
Abstract
Background
Insufficient school-night sleep is common among U.S. adolescents. The 2023 Youth Risk Behavior Survey (YRBS) includes a basic-needs support item about adult effort to ensure safety, clean clothes, and food.
Methods
We conducted a cross-sectional secondary analysis of the 2023 national YRBS. Insufficient sleep was defined as fewer than 8 hours on an average school night. Support was coded as present versus lacking. Survey-weighted models adjusted for demographic, behavioral, mental-health, and BMI covariates.
Results
Among students with nonmissing sleep data (n = 17,441), 76.8% reported insufficient sleep. In the sleep/support frame (n = 15,607), prevalence was 76.0% with support present and 82.0% with support lacking. In the multiply-imputed primary model (m = 20), lacking support was associated with a small, statistically detectable increase in insufficient sleep (aPR = 1.052, 95% CI 1.007 to 1.098; ARD = +4.3 percentage points, 95% CI + 0.5 to +8.1). A complete-case sensitivity model gave a comparable but less precise estimate (aPR = 1.036, 95% CI 0.990 to 1.085).
Conclusions
Lacking perceived basic-needs support marked higher unadjusted insufficient-sleep prevalence, but adjusted estimates were modest. Sleep screening and basic-needs assessment may be clinically useful together; longitudinal work is needed to clarify directionality.
Plain Language Summary
Many high-school students sleep less than the recommended amount on school nights. This study used 2023 national Youth Risk Behavior Survey data to examine whether sleep differed by students’ reports that an adult in their household tried hard to make sure their basic needs were met, such as safety, clean clothes, and enough to eat. Students who reported lacking this support had higher insufficient-sleep prevalence than students who reported support. After adjustment, the difference was small; the primary model was statistically detectable, while the complete-case sensitivity estimate was less precise. These findings do not prove that household support causes better sleep, but they suggest that sleep screening and basic-needs assessment may be useful together in adolescent care.
Keywords
Introduction
Most U.S. high school students do not get the recommended amount of sleep on school nights, and this shortfall has widened over the past decade (Centers for Disease Control and Prevention, 2024b). The Youth Risk Behavior Survey asks students how many hours they sleep on an average school night, and CDC classifies fewer than 8 hours as insufficient sleep for this age group. The threshold is clinically recognizable and useful for surveillance, but the ordinal distribution still matters: very short sleep may carry different risks than sleep that falls just below the recommended range. Short or disturbed sleep is associated with poorer mental health, suicidal behaviors, and neurocognitive development concerns (Marino et al., 2021; Wang et al., 2024; Yang et al., 2022). Sleep is therefore a clinical and prevention concern, not only a school-policy issue.
Family context may shape whether adolescents can obtain adequate school-night sleep. The 2023 national YRBS added a protective-experiences item asking whether an adult in the household tried hard to ensure basic needs such as safety, clean clothes, and enough to eat (Centers for Disease Control and Prevention, 2024a; Verlenden et al., 2024). The item captures adolescents’ perceived reliability of adult effort, and nothing more. It is not a measure of household income, caregiver warmth, or bedtime structure. A household that reliably meets these needs may also have more stable routines, lower material strain, or adult monitoring, but those mechanisms are not measured by this item and should be treated as explanatory context.
Bedtime routine and evening structure are not the same construct: a household may reliably ensure food, clothing, and safety and still lack the calmer evenings associated with longer sleep. We therefore frame basic-needs support as a clinically interpretable marker of household context, not as proof that routine quality explains sleep differences. Related evidence links food insecurity, parent-adolescent bedtime or waketime interactions, and school-start-time policies with sleep outcomes, but the present analysis tests only one cross-sectional YRBS exposure (de Camargo et al., 2024; Ewing et al., 2024; Yip et al., 2022).
We tested whether lacking household basic-needs support is associated with insufficient sleep in the 2023 national YRBS. We emphasize prevalence ratios, adjusted risk differences, and confidence intervals, because the outcome is common and odds ratios can overstate effect size. We also report the ordinal sleep distribution descriptively, so the binary under-8-hour outcome can be interpreted against the broader sleep pattern.
