
Abstract
Past research has identified shifts in the demographics and co-occurring mental health issues of youth referred to certain gender dysphoria services. The present study examined shifts in demographics (age, sex and social transition status), social adversity (bullying experiences and abuse) and psychological functioning (mood, anxiety, suicidality and autism spectrum disorder) at time of referral (of both children and adolescents) to the Gender Identity Development Service, London between the years of 2012 and 2015. Patients were 782 children and adolescents (M = 13.94, SD = 2.94, range 4–17; 63.8% assigned female at birth). Little change in sex ratio or age was observed between these two time points. However, we observed greater rates of depression and anxiety of birth-assigned females (but not birth-assigned males) in the more recent cohort, at the same time that reported social adversity (bullying and abuse) was falling. Also, of interest, the proportion of young people who had partially or fully socially transitioned prior to contact with the service had increased overtime. We discuss potential factors driving these shifts and their implications for supporting recent cohorts of gender diverse young people.
There has been a surge in the number of children and adolescents referred to gender identity services in recent years. For instance, youth referrals to the Gender Identity Development Service (GIDS) in London, UK increased by ∼2500% between 2009 (n = 97) and 2017 (n = 2519) (de Graaf et al., 2018c). A similar increase in the number of youth referrals has been observed as far afield as North America (Aitken et al., 2015) and Australia (Telfer and Ikeda, 2017). At the same time, there is evidence of a shift in the demographics of those referred. Perhaps the most well-documented shift is in the sex ratio of adolescent referrals. Whereas historically birth-assigned males made up the bulk of adolescent referrals to gender identity clinics, there is evidence from multiple sites that birth-assigned females now predominate (Aitken et al., 2015; de Graaf et al., 2018a; Meyenburg et al., 2021; Kaltiala et al., 2020). For instance, Aitken, Steensma, et al., (Aitken et al., 2015) reporting on adolescent referrals to the Gender Identity Service in Toronto, Canada, found that whereas birth-assigned male referrals outnumbered birth-assigned female referrals (67.9% vs. 32.1%) in the period 1999–2005, birth-assigned female referrals outnumbered birth-assigned male referrals in the period 2006–2013 (66.2% vs. 33.8%). A similar pattern was observed at the Centre of Expertise on Gender Dysphoria at the VU University Medical Center in Amsterdam, where birth-assigned males were more prevalent than birth-assigned females (58.6% vs. 41.1%) for the period 1989 to 2005, but less prevalent (36.7% vs. 63.3%) for the more recent period 2006 to 2013.
At present, it is unclear what accounts for the surge in adolescent referrals to gender identity services, and why adolescent referrals are now predominately birth-assigned females. One explanation is that with increasing societal acceptance of transgender folk, transgender adolescents are more readily acknowledging and seeking assistance for their gender dysphoria. However, this fails to explain why birth-assigned females are now coming forward in disproportionate numbers. Some have suggested that the recent preponderance of adolescent birth-assigned females reflects the emergence of a new type of gender dysphoria or a new developmental pathway to gender dysphoria predominately impacting birth-assigned females (Kaltiala-Heino et al., 2015). If this new cohort of transgender teens is experiencing gender dysphoria via a distinct development pathway, it might likewise require a unique treatment approach.
Recent data suggests that these shifts might not be restricted to adolescents – but seem to be occurring among pre-pubescent children as well. At the Amsterdam clinic, data indicates that starting in the mid-2000s, the sex ratio favouring birth-assigned male children changed to relative parity or to one favouring birth-assigned female children (de Graaf et al., 2018a). Showing a similar trend, recent data from the GIDS, London, found that whereas birth-assigned male children outnumbered birth-assigned female children every year from 2009 to 2015, birth-assigned females surpassed birth-assigned males in 2016 (de Graaf et al., 2018c). These trends however were not observed at the Toronto Clinic, with child referrals still favouring birth-assigned males (de Graaf et al., 2018a) suggesting this shift is not universal and that more data is needed on this age group.
