
Abstract
Background
Mental disorders affect around 14% of adolescents worldwide and often lead to lasting cognitive and emotional difficulties. Executive functions (EF) are frequently impaired and health-related quality of life (HRQoL) is reduced. Chess has been proposed as a low-cost cognitive remediation training (CRT). This pilot study examined whether a chess-based CRT could enhance EF and HRQoL in adolescents with mental disorders.
Methods
A quasi-experimental study was conducted at a child and adolescent psychiatry department. Participants aged 13–17 years were assigned to either a six-week chess intervention (experimental group, EG) or treatment as usual (control group, CG). Both groups received standard multidisciplinary therapy, while the EG additionally participated in weekly 90-min chess sessions based on The King’s Plan for Kids. Cognitive flexibility (DCCS), inhibitory control (Stop-Signal Task), sustained attention (d2-R), and working memory (n-back task) were assessed alongside HRQoL (KIDSCREEN-27). Data were analyzed using t-tests.
Results
Thirty-three adolescents were included (19 EG, 14 CG; 82% female). The EG showed significantly faster reaction times in the working memory task (p = .016, d = 0.79) and greater Psychological well-being CG (p = .035, d = 0.67). No significant group differences were found for other EF measures.
Conclusion
Chess-based CRT was associated with improved working memory efficiency and psychological well-being, supporting its potential as a feasible, engaging, and low-risk adjunct to standard therapy. Larger randomized trials are needed to confirm these preliminary results.
Plain Language Summary
Many adolescents experience mental health problems that can make it harder to think clearly, focus, and handle emotions. These difficulties often affect their daily life and overall well-being. This study explored whether playing chess could help improve certain thinking skills (so called executive functions) and quality of life in young people receiving mental health treatment. The study took place at a child and adolescent psychiatry department between 2022 and 2024. Thirtythree adolescents aged 13 to 17 took part. All received standard therapy, but one group also joined a six-week chess program with weekly 90-min sessions using a structured training plan called The King’s Plan for Kids. The researchers tested several thinking abilities, such as attention, memory, and flexibility, as well as health-related quality of life before and after the program. The results showed that adolescents who played chess became slightly quicker in a memory task, suggesting their working memory worked more efficiently. More importantly, they also reported feeling better psychologically compared to those who received only standard care. Other thinking skills, such as attention and cognitive flexibility, did not show clear improvements. Overall, playing chess alongside regular therapy was safe, enjoyable, and linked to better mood and mental efficiency. While this was a small pilot study, the findings suggest that chess could be a helpful and low-cost way to support cognitive and emotional recovery in young people with mental health challenges. Larger studies are needed to test these results more clearly.
Keywords
Introduction
According to the World Health Organization (World Health Organisation WHO, 2021) 14% of 10- to 19-year-olds worldwide experience mental health problems, most commonly emotional and behavioral disorders. The associated costs pose significant challenges for both healthcare systems and society (European Union OECD, 2016). This is particularly concerning as, in some cases, these disorders persist into adulthood—around half of adults with mental disorders report symptom onset during childhood or adolescence—increasing the risk of long-term impacts on development, quality of life, and daily functioning (Fuchs et al., 2013; Hammud et al., 2023; Klipker et al., 2018).
Mental disorders in children and adolescents, for example the prevalent and commonly studied attention deficit hyperactivity disorder (ADHD), anorexia nervosa, or depression, are often linked to cognitive impairments, particularly in executive functioning (EF), including cognitive flexibility, inhibition, sustained attention, and working memory (e.g., Cortese et al., 2015; Goodall et al., 2018; Lima et al., 2018; Tchanturia et al., 2017; Wang et al., 2023). Thus, cognitive functioning more broadly refers to mental abilities such as attention or memory whereas EF more specifically describes higher-order control processes that regulate thoughts and actions in a goal-directed manner. In this study, we focus on EF as a core aspect of cognitive functioning that is frequently impaired across different child and adolescent mental disorders. Although the developmental pathways and clinical presentations of these disorders differ, they share transdiagnostic difficulties in EF, which are closely related to everyday functioning and treatment response. These children and adolescents also typically report a significantly lower quality of life (QoL), specifically health-related QoL (HRQoL), than their peers—often comparable to or worse than that of individuals with physical illnesses (Bastiaansen et al., 2020; Dey et al., 2012; Klipker et al., 2018; Otto et al., 2021; Sawyer et al., 2002). Furthermore, difficulties in EF and poor self-regulation have been suggested to negatively impact QoL in children with emotion regulation disorders, indicating a possibly causal relationship (Hammud et al., 2023).
Conversely, better EF is not only associated with higher QoL (Hammud et al., 2023; Wang et al., 2023), but also with reduced risk of disease recurrence (Wang et al., 2022) and greater therapy engagement or shorter hospital stays (Jeste et al., 2003; McKee et al., 1997). EF can be improved throughout childhood and adolescence through training and targeted interventions (Diamond, 2013; Serpell & Esposito, 2016; Tchanturia et al., 2017) and are thus essential in the context of mental disorders. In this sense, strengthening EF may not only reduce core symptoms in some disorders, but also help young people better understand, remember, and apply psychotherapeutic content in everyday life. To this end, cognitive training can enhance psychotherapeutic outcomes (Bowie & Harvey, 2006). Diamond (2013) further emphasizes the importance of supporting children in developing strong EF, given its ties to QoL. Specifically, Cognitive Remediation Training (CRT) has been shown to improve EF and is increasingly used in this context (Cella et al., 2016). It has shown promising effects on inattention symptoms and working memory in ADHD (Cortese et al., 2015), cognitive flexibility, problem-solving, and QoL in ASD (Hajri et al., 2019; Pasqualotto et al., 2021), as well as attention and other EF in psychosis (Anagnostopoulou et al., 2019). However, mixed results have also been reported—for example, in anorexia nervosa (Tchanturia et al., 2017). Overall, these findings suggest that CRT represents a transdiagnostic adjunctive approach that targets common cognitive mechanisms across different mental disorders, rather than being specific to one diagnosis.
