
Abstract
In a growing body of literature, poor sleep quality has been associated with externalizing problems. In adults, anxiety was found to mediate the relationship, and callous-unemotional (CU) traits were found to moderate it. We sought to examine these relationships in a child population. We examined these relationships in 239 clinic-referred youth (age 6–17) in Singapore with externalizing behavior problems. Parent- but not child-rated sleep problems were associated with increased parent-rated externalizing problems. This association was partially mediated by anxiety. Unlike in adults, CU traits did not moderate the relationship. Sleep problems were associated with externalizing problems regardless of the level of CU traits. It is possible externalizing behaviors may lead children to internalize experiences, leading to anxiety about their behaviors. Another possibility is externalizing behaviors may lead to more stressful life experiences due to negative reactions children with externalizing behaviors receive from parents, teachers, or peers. Regardless, the partial mediation found indicates anxiety may be an important factor to consider in future interventions focused on improving sleep as a means to reduce externalizing problems.
Keywords
There has been a growing interest in the relationship between externalizing behaviors and sleep problems. Externalizing behaviors, including general antisocial behaviors like rule-breaking, stealing, cheating, and physical aggression, have been associated with poor sleep quality (Barclay et al., 2011; Roth et al., 2006; Semiz et al., 2008). While the nature of this relationship is still being explored, it is important to investigate factors that could explain how sleep and externalizing behaviors are associated. Two such possible factors are anxiety and callous-unemotional traits. Both of these factors have been associated with externalizing behaviors and sleep problems. We will analyze the former as a mediator and the latter as a moderator in this study.
Researchers have found poor sleep quality is associated with externalizing behaviors, including aggression. In an adult sample, individuals with Antisocial Personality Disorder (ASPD) were more likely to experience poor sleep quality on a variety of metrics, including lower subjective sleep quality, shorter duration of sleep, and more sleep disturbances than healthy controls (Semiz et al., 2008). In a sample of 9282 adult community members, Roth et al. (2006) found significant comorbidity between impulse control disorders, like Conduct Disorder (CD) and Attention-Deficit/Hyperactivity Disorder (ADHD), and sleep problems. Researchers have also studied the relationship between sleep quality and externalizing problems in children. In a non-referred sample of youth ages 12–19, poor sleep quality has been associated with externalizing behaviors (Barclay et al., 2011). In a study using actigraphy in children ages 7–12, Aronen et al. (2000) found externalizing behaviors were associated with several indicators of sleep quality, with the strongest association observed for low sleep time (amount of sleep). In a longitudinal study, Gregory and O'Connor (2002) measured sleep problems and behavioral problems using the Child Behavior Checklist (CBCL), a parent-report scale, at age four and then later in mid-adolescence (ages 13–15). They found sleep problems measured at age four predicted behavior problems in mid-adolescence.
Anxiety may be worth examining as a mediator of the relationship between externalizing problems and sleep problems, as it is associated with both externalizing problems and sleep problems. In several studies of youth, anxiety has been associated with poor sleep quality (Alfano et al., 2006; Chase & Pincus, 2011; Hudson et al., 2009; Schlarb et al., 2016). In a study using retrospective chart reviews of children aged 6–17 years, Alfano et al. (2006) found, in parents of children with anxiety disorders, 83% reported their child had at least one sleep complaint. Using the CBCL, Johnson et al. (2000) found parents who reported their children had sleep problems were significantly more likely to report symptoms of anxiety/depression on the same scale. In another study using the CBCL to measure parent-reported sleep problems, Chase and Pincus (2011) examined the relationship between anxiety and sleep problems in children with anxiety disorders. In this sample, they found 90% of children exhibited at least one sleep problem, and 82% exhibited two or more sleep problems (Chase & Pincus, 2011).
Additionally, externalizing behaviors have been found to co-occur with anxiety in youth (Polier et al., 2012; Stalk et al., 2015). In a study of non-referred children age 9–16, Rowe et al. (2005) found significant comorbidity between CD (of which several symptoms can be classified as externalizing behaviors) and anxiety disorders. Similarly, in a clinical sample of children with a mean age of 10.7 years, Greene et al. (2002) found a 42% comorbidity rate between CD and anxiety disorders. These studies and several others have served to demonstrate comorbidity between externalizing problems (often operationalized as CD) and anxiety. Additionally, some children with conduct problems have been found to have heightened brain responses to fear stimuli presented outside of conscious awareness, suggesting a hypervigilance to possible threat, which may disrupt sleep (Viding et al., 2012). Thus, anxiety may be a potential mediator of the relationship between externalizing problems and poor sleep.