In addition to shifts in sex ratio, authors have noted other clinically significant changes among child and adolescent referrals. One such change is the increased proportion of referrals who have socially transitioned prior to first contact with gender services. Steensma and Collen-Kettenis (Steensma & Cohen-Kettenis, 2011) reported that before the year 2000, only 1.7% of pre-pubertal boys and 3.3% of pre-pubertal girls had fully socially transitioned prior to initial contact with the Amsterdam clinic (i.e. had changed their clothing, hairstyle, name and pronouns to match their gender identity). Between 2005 and 2009 this had increased to 8.9% of referrals having fully socially transitioned (and 33.3% having partially transitioned) prior to contact with the service. As there is some evidence that social transition is associated with greater stability of transgender identities – this trend might be relevant to the long term outcomes for gender dysphoric youth (Steensma et al., 2013). We are not aware of more recent work documenting shifts in prevalence of childhood social transition specifically; however, a study pooling data on child and adolescent referrals (all paediatric referrals to the GIDS, London, from 2012–2013) reported that 54.6% were living in their chosen gender full-time at time of assessment (Holt et al., 2016). As such it seems that the trend toward social transition before contact with specialist services is increasing dramatically – with potential clinical consequences.
It is well established that gender dysphoria in children and adolescents is associated with a range of psychological difficulties (Bechard et al., 2017; Holt et al., 2016; Spack et al., 2012). For instance, based on initial assessments with paediatric referrals to the GIDS, London, 39.4% reported mood disorders, 21% anxiety disorders, 32.8% reported suicidal ideation, 12.3% suicide attempts, and 26% reported engaging in self-harm (Holt et al., 2016). A recent study examined psychological functioning in adolescents in four specialist gender identity clinics across Europe on standardised measures (de Graaf et al., 2018b). On the Child Behaviour Checklist (CBCL), this study found that between 44 and 67% of youths demonstrated internalising problems within the clinical range, and between 21 and 37% of youths demonstrated externalising problems within the clinical range. Notably, birth-assigned females reported more total problems in the clinical range than birth-assigned males. Exactly why this is the case is still unclear – and is the subject of current debate within the literature. One possibility is that as birth-assigned females reach puberty sooner, they will have experienced a more protracted period of anatomic gender dysphoria (distress related to changes in their body brought about by puberty) than their male counterparts by assessment. Another possibility is that birth-assigned females might be more likely than birth-assigned males, to experience gender dysphoria in the context of complex psychiatric presentations (Kaltiala-Heino et al., 2015).
There is some reason to suspect that recent cultural shifts in acceptance and visibility of transgender youth might be influencing the psychological functioning of referrals to gender clinics. On the one hand, given that experiencing stigma and discrimination related to being transgender or gender non-conforming is a reliable predictor of psychological difficulties (Hendricks & Testa, 2012), and given some indication of a reduction in this stigma of late, recent referrals to gender services might be expected to demonstrate superior functioning to those in the past. Moreover, with greater awareness and acceptance of transgender youth and greater access to specialist gender services, it is possible that youths may be presenting with lower intensities of gender dysphoria (than observed in the past). On the other hand, as access to medical treatment options for gender dysphoric youth has become more accessible, gender clinics might be seeing an influx of children and adolescents from less privileged or supportive families, that could be linked to poorer psychological functioning (Arnoldussen et al., 2020).
To this point, only two studies have examined whether there have been shifts in the psychological functioning of referrals to paediatric gender dysphoria clinics over time. Chiniara, Bonifacio (Chiniara et al., 2018) comparing psychological functioning of n = 203 referrals (aged 12–18) between 2014 and 2016 found no significant change in chart-reported mental health history or Beck Depression Inventory of referrals over the 2.5-year period. In a recent study of n = 1072 adolescent GD referrals (aged 10–18) to the Amsterdam clinic between 2000 and 2016, Arnoldussen, Steensma (Arnoldussen et al., 2020) found that psychological functioning of referrals had improved overtime. Specifically, recent adolescent referrals demonstrated fewer externalising problems on the CBCL and improved peer relations on the Youth Self Report (YSR) scale compared to referrals in earlier years. Given the mixed evidence to date, more data is required from other paediatric gender identity clinics, before a clear picture of shifts (or lack there-of) in psychiatric co-morbidities among GD referrals can be attained.