Similarly, chess has gained popularity as a cognitive and social training tool. Reflecting its global appeal and potential educational benefits, the European Parliament (European Parliament, 2012) recommended the inclusion of chess in school curricular, as play—including chess—has been shown to support both cognitive and social development (Aciego et al., 2012; Cordier et al., 2009). Playing chess engages multiple EF, such as cognitive flexibility, inhibition, attention, memory, problem-solving, and planning (Bilalić et al., 2009; Unterrainer et al., 2006). From a psychological perspective, chess requires children and adolescents to maintain complex positions and plans (working memory), inhibit impulsive moves (inhibitory control), sustain concentration over time (sustained attention), and flexibly adjust strategies in response to the opponent (cognitive flexibility), thereby closely mirroring the EF domains that are frequently impaired across many mental disorders. Chess players in grades 5 to 9 have demonstrated better mathematical problem-solving and metacognitive abilities compared to control groups (Kazemi et al., 2012). Similarly, children who play chess show improvements not only in cognitive abilities such as EF (Ramos et al., 2018) but also in socio-emotional aspects such as self-confidence (Aciego et al., 2012).
Despite growing interest, research on the specific cognitive effects of chess in young people with mental disorders remains limited—especially regarding EF and QoL- and studies primarily focused on ADHD. They have reported positive effects of chess on concentration, listening skills, and task focus in children aged 11 to 13 (ElDaou & El-Shamieh, 2015) as well as reduced ADHD symptoms—including inattention and hyperactivity—in children aged 6 to 17 (Blasco-Fontecilla et al., 2016). However, it is largely unknown whether similar cognitive and well-being benefits can be observed in more heterogeneous, clinically treated samples of adolescents with various mental disorders, as typically seen in routine inpatient care. More broadly, research on chess’s effects on cognitive functions such as EF in children and adolescents is mixed and typically yields small to moderate effect sizes (Sala & Gobet, 2016).
Regarding QoL, a study in school children examined important aspects of QoL by self-report measures of school satisfaction, engagement as well as self-efficacy, and found self-perceived positive effects by chess, e.g. on self-efficacy or engagement in learning (Chitiyo et al., 2023). A pilot study in adults found that female chess experts showed increased satisfaction with life and less physical complaints than the average female population (Vollstädt-Klein et al., 2010). A study in older adults found that a 12-week chess-training protocol with two 60-min sessions per week improved cognition, i.e., attention, processing speed and EF, and QoL (Cibeira et al., 2021).
Moreover, existing findings suggest that chess has potential as an effective therapeutic intervention for enhancing EF and QoL also in the population of adolescents. It also offers several advantages: it is simple, cost-effective, free from side effects, and generally well-accepted by children and parents. Furthermore, chess can be implemented in various settings (inpatient, outpatient, or at home) and promotes social integration, making it a versatile intervention (Agarwal, 2023; Blasco-Fontecilla et al., 2016).
Consequently, an innovative therapeutic approach for children and adolescents with mental disorders involves chess-based CRT. This pilot study aimed to explore whether chess-based CRT could improve cognitive flexibility, inhibitory control, sustained attention, and health-related quality of life (HRQoL—both physical and psychological well-being) in a naturalistic sample of adolescents with various mental disorders receiving inpatient psychiatric and psychotherapeutic treatment. Rather than focusing on a single diagnosis, we deliberately adopted a transdiagnostic perspective to examine whether adolescents with different mental disorders, but shared EF difficulties, may benefit from the same chess-based intervention in a routine clinical setting. We hypothesized that chess training, delivered as a six-week add-on intervention, would improve (1) cognitive flexibility, (2) inhibitory control, (3) sustained attention, (4) working memory and both (5) physical and (6) psychological well-being compared to treatment as usual (TAU) alone.
Materials and Methods
Procedure and Participants
This quasi-experimental pilot study was conducted at the Department of Child and Adolescent Psychiatry and Psychotherapy (CAP), Central Institute of Mental Health (CIMH), Mannheim, Germany. The non-equivalent group design resulted in a 2 (group: experimental, control) × 2 (time: pre-test, post-test) mixed-factor design, with time as the within-subjects factor and group the between-subjects factor. For logistic reasons, group allocation was quasi-randomized to either the experimental group (EG; enrolment and data collection September 2022 until September 2023) or the control group (CG; data collection and enrolment July 2024 until April 2024). An a priori power analysis for one-sided t-tests for independent samples was conducted out using G*Power 3.1.9.7 (Faul et al., 2009). A medium effect size of d = 0.5 (Cohen, 1988) was targeted. Based on a desired power of (1 - β) = .80, an error probability of α = .05 and groups of equal size, a total sample size of 102 adolescents was targeted, with 51 participants in each EG and CG.
Inclusion criteria encompassed: age between 13 and 17 years and sufficient verbal and written communication abilities, both to ensure that participants could meaningfully engage with the chess training and complete assessments. Further, and to ensure full participation over the six-week study period, patients (in-house, outpatient, or in inpatient-equivalent settings) were included during the first three weeks after treatment initiation, provided their treatment duration was expected to be adequate.
Exclusion criteria encompassed severe neurological, psychiatric, or somatic comorbidities (including a body mass index below 14) which in the opinion of the treating physicians, contraindicates participation in the study, and placement under the German Civil Code).
Ongoing medication use (e.g., antidepressants, ADHD medication) was permitted during study participation and was not defined as an inclusion or exclusion criterion. We included all adolescents, i.e. both boys and girls, and recorded sex assigned at birth, as well as social gender, as routinely documented in the clinic’s patient management system.
As financial compensation, participants received €20 after completing all assessments, which was donated by the Munich Chess Foundation (Münchener Schachstiftung, https://schachstiftung-muenchen.de). The overall study of which this data derived from was pre-registered at ClinicalTrials.gov (NCT05698615). Study procedures were in line with the recommendations of the World Medical Association (revised Declaration of Helsinki) as well as in accordance with good clinical practice guidelines, and were approved by the local Ethics Committee of the of the Medical Faculty Mannheim, Heidelberg University (approval # 2021-593).