It has been hypothesized that individuals with high levels of callous-unemotional (CU) traits, who may be less prone to anxiety, may not have the sleep disturbances observed in individuals with externalizing problems without CU traits (Gregory & Sadeh, 2016). In the previously mentioned study suggesting children with conduct problems are more likely to have sleep problems due to hypervigilance to possible threat (Viding et al., 2012), this effect was only observed in children with conduct problems with low levels of CU traits. Other studies have also shown those with high levels of CU traits appear less reactive to threat, and because of this, they may have fewer sleep problems (Lozier et al., 2014; White et al., 2012). Thus, it seems CU traits may moderate the relationship between sleep quality and externalizing problems such that sleep problems are only present in youth with externalizing problems and low levels of CU traits.
Denis et al. (2017) recently examined the role of anxiety and CU traits in the relationship between externalizing problems and sleep quality in an adult population. They found the relationship between self-reported sleep quality and externalizing behavior was partially mediated by anxiety. They also found CU traits moderated the relationship between externalizing behavior and sleep quality; the relationship between externalizing problems and sleep quality was stronger in participants who were low in CU traits, as hypothesized by Gregory and Sadeh (2016).
It is especially important to expand the literature in this area to youth populations, as sleep patterns in this group are fundamentally different from those of adults. On a general level, school-age children need 9–11 hours of sleep, and adolescents need 8.5–9.5 hours of sleep, while adults only need 7–9 hours of sleep per night (Meltzer & McLaughlin Crabtree, 2015). Furthermore, from school age to adolescence, amount of sleep needed decreases (Meltzer & McLaughlin Crabtree, 2015). However, for adolescents, there is a delay in circadian phase, which has been shown to decrease total sleep time (Carskadon, 2002). This, combined with other factors such as increased homework requirements, extracurricular activities, part-time jobs, and earlier school start times lead to a pattern of adolescents getting less than the recommended amount of sleep (Carskadon, 2002). For these reasons, it is unknown if findings in studies of adults concerning relationships between anxiety, CU traits, externalizing problems, and sleep problems would generalize to youth populations. If such relationships do exist in youth populations, a greater understanding of the nature of these relationships could shed light on childhood factors that contribute to the development of externalizing/antisocial behaviors in adulthood.
To date, no study has examined the influence of anxiety and CU traits on the relationship between sleep problems and externalizing behavior in youth. The goal of the present study was to assess replicability of the findings of Denis et al. (2017) in a youth sample. Based on the Denis et al. (2017) study, as well as previous literature, we hypothesized: (1) there would be a positive association between sleep problems and externalizing behavior, (2) this relationship would be mediated by anxiety, and (3) this relationship would be moderated by CU traits such that the relationship between externalizing behavior and sleep problems would be stronger for youth with low levels of CU traits.
Methods
Participants and procedures
Data analyzed for the present study were pre-screen and baseline scores derived from a randomized, placebo-controlled trial (RCT) of a nutritional and social skills intervention among children with ADHD, Oppositional Defiant Disorder (ODD), and/or CD recruited from a tertiary outpatient child psychiatric clinic in Singapore. The RCT study was approved by both institutional and hospital group ethics review boards (DSRB A/08/410; CRC 240/2008). All participants and their parents provided informed consent. All participants had previously received an ADHD, ODD, and/or CD diagnosis from a licensed clinician based on ICD-9 (World Health Organization, 1977) and DSM-IV-TR (American Psychiatric Association[APA], 2000) criteria. These children were included in the RCT study if they fulfilled the following inclusion criteria conducted at pre-screening: (a) 7–16 years old; (b) had a clinical diagnosis of ADHD or ODD/CD by the DSM-IV-TR criteria (APA, 2000), (c) met the criteria of ADHD, ODD/CD or both based on the parent version of the Diagnostic Interview Schedule for Children (C-DISC) (Shaffer et al., 2000) and (d) IQ of 70 and above. The C-DISC interview was administered by trained Research Assistants using a laptop computer, and the results were reviewed by the Principal Investigator and clinicians who were part of the study team. Those with serious brain pathology, such as epilepsy, were excluded. Subsequently, children and parents were asked to complete questionnaires (see Measures) at the outpatient clinic prior to the start of the RCT study (i.e., study visits at either pre-screen or baseline). In the present study, data from 239 children between 7 and 16 years (M = 10.60 years, SD = 1.91) were included and analyzed.
One participant was removed because Externalizing problems on the CBCL were more than three SD above the mean. Participants (n = 239, 88.3% male) ranged in age from 7 to 16 (M = 10.50, SD = 1.83). Rates of diagnoses were as follows: 33.9% (ADHD only), 11.3% (CD), and 54.8% (both ADHD and CD). Level of sleep problems did not significantly differ by diagnosis (F(2,245) = .720, p = .488). As might be expected, level of externalizing problems did significantly differ in children with different diagnoses (F(2,239) = 18.808, p < .001). The mean externalizing score was 13.44 for children with ADHD alone, 19.29 for children with CD alone, and 20.82 for children with ADHD and CD. The sample was 81.6% Chinese ethnicity, 6.7% Malay, 8.4% Indian, and 3.3% Other. 147 participants (61.3%) reported taking stimulant medication, and three participants (1.3%) reported taking SSRIs.