The present study examined shifts in demographics (age, sex and social transition status), social adversity (bullying experiences and abuse) and psychological functioning (mood, anxiety, suicidality and ASD) of a subset of paediatric referrals (both children and adolescents) to the Gender Identity Development Service, London between the years of 2012 and 2015. In doing so, we aimed to provide clinically relevant information regarding potential changes in the types of patients referred to specialist gender clinics in recent years. This information is critical to understanding and responding to patient needs – and also to determining whether psychosocial and medical treatments found to be effective in reducing distress in paediatric GD referrals of years past – can be generalised to recent referrals.
Methods
Participants
Participants were drawn from a sample of 782 children and adolescents (M = 13.94, SD = 2.94, range 4–17) who were referred to the Gender Identity Development Service (GIDS) during 2012 (n = 218 [83% of overall n = 263 referrals]) and 2015 (n = 564 [48% of overall n = 1162 referrals]) and for whom an Associated Difficulties form (Holt et al., 2016) was completed following assessment. Patients’ who completed the Associated Difficulties form necessarily represent a subsample of the larger pool of referrals referred to the GIDS in 2012 (n = 265) and 2015 (n = 1162) as reported in de Graaf et al., 2018b. This is because the Associated Difficulties form was completed post-assessment – and a proportion of referrals dropout during the assessment phase. Additionally, some data are missing due to clinicians failing to complete the Associated Difficulties form post-assessment or the form being misplaced (clinician/researcher error).
To determine whether the subsample of referrals with completed Associated Difficulties forms was representative of the broader sample referred to GIDS during 2012 and 2015 (see de Graaf et al., 2018a), we compared each sample on available demographics (age; child vs. adolescent status). A chi-square test found that the present sample (those who had completed Associated Difficulties data) and the total referral pool failed differ with regard to the proportion of adolescent birth-assigned males, adolescent birth-assigned females, child-birth-assigned males or child-birth-assigned females, in either 2012 or 2015 (χ2 (9) = 7.048, p = .632). We think it is unlikely therefore that findings relating to variables in our study (i.e. social transition status, name change status, mood, anxiety, suicide attempts, bullying, abuse and ASD) will differ systematically between our sample and the broader set of referrals, although this does remain a possibility. It does mean however that shifts reported in composition of birth-assigned males versus females, and adolescents versus children, are representative of those observed in the total referral pool.
Shifts in demographics among birth-assigned males and females for 2012 versus 2015.
