
Abstract
Background
The aim of this paper is the systematic review of psychological/psychosocial interventions for gender diverse youth under 18 years of age and their families, based on the published protocol: PROSPERO 2020 CRD42020163995.
Methods
A search strategy was developed using key terms. An electronic literature search was completed using the following data bases (OVID MEDLINE; EBSCO CINAHL; ProQuest MEDLINE; OVID PsycINFO). Only studies published in English between 2001–2021 were included. This review is based on PRISMA guidance. Studies meeting inclusion criteria were quality appraised using the Mixed Methods Assessment Tool (MMAT).
Results
8405 studies were independently screened. Four studies met the inclusion criteria for the study. Parents of transgender youth attended between one and 11 psychological/psychosocial group interventions. Parents reported reduced isolation and increased knowledge, which enabled them to advocate for their young person`s needs. Psychological/psychosocial group interventions were creating challenges in terms of group processes, with some parents dominating interactions. Psychological/psychosocial group interventions were positive for parents, but no outcomes were collected for transgender young people.
Conclusion
More research is required to understand the role of group facilitators, the optimal group size and the number of psychological/psychosocial intervention sessions required.
Keywords
Background
Transgender or gender diverse young people have a higher risk of poor mental health outcomes compared to their cis gender (non-transgender) age peers (Connolly et al., 2016; Reisner et al., 2015). This is not necessarily surprising given the multitude of challenges gender diverse adolescents’ face, in trying to cope with the mismatch between their growing physical bodies and their internalised sense of self. Transgender adolescents are four times more likely to have depression compared to their cis gender peers (Peterson et al., 2017). Clinically, young people with depression can present as sad, hopeless, irritable and tired with loss of interest in previously enjoyable activities (Thapar et al., 2012). Depression can impact negatively in terms of school, home and leisure activities. In 2007, Grossman and D`Augelli suggested that 58% of transgender adolescents receive a diagnosis of depression, of these, 51% experience suicidal ideation and 32% attempt suicide. These figures are alarming and highlight the need for a greater understanding of the relationship between adolescent transgender identity and mental health, in order to find ways to support young people and to reduce their risk of suicidality.
Increased risk of poor mental health outcomes has been associated in the literature with minority stress (Hendricks & Testa, 2012). In 2003, Meyer described the minority stress model, in which stigma, prejudice and discrimination impact negatively on mental health. While this concept was originally developed to understand the impact of a sexual minority status, it can be applied to a range of minority populations. It is worth noting, that many young gender diverse people, belong to more than one minority group. Aside from their transgender identity, they could be part of a sexual, ethnic or disability minority group, with overlapping areas of stigma and discrimination. Minority stressors can be described as distal (environmental), interactive (expectation of external threat) and internalised (internalised negative attitudes) (Meyer, 2003). While minority stressors can cause poor mental health, this is not a given. In a recent systematic review in 2021, Tankersley et al. identified risk and resilience factors for mental health in transgender young people. Risk factors were reported as: (1) physical and verbal abuse, (2) exposure to discrimination, (2) social isolation, (3) poor peer relations, (4) low self-esteem, (5) weight dissatisfaction and (6) age, with older adolescents identified at increased risk (Tankersley et al., 2021). Resilience promoting factors in the systematic review included: (1) parent connectedness, (2) social support, (3) school safety and (4) the ability to use the preferred name (Tankersley et al. 2021). Parent connectedness in this context refers to the closeness between the transgender young person and their parent or caregiver.
Looking in more detail at parent connectedness and family relationships could identity resilience promoting behaviours, which support gender diverse young people. Positive relationships between young people and their parents in some of the reviewed studies, promoted resilience in young people who were seeking gender affirming treatments and those who were not. Gower et al., (2018) reported lower odds of depression, suicidality and suicide attempts in young people with greater parental connection. In 2013, Simons et al. emphasised the positive association of parental support with a higher quality of life for transgender adolescents, highlighting the value of interventions, which promote parental support. Psychosocial or psychological interventions involve therapies or actions used to help gender diverse young people assimilate healthily with their families into society. While there is research evidence to highlight the positive impact of family acceptance on young people`s mental health (Olson et al., 2016), little is known about how to best provide psychological and psychosocial support to families of gender diverse young people. This systematic review aims to address this current gap in knowledge.
Methodology Used for this Review
Aims
• To review the evidence on psychological and psychosocial support for families of gender diverse youth. • To review established interventions/therapies for families of children and young people exploring gender diversity • To determine the effectiveness of the above interventions/therapies in improving family relationships and mental wellbeing for transgender young people
Design
Systematic reviews have been described as the gold standard among reviews, collecting research in a systematic, transparent and reproducible way (Davis et al., 2014). High quality systematic reviews can avoid unnecessary primary research (Gough et al., 2017). In transgender healthcare, research studies are frequently conducted with small sample sizes in dispersed specialist centres. Gender diverse individuals have been the subject of a range of research studies, with some transgender individuals reporting research participation fatigue (Ashley, 2021).
Protocol and registration
This systematic review is based on the published protocol: Psychological/psychosocial interventions for gender diverse youth under 18 years of age and their families: a systematic review: PROSPERO 2020 CRD42020163995.The protocol states that risk of bias assessments will be completed using the ROBIS tool (Whiting et al., 2016). On further evaluation, the ROBIS tool was found to be unsuitable for this type of systematic review as it focuses on assessing risk of bias in systematic reviews rather than primary research studies. This is a deviation from the original protocol, with the Mixed Methods Appraisal Tool (MMAT) developed in 2018 by Hong et al. chosen to assess risk of bias in its place. As the protocol had been published in 2020, the inclusion period for studies has been adjusted from (2000-2020) to 2001 to 2021 to capture the last 20 years of research.
