
Abstract
Cognitive disengagement syndrome (CDS) has been found to be associated with internalizing symptoms. Yet, no study thus far has focused on whether there is an association between obsessive-compulsive disorder (OCD) and CDS. The purpose of this study is to examine the symptom frequency and clinical implications of CDS in children with OCD. The study included sixty-one children with OCD and sixty-six typically developing children. Children were evaluated by a semi-constructed diagnosis interview, Obsessive-Compulsive Inventory, Barkley Child Attention Scale, and Stroop test. The frequency of elevated symptoms of CDS, and total time, total error, and total correction scores of the Stroop test were significantly higher in the OCD group compared to the controls. Elevated CDS symptoms were significantly associated with higher OCD symptom prevalence and poorer performance on the Stroop Test. Moreover, poor insight, hoarding symptoms, mental compulsions, and ADHD comorbidity were significantly higher in those with elevated CDS symptoms than in those without CDS in the OCD group. The findings of this study provide clinical implications that CDS symptoms may contribute to deficits in attentional orientation, conceptual flexibility, and cognitive processing speed in OCD.
Keywords
Introduction
Obsessive-compulsive disorder (OCD) is characterized by repetitive, intrusive, unwanted, and distressing thoughts, images, or urges (obsessions), and repetitive behaviors or mental acts (compulsions) that a person feels driven to perform in response to the obsessions (American Psychiatric Association, 2013). Pediatric OCD is often present with other psychiatric disorders. In the National Comorbidity Survey Replication, 90% of respondents with lifetime OCD in the general population met the diagnostic criteria for another lifetime disorder (Ruscio et al., 2010). Available prevalence estimates of overall comorbid conditions range from 56% to 91% for pediatric-onset OCD (Ruscio et al., 2010; Saad et al., 2017). The most common psychiatric comorbid conditions include anxiety disorders, depression, tic disorders, attention-deficit/hyperactivity disorders (ADHD), and autism spectrum disorders (Abramovitch et al., 2015; Ruscio et al., 2010; Saad et al., 2017).
Cognitive disengagement syndrome (CDS), formerly known as ‘sluggish cognitive tempo’ (SCT), is characterized by a cluster of symptoms including a sleepy appearance, excessive daydreaming, being confused, staring blankly, getting lost in one’s thoughts, being sluggish, and slowed behavior/thinking (Barkley, 2013; Becker et al., 2016, 2022). Epidemiological studies have reported that the prevalence of CDS in the community is 11% (Camprodon-Rosanas et al., 2017).
Although first arising from research examining the dimension of ADHD, it is now evident that SCT symptoms are separate from, yet closely related to, ADHD-inattentive (ADHD-IN) symptoms (Becker et al., 2022). Currently, strong empirical evidence exists to support the distinction between CDS and ADHD-IN symptoms (Becker et al., 2020; Burns & Becker, 2021; Servera et al., 2018). Also, it has been stressed that CDS may be best conceived of as a trait-like phenotype rather than a disorder of any kind (Burns et al., 2020). However, research is required to determine whether CDS is better conceived of as its own disorder, a specifier within ADHD, or a transdiagnostic entity. Moreover, unlike ADHD, CDS is more closely associated with internalizing symptoms (anxiety/depression symptoms) (Becker et al., 2020; Camprodon-Rosanas et al., 2017; Mueller et al., 2014). Therefore, it has been stated that CDS may be a valuable factor to investigate not only in ADHD but also in other psychopathologies (Mueller et al., 2014).