After identifying eligible patients using the clinic’s patient management system, study participation was proposed by their practitioner. Written informed consent was obtained from the legal guardians and informed assent was obtained from the children and adolescents. All parties were informed via telephone, email, or in person and received written information about the study.
Data were collected at two time points, see Figure 1, using the electronic data capture tool REDCap, hosted locally at our institute (Harris et al., 2019): before (A1) and after (A2) the six-week study period. Each assessment lasted approximately 2 hours and included several neuropsychological tasks and questionnaires, administered in the same order and at approximately the same time of day for all participants. Study procedure including two assessment time points, A1 and A2. EG = experimental group, CG = control group, TAU = treatment as usual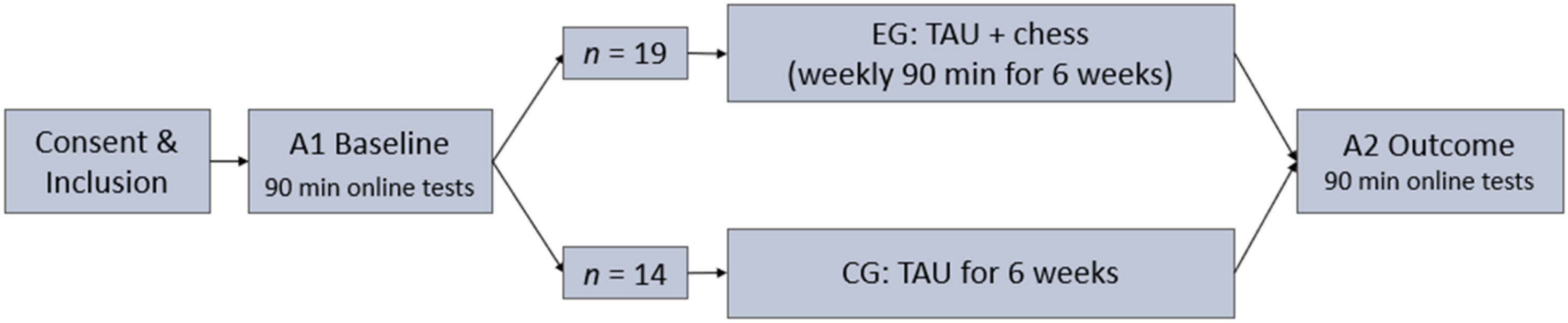
Both the control group (CG) and experimental group (EG) received TAU, delivered by a multidisciplinary team. This included psychotherapy—primarily cognitive behavioral therapy (CBT)—as a core component, along with pharmacotherapy when necessary.
Chess Training
Participants in the EG took part in a 90-min, in-person chess training – conducted in a group-setting - led weekly in the late morning by a chess trainer (RS and AS) over the six-week study period. First, the basic rules of chess were introduced using a demonstration board and video assistance based on the established training concept Smart by Chess – The King’s Plan for Kids (Kindermann & Exler, 2023). This concept teaches the thinking and problem-solving strategies of chess players in an accessible way, aiming to develop EF through an engaging, creative, and playful approach. When playing chess, players must hold positions and planned moves in mind (working memory), resist impulsive or premature moves (inhibitory control), maintain concentration during prolonged games (sustained attention), and flexibly adapt their strategy in response to the opponent’s actions (cognitive flexibility), making these domains particularly suitable as outcomes for a chess-based intervention. Each session began with chess yoga for relaxation and concentration. The trainer then introduced theoretical concepts and integrated physical exercises, role-playing, and concentration techniques. This was followed by active chess play, supported with guidance and tips. Sessions were balanced between theory and practice. For this study, the trainer (RS) adapted The King’s Plan for Kids to better suit the adolescent age group. Adaptations are described in Supplemental Table 4.
Psychometric Questionnaires
The self-report KIDSCREEN-27 questionnaire was used to assess HRQoL in children and adolescents aged 8 to 18 years (Ravens-Sieberer et al., 2014). It consists of 27 items across five scales: Physical well-being, Psychological well-being, Autonomy and Parent relations, Social support and peers, and School environment (internal consistency α = .80 – .84; test-retest reliability .61 – .74). For this study, the Physical well-being scale (assessing activity level, energy, and health—lower scores reflect exhaustion, low energy, and feeling unwell; α = .80; test-retest reliability .65) and the Psychological well-being scale (covering mood, emotions, self-perception, and life satisfaction—lower scores indicate low self-esteem, unhappiness, and depressive feelings; α = 84; test-retest reliability .64) were used.
Neuropsychological Tasks
All participants completed neuropsychological tasks (35 minutes) and, after a short break, questionnaires (30 minutes). Tasks were administered via an in-house JavaScript-based platform. For the present analyses, the Dimensional Change Card Sort Test (DCCS; (Zelazo, 2006)), the Stop-Signal Task (SST; (Sebastian et al., 2013)), the d2 Test of Attention – Revised (d2-R; (Brickenkamp et al., 2010)), and the n-back working memory task (Callicott et al., 1999) were used to assess cognitive flexibility, inhibitory control, attention/concentration, and working memory capacity respectively.
DCCS performance was scored using the two-vector method (Zelazo et al., 2014), which combines accuracy and reaction time (RT) for participants with >80% accuracy. This method captures the RT “cost” associated with EF (Davidson et al., 2006). Each vector ranges from 0 to 5, yielding a total score from 0 to 10. For participants with ≤80% accuracy, the score equaled the accuracy vector. Higher scores indicate better performance. The change in DCCS scores from pre- (A1) to post-test (A2) was used; positive differences reflect improvement.
Inhibitory control was assessed using the Stop-Signal Reaction Time (SSRT), calculated via the race model (Logan & Cowan, 1984) by subtracting the mean Stop Signal Delay (SSD) from the mean RT in correct go trials. Shorter SSRTs reflect better inhibitory control. Negative SSRT differences (A2 minus A1) indicate improvement, with greater negative values reflecting stronger gains.