The eligibility criteria are clearly stated in the systematic review protocol in terms of the population, interventions, comparators and outcomes. The population are families of gender diverse youth, defined as children or adolescents under the age of 18 years of age with a parent or caregiver. Interventions are defined as any psychological or psychosocial intervention, offered to gender diverse youth and their families. If studies include comparisons between groups or within groups, comparators are defined as other types of psychological, psychosocial interventions or no treatment. Outcomes in this review include the identification of relevant interventions and effectiveness of these interventions.
Search Methods
An electronic literature search was conducted using OVID MEDLINE; EBSCO CINAHL; ProQuest MEDLINE; OVID PsycINFO. Only studies published in English from 2001–2021 were included in the search. The last 20 years were used as the period for the assessment of the most recent subject material, which is likely to include or relate to the specified population. The search strategy was developed based on key terms. Search terms were reviewed with guidance from the university subject librarian. The search strategy terminology was adjusted slightly in keeping with search terminology of each data base.
Example of Search Strategy
(1) exp Family/ (2) exp Parents/ (3) siblings mp. (4) (famil* or parent* or sibling* or brother* or sister* or father* or mother*or grandparent* or grandmother* or grandfather* or guardian* or spouse* or adopt*) mp. (5) 1 or 2 or 3 or 4 (6) transgender persons mp. (7) Exp transsexualism/ (8) (transgender* or transsexual* or gendervariant* or gender divers* or gender incongruent* or non-binary or gender dysphor* or genderqueer or queer or genderfluid) mp. (9) 6 or 7 or 8 (10) 5 and 9 (11) Limit 10 to yr=“2001–2021” (12) (intervent* or treatment* or therap* or education* or support*) mp. (13) 11 and 12
Search Outcome
During the data collection process, the protocol authors independently screened titles and abstracts identified through the electronic searches and compared them against the inclusion criteria. The authors accessed full text studies if the titles and abstract met the inclusion criteria or if there was uncertainty. Both reviewers screened full text articles and made decisions about the inclusion of the study. Any disagreements were resolved through further discussion.
Quality Appraisal
Assessment of the methodological quality is the key to ensuring that systematic reviews are trustworthy, valid and reliable (Harden & Gough, 2012). The MMAT version 2018 was developed to focus on reporting, conceptual and methodological aspects of mixed methodological studies (Hong et al., 2018), highlighting potential bias in each area. The MMAT tool 2018 was piloted prior to use. Both authors independently followed the algorithm for study categories and completed the appropriate sections of the MMAT (Hong et al., 2018) for each included study. Disagreements were resolved through further discussion.
Data Abstraction
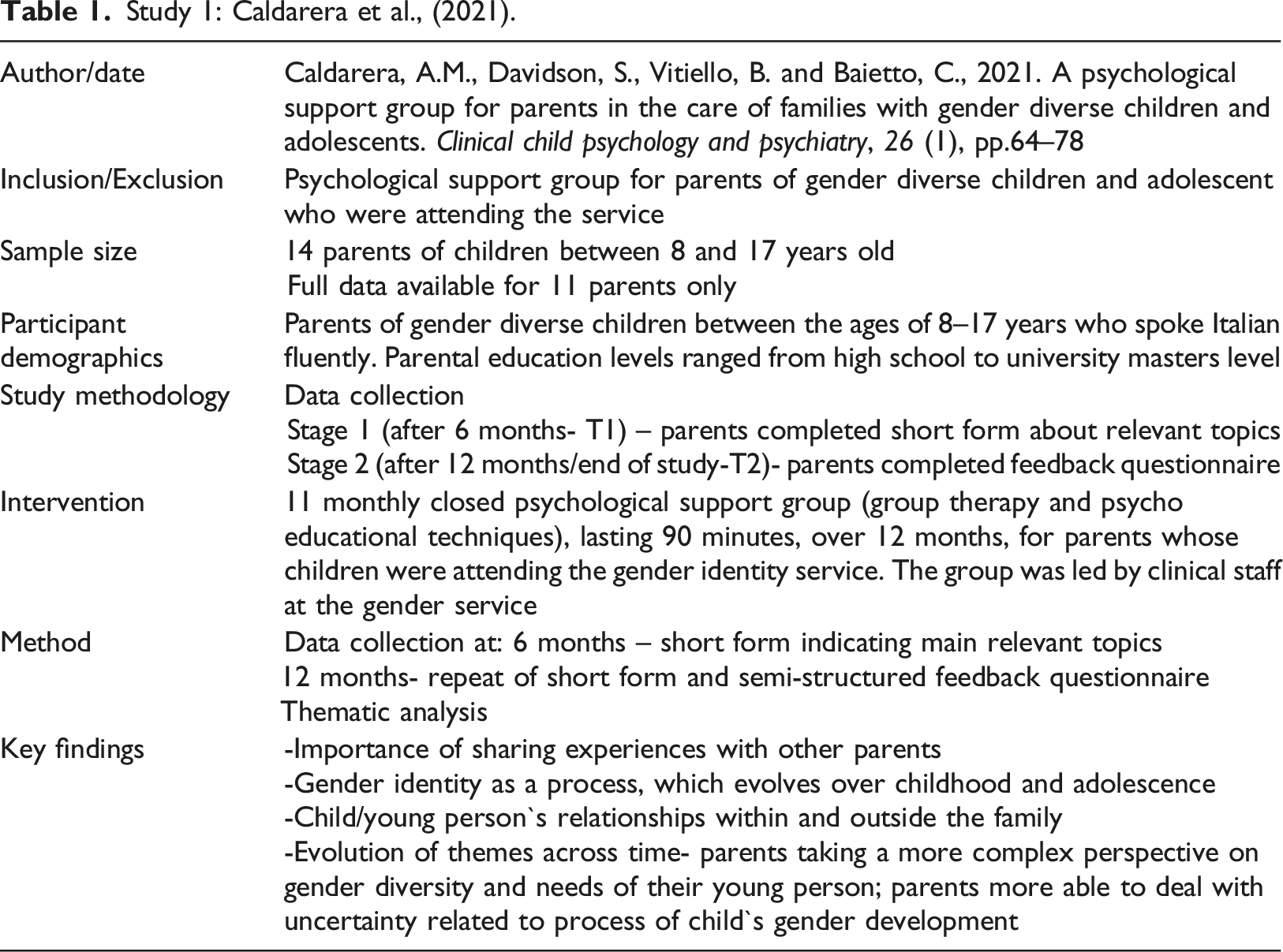
Study 1: Caldarera et al., (2021).