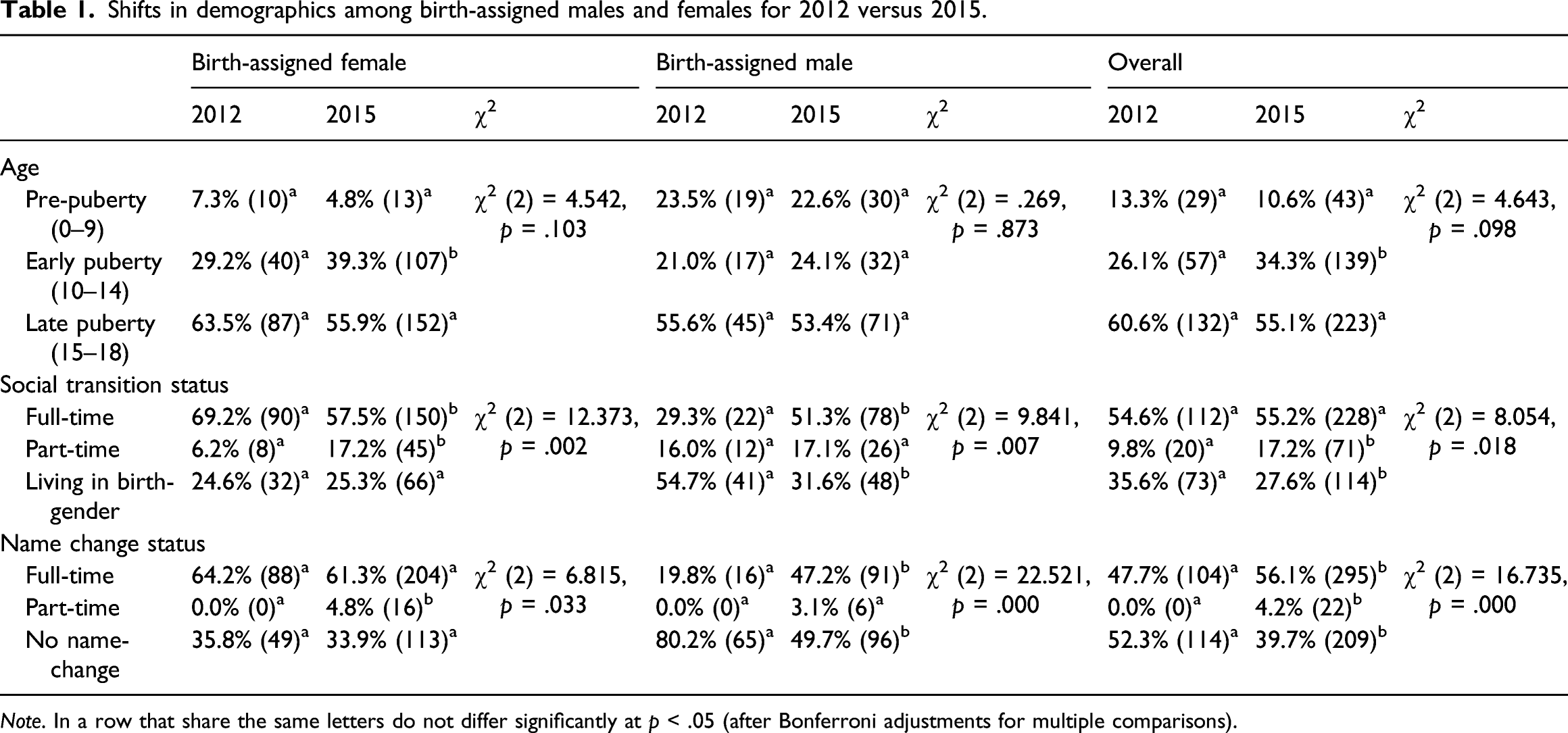
Note. In a row that share the same letters do not differ significantly at p < .05 (after Bonferroni adjustments for multiple comparisons).
Procedure
Upon first contact with the GIDS, patients and their families undertook in-depth assessment of gender dysphoria, co-morbid psychological disorders and relevant psychosocial stressors. These assessments involved a minimum of three, one-hour assessments, with two mental health clinicians (who were either psychiatrists, clinical psychologists or registered psychotherapists). Assessment sessions involved both child/adolescent patients and their families, assessed individually and together as a family. At the end of the assessment period, the Associated Difficulties form was completed by both mental health clinicians (i.e. clinicians conferred with one another to ensure agreement on diagnoses). Referral letters and clinician reports referencing mental health functioning prior to contact with the GIDS were also taken into account in making these judgements.
The Associated Difficulties form involved 25 questions relevant to demographics, psychosocial stressors and DSM-V diagnoses. These questions are outlined in detail in a past study from our service using these data (Holt et al., 2016). In the present study, we examined data on 10 variables from the Associated Difficulties form: birth-assigned gender, age at time of referral, social transition (no, partly, fully), name change (no, partly, fully), presence of current mood and anxiety difficulties at time of assessment, autism spectrum disorder, past suicide attempts and presence of bullying or abuse in the past 12 months. Mood difficulties reflected a full diagnosis of a DSM-5 Depressive disorder (e.g. Major Depressive Disorder or Persistent Depressive Disorder). Anxiety difficulties reflected a full diagnosis of a DSM-5 Anxiety disorder (e.g. Social Anxiety Disorder, Panic Disorder and Generalised Anxiety Disorder). Autism Spectrum Disorder reflected the presence of a formal diagnosis as per DSM-V. All data were anonymised in order to ensure the confidentiality of participants.