Regarding the neuropsychological links between frequently co-occurring ADHD, tic disorders, and OCD, neuropsychological and neuroimaging studies show that similar executive functions are affected in these disorders, suggesting shared etiology factors and mechanisms for these disorders (Vloet et al., 2006). In these disorders, neuropsychological deficits have been documented in executive functions especially impaired inhibition, interference control, and planning, deficits in processing speed, vigilance, and working memory, decreased cognitive flexibility in switching, and cognitive alternation tasks (Brem et al., 2014; Cabarkapa et al., 2019; Geller et al., 2018; Shin et al., 2014). Again, these disorders are assumed to result from frontostriatal pathophysiology and dysfunction within cortico-striato-thalamico-cortical circuit responsible for cognitive control and performance monitoring processes (Cabarkapa et al., 2019; van den Heuvel et al., 2010). This common neurological background and neuropsychological profile may also be possible between OCD and CDS, despite different clinical manifestations in CDS, and CDS being statistically related to other symptom constellations, such as ADHD-Inattentive symptoms (Camprodon-Rosanas et al., 2019; Creque & Willcutt, 2021; Flannery et al., 2017; Geller et al., 2018; Jacobson et al., 2018; Mueller et al., 2014; Shin et al., 2014). In addition, there may be an overlap between the clinical presentation of OCD and CDS, a possible mechanism for which is “mind-wandering” (Christoff et al., 2016). Mind wandering is defined as a sudden attentional shift to our inner cognitions and unrelated inner thoughts, feelings, memories, plans, or wishes rather than the outside world and here-and-now (Christoff et al., 2016). Mind wandering is a sort of spontaneous thought that is different from but similar to daydreaming which is used most usually as a cardinal item of CDS, and is a mental state in which there are no strong constraints on thought contents (Becker & Barkley, 2021; Christoff et al., 2016). Recent studies have highlighted a potential link between CDS and mind-wandering and that SCT may represent one characterized by internal distractibility (Becker & Barkley, 2021; Fredrick et al., 2020), and found that CDS symptoms are more significantly linked to greater mind-wandering (Fredrick et al., 2020). Similarly, mind-wandering is also closely related to OCD symptomology, and the intrusive nature of obsessional-compulsive thoughts overlaps with the concept of spontaneous mind-wandering that abruptly into one’s consciousness without any identifiable evoking stimuli (Cole & Tubbs, 2022; Seli et al., 2017). However, according to Christoff and colleagues, mind wandering is a specific state of spontaneous thought that is less constrained and more goal-directed thought compared with rumination and obsessive thoughts. Furthermore, mind wandering can be readily distinguished from rumination and other types of thought that are characterized by the strongest levels of automatic constraints, such as obsessive thought (Christoff et al., 2016). Researchers have found that the type and extent of OCD symptoms are predicted by the frequency of spontaneous, but not deliberate, mind-wandering experiences (Cole & Tubbs, 2022; Seli et al., 2017). It has been revealed that mind-wandering confers an increase in obsessive-compulsive thoughts and the severity of obsessive-compulsive symptoms is positively associated with excessive mind-wandering (Seli et al., 2017; Wang et al., 2021).
Aims of this article
Determining whether CDS accompanies OCD may be crucial in terms of patient management, treatment modality, and outcomes, because findings indicating the relationship between CDS and OCD symptoms may serve as a guide for investigating novel psychological therapies for OCD. The purpose of this study is to determine the frequency of CDS symptoms accompanying OCD and to describe the differences between clinical features in an OCD sample with and without elevated CDS symptoms.
Materials and methods
Participants
Participants were selected from two child and adolescent psychiatry departments. The sample of the study consisted of 61 children aged 9–13 years who were diagnosed with OCD [36 males (59%), the mean (SD) age: 11.43 ± 0.90 years] and 66 controls [37 males (56.1%), the mean (SD) age: 11.26 ± 0.87 years] who were similar to the patient group in terms of age and sex. The control group was selected from community-based primary and secondary school samples who did not refer to child and adolescent psychiatry for any psychiatric condition. Children with a chronic medical condition such as epilepsy, those with tic disorders, intellectual disability and/or autism spectrum disorder, and those who had major head injury were excluded from the study. To create a more homogeneous group, the OCD sample was selected from children with a diagnosis of OCD for at least 1 year and who had been prescribed only selective serotonin reuptake inhibitors (SSRI) as monotherapy for OCD. Patients using multiple drugs which could affect cognitive assessments, and patients not taking any medication were not included in the study.
Data collection tools
Sociodemographic data form
This form was prepared specifically for the study by the researchers and included information about age, sex, socioeconomic status, psychiatric history and family history, age of onset of OCD confirmed by semi-structured clinical interview, age of diagnosis, duration of OCD, types of obsessions and compulsions, and prescription medications. These parameters were evaluated by the researchers during interviews with children and their parents.
Schedule for affective disorders and schizophrenia for school-age children (6–18 years)-present and lifetime version (K-SADS-PL-DSM-5)
This semi-structured interview schedule was updated by Kaufman et al. (2016) and the Turkish version was conducted by Ünal et al. (2019). K-SADS-PL is used to identify current and past episodes of psychopathology in children and adolescents. Current and past symptoms were scored on a three-point scale (1 = “not present,” 2 = “subthreshold,” 3 = “threshold”).
Maudsley obsessive-compulsive inventory (MOCI)
MOCI is a self-report scale consisting of 37 questions answered in the form of true-false, developed by Hodgson and Rachman (1977), and used to measure the type and prevalence of obsessive and compulsive symptoms. The Turkish validity and reliability study was performed by Erol and Savasir (1988). While the original scale includes checking compulsions, washing cleaning, slowness, and doubting subscales, the rumination subscale was added in the Turkish version.