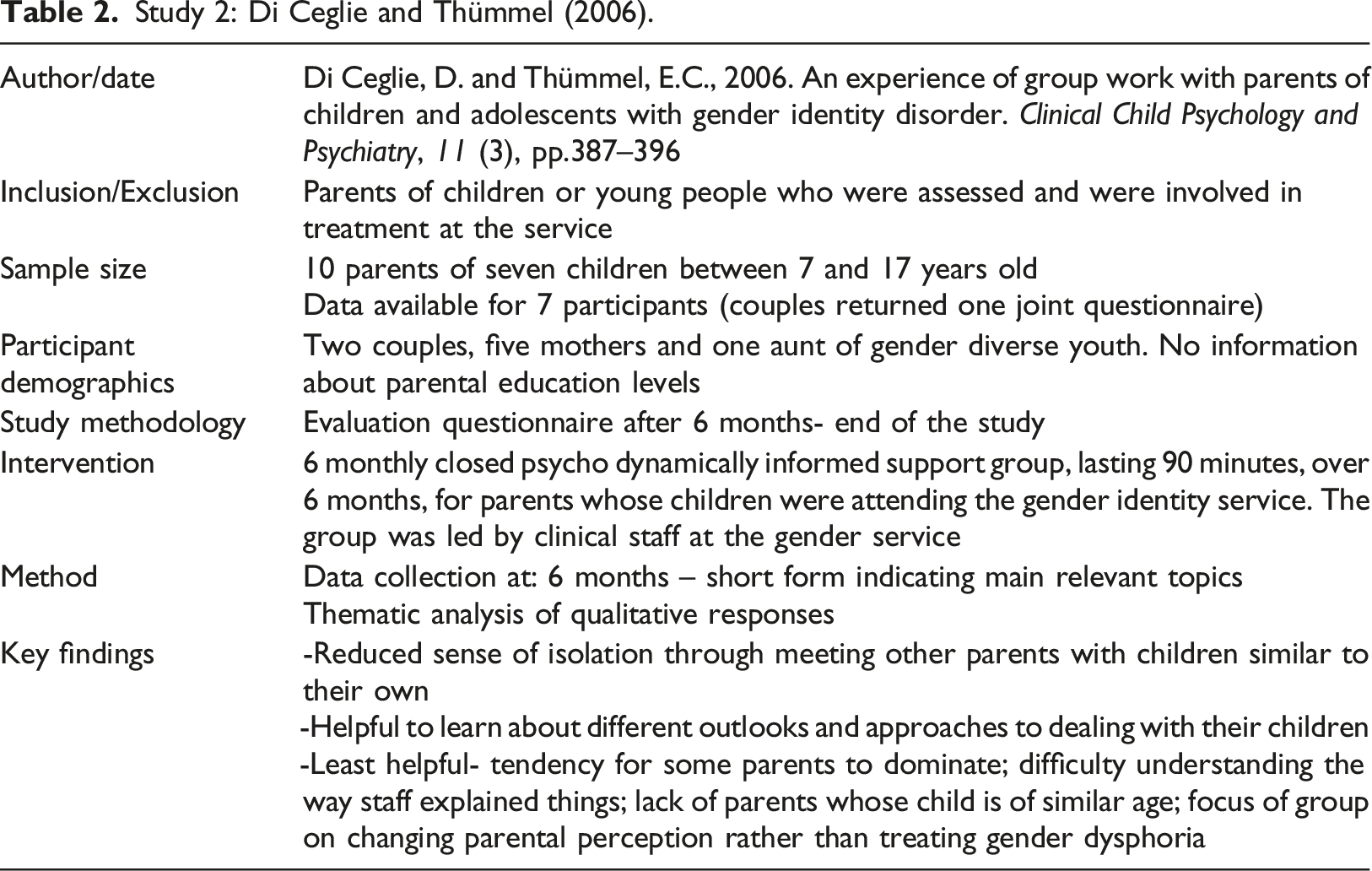
Study 2: Di Ceglie and Thümmel (2006).