Measures
Demographic variables of interest included birth-assigned sex, age at referral, and two variables relevant to social transition status, name change and living in role. Age at referral was coded into three age groups: 0–9, 10–14 and 15–18 years old to delineate pre-pubescent, early pubescent and late pubescent developmental stages (this is a coarse estimate of puberty rather than an exact one due to individual differences). Living in role, which referred to whether young people were currently living in their preferred gender role (e.g. adopting gender markers including clothes and hair styles of their felt gender), was divided into fulltime, part-time and not living in role. Name change, which referred to whether young people had adopted a name and pronouns congruent with their felt gender, was divided into yes (full-time), partly (part-time) and no (had not adopted a new name). Mental health difficulties (mood, anxiety, suicide attempts and autism-spectrum-disorder) and other associated difficulties (bullying, family abuse) were all assessed as either present or absent in the past 12 months by clinicians.
Data analytic plan
To examine shifts in demographics and associated-difficulties experienced by young people who presented in 2012 versus 2015 we applied chi-square goodness-of-fit tests. In each analysis, we examined whether shifts occurred in the frequency of the variable of interest between 2012 and 2015, in birth-assigned females and males separately, as well as in both groups combined. Where the chi-square omnibus test was significant, we undertook binomial follow-up tests to identify exactly which variables differed between 2012 and 2015.
There were some missing data on variables within our dataset. Of 782 data points, n = 629 included participant age; n = 648 included living in role; n = 776 included name change; n = 772 included a mood evaluation; n = 771 included an anxiety evaluation; n = 769 included information on suicide attempts; n = 774 included information on bullying; n = 772 included information on abuse history; and n = 743 included information on ASD. Listwise deletion was not employed–rather we analysed all patient data on relevant variables.
Results
Changing trends in demographics
Sex
We failed to find evidence of a shift in the sex ratio of birth-assigned male to birth-assigned female referrals between 2012 and 2015. A chi-square goodness of fit omnibus test comparing proportion of assigned male at birth and assigned female at birth referrals in 2012–2015 was non-significant X2 (1, N = 748) = .002, p = .964.
Age
Table 1 reports the age at referral, social transition status and name change status of birth-assigned females and birth-assigned males, who presented to the GIDS in 2012 and 2015. The chi-square goodness of fit omnibus test on age at referral revealed a suggestive shift in the proportion of pre-pubescent, early pubescent and late pubescent referrals (p < .10). Binomial follow-up tests revealed that overall, there was an increase in the proportion of early pubescent referrals from 2012 to 2015 – however, further inspection revealed that this was occurring only among birth-assigned females, but not birth assigned-males.
Social transition status
With regards to social transition status, we observed significant chi-square omnibus tests for birth-assigned females, birth-assigned males and overall. Binomial follow-up tests revealed a slight, yet significant reduction in the number of birth-assigned females who had fully socially transitioned, and a significant three-fold increase in the proportion of birth-assigned females who presented having partly socially transitioned, between 2012 and 2015. Bucking this trend, among birth-assigned males, there was an almost doubling in the proportion who had fully socially transitioned prior to presentation – and no shift in the proportion of those who had partly socially transitioned. Across both groups combined, a reduction in the proportion of referrals who had not socially transitioned prior to contact with GIDS was observed from 2012 to 2015.