For the d2-R, sustained attention (KL) was calculated by subtracting missed targets (AF) and confusion errors (VF) from the total correct targets (BZO): KL = BZO – AF – VF. Higher KL values indicate better attention. Processing speed (BZO) and accuracy (F%) were also derived, with F% = 100 × (AF + VF)/BZO; lower F% indicates higher accuracy. Only data from trials 2–13 were used (excluding first and last lines). Change scores between A2 and A1 were used, with positive values indicating improvement.
Working memory capacity was assessed using the n-back working memory task in a low (0-back) and high cognitive load condition (2-back). Outcome measures include the error rate (in %) as well as reaction times in the 2-back condition.
Statistical Analyses
Statistical analyses were conducted using IBM SPSS Statistics version 29.0.0 (IBM Corp., 2022) with a significance level of α = .05. Group comparisons between the EG and CG were performed for the within-group mean change in the respective variable between times A2 and A1 as dependent variables. Two-tailed t-tests for independent samples and χ2-tests were applied. One-tailed t-tests with α = .05 were used to test the directional hypotheses, accompanied by 90% bias-corrected and accelerated (BCa) confidence intervals. Bootstrapping with 10,000 iterations was used to compute confidence intervals and conduct inferential tests. Dependent variables included the change in DCCS performance score (cognitive flexibility), SSRT and SSD (inhibitory control), d2-R KL score (sustained attention), error rate and reaction times for correct responses (working memory), and the sum scores for the Physical well-being and Psychological well-being scales. Changes in reaction times were calculated as percentage related to A1 reaction times. For all other variables mean differences between A1 and A2 were used. Analyses encompassed only participants with complete data for the relevant neuropsychological tests and questionnaires at both A1 and A2, thus leading to a reduced number of data sets available for specific analyses due to missing or invalid data
Results
Sample, Sociodemographics, and Comorbidities
After pre-screening, 92 patients in the CAP met the in- and exclusion criteria for potential participation, out of which 33 could be included in the study (19 EG, 14 CG; see CONSORT Flow Diagram, Supplemental Figure 1, also describing reasons for non-participation or drop-out). According to Verbruggen et al. (2019), SSRT scores were invalid for 12 participants (9 EG, 3 CG) and thus were not analyzed. Two EG participants were not suitable for the d2-R task analyses due to missing A1 data but had complete data for all other measures. Additionally, four participants (1 EG, 3 CG) were not suitable for the physical well-being analyses, and one (CG) from the psychological well-being analyses, due to missing data at A1 or A2.
The sample comprised mostly girls. In the experimental group (EG), there were 15 girls and 4 boys (biological sex; age: M = 15.16, SD = 0.96, range = 13–17 years). In the control group (CG), there were 12 girls and 2 boys (biological sex; age: M = 15.36, SD = 1.55, range = 13–17 years).
Social gender largely overlapped with biological sex. In the intervention one participant (assigned female at birth) identified as a boy, in the control group, two participants (assigned female at birth) identified as boys. For one participant (assigned female at birth) in the control group, information on social gender was not available. For main diagnoses of mental disorders, see Supplemental Table 1. For psychotropic medication, see Supplemental Table 2. Each participant in the EG attended at least two chess training sessions, with a maximum of six sessions (M = 4.653, SD = 1.754, Median = 5, Interquartile Range = 3). Three adolescents voluntarily choose to participate in a seventh session after the second study appointment.
Neuropsychological Data
DCCS performance scores were generally high, indicating good cognitive flexibility, with participants achieving over 80% of the maximum score at A1. The EG showed less improvement from A1 to A2 compared to the CG; however, the difference was not significant (t (16.57) = −1.33, p = .101, d = −0.52, ΔM = −0.67, BCaCI90% = [−1.58, 0.11]).
The SSRT in the EG decreased from A1 to A2, indicating an improvement in inhibitory control. In contrast, the CG showed a decline, with an increase in mean SSRT (M = 4.94, SD = 96.84). A one-tailed t-test for independent samples revealed a non-significant effect (t (19) = −1.02, p = .161, d = −0.45, ΔM = −34.58, BCaCI90% = [−96.49, 22.45]). Similarly, the EG showed an increase in mean SSD (M = 49.53, SD = 79.83), while the CG demonstrated a slight decrease (M = −10.94, SD = 123.37). However, group differences were not significant (t (19) = 1.32, p = .102, d = 0.58, ΔM = 60.47, BCaCI90% = [−2.67, 130.41]).
The EG showed a greater but non-significant improvement in sustained attention (d2-R KL) from A1 to A2 (M = 18.88, SD = 29.29) than the CG (M = 18.50, SD = 13.73; t (29) = 0.05, p = .482, d = 0.02, ΔM = 0.38, BCaCI90% = [−12.17, 12.55]). Likewise, neither BZO nor F% yielded significant results (BZO: t (29) = 0.67, p = .253, d = 0.24, ΔM = 12.13, BCaCI90% = [−14.17, 39.46]; F%: t (29) = 0.43, p = .335, d = 0.16, ΔM = 2.55, BCaCI90% = [−6.58, 12.04]).
The performance in the working memory task - measured by the number of errors in the N-Back task in the high cognitive load condition (2-back) - did not change from A1 to A2, neither in the EG (t (18) = .925, p = .367) nor in the CG (t (13) = .448, p = .663). However, the reaction times showed a larger reduction from A1 to A2 in the EG (85.90 % of the A1 value) compared to the CG (110.99 % of the A1 value). A one-tailed t-test for independent samples revealed a significant effect (t (31) = 2.23, p = .016, d = 0.79, ΔM = 25.09, BCaCI90% = [.81, 51.93]).