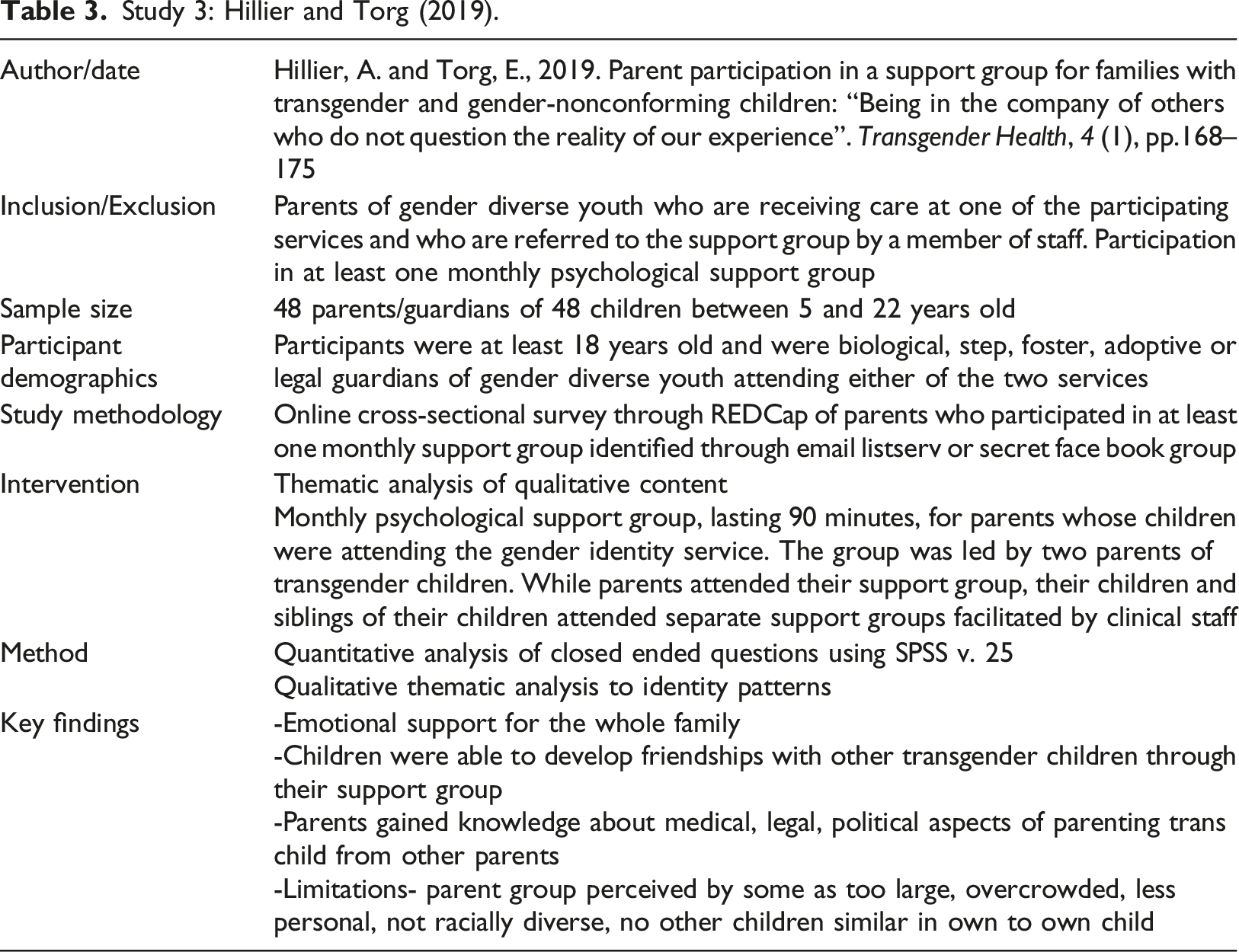
Study 3: Hillier and Torg (2019).
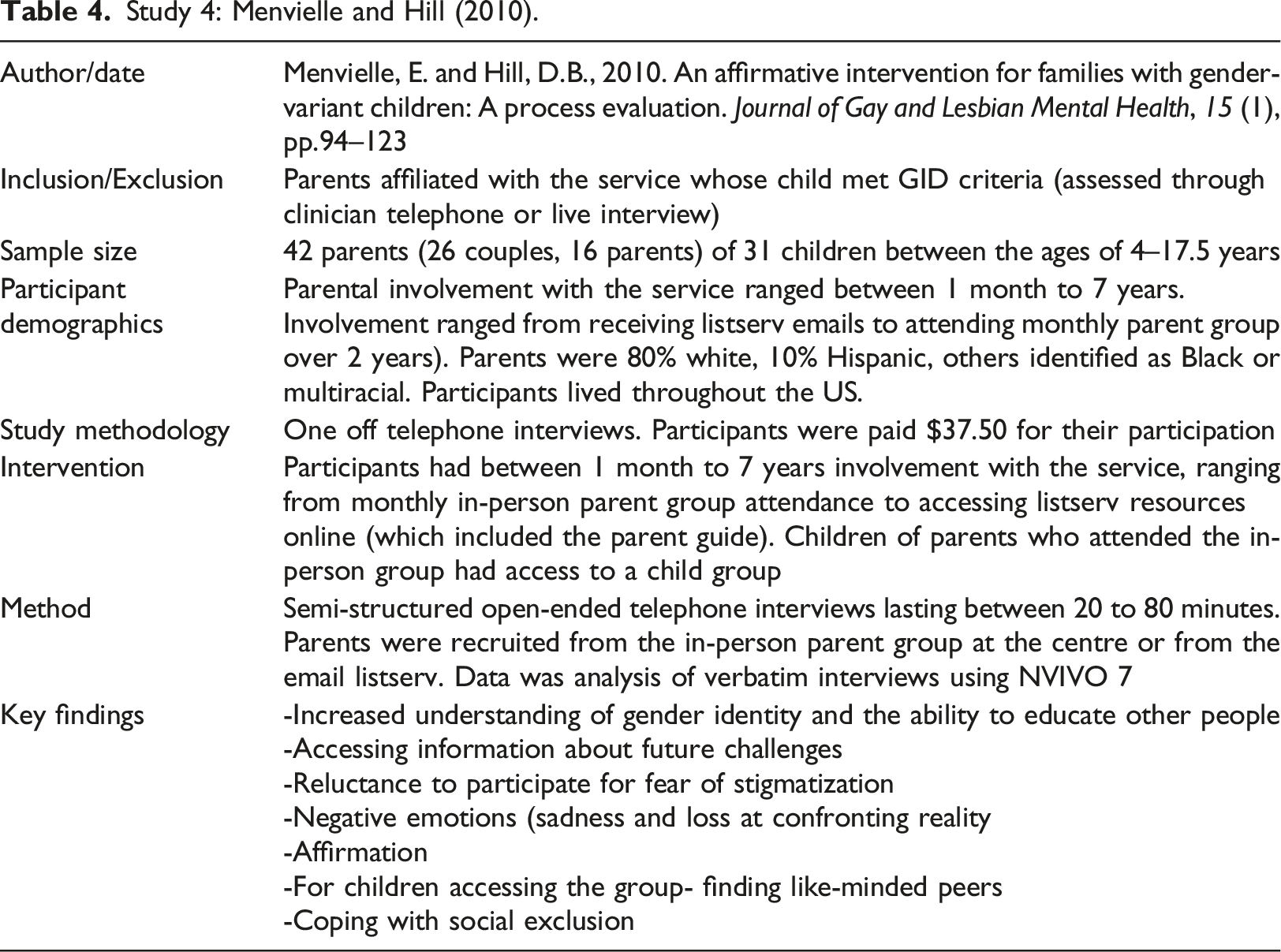
Study 4: Menvielle and Hill (2010).
Synthesis
Synthesising qualitative research is a complex area, with ongoing debates about appropriate methods and whether qualitative data is too specific in terms of context, time and participants to be generalisable (Thomas & Harden, 2008). This has led to suggestions, that qualitative synthesis de-contextualises findings (Sandelowski & Barroso, 2006). Thematic analysis of primary qualitative data follows a structured process: (1) familiarisation with the data, (2) initial line by line coding, (3) sorting of initial codes into broader themes, (4) review of emerging themes and (5) renaming and refining codes (Braun & Clarke, 2006). Thematic synthesis has been developed to analyse secondary data, following a number of steps: (1) line by line coding, (2) the development of descriptive themes close to the primary studies and finally (3) generation of new hypothesis (Thomas & Harden, 2008).