Mirroring those findings for social transition, significant chi-square omnibus tests were observed for name change between 2012 and 2015 for birth-assigned female and males as well as for both groups combined. Among birth-assigned females there was a significant increase in the proportion of those reporting a part-time name change. In birth-assigned males, there was a dramatic increase in the prevalence of full-time name change, and a reduction in those who had not adopted a gender-congruent name, between 2012 and 2015. When groups were combined, a significant increase in the prevalence of full-time and part-time name change was observed, with a concomitant reduction in the proportion of young people retaining their birth name.
Changing trends in mental health and associated difficulties
Shifts in associated difficulties among birth-assigned males and females for 2012 versus 2015.
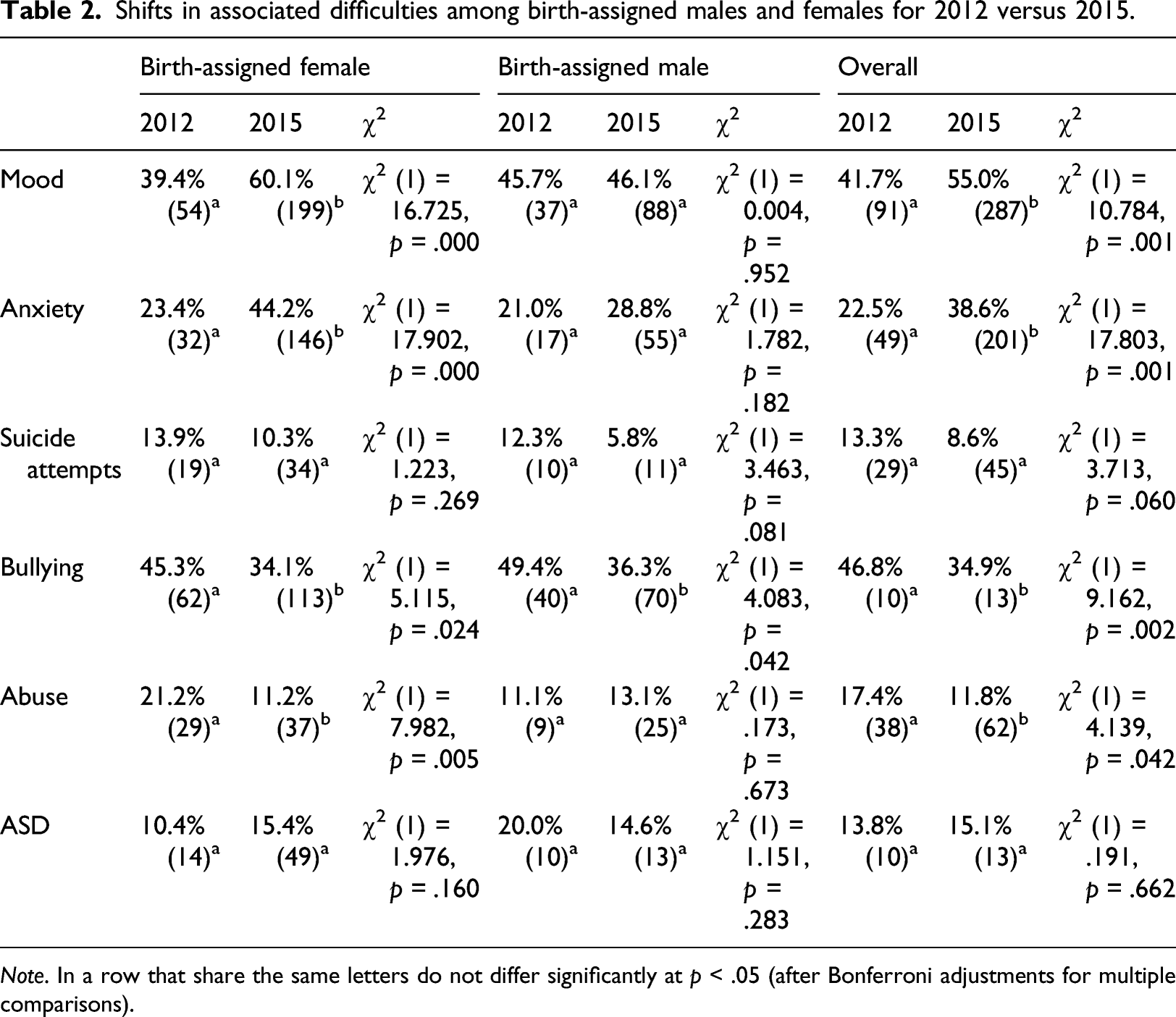
Note. In a row that share the same letters do not differ significantly at p < .05 (after Bonferroni adjustments for multiple comparisons).