Methods
Results
Among 17,441 students with nonmissing sleep data, 13,435 reported fewer than 8 hours of sleep; the weighted prevalence was 76.8% (95% CI 75.0 to 78.6). The ordinal sleep distribution showed that insufficient sleep was not concentrated only near the 8-h threshold: 8.8% reported 4 or fewer hours, 14.4% reported 5 hours, 25.0% reported 6 hours, 28.6% reported 7 hours, 17.6% reported 8 hours, 4.1% reported 9 hours, and 1.5% reported 10 or more hours. The binary outcome is therefore CDC-aligned while still reflecting wide variation in sleep duration. Very short sleep (5 hours or fewer) was reported by 22.4% of students with household basic-needs support present and 35.6% of those with support lacking, indicating that the elevation among students lacking support was concentrated in the very-short-sleep range as well as the conventional under-8-hour threshold.
Selected Characteristics by Household Basic-Needs Support
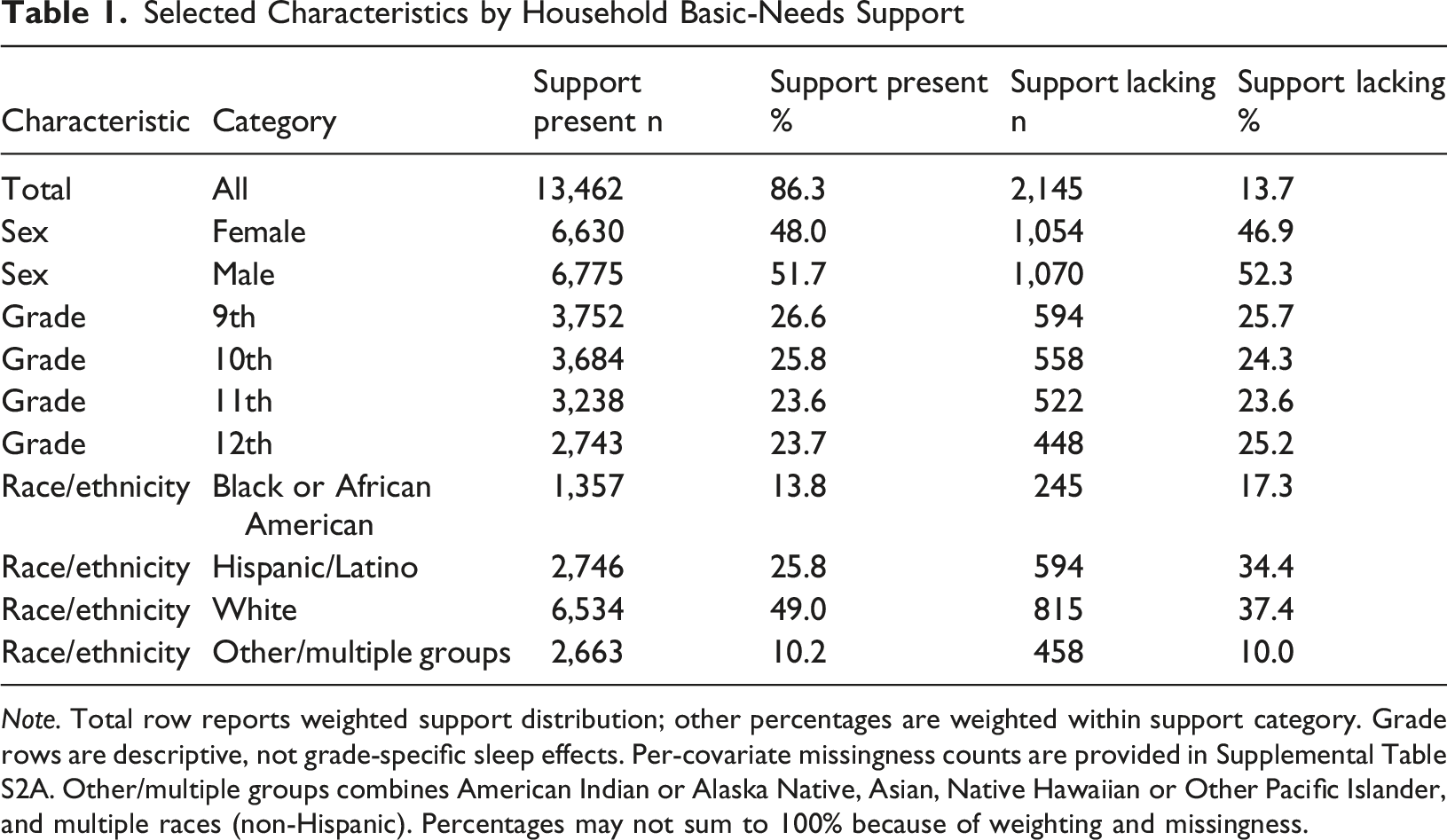
Note. Total row reports weighted support distribution; other percentages are weighted within support category. Grade rows are descriptive, not grade-specific sleep effects. Per-covariate missingness counts are provided in Supplemental Table S2A. Other/multiple groups combines American Indian or Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, and multiple races (non-Hispanic). Percentages may not sum to 100% because of weighting and missingness.