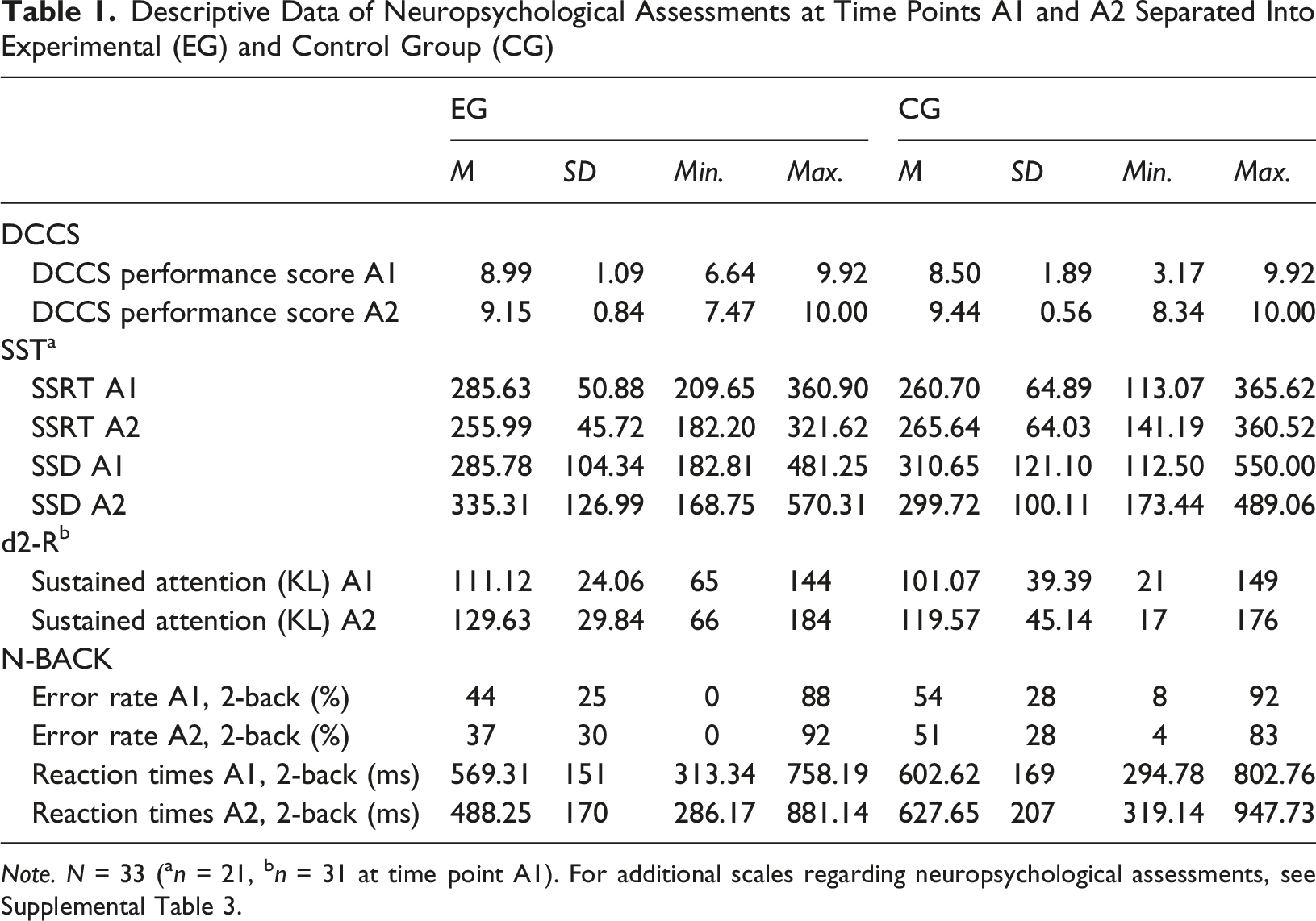
See Figure 2 and Table 1. A: Mean change in cognitive flexibility from A1 to A2 for experimental and control group. B: Mean change in inhibitory control measured by the SSRT from A1 to A2 for experimental and control group. C: Mean change in inhibitory control measured by the SSD from A1 to A2 for experimental and control group. D: Mean change in sustained attention from A1 to A2 for experimental and control group. E: Mean reaction time improvement from A1 to A2 for experimental and control group. Note. The error bars represent the 90% confidence intervals Descriptive Data of Neuropsychological Assessments at Time Points A1 and A2 Separated Into Experimental (EG) and Control Group (CG) Note. N = 33 (an = 21, bn = 31 at time point A1). For additional scales regarding neuropsychological assessments, see Supplemental Table 3.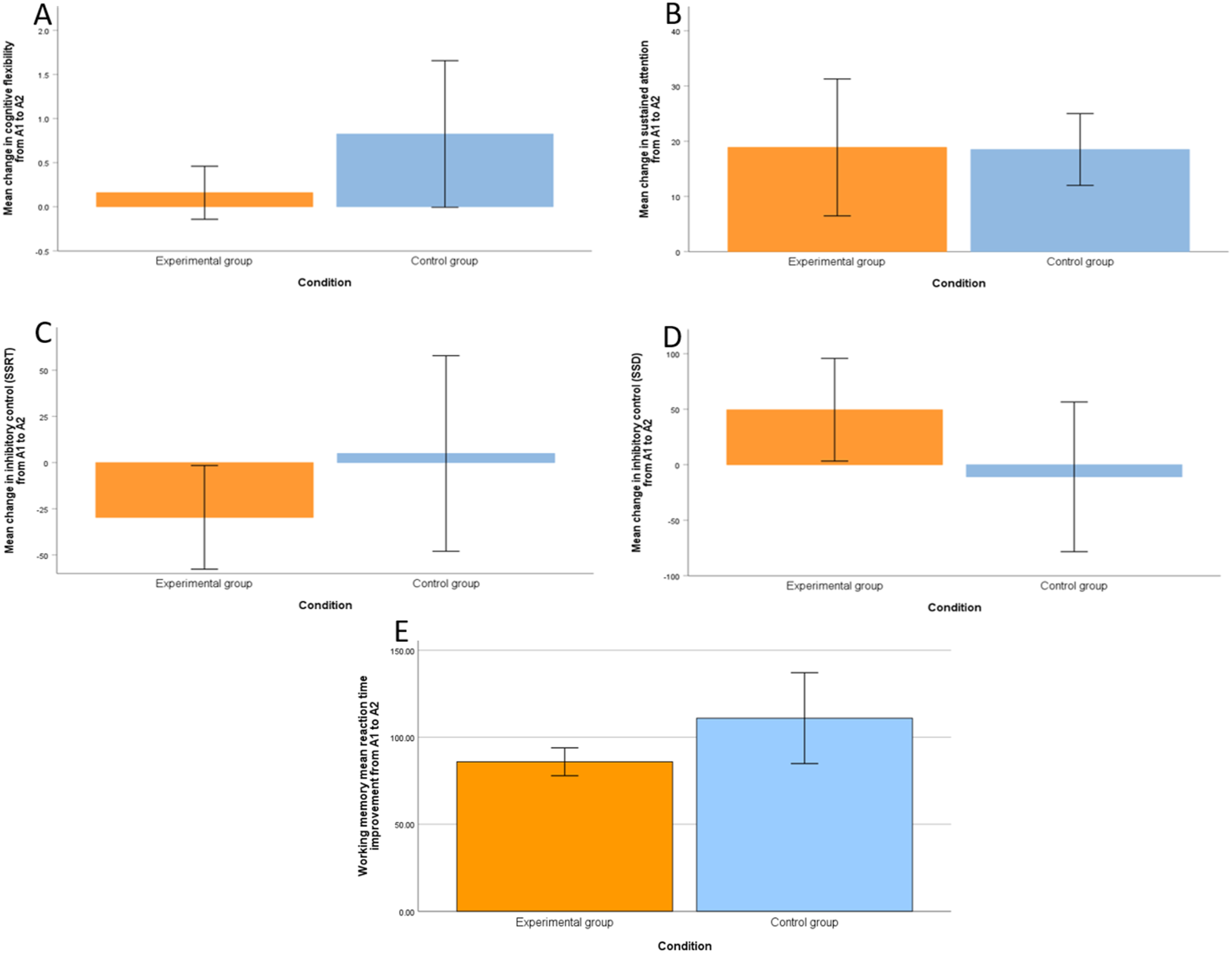
Quality of Life
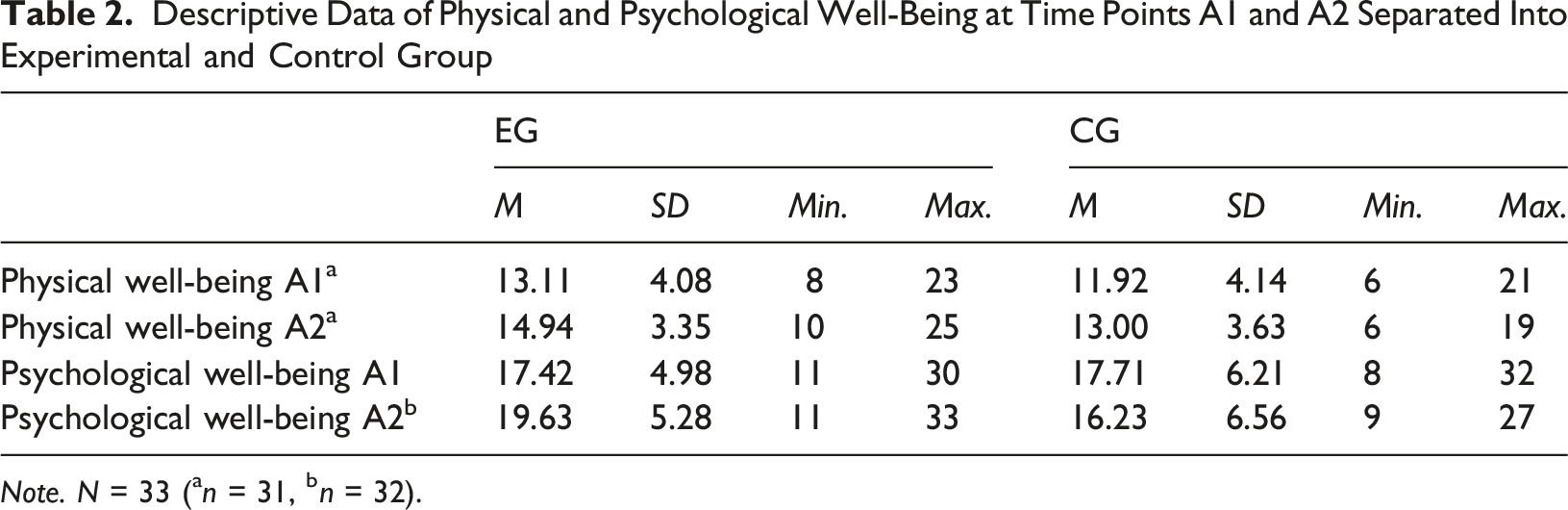
The EG showed a greater but non-significant improvement in physical well-being from A1 to A2 (M = 1.72, SD = 3.58) compared to the CG (M = 0.73, SD = 4.63), with a mean difference of ΔM = 0.99 (t (27) = 0.65, p = .261, d = 0.25, BCaCI90% = [−1.57, 3.66]).
In terms of psychological well-being, the EG showed a significant medium improvement (M = 2.21, SD = 5.16) from A1 to A2, whereas the CG showed a decline (M = −1.46, SD = 5.85; group comparison t (30) = 1.87, p = .035, d = 0.67, BcaCI90% = [0.38, 6.82]).