Due to the small number of included studies, there was limited data to analyse. Qualitative data analysis was thematic and were possible thematic synthesis steps were followed. Data was initially described on the basis of the PICO criteria-families of gender diverse youth (population), psychological/psychosocial support group (intervention) and outcomes. As none of the studies included a comparison group, the comparator aspect was removed. The limited quantitative data is reported separately.
Results
Study Selection
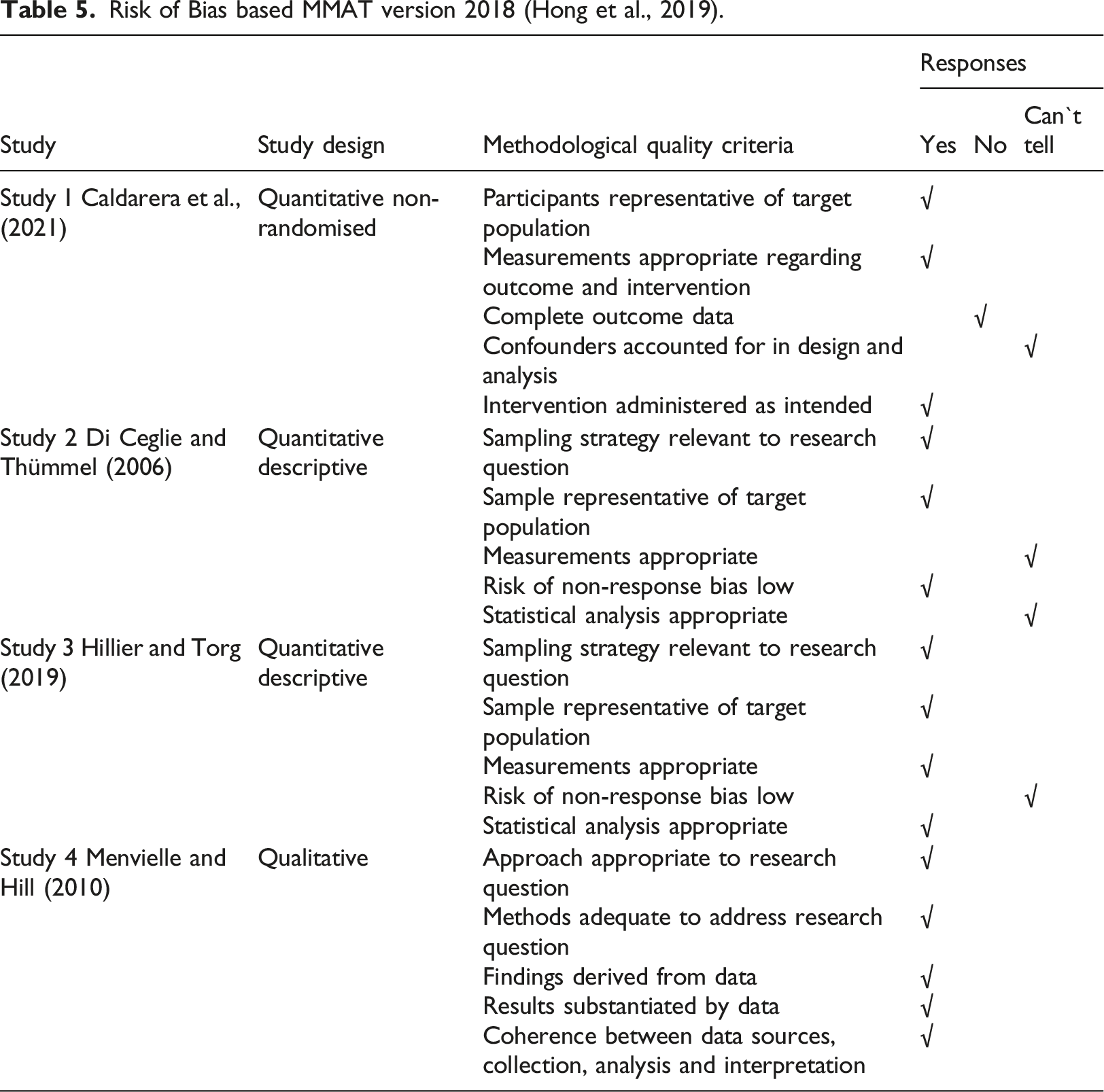
Overall 8405 studies were independently screened. By the screening of titles and abstracts 8292 studies were excluded, while 113 studies were screened for further detailed analysis, from which 109 studies did not meet the eligibility criteria. Only four studies met inclusion criteria for the review. Figure 