Barkley child attention scale (BCAS)
It was developed by Barkley to evaluate CDS symptoms in individuals. It includes 12 4-point Likert-type items and consists of two subscales: sluggishness and daydreaming (Barkley, 2013). The Turkish validity and reliability study was performed by Firat et al. (2018). A child will be above the 93rd percentile for the population, the traditional index of statistical deviation if parents report that three or more of the 12 SCT items occur frequently or more frequently (scores of 3–4). Each item for which the parents report three or four points is deemed to be present. In total, the presence of SCT is mentioned if three or more of the items are present.
Stroop TBAG test
This test assesses the cognitive ability to direct attention, conceptual flexibility, and the processing speed of the mind (Stroop, 1935). This test reflects three basic processes: selective attention, reading, and color naming. The Stroop Test is one of the tests included in the Neuropsychological Test Battery for Cognitive Potentials and is considered the “gold standard” of attention measures. The test measures the ability to change the perceptual setup according to changing demands and under a “disruptive influence”; the ability to suppress a habitual behavior pattern, and focused/selective attention, and was used in this study to evaluate cognitive potential. The Turkish validity and reliability study was performed by Karakaş et al. (1999). Three types of scores including the time between the beginning and the end of each subtest, the number of errors made, and the number of corrected responses are calculated in the Stroop Test TBAG form.
Statistical analysis
Statistical data were analyzed using SPSS Statistics 22 package program. Continuous variables were shown as mean ± standard deviation (SD); categorical variables were shown as the numbers (n) and percentage. Comparisons of the groups were performed using the chi-square test, Fisher’s exact test for categorical variables, and Mann–Whitney U test for continuous variables. Correlations were evaluated using Spearman’s correlation coefficients. A value of p < .05 was considered statistically significant.
Ethics