Measures
The School Sleep Habits Survey (Shahid et al., 2011) is a 63-item self-report survey completed by the child measuring total sleep time, bedtime, and wake time over the past 2 weeks. It also has a sleepiness subscale, a sleep/wake problems subscale, and a depressive mood scale. The sleepiness subscale contains 10 items asking whether the child struggled to stay awake in various settings over the 2-week period. The sleep/wake problems subscale contains 15 items asking about behaviors indicative of inconsistent sleep/wake times over the 2-week period (i.e., being late to school because you overslept, difficulty falling asleep). The depressive mood subscale contains six items rated on a three-point scale (not at all, somewhat, much), asking how much various situations over the 2-week period negatively affected the child’s mood (Shahid et al., 2011; Wolfson & Carskadon, 1998). Only 128 participants completed this scale.
The Antisocial Process Screening Device (APSD; Frick & Hare, 2001) is a 20-item questionnaire assessing aggression and antisocial features in children. The APSD consists of three subscales: Callous-Unemotional traits, Narcissism, and Impulsivity. Parents rated their child on each item on a 3-point scale (0 = Not True, 1 = Sometimes True, or 2 = Definitely True). For the present study, only the 6-item Callous-Unemotional traits subscale was included in analyses. This subscale has demonstrated acceptable internal consistency (α = .65–.76), in addition to excellent construct validity (via association with the Psychopathy Checklist-Revised and with DSM criteria for related disorders; Frick et al., 2000; Frick & Hare, 2001).
The CBCL (Achenbach & Rescorla, 2001) is a parent-rated form including 118 items that describe the child’s behavioral, emotional, and social problems over the past 6 months. Parents rated each item on a 3-point scale (0 = Not True, 1 = Somewhat or Sometimes True, 2 = Very True or Often True). Items on the CBCL can be summed up to provide eight “narrow-band” syndromes (Anxious/Depressed, Withdrawn/Depressed, Somatic Complaints, Social Problems, Thought Problems, Attention Problems, Rule-breaking Behavior, and Aggressive Behavior), two “broad-band” syndromes (internalizing and externalizing problems), and a total problems scale (Achenbach & Rescorla, 2001). In the present study, the Externalizing Problems and Anxious/Depressed subscales were used. The CBCL has good test–retest reliability and internal consistency (α = .91; Achenbach & Rescorla, 2001; Tehrani-Doost et al., 2011) and has been used in various societies (Ivanova et al., 2007; Rescorla et al., 2007). The CBCL Externalizing Problems and Anxious/Depressed subscales have demonstrated good test–retest reliability (r = .87 and r = .86, respectively) and inter-rater reliability (r = .67 and r = .77, respectively; Achenbach, 1991). The Anxious/Depressed subscale has been shown to discriminate between youth with and without an anxiety disorder diagnosis (Aschenbrand et al., 2005; Biederman et al., 1993; Edelbrock & Costello, 1988). Additionally, correlations between the subscales of the CBCL are consistent with generally accepted comorbidities (Tehrani-Doost et al., 2011).
The sleep composite of the CBCL was used as a parent rating of overall sleep functioning. This composite consists of seven specific questions from the CBCL, including nightmares, being overtired without good reason, sleeps more/less than most kids, talks/walks in sleep, trouble sleeping, wets the bed. This composite has been shown to be a good measure of overall sleep functioning when compared with other parent-rated measures of sleep functioning (Becker et al., 2015).
Data analysis
Multiple regression was performed to test the hypothesis that externalizing behavior would be associated with sleep problems. The interaction between externalizing behavior and CU traits was added to the model to test whether the relationship between externalizing behavior and sleep problems was moderated by CU traits. Anxiety was examined as a mediator of the relationship between externalizing behavior and sleep problems by using bootstrapped regression, which increases statistical power and does not assume normally distributed data. It was run using the PROCESS macro for SPSS (Hayes, 2013). Anxiety was also examined as a moderator of this relationship. Variables were converted to z-scores prior to conducting these analyses.
Results
Descriptive statistics for study variables.
