention on parental and peer attachment in adolescents with respect to BD and ED symptomatology. Another proposal would be to carry out a longitudinal study to observe if the attachment style and its relationship with BD remains over time, since the studies carried out to date have been controversial. A meta-analysis by Pinquart et al. (2013) concluded that although short-term stability may be relatively high, long term stability is quite weak.
An interesting line of research would be to evaluate possible gender differences in attachment and BD in adolescents with ED. In our study, there were more girls in the control group than in the ED group. This is due to the higher incidence and prevalence of ED in girls compared with boys (Herpertz-Dahlmann, 2015). It would be recommendable to carry out future research to expand the presence of males with ED. Previous studies with adolescents have provided promising data. For example, Szalai et al. (2017) reported that boys had significantly higher body satisfaction, and worse maternal attachment than girls, who showed worse paternal attachment and higher depression. Higher paternal anxiety and avoidance, and maternal avoidance predicted lower body satisfaction in both genders. A recent meta-analysis (Cortés-García et al., 2019b) highlighted the differential and gender-specific contribution of attachment figures on the development of disordered eating in adolescence. They concluded that positive attachment to parents, primarily mothers, leads to less eating problems. Fathers also seem to be a source of security and comfort among boys who report more disordered eating. However, to our knowledge, there are no studies which evaluate these gender differences in adolescents with ED.
In conclusion, this study highlights that the parental attachment and feelings of alienation that occur with friends could influence the degree of body dissatisfaction in adolescents with ED. Therefore, adequate communication and trust with parents, and a low degree of adolescent alienation with their parents and friends might contribute to create an adequate body satisfaction and to prevent the development of an ED.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.