See Figure 3 and Table 2. A: Mean change in physical well-being from A1 to A2 for experimental and control group. B: Mean change in psychological well-being from A1 to A2 for experimental and control group. Note. The error bars represent the 90% confidence intervals Descriptive Data of Physical and Psychological Well-Being at Time Points A1 and A2 Separated Into Experimental and Control Group Note. N = 33 (an = 31, bn = 32).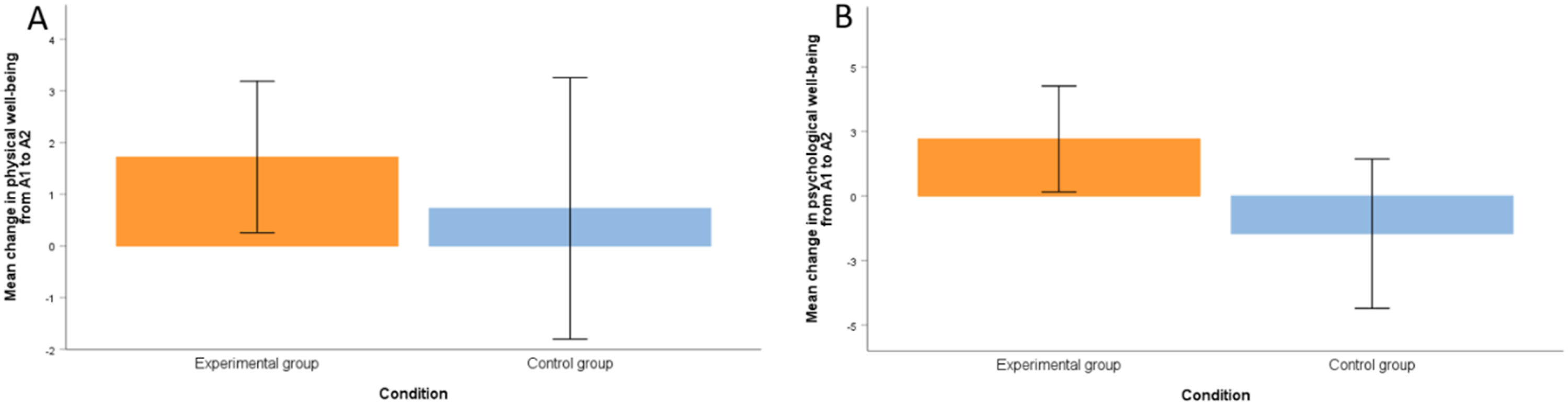
Discussion
The aim of this pilot study was to investigate whether a six-week chess training program, used as a therapeutic add-on, could improve EF and quality of life in adolescents with mental disorders compared to treatment as usual (TAU) alone. A clinical -experiment with quasi-randomization was conducted, involving two measurement points, an experimental group, and a control group. The chess intervention followed the concept of “The King’s Plan for Kids”. While the hypotheses regarding improvements in cognitive flexibility, inhibitory control, sustained attention, and physical well-being were not confirmed, the data supported a significant improvement in psychological well-being and working memory efficiency following the six-week chess intervention.
Hypothesis 1 postulated that chess training would improve cognitive flexibility compared to TAU; however, this was not supported. In fact, results showed a slight trend in favor of the control group. Both groups improved over time, but many participants already scored highly at baseline, suggesting ceiling effects that limited potential gains. These findings, alongside small sample sizes, wide confidence intervals, and unequal variances, hinder definitive conclusions (Dumont et al., 2022; Eichorn et al., 2018; Lessing et al., 2019). Additionally, a pre-/self-selection bias may have resulted in cognitively stronger individuals opting for chess (Blanch, 2022). Although the EG may have employed more strategic thinking (Unterrainer et al., 2006), the results diverge from prior studies reporting positive effects of chess on cognitive flexibility (Goncalves et al., 2014; Grau-Pérez & Moreira, 2017; Ramos et al., 2018) and are more consistent with findings of limited or no effects (Sala & Gobet, 2016, 2017).
Hypothesis 2, which anticipated improved inhibitory control following chess training compared to TAU, was also not confirmed. However, the EG’s slower reaction times may indicate increased deliberation and cognitive control (Blasco-Fontecilla et al., 2016; ElDaou & El-Shamieh, 2015), despite the absence of statistical significance. The CG’s superior baseline performance suggests that the EG had greater potential for improvement.
Hypothesis 3 predicted that chess training would improve sustained attention, but this was not supported. Both groups showed improvement, with the EG starting from a higher baseline, potentially limiting observable gains. The broader range of maximum scores in the EG may reflect increased individual variability. This pattern could suggest a general training or practice effect—rather than a chess-specific benefit—as noted by Daseking and Putz (2015). These findings contrast with previous studies reporting benefits of chess for children with ADHD (Blasco-Fontecilla et al., 2016; ElDaou & El-Shamieh, 2015), healthy children (Aciego et al., 2012), or following cognitive training (Anagnostopoulou et al., 2019; Cortese et al., 2015).
An exploratory analysis of processing speed revealed small, non-significant effects in the EG, with a higher increase in processed target items—again diverging from prior findings. This inconsistent pattern underscores the challenge of interpretation, especially given the increased risk of Type I error across multiple tests (Bühner & Ziegler, 2017). Finally, non-significant results for accuracy (F%) should be interpreted cautiously, due to the measure’s limited reliability (Daseking & Putz, 2015) and potential fatigue effects, as the d2-R was administered last in the test battery.
In Hypothesis 4 we expected a beneficial effect of chess training on working memory. Although both groups did not show an increase in working memory performance (i.e. number of errors), the EG showed a larger improvement regarding faster reaction times from A1 to A2 compared to the CG while keeping the error rate stable. This could indicate an enhanced working memory efficiency in the EG which is suggested to be a beneficial effect of chess (review by Williams et al., 2025).
While the expected improvement in physical well-being (Hypothesis 5) was not confirmed, Hypothesis 6 was supported, with a significant improvement observed in psychological well-being. This aligns with the positive findings reported by Aciego et al. (2012) on the impact of chess on QoL in healthy children and adolescents—particularly in areas such as happiness, which can be considered indicators of QoL. It is also consistent with evidence from other forms of CRT in individuals with mental disorders, both in adults (e.g., Tchanturia et al., 2017) and in children and adolescents (Pasqualotto et al., 2021).
The positive effect of chess-based trainings on improved EF and psychological well-being might be due to, firstly, the structured and goal-directed application of our chess-based training that explicitly targets EF. Therefore, increased EF could be expected based on training effects. Secondly, increased self-efficacy or perceived competence. Repeated practice and gradual improvement in successful problem solving could lead to mastery experiences that might strengthen the adolescents’ belief in their own abilities. Thirdly, playing in a group setting creates opportunities for positive social interaction and a sense of group belonging, which may enhance enjoyment and positive affect and, in turn, contribute to perceived improvements in quality of life. The small, non-significant upward trend in physical well-being might also be attributed to additional components of the intervention, such as physical activity (e.g., chess yoga). However, it remains unclear whether the observed effects on psychological well-being stem directly from chess itself, the group-based social interaction, or simply the engagement in an additional structured activity alongside TAU. In contrast, any cognitive improvements observed are more likely to be directly linked to the chess training.