Discussion
The present study is amongst the first to examine shifts in demographics and psychological functioning among children and adolescents referred to a specialist gender dysphoric clinic. A number of clinically important trends were observed. First, we found a significant increase in mood difficulties and anxiety among birth-assigned females, but not birth-assigned males, between 2012 and 2015. This is the first indication of poorer psychological functioning in recent cohorts of child and adolescent referrals – and contrasts with past findings of no change (Chiniara et al., 2018) or a reduction in psychiatric co-morbidities in this population (Arnoldussen et al., 2020). It is possible that differences in the assessment of mental health between studies may partly account for discrepant findings. In this study, mental health was clinician rated (unlike in the previous two which were self-report) and was assessed in terms of the presence or absence of psychological disorders (unlike the past two studies which deployed standardised measures of psychological functioning). Arguably, our study would have been less sensitive to differences in psychological functioning outside of the clinical range – and this may account for our failure to detect any change in psychological functioning in birth-assigned males over time. However, this does not explain our finding of poorer well-being in more recent cohorts of birth-assigned females. It is possible that this finding reflects the worsening rates of emotional difficulties among birth-assigned females in recent years, regardless of gender identity (Sadler et al., 2017). It is also possible that we may need to consider whether shifts in the psychological functioning of youth referrals to GD services are culture or referral site specific. Whereas Arnoldussen et al., 2020 and Chiniara et al., 2018 drew on data from the Dutch and Toronto clinics, respectively, our data were the from the Tavistock Hospital, London. It possible that recent youth referrals to the Tavistock differ in some ways from those referred to the Dutch and Toronto clinics (e.g. socioeconomic status). Future research may compare relevant referral characteristics across GD clinics to identify factors driving these differences.
Another question which begs explanation is why the increase in psychiatric morbidity between 2012 and 2015 was specific to birth-assigned females. It is possible that this effect is part of a more general increase in mental health problems observed in adolescent birth-assigned females in recent years – which may be related to increasing stressors on birth-assigned females such as cyberbullying and problems related to social media use (Viner et al., 2019).
Given that mental health problems appeared to be increasing in birth-assigned female referrals, it is surprising to observe that the prevalence of reported bullying and abuse has decreased among birth-assigned females over the same period. The reduction in bullying and abuse might reflect increasing visibility and tolerance of transgender people in society, and of transgender children and youth more specifically (Steinmetz, 2017). It might also reflect the successful implementation of school-based policies to support transgender students and facilitate safe social transition (Mitchell et al., 2014). These findings provide cause for optimism regarding improving social conditions for transgender young people in the UK. However, it should be noted that although a reduction in bullying was observed among birth-assigned males – this was not accompanied by a reduction in abuse. The cause of this discrepancy is unclear at present – however, it might be that peer-based bullying has reduced (due to improving attitudes to gender diversity in younger people) – whereas family or carer-based abuse remains unchanged at this point.