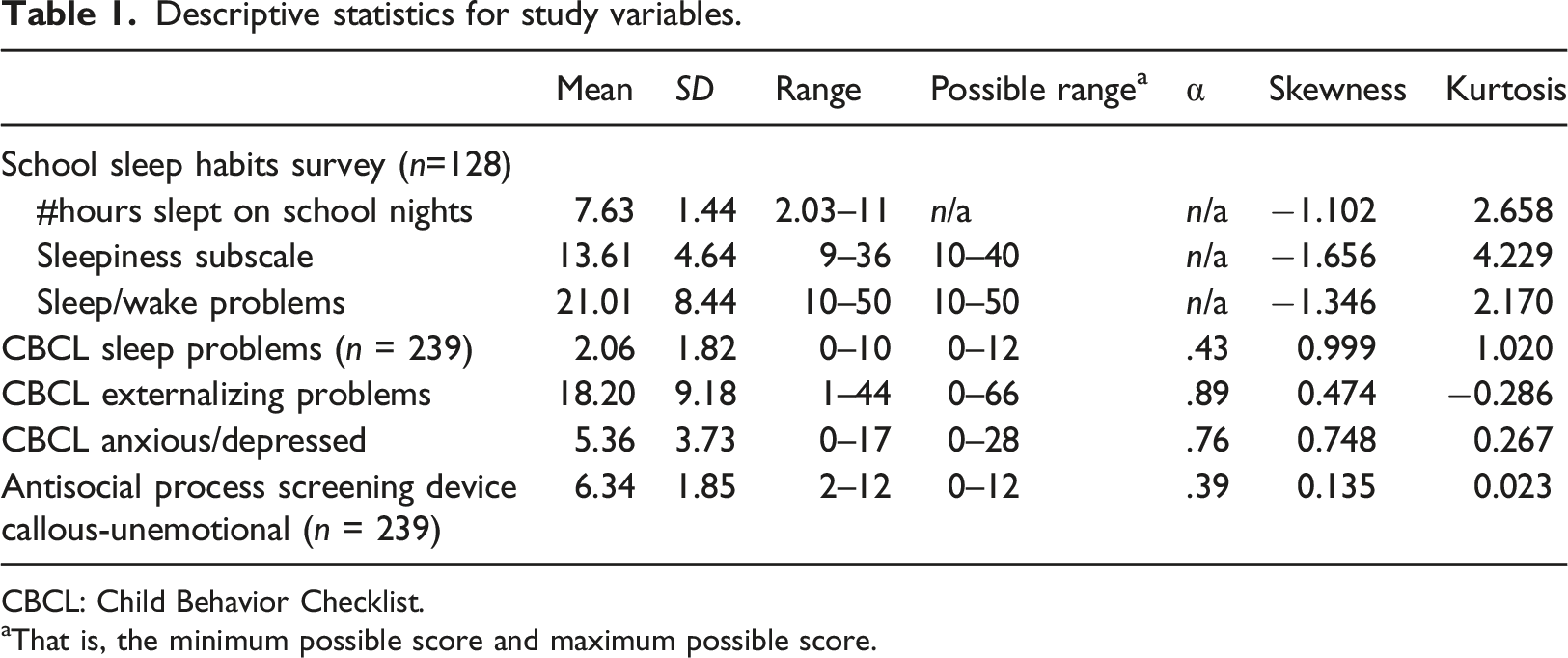
CBCL: Child Behavior Checklist.
aThat is, the minimum possible score and maximum possible score.
Partial correlations (controlling for age) between parent-rated externalizing problems and parent- and child-rated sleep problems.
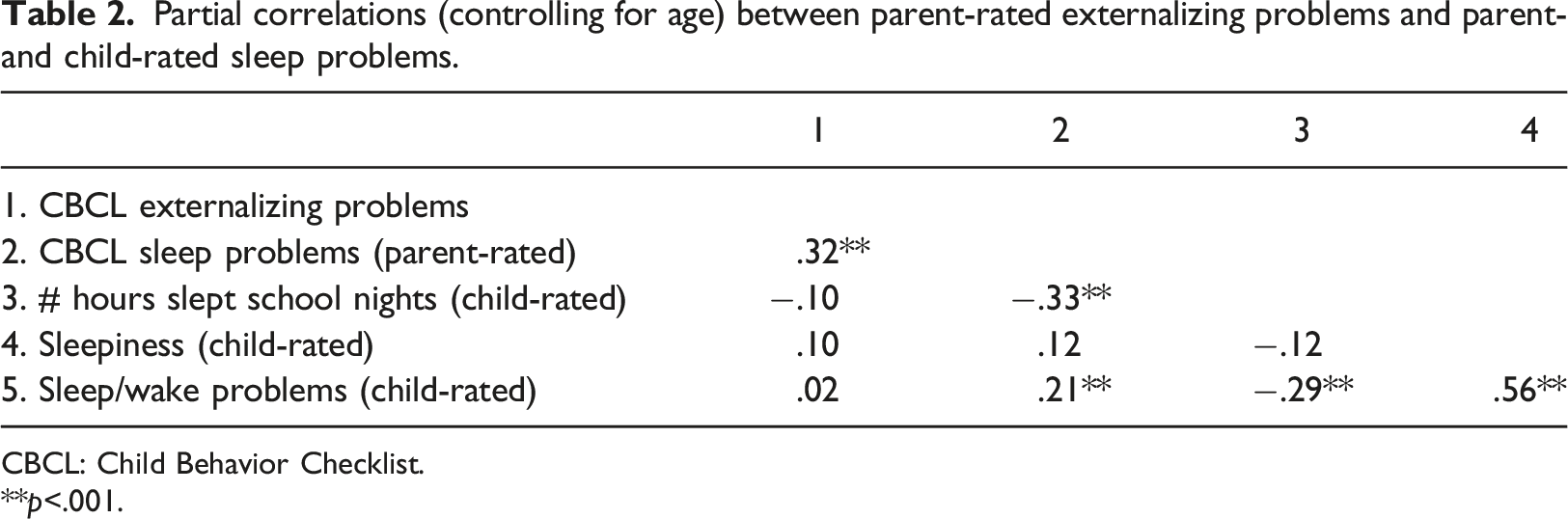
CBCL: Child Behavior Checklist.