Sleep Prevalence and Adjusted Focal Association
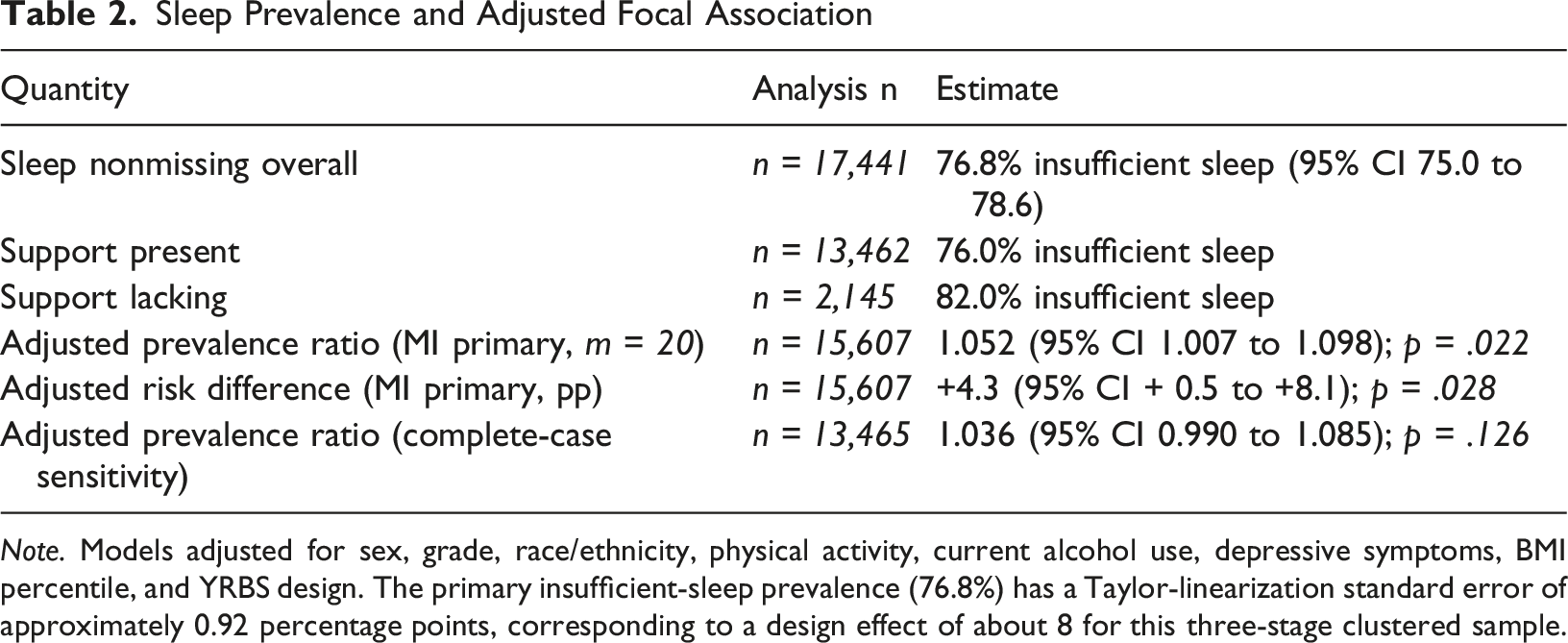
Note. Models adjusted for sex, grade, race/ethnicity, physical activity, current alcohol use, depressive symptoms, BMI percentile, and YRBS design. The primary insufficient-sleep prevalence (76.8%) has a Taylor-linearization standard error of approximately 0.92 percentage points, corresponding to a design effect of about 8 for this three-stage clustered sample.