We observed very little shift in the demographics of referrals between 2012 and 2015, contrasting with shifts observed in other recent studies, for example, (Aitken et al., 2015; de Graaf et al., 2018b). There was no change in the sex ratio of referrals–suggesting that either the dramatic shift in the proportion of birth-assigned female to birth-assigned male GD referrals demonstrated in past research (Aitken et al., 2015) has stabilised in recent years, or that shifts in the UK do not mirror those reported at clinics in North America and the Netherlands. Likewise, there was little shift in the age of referrals. For each birth-assigned sex, most referrals were between 15–18 years of age (>50%). In birth-assigned females, but not birth-assigned males, it appeared there had been a slight increase in the proportion of 10–14-year-olds between 2012 and 2015. This might reflect both earlier onset of puberty in birth-assigned females (than birth-assigned males) coupled with increasing awareness of transgender phenomena among young people. Next, although the co-occurrence of Autism Spectrum Disorders (ASD) and gender dysphoria in youth is well established (Cohen-Kettenis, 2018), we found no evidence that this association was increasing over time (the proportion of referrals with ASD may have stabilised between 2012 and 2015 at ∼15%).
Finally, we found that the proportion of birth-assigned males who had socially transitioned prior to presentation at our service increased between 2012 (19.8%) and 2015 (47.2%). This may reflect increasing acceptance and visibility of gender diverse birth-assigned males over this period. In birth-assigned females, on the other hand, there was a slight reduction in the proportion of birth-assigned females presenting fully socially transitioned, and an increase in those who had partly socially transitioned. It is possible this shift is related to the increasing proportion of early adolescent birth-assigned females observed between 2012 and 2015 (i.e. birth-assigned females are now presenting to treatment slightly earlier). Shifts in the prevalence of social transition prior to first contact with specialist services are significant in light of research which finds that early social transition is associated with the trajectory of a child’s gender dysphoria (Steensma et al., 2013). These findings require that clinicians are knowledgeable of stressors related to social transition (e.g. concerns related to passing, using gender segregated spaces like change rooms or toilets) and factor these into psychological formulation and treatment.
A notable limitation of the present study is that we did not have Associated Difficulties data on all referrals the GIDS in 2012 and 2015. As a result, it possible that shifts observed in our subsample of patients for whom Associated Difficulties data is available are not representative of the broader pool of referrals to the service, on some relevant variables. Future studies should attempt to collect data on all patients who are referred to service, including those who drop out of treatment during the assessment phase, to ensure findings are representative of trends in the broader population accessing specialist Gender Services. That being said, given that our sample did not differ systematically from the larger referral pool on relevant demographics, we argue it is unlikely that trends reported in this study are artefacts of the subsample of patients for whom Associated Difficulties data were available.
Conclusion
In recent years, there has been some evidence of a shift in the type of young person referred to specialist gender clinics, for example, (Aitken et al., 2015; de Graaf, et al., 2018b). In some sense, gender dysphoric youth appear to be a moving target, and it is incumbent on researchers and clinicians to keep abreast of exactly who their paediatric patients are, so that they can target treatment accordingly. The present study found little change in the demographics of those referred to the Tavistock Gender Identity Development Service in 2012 and 2015. However, some important changes were observed in the mental health and social transition status of more recent referrals. Specifically, there has been an increase in the psychiatric morbidity of birth-assigned female (but not birth-assigned male) referrals in recent years, at the same time that reported bullying and abuse appear to be decreasing. These findings provide snapshot of recent demographic and mental health trends among gender dysphoric youth and may have implications for research and clinical work with this population. Future research should examine if the trends observed in the present study are also evident in gender clinics in continental Europe, North America, Australia/New Zealand, as well as non-Western nations.
Footnotes
Acknowledgements
We would like to thank Michael Dunsford at the Tavistock and Portman Gender Identity Development Service (GIDS) for developing the Associated Difficulties assessment form.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and material
Data available upon request code availability: Descriptive statistics (syntax available on upon request).
Author biographies
James S. Morandini, School of Psychology, The University of Sydney, Australia
Aidan Kelly, Tavistock and Portman Gender Identity Development Service (GIDS), London, UK
Nastasja de Graaf, VU University Medical Center, Amsterdam, NL; The University of Sydney, Australia
Ilan Dar-Nimrod, School of Psychology, The University of Sydney, Australia
Polly Carmichael, Tavistock and Portman Gender Identity Development Service (GIDS), London, UK.