**p<.001.
Partial correlations (controlling for age) between key study variables in the current study (Singapore youth sample) compared to correlations from the study by Denis et al. (2017).
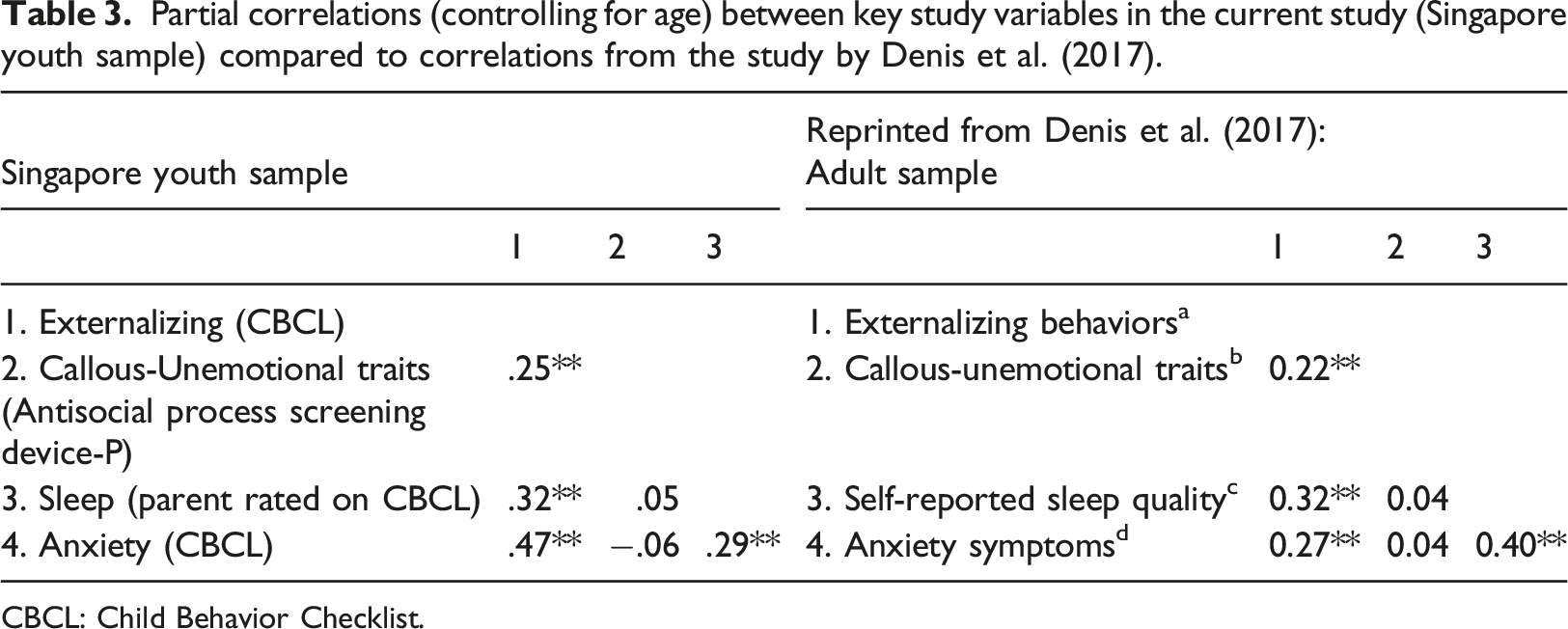
CBCL: Child Behavior Checklist.