1 outlines the study selection process based on PRISMA guidance. The following results are organised and expanded on the basis of the PICO criteria. Quality appraisal of each study was conducted using the MMAT tool (Hong et al., 2018). This highlighted potential risks of bias in each study, in terms of for example missing data (Caldarera et al., 2021) and missing standard deviations (Di Ceglie & Thümmel, 2006). In other studies it was impossible to know whether there was coherence between data sources and analysis (Menvielle and Hill, 2010) or whether the risk of non-response bias was low (Hillier & Torg, 2019). As these studies represent the limited available research available on family interventions for transgender youth, the quality of included study was accepted as basis for this review. PRISMA flow diagram (Moher et al., 2009).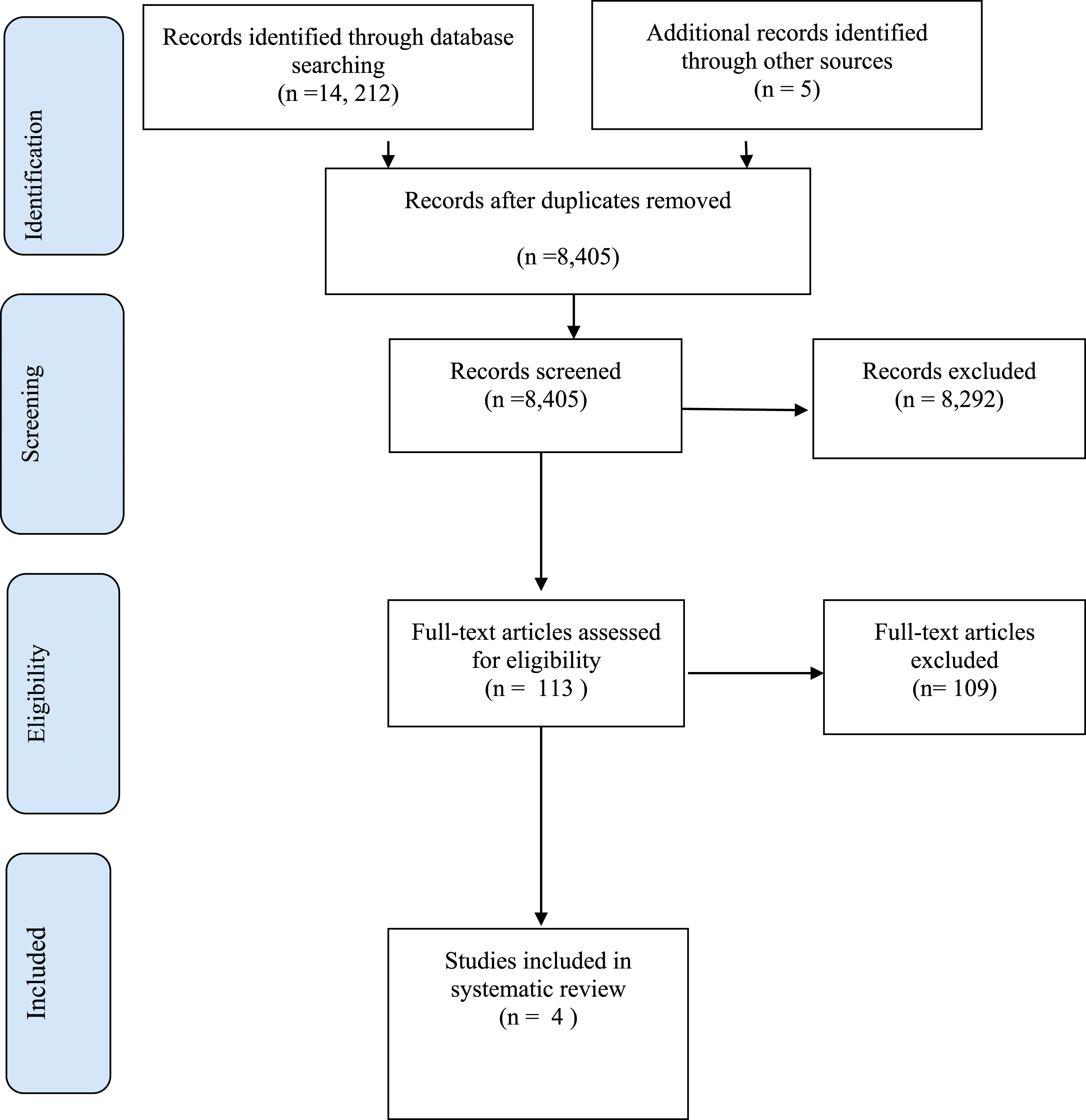
Population
Risk of Bias based MMAT version 2018 (Hong et al., 2019).