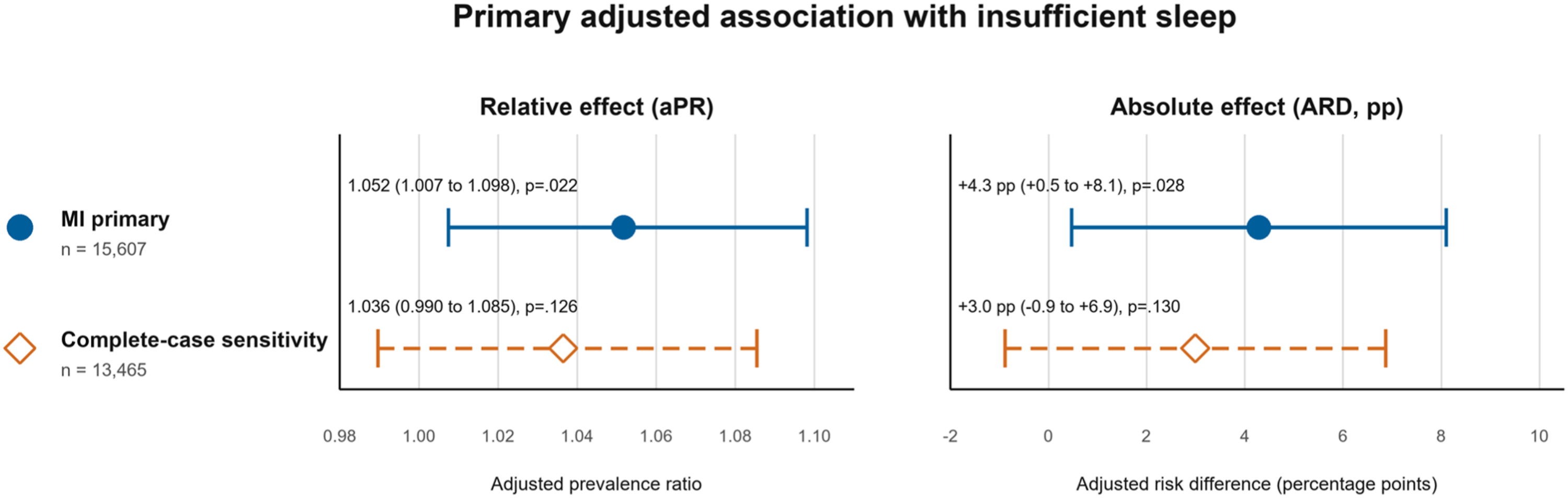
Primary adjusted association of lacking household basic-needs support with insufficient sleep. Note. Points show estimates; bars show 95% confidence intervals. MI = multiple imputation; aPR = adjusted prevalence ratio; ARD = adjusted risk difference; pp = percentage points
In the multiply-imputed primary model (n = 15,607), support lacking was associated with a small, statistically detectable increase in insufficient sleep (aPR = 1.052, 95% CI 1.007 to 1.098; p = .022; ARD = +4.3 percentage points, 95% CI + 0.5 to +8.1; p = .028). A complete-case sensitivity model (n = 13,465) gave a comparable point estimate with a wider, null-spanning interval (aPR = 1.036, 95% CI 0.990 to 1.085; p = .126; ARD = +3.0 percentage points, 95% CI -0.9 to +6.9; p = .130). These estimates are consistent with a modest adverse association of small magnitude.
Discussion
In this national cross-sectional sample, students who perceived less reliable adult effort to meet basic needs were also more likely to sleep fewer than 8 hours on school nights. The association remained after multiply imputed adjustment but was small (aPR = 1.052, 95% CI 1.007 to 1.098); the complete-case sensitivity estimate pointed in the same direction but was less precise. Students who perceived less reliable adult effort to meet basic needs also carried a slightly higher burden of insufficient sleep, but the estimate is not evidence of a large independent effect.
The exposure item requires a narrow reading. It reflects an adolescent’s report that an adult in the household made strong efforts to meet basic needs; it does not directly measure household income, food security, caregiving skill, bedtime routines, or sleep opportunity. That distinction matters because short sleep may arise through several pathways, not through a single socioeconomic, caregiving, or sleep-opportunity mechanism. A caregiver may provide food, clothing, safety, and emotional effort, and still be unable to protect sleep when shift work, transportation, crowded housing, neighborhood safety, or school timing run in the other direction. CDC work similarly treats sleep as socially patterned across family, school, community, and structural levels, rather than solely as an individual behavior (Wheaton & Claussen, 2021). Pairing youth appraisal with caregiver report and more specific social-needs measures would help separate perceived effort from material adequacy, household routine, and environmental constraint.