A multiple regression model predicting parent-rated sleep problems from externalizing problems and CU traits accounted for a significant proportion of variance in sleep problems after controlling for age [overall model: F(3, 235) = 10.57, p < .001, R2 = .12]. Externalizing problems were associated with more parent-rated sleep problems; β=.33, p < .001, 95% CI = .05 to .12. CU traits were not associated with parent-rated sleep quality; β = −.03, p=.60, 95% CI = −.04 to .02.
Controlling for age, the interaction between externalizing problems and CU traits in predicting parent-reported sleep problems was not significant (β = −0.05, p = .60, 95% CI = −.04 to .03). Mediation analyses using bootstrapped regression (Hayes, 2013) [number of samples = 5000] showed anxiety mediated the relationship between externalizing behaviors (independent variable) and sleep problems (dependent variable, consistent with Denis et al. (2017); see Figure 1; indirect effect, β = .002, CI = .0002 to .0046). Mediation was only partial, as externalizing behaviors remained statistically significant once anxiety was included in the model (p = .0005). The mediator accounted for 25% of the total effect, PM = .25. Anxiety partially mediates the relationship between externalizing and sleep problems.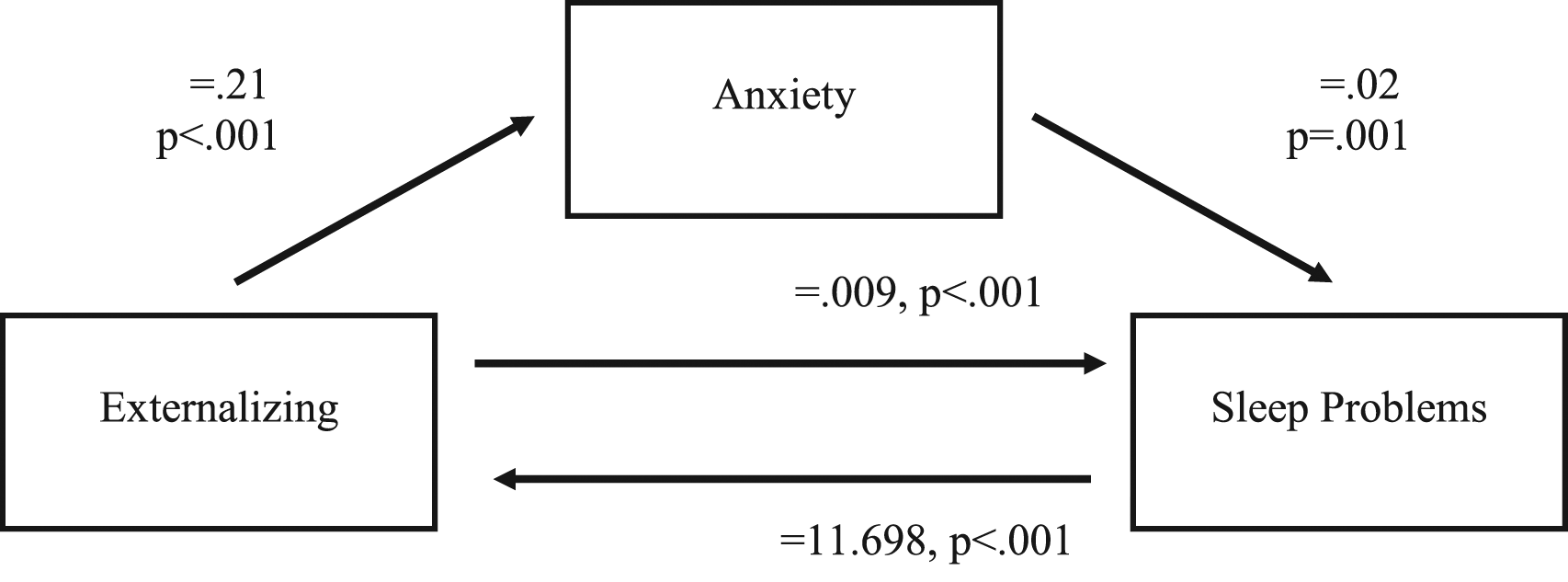
Anxiety was also analyzed as a moderator of the relationship between externalizing and sleep problems. However, the interaction between anxiety and externalizing problems in predicting sleep problems was not significant (β = .197, p = .302). Because age was associated with several study variables, we also examined age as a moderator of the relationship between externalizing problems and parent-reported sleep problems, but the interaction between age and externalizing problems in predicting parent-reported sleep problems was not significant (β = .08, p > .22, 95% CI = −.01 to .05).
Discussion
The goal of the present study was to assess replicability of the findings of Denis et al. (2017) in a youth sample. As hypothesized, and consistent with Denis et al. (2017), in a clinic-referred sample of youth with externalizing problems, we found parent-rated sleep problems were associated with increased externalizing behavior. However, there was no association between child-rated sleep problems and externalizing behavior. Like Denis et al. (2017), we also found the relationship between parent-rated sleep problems and externalizing behavior was partially mediated by anxiety. Finally, unlike Denis et al. (2017), we found the relationship was not moderated by CU traits; parent-rated sleep problems were associated with externalizing problems regardless of the level of CU traits. This was the first study to examine these variables in a sample of youth.