Ethical approval for the study was obtained from the local ethics committee and the study was conducted in accordance with Good Clinical Practice procedures and the current revision of the Declaration of Helsinki (2021/2159).
Results
Socio-demographic and clinical characteristics
Sociodemographic and clinical characteristics of participants.
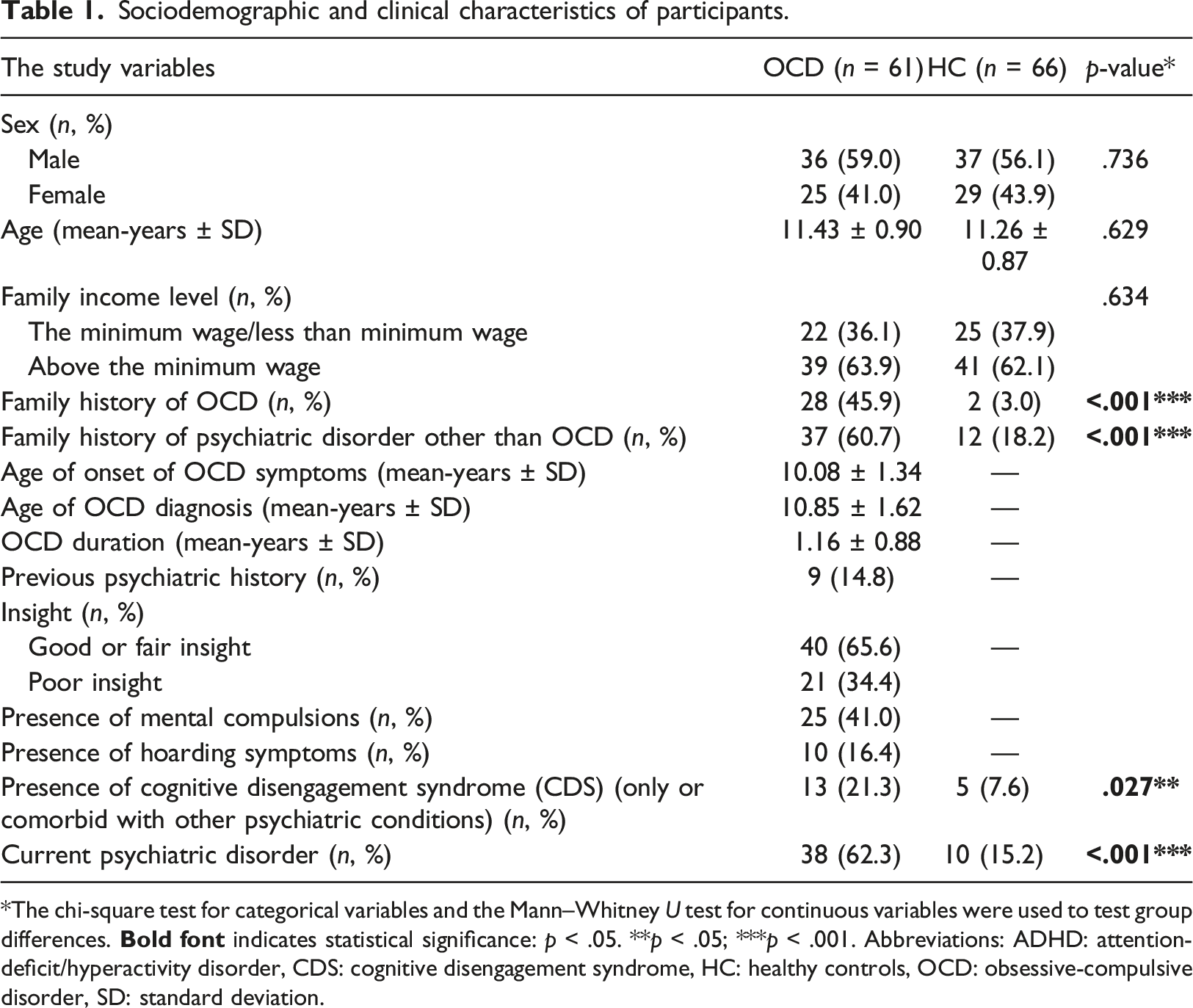
*The chi-square test for categorical variables and the Mann–Whitney U test for continuous variables were used to test group differences.
According to the results of the psychiatric examinations, elevated symptoms of CDS (solely or comorbid with other psychiatric disorders) were found in 21.3% (n = 13) of the patients with OCD and 7.6% (n = 5) of the control group; the difference was statistically significant (p = .027). In addition, it was detected that there was a significant difference between the groups in terms of current psychiatric disorder (p < .001); 15.2% (n = 10) of the participants in the control group were diagnosed with at least one psychiatric disorder. On the other hand, in the study group, 62.3% (n = 38) of the patients with OCD had at least one psychiatric disorder diagnosis other than OCD. The socio-demographic and clinical characteristics of participants are presented in Table 1.