Together, these cognitive, motivational, and social processes provide a plausible psychological framework that still warrants further, well-designed studies for understanding how a chess-based intervention could influence both EF and well-being in adolescents with mental disorders.
Strengths and Limitations
A key strength of this study is its direct investigation of chess training effects in adolescents with mental disorders—not only on EF but also on HRQoL, specifically physical and psychological well-being. Notably, it found a significant improvement in psychological well-being despite both groups receiving comprehensive TAU and the small sample size.
However, several limitations may affect the generalizability. The small and uneven sample likely influenced results, and replication with a larger, more balanced sample is needed to confirm effects. The intervention was not blinded, and quasi-randomization may have introduced selection bias—participants in the chess group may have been more cognitively proficient or motivated (Blanch, 2022). No stratification by diagnosis or treatment type was conducted which led to differences in diagnostic composition between groups and may limit internal validity. Also, our design does not allow for disorder-specific conclusions or detailed analyses of illness duration, treatment history, or change in psychotropic medication. Similarly, gender diversity or gender-related differences were not addressed in this study and should be acknowledged in more differentiated assessments of gender identity in future studies. The absence of an active control group further limits interpretability; comparing therapeutic chess to classical instruction within “The King’s Plan for Kids” could be informative. Prior chess experience or continued play beyond the intervention was not recorded, which could influence skill transfer. Attendance varied, and the interval between final session and follow-up was undocumented, which may also impact outcomes.
Cognitive test performance may have been affected by fatigue, particularly as the d2-R was administered last without a break.
Although impairments in EF vary across psychiatric diagnoses, we deliberately chose not to restrict participation to a single disorder. Our aim was to use an inclusive, transdiagnostic approach that reflects real-world inpatient child and adolescent psychiatry, where patients often present with complex symptomatology and multiple comorbid diagnoses. From a clinical perspective, it is highly relevant to examine whether adolescents with mental disorders in general may benefit from chess training.
Clinical Implications
This pilot study suggests that incorporating a chess training intervention into treatment as usual may offer clinically meaningful benefits for the psychological well-being of adolescents with mental disorders. The improvement in well-being, highlights the potential of chess training as a low-risk, cost-effective, and easily implementable supplement to standard care. While effects on EF were not robust—likely influenced by ceiling effects and the small sample size—the intervention may nonetheless promote greater reflection and more deliberate decision-making in some participants. Faster reaction times after chess training might suggest increased neural efficiency, which could be examined in future studies. Future research should seek to replicate these results in larger, more diverse samples, control for baseline differences, and further explore the mechanisms by which chess training may contribute to mental health and well-being in vulnerable youth. A promising direction for future research is to examine how EF relates to psychological well-being (e.g., Casey, 2023; Diamond, 2013), potentially as a mediating mechanism, as improvements in EF may contribute to better psychological outcomes.
Conclusion
This pilot study provides valuable insights into the potential of chess as a therapeutic intervention for enhancing EF and HRQoL in adolescents with mental disorders. While the findings did not demonstrate significant effects on cognitive flexibility, inhibitory control, or sustained attention, they did indicate a positive impact on psychological well-being and potentially working memory. Despite limitations, this study underscores the potential of chess as an accessible, engaging, and low-risk approach to supporting the mental health and well-being of adolescents facing psychiatric challenges.
Supplemental Material
Supplemental Material - Move by Move Towards Mental Health: A Quasi-Randomized Pilot Study on Chess as a Therapeutic Approach in Adolescents With Mental Disorders
Supplemental Material for Move by Move Towards Mental Health: A Quasi-Randomized Pilot Study on Chess as a Therapeutic Approach in Adolescents With Mental Disorders by Sarah Gerhardt, Stefanie Hoier, Alexandra Seeger, Roland Schmidt, Larissa Weber, Konstantin Mechler, Tobias Banaschewski, Alexander Häge, and Sabine Vollstädt-Klein in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgments
We would like to thank all children and adolescence for their study participation. We further thank Paul Illner for his assistance with the ethics application and the study setup, Yury Shevchenko for programming the neuropsychological test battery, as well as Sophie Frahm and Ronja Bednar for her assistance in data collection. We further thank Grandmaster Stefan Kindermann for his support during the implementation of the chess training “Der Königsplan für Kinder”.
Ethical Considerations
Study procedures were in line with the recommendations of the World Medical Association (revised Declaration of Helsinki) as well as in accordance with good clinical practice guidelines, and were approved by the local Ethics Committee of the Medical Faculty Mannheim, Heidelberg University (approval # 2021-593 on 2021-08-12).
Consent to Participate
All parties were informed via telephone, email, or in person and received written information about the study. Written informed consent was obtained from the legal guardians and informed assent was obtained from the children and adolescents.
Authors Contributions
SH and AS recruited the participants and collected the data. AH, LW and KM helped with the recruitment of the participants and data collection. RS and AS conducted the chess training. SH, SG and SVK performed the data analysis. SG and SH wrote the manuscript. SVK and TB were responsible for the study design of the original study and procured the funding of the original study. All authors commented on the manuscript, provided intellectual input, and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by grants from the Münchener Schachstiftung (Munich Chess Foundation) and the Deutsche Forschungsgemeinschaft (German Research Foundation; Project ID 421888313 and Project ID 402170461, TRR 265, recipient SVK).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AH: advisory board of Medice and speaker’s fees from Medice and Takeda. KM: speaker’s fees from Takeda and Medice. TB: advisory or consultancy role for AGB pharma, eye level, Infectopharm, Medice, Neurim Pharmaceuticals, Oberberg GmbH and Takeda, conference support or speaker’s fee from AGB pharma, Janssen-Cilag, Medice and Takeda, royalities from Hogrefe, Kohlhammer, CIP Medien, Oxford University Press. The present work is unrelated to these affiliations. All other authors state that they have no conflicts of interest.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.