As in the study by Denis et al. (2017), the present study is cross-sectional, and thus was not able to provide information about the direction of the relationship between externalizing behaviors and poor sleep quality. It is possible there is not a causal relationship between poor sleep quality and externalizing behaviors, but these two constructs may simply be co-occurring (e.g., poor parental supervision may contribute to both externalizing behaviors and sleep problems, causing them to co-occur but not be causally related). However, some have speculated poor sleep quality leads to poor emotion regulation and poor impulse control, which may lead to reactive aggression or anxiety. On the other hand, individuals who engage in externalizing behaviors may worry about the consequences of their actions, and this anxiety may disrupt sleep. It is also possible there are some individuals who engage in externalizing behaviors who also exhibit CU traits, precluding them from feeling anxiety; because of this, their sleep is undisturbed by worrying about the consequences of their actions.
It is interesting parent-rated sleep problems were associated with increased externalizing behavior, while there was no such relationship between child-rated sleep problems and externalizing. In a post-hoc analysis, the authors attempted to fit a structural equation model with parent- and child-rated sleep problems loading onto a single latent variable with sleep problems. Despite several attempts (total scores from parents and children as manifest variables; each item from both scales as manifest variables), the model either did not converge or did not have an adequate fit. All of this indicates significant differences between parent- and child-rated sleep problems. There are several possible explanations for this result. The most likely is, since parents reported both sleep problems and externalizing problems, reporter bias or shared-method variance is driving this association. It is also possible parents view sleep problems as a manifestation of externalizing behavior. On the other hand, it may simply be parent-rated, but not child-rated, sleep problems were associated with increased externalizing behavior due to the low power caused by the lower N for child-reported sleep problems (N = 128) than for parent-reported sleep scale (N = 262). Regardless, studies have demonstrated parent-reported sleep quality to be highly correlated with objective measures of sleep, like actigraphy (Sadeh, 1996, 2004).
This study adds to a growing body of literature, demonstrating a link between sleep problems and increased externalizing problems (Barclay et al., 2011; Denis et al., 2017). However, in the present study, parent-rated externalizing problems were associated with higher parent-rated sleep problems but were not associated with child-reported sleepiness, sleep problems, or number of hours slept on school nights. It was not clear why this is the case. Parent-rated sleep problems on the CBCL were moderately associated with the child reporting sleeping less on school nights and having more sleep/wake problems, suggesting some consistency between reporters. Becker et al. (2015) also found moderate correlations between the CBCL sleep composite measure and adolescent reports of sleep problems. One possibility is children are less accurate in reporting sleep problems than parents. Studies have not examined which measure of sleep used in the present study (the CBCL sleep composite or the School Sleep Habits Survey) is a better indicator of objective measures of sleep, such as sleep diaries. However, Gregory et al. (2011) found several sleep items on the CBCL were modestly correlated with data from a sleep diary.
We also examined the role of anxiety and CU traits in the relationship between parent-rated sleep problems and externalizing problems. Relationships between these variables were strikingly similar to those found by Denis et al. (2017) (Table 3). Externalizing problems were associated with sleep problems, CU traits, and anxiety, but CU traits were not associated with sleep problems or anxiety. Like Denis et al. (2017), we found anxiety partially mediated the relationship between sleep problems and externalizing problems, accounting for approximately one-quarter of the total effect. One possibility is children who engage in externalizing behaviors later internalize the experience, leading to anxiety about the behaviors committed. Another possibility is children with higher levels of externalizing behaviors have a more stressful life experience because of negative feedback they receive from parents and teachers, or because they have more conflicts with peers. Future studies should be able to clarify the type of anxiety that mediates this relationship (e.g., worrying about behaviors, worrying about relationships, etc.). The fact that mediation was only partial suggests other factors, such as poor emotion regulation, play a part in the relationship between sleep quality and externalizing problems.
Unlike Denis et al. (2017), we did not find CU traits moderated the relationship between externalizing behavior and sleep problems. Although it has been assumed in the past CU traits reflect an imperviousness to anxiety, in this study and in Denis et al. (2017), CU traits were not correlated with anxiety, suggesting there is not a clear relationship between CU and anxiety. This is consistent with previous studies that find while some youth with CU traits show low anxiety, others may show co-occurring anxiety and CU traits. For example, Short et al. (2016) found adolescents with CD and a comorbid anxiety disorder had the same level of CU traits as adolescents with only CD. In light of these and similar findings, it has been suggested there are two subgroups of youth with CU traits: individuals with and without co-occurring anxiety (Newman et al., 2005; Skeem et al., 2007).