Comparison of the MOCI, BCAS, and stroop test scores between the OCD and control groups
Comparison of the MOCI, BCAS, and stroop test scores between the OCD and control groups.
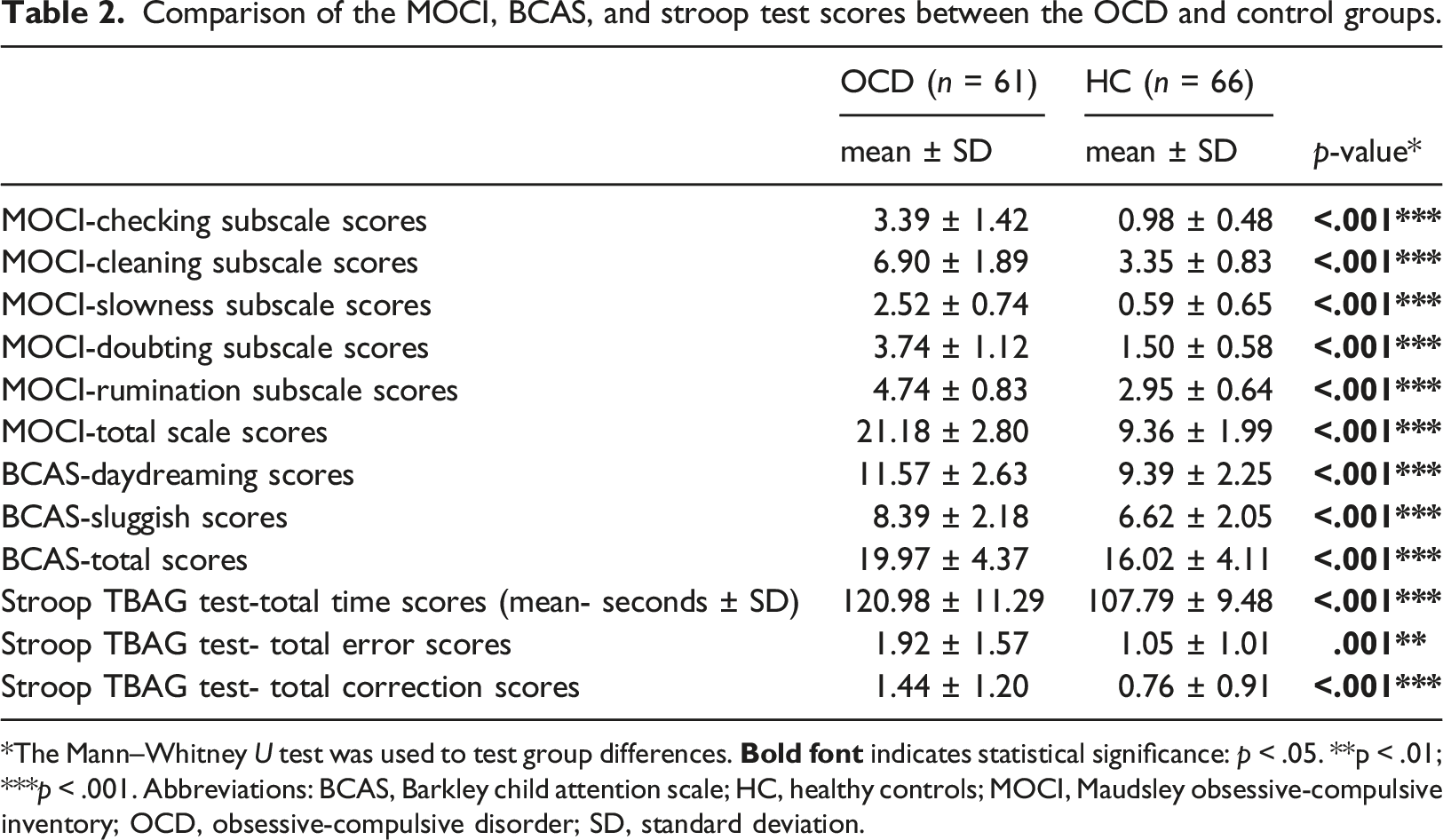
*The Mann–Whitney U test was used to test group differences.
Correlations between BCAS scores and MOCI and stroop TBAG test scores
Correlations between BCAS scores and MOCI and stroop TBAG test scores.
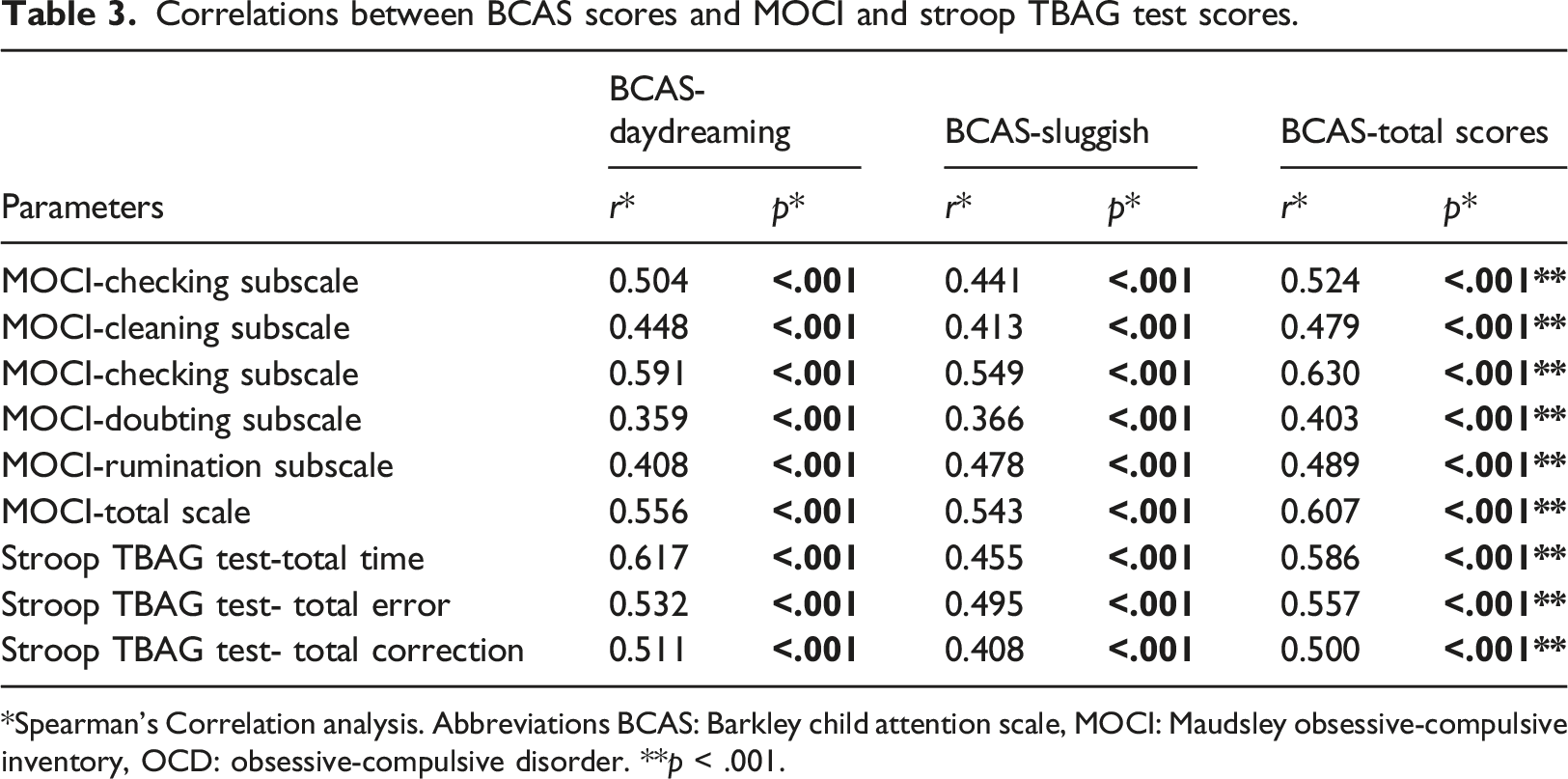
*Spearman’s Correlation analysis. Abbreviations BCAS: Barkley child attention scale, MOCI: Maudsley obsessive-compulsive inventory, OCD: obsessive-compulsive disorder. **p < .001.
Clinical features regarding CDS in the OCD group
Clinical features regarding CDS in the OCD group.
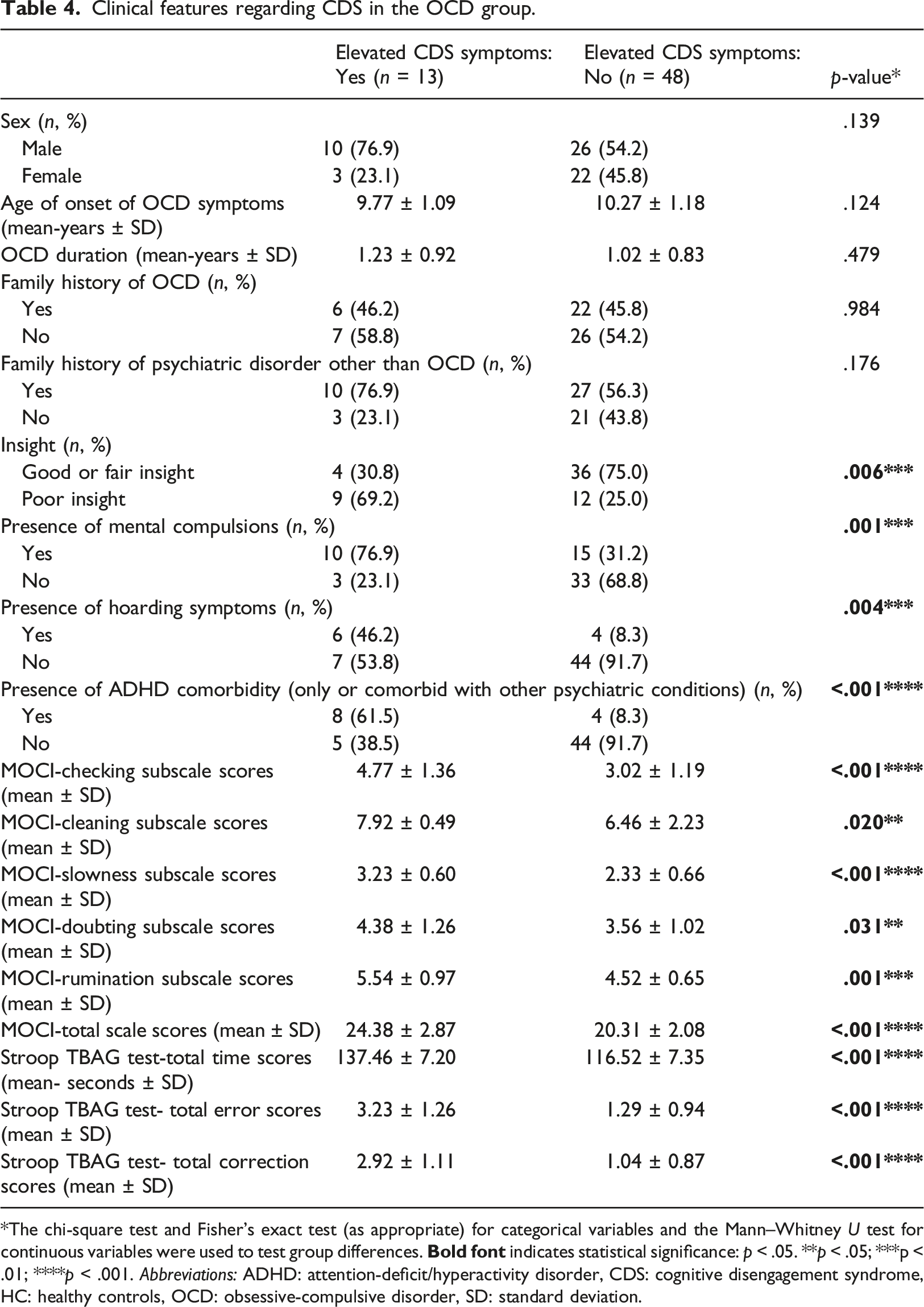
*The chi-square test and Fisher’s exact test (as appropriate) for categorical variables and the Mann–Whitney U test for continuous variables were used to test group differences.