Intervention
Most of the included studies provide details about the group intervention offered to parents, apart from Hillier and Torg (2019), who only make reference to the support group, without providing specific details. Groups were led by clinical staff, some of whom had other types of contact with the families in the studies. Hillier and Torg (2019) study was conducted by two parents who were attending the monthly support groups, while the other studies were conducted by clinical staff who were leading the support groups. The definition of intervention differed across studies. Participants in the studies by Di Ceglie and Thümmel (2006) and Caldarera et al., (2021), attended at six monthly parent groups (Di Ceglie & Thümmel, 2006) and up to 11 monthly parent groups (Caldarera et al., 2021). The other studies specified one or more attendance at the monthly support group (Hillier & Torg, 2019) and a range of different interventions on their own, or in combination, such as monthly parent groups, listerv (internet forum) contact and website access (Menvielle & Hill, 2010). Parent groups lasted between sixty to 90 minutes (Caldarera et al., 2021; Hillier & Torg, 2019; (Di Ceglie & Thümmel, 2006). No details about the group length were available for Menvielle and Hill (2010). The group formats were therapeutic, with some educational elements (Di Ceglie & Thümmel, 2006). Parent groups were closed in two studies (Di Ceglie & Thümmel, 2006; Caldarera et al., 2021) with consistent group membership and open in the other two studies.
Comparators
None of the studies included comparison of the intervention with treatment as usual or other interventions.
Outcomes
Studies used a range of quantitative and qualitative outcome measures for parents. None of the measures used were standardised tools. In terms of feedback surveys, studies included quantitative elements, based on closed questions and open ended questions, which invited parents to include free text, which was thematically analysed. Menvielle and Hill (2010) was the only study which was based on interview data.
Quantitative Outcomes
Two studies (Di Ceglie & Thümmel, 2006; Caldarera et al., 2021) contained the same questions in their survey, in terms of helpfulness of the group, meeting other parents, reduced isolation and parents having a changed approach as a result of the group. This was deliberate as the second study was based on previous research. Both studies used very similar interventions, offering a closed therapeutic group with similar sample sizes in their studies. A comparison between studies, highlights a mean difference of 0.25 (helpfulness of group, 0.4 (meeting other parents), 0.38 (reduced isolation) and 1.35 (changed approach as a result of the group). Mean scores for Di Ceglie and Thümmel (2006) were marginally higher for all items, but no standard deviations were reported. Data was collected after 6 months (Di Ceglie & Thümmel, 2006) compared to after 12 months (Calderera et al., 2021).
Hillier and Torg (2019) collected information about the importance of the support group for family members on a Likert scale containing four categories (ranked from not particularly helpful to single most important). In this study authors reported proportions in each category, with a majority of 35/48 (73%) indicating importance or critical importance in terms of the support group.
Theme 1- Reduced shame and isolation
Participants reported reduced shame about their child or young person`s gender identity (Caldarera et al., 2021) and felt less isolated (Caldarera et al., 2021; Di Ceglie & Thümmel, 2006; Hillier & Torg, 2019). Listening to others also reduced anxiety (Hillier & Torg, 2019). Participants reported the value of emotional support, in particular the opportunity to build friendships with other families (Menvielle & Hill, 2010). Participants in Hillier and Torg (2019) study expanded on the concept of friendship, describing other participants as friends or chosen family. Parents took the role of supporters to other parents who had less experience with their transgender child (Hillier & Torg, 2019).
Theme 2- group processes
For some participants, the group format itself brought challenges, which differed in terms of the group set up. In the open group set-up by Hillier and Torg (2019), some participants felt the group had become less personal and overcrowded. It is unclear what group sizes were offered by the service. In the closed group set-up by Di Ceglie and Thümmel (2006), some participants reported that other group members dominated interactions. Some participants were critical of the lack of racial diversity in the group (Hillier & Torg, 2019), while group formats in other services were set up specifically for interracial families (Menvielle & Hill, 2010). The logistics of attending the group were reported as difficult by some participants due to physical distances, requiring overnight stays for some (Hillier & Torg, 2019).
Theme 3- Looking into the future
Participants in Di Ceglie and Thümmel (2006) study, valued talking to others about different approaches in managing their children and different outlooks into the future. Participants in Menvielle and Hill (2010) study reported that taking part in the group allowed them a window into the future, preparing them for what might be ahead of them. Combining parents of children and young people at different developmental and transition stages in a group also brought challenges, with some parents presenting a terrifying and gloomy picture of the future (Di Ceglie & Thümmel, 2006) to others. This experience was shared by participants in (Hillier & Torg, 2019) who requested a splitting of groups by age, feeling overwhelmed after having to listen to other parents talk about surgical procedures when they were only beginning to get used to different pronouns.
Theme 4- increased understanding of transgender young person`s experience
Participants reported an increased understanding about their child`s experience in terms of navigating their development in the context of gender incongruence (Di Ceglie and Thümmel), while others reported gaining knowledge in terms of medical, legal and political aspects of parenting a transgender child (Hillier & Torg, 2019). Parents in the study by Caldera et al., (2021) reported the importance of increased awareness of difficulties faced by gender diverse young people and the legal issues they may face.