The present study shows anxiety is more of a central factor than CU traits. Furthermore, the significant interaction between externalizing behavior and CU traits in the Denis et al. (2017) study was very small (β = −0.05, 95% CI = −0.09 to −0.01). It is likely this size of an effect was detected because of the very large sample size in that study (N = 1556). However, it is questionable whether this is clinically meaningful.
Although we obtained the same β of −0.05, this was not significant with our smaller sample size. One of the main reasons for replicating the analysis in Denis et al. (2017) was to analyze the same factors in a child population, to determine whether results and implications from adult populations generalize to youth populations. It is possible the same relationships may not exist in youth as in adults due to differences between these two groups in sleep-related factors such as circadian rhythm (Carskadon, 2002). The lack of CU traits as a significant moderating factor in this analysis is the principal difference in results from Denis et al. (2017) to the present study. The most likely explanation for this disparity is not developmental, but rather has more to do with smaller sample size.
There are several limitations to this study. First, we relied on parent- and self-reports of behavior problems and sleep problems. In particular, using more objective measures of sleep quality may help to clarify relationships between these variables. For example, when using self-report measures, Denis et al. (2017) did not find an association between sleep quality and CU traits, which is consistent with our findings. However, when using actigraphy in a smaller sample of participants, Denis et al. (2017) found that CU traits were associated with better sleep quality on some measures (better efficiency and less sleep fragmentation). Thus, future studies using actigraphy or other measures of sleep quality may help to clarify these relationships in youth.
Second, we did not have a pure measure of anxiety in our study, and instead used the anxiety/depression subscale of the CBCL, which also assesses depressive symptoms. Since sleep quality is a major part of the symptomology of depression, it is possible our results reflect the influence of depressive symptoms as well. However, factors such as rumination, which are linked to sleep problems, are associated with both anxiety and depression. For future studies, it may be beneficial to use a measure of pure anxiety, such as the Multidimensional Anxiety Scale for Children (March et al., 1997). In addition, it would be interesting to examine measures of threat processing or measures that focus on specific types of anxiety-related behaviors such as rumination.
Third, our sample was clinic-referred and was specially selected for high rates of externalizing behaviors. For this reason, results may not generalize to children with lower levels of such behaviors. However, an advantage of this study was that our sample had a broader range of externalizing behavior problems than an unselected sample.
Additionally, our findings regarding callous-unemotional traits should be interpreted with caution due to the low reliability of the measure. Other studies have also found low internal consistency on the APSD (Bijttebier & Decoene, 2009; Muñoz & Frick, 2007; Polythress et al., 2006). Polythress et al. (2006) reported a median alpha for the CU subscale across 11 studies was .46. However, despite this low internal consistency, Muñoz and Frick (2007) reported relatively high stability estimates for ratings one and 2 years later and found expected correlations with antisocial behavior, both concurrently and predictively, suggesting good validity of the scale.
The CBCL Sleep Problems subscale had also had low reliability and should also be interpreted with caution. Reliability of the measure was not reported in Becker et al. (2015). One potential explanation is that some of the items have very low rates of endorsement (e.g., 78.7% of parents rated “Talks/walks in sleep” as Not True and 86.9% of parents rated “Wets bed” as Not True). Becker et al. (2015) found that 80% of parents rated “Wets bed” as Not True, and 85% of parents rated “Trouble sleeping” as Very True or Often True. However, Becker et al. (2015) still found the scale to correspond to other parent-rated measures of sleep functioning.
Finally, the data collected for this study were cross-sectional. As stated previously, the direction of the relationship between sleep quality and externalizing behaviors is unknown. Longitudinal studies examining sleep and externalizing problems are needed. One recent study investigated the relationship between adolescent sleepiness and subsequent adult criminal behavior after 15 years (Raine & Venables, 2017). Not only did sleepiness predict adolescent antisocial behaviors, but this longitudinal study showed that, even controlling for adolescent antisocial behavior, self-reported adolescent sleepiness predicted adult criminal behavior. It is also worth noting that self-reported adolescent sleepiness predicted adult criminal behavior better than objective measures of sleepiness (EEG measures of arousal; Raine & Venables, 2017). These findings are similar to previously mentioned studies, which found that childhood sleep problems predicted adolescent externalizing behaviors (Gregory & O'Connor, 2002; Gregory et al., 2008).
In light of the limitations presented, as well as the dearth of existing research concerning the relationship between externalizing behaviors and sleep quality, it is premature to suggest concrete practical implications. However, with further research in this area, a greater understanding of this relationship can inform how both sleep problems and externalizing behaviors are treated when exhibited concurrently.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Singapore Ministry of Health’s National Medical Research Council Individual Research Grant (NMRC 1170/200)