Discussion
To our knowledge, this study is the first study on CDS symptom frequency in OCD. Our findings contribute to the literature by demonstrating the high frequency of elevated CDS symptoms in children with OCD and the positive correlation between increased OCD symptoms and elevated CDS symptoms.
In our OCD sample, the frequency of elevated CDS symptoms was detected to be 21.3%, and this rate was significantly higher compared to the control group (7.6%). More importantly, the frequency of CDS symptoms and OCD symptoms showed a significant positive association. Poor insight, hoarding symptoms, mental compulsions, and the frequency of concomitant ADHD were found to be significantly higher in OCD-elevated CDS symptoms coexistence compared to OCD patients without elevated CDS symptoms. Again, patients with OCD and elevated CDS symptoms performed worse on cognitive testing than patients with low CDS symptoms, suggesting a more severe attention deficit and greater cognitive impairment.
Although the phenomenology of OCD and CDS may appear to differ, both conditions have similar characteristics such as attention problems, high ADHD comorbidity, various deficits in frontal and executive functions, and being associated with internalizing symptoms (Camprodon-Rosanas et al., 2019; Creque & Willcutt, 2021; Flannery et al., 2017; Geller et al., 2018; Jacobson et al., 2018; Shin et al., 2014; van den Heuvel et al., 2010). It seems that individuals with OCD and CDS often present similar neuropsychological profiles. For example, both disorders tend to show lower performance on executive function tasks such as working memory, planning, and response inhibition, compared to non-psychiatric controls (Camprodon-Rosanas et al., 2019; Creque & Willcutt, 2021; Flannery et al., 2017; Geller et al., 2018; Jacobson et al., 2018; Mueller et al., 2014; Shin et al., 2014). In many studies evaluating neuropsychological functioning, it was determined that children with CDS act more slowly, and process and respond to stimuli for longer times. In addition, it has been found that CDS greatly compromises task performance by slowing down task-related processes and CDS symptoms were associated with poor processing speed (Barkley, 2013; Burns & Becker, 2021; Camprodon-Rosanas et al., 2017; Creque & Willcutt, 2021; Flannery et al., 2017; Jacobson et al., 2018). Similarly, there are many studies showing that OCD affects neuropsychological performance and leads to neurocognitive impairment, various cognitive deficits related to frontostriatal functions, and processing speed weakness (Geller et al., 2018; Shin et al., 2014; van den Heuvel et al., 2010). Previous studies have found that OCD patients have various deficits in attention processing and executive functions and it has been reported that executive functions are inhibited, and attention and cognitive flexibility functions are impaired in individuals with OCD and it is associated with lower general cognitive functionality (Geller et al., 2018; Shin et al., 2014; van den Heuvel et al., 2010). In addition to these findings in the literature, we also found that patients with OCD accompanied by elevated CDS symptoms had a higher frequency of OCD symptoms and showed poor performance on cognitive testing compared to the patients with low levels of SCT symptomatology. Our results also showed that in patients with OCD and elevated CDS symptoms concomitantly, there were more neurocognitive weakness and attention deficits. Thus, our findings provide important data to the literature by showing that increased CDS symptoms in OCD cause more severe attention deficit and greater cognitive impairment.