Theme 5- parents as advocates for transgender youth
Participants in Menvielle and Hill (2010) reported feeling more open to discuss difficult topics with their child, with the group intervention serving as a reference point. In the study by Caldarera et al., (2021), participants reported that mutual learning created better insights into different ways of coping with the same situation, while also decreasing parental sense of guilt. In some of the studies, parents made specific reference to the benefit of support from clinical staff in the group, which some described as sympathetic and professional (Di Ceglie & Thümmel, 2006; Caldarera et al., 2021). For participants, having access to a network of knowledge from other parents and clinicians increased their knowledge about specific doctors and health insurance coverage, enabling them to effectively advocate for their children (Hillier & Torg, 2019).
Discussion
Family support is a known protective factor against health risks for transgender youth (Simons et al., 2013; Olson et al., 2016). This review reported on group interventions for parents of transgender youth. The total sample of participants in the review was 114, highlighting the limited available amount of research studies in this area. None of the included studies measured outcomes in terms of transgender youth and it is unclear if any transgender young people benefited from parents attending the group interventions. Two studies (Di Ceglie & Thümmel, 2006; Caldarera et al., 2021) completed an evaluation of a structured closed group intervention, indicating benefits for parents in terms of increasing their understanding, meeting other parents, feeling less isolated and changing their approach to managing their child`s gender diversity. As parents and their young people received other supports from services, it is unknown whether the group intervention created the reported change. It is unclear whether the context of the group interventions based in specialist gender services impacted on the reported outcomes by parents. Clinicians in specialist gender services are put in the position of gate-keepers to physical interventions. Lev (2009) argues that the gate-keeping role impacts on the building of healthy therapeutic relationships. It unknown whether facilitation of the groups by clinical staff was viewed by parents as part of a wider assessment process for their children`s eligibility to access gender affirming interventions and if this influenced their feedback about the groups.
Studies highlighted the need to address potential negative group dynamics (Di Ceglie & Thümmel, 2006; Hillier & Torg, 2019), in terms of parents having different needs, based on the developmental stages of their children and the risk of some parents dominating discussions. This highlights the need to explore the role of group facilitators and whether groups should be managed by clinical staff, parents or both. Group size and group membership were also crucial aspects for some parents. While participants attended between one and 11 group sessions in the studies, it is not clear whether the number of group attendances is important for parents. Lawlis et al., (2020) completed a survey of parental preferences for group interventions, which highlighted that the majority of parents liked monthly meetings, with a group size of between six and 10 people, with the majority of parents happy to attend the clinical service base for the group as long as travel time to the group was between 11 and 20 minutes. This highlights many common barriers relevant to all types of group attendances in terms of time and convenience. Some parents reported reduced need for the group intervention over time (Hillier & Torg, 2019), which could be directly related to the positive impact of the intervention or due to natural development processes in the child which reassured the parent.
Measuring the impact of group interventions is complex and none of the studies in the review used before and after measures. It is therefore unknown whether group interventions impacted on parenting practices or family dynamics. Brown et al., (2020) in their review of family relationships of transgender youth, differentiate between general family support and gender-identity specific support. All included studies offered a gender-identity specific group intervention to parents. Brown et al., (2020) argue that while both types of family support can be protective, it is unclear if the need for general family and gender identity specific support varies within family members.
The studies by Menvielle and Hill (2010) and Hillier and Torg (2019) focused a group intervention as part of a range of activities of an affirmative service programme. The use of incentives by Menvielle and Hill (2010) and the participation of the researchers as parents in the group (Hillier & Torg, 2019) may have introduced recruitment bias. As all the studies were based in specialist gender services, group interventions may have been offered to parents who were at least somewhat supportive of the gender diversity of their children. This could have excluded parents who did not support their children`s gender diversity or who were at the very early stages of their child, questioning their gender identity. As there were no comparison groups, this cannot be established. It is also not clear whether clinical staff input or parental input into the groups made a difference to the experience, as groups tended to be facilitated by clinical staff, but parents reported benefits in meeting other parents. Studies highlighted risks and benefits of incorporating parents of children and adolescents but it is unclear whether parents of young children would have received greater benefit without hearing the potential frightening aspects of adolescence and whether parents of adolescents gained no benefit themselves hearing about childhood experiences, they had already managed.
There were a number of limitations in this review. None of the included studies measured outcomes of the interventions for transgender youth and it was therefore impossible to ascertain whether the interventions for parents resulted in improved mental health for transgender young people. In terms of group facilitation there was no consensus about who is best placed to facilitate parent groups, whether open or closed groups were better, how many sessions provided the best outcomes for parents and whether parents of young people in different age groups should be combined in the same group. As none of the studies completed before and after measures, it was also difficult to know whether the group intervention rather than another factor created positive change for parents.
Conclusion
This review highlights the limited available research in terms of family interventions which could increase resilience in transgender youth and protect them from potential adverse mental health outcomes. This review compares and summarises available evidence of group family interventions, which show a positive impact on parents in terms of reducing their isolation and meeting their needs for knowledge in managing their transgender young person.
Looking at the needs of families of gender diverse youth highlights that they experience marginalisation alongside their young person. From a minority stress theory point of view, parents are struggling to meet the needs of their transgender young person in a family and community context which could be unwelcome or even hostile. The group interventions for many parents reduced their isolation and created a new network of supportive adults. Whether this in turn has enabled parents to create more psychologically healthy and supportive home environments for their children is unclear. There is a need for further research to investigate whether families require general family interventions or specific gender identity focused family interventions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.