The ordinal sleep distribution places this finding in a wider public-health frame. AASM, endorsed by the AAP, recommends 8 to 10 hours per 24 hours for adolescents aged 13 to 18 and links adequate sleep with attention, learning, emotional regulation, physical and mental health, and safety (Paruthi et al., 2016). CDC YRBS trend data show that in 2023 only about one in four high school students reported at least 8 hours on an average school night, with declines from 2013 to 2023 (Centers for Disease Control and Prevention, 2024b). The 8-h threshold is therefore clinically recognizable and aligned with surveillance practice; this cut point compresses meaningful variation in adolescent sleep. Very short sleep, weekday-weekend discrepancies, sleep timing, regularity, sleep quality, and daytime sleepiness may each carry distinct clinical and social implications.
The result is useful as a case-finding signal, not a predictive one. Asking adolescents about both school-night sleep and household basic-needs support during routine visits could surface students who may benefit from care navigation, family support, behavioral sleep counseling, or school-based services. This implication is consistent with pediatric social-needs screening literature, which emphasizes linking screening to feasible referrals rather than treating screening as an intervention by itself (Sokol et al., 2019). International evidence from Taiwanese adolescents supports the plausibility of hardship-sleep clustering (Lee et al., 2021), but this study did not test food insecurity, material hardship trajectories, or intervention effects.
The likely direction and magnitude of bias warrant explicit discussion. Reverse causation is plausible: adolescents with insufficient sleep may evaluate household effort less favorably, which would tend to overstate the cross-sectional aPR as an estimate of any prospective effect of household support on sleep. Residual confounding by parental work hours, household structure, screen environment, and neighborhood safety could move the estimate in either direction. Given the modest association, however, the observed aPR of 1.052 could plausibly attenuate toward the null under typical confounding scenarios. CDC weighting partially addresses nonresponse in the setting of the 35.4% overall response rate, but residual nonresponse bias may remain. If students with both low household support and short sleep were less likely to be present on survey administration days, the remaining bias would most likely attenuate the association.
Supplemental Material
Supplemental material - Household Basic Needs Support and Insufficient Sleep Among United States High School Students: Evidence from the 2023 National Youth Risk Behavior Survey
Supplemental material for Household Basic Needs Support and Insufficient Sleep Among United States High School Students: Evidence from the 2023 National Youth Risk Behavior Survey by Sasha R. Sioni, Nishka Jakkidi, Claudia Morales, Rachel D. Clarke, Onelia G. Lage in Clinical Child Psychology and Psychiatry.
Footnotes
Ethical Considerations
This study involved secondary analysis of de-identified 2023 national Youth Risk Behavior Survey microdata and met criteria for exemption under 45 CFR 46.104(d) (4). The project was reviewed and exempted by the Florida International University Institutional Review Board on May 21, 2025 (reference #115946).
Consent to Participate
This study is a secondary analysis of de-identified public-use survey data with no direct contact with participants.
Consent for Publication
No identifiable individual person’s data, images, videos, or case-level descriptions are included.
Author Contributions
Sasha R. Sioni, DBH, MPH, LMHC: Conceptualization; Methodology; Software; Formal analysis; Visualization; Writing - original draft; Writing - review and editing; Supervision.
Rachel D. Clarke, PhD: Conceptualization; Methodology; Writing - review and editing.
Nishka Jakkidi: Data curation; Investigation; Writing - review and editing.
Claudia Morales: Data curation; Validation; Writing - review and editing.
Onelia G. Lage, MD: Supervision; Resources; Writing - review and editing.
All authors approved the final manuscript and agree to be accountable for its content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Public-use, de-identified 2023 national YRBS microdata and documentation are available from the Centers for Disease Control and Prevention Youth Risk Behavior Surveillance System Data and Documentation portal. Project materials will be deposited in the Open Science Framework repository (OSF project identifier x5w8b) upon acceptance for publication.
Preprint
The authors have not posted this manuscript to a preprint server.
Artificial Intelligence Disclosure
AI tools were not used to generate analysis code, statistical results, scientific writing in the manuscript body, or citations. The authors reviewed, revised, and verified the final content, analyses, citations, and interpretations and retain full responsibility for the submitted work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.