In addition, CDS and OCD may also share a similar neurobiological basis such as frontostriatal pathophysiology suggesting common etiology, given that ADHD and OCD have similar neuropsychological impairments in executive functions, and these disorders frequently co-occur (Vloet et al., 2006). Another explanation for the high frequency of elevated CDS symptoms detected in this study may be that OCD may lead to phenotypic expressions similar to CDS symptomatology. For example, a long time and intense mental pursuits spent on obsessions and compulsions in patients with OCD may reduce the capacity for basic cognitive processes, impact time management and concentration, cause a slower reaction/movement and getting lost in thoughts, which are also seen in CDS (Fitzgerald et al., 2021; Shin et al., 2014; Stern et al., 2017). Furthermore, given the potential associations of both OCD and CDS with mind-wandering (Becker & Barkley, 2021; Fredrick et al., 2020; Seli et al., 2017; Wang et al., 2021), similar behavioral symptoms (e.g., not paying attention to the surrounding environment) may be seen in both conditions as a reflection of different internal states that are difficult to differentiate. That is, in both cases, people may be internally focused because they are mind-wandering, worrying, ruminating, etc. Further, these different internal states could produce the same types of impairments on neurocognitive tests, including the Stroop. All of this may lead to individuals with OCD artificially being elevated on CDS symptoms, or vice versa. However, research is still needed to understand to what extent these different internally focused processes are at play among individuals with elevated CDS symptoms and OCD.
Besides, given that most of the patients with elevated CDS symptoms in our sample also had ADHD, the coexistence of elevated CDS symptoms and OCD we detected in our study may possibly represent the comorbidity between OCD and ADHD. From a neurodevelopmental point of view, impaired neuronal maturation processes or insufficient neuromaturational processes in ADHD and pediatric OCD (Abramovitch et al., 2015) may also cause an increased frequency of OCD-CDS association, considering the relatively low mean age of the sample in our study. However, since there is not enough data on the onset of symptoms for CDS symptoms in our study, depending on the results of our study, it is difficult to interpret whether the CDS symptoms are the result of OCD and other associated clinical manifestations, or whether there is really a coexisting condition. There is a need for more research to clarify the relationship between CDS and OCD.
One of the important findings of our study was that there was a significant relationship between high levels of SCT symptomatology and the clinical features of OCD, including poor insight, the presence of hoarding symptoms, and mental compulsions. This result can be explained by the fact that these clinical features are associated with the severity of the symptoms, treatment compliance problems, and loss of functionality in clinical practice (Samuels et al., 2014; Sharma et al., 2021). Furthermore, the presence of mental compulsions and lack of insight may cause patients to spend most of their time with problems regarding OCD, which may result in decreased attention capacity, deficiency in time management skills, and ultimately more functional impairment. This may cause the patient to seem more lethargic and slow. Significantly higher OCD symptoms and poor performance on cognitive testing in those with elevated CDS symptoms may also be associated with this result.
Limitations and conclusion
When considered together, the results of the current study provide the first evidence that the high levels of SCT symptomatology in pediatric OCD and the elevated CDS symptoms are substantially related to the increased OCD symptoms. Therefore, our data offer an important step towards revealing the relationship between CDS and OCD in children. Additional strengths of the study include the use of a semi-structured clinical interview. However, this study has some limitations. First, we used only the attention-related Stroop-TBAG test in the evaluation of the neuropsychological profile, other neuropsychological tests were not applied. Second, the age range of our sample was relatively narrow. This limited us to analyze the relationships between CDS and age, age of onset of OCD symptoms, and disease duration. Third, we did not evaluate patients who had not taken any medication. Again, tic disorders were entirely excluded from the analysis, which may have weakened the findings, because tic disorders could be part of what increases the likelihood of coexistence between OCD and CDS. Finally, the cross-sectional nature of the study design and our small sample size did not allow us to establish cause-effect relationships and make causal attributions. Our findings need to be confirmed by further studies using other neuropsychological tests, involving a wider age range and treatment process. The lack of information on CDS-OCD coexistence needs to be addressed by further research. In addition, it would be extremely valuable to re-evaluate the co-occurrence of OCD and CDS after remission from OCD. Thus, it will be possible to prove and clarify whether OCD temporarily causes CDS symptoms or whether CDS and OCD are concomitant conditions.
Footnotes
Acknowledgements
The authors would like to thank all the children and their families for their collaboration with the study.
Author contributions
Study design and method: AUC, IU. Data collection: AUC, IU, GT. Analysis of data: AUC, IU, CMI. Preparation of original draft: AUC. Review: IU.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.