
Abstract
Background
Children and adolescents with attention deficit hyperactivity disorder (ADHD) often experience comorbid emotional and behavioral difficulties, yet evidence for meditation-based interventions remains limited. This randomized controlled trial evaluated the effectiveness of an online self-reflective meditation program (True Self Meditation; TSM) on emotional, behavioral, and attentional outcomes in youth with ADHD.
Methods
Forty youth with ADHD were randomly assigned to a 12-week online TSM program or a wait-list control group. Assessments were conducted at pre-intervention, post-intervention, and 12-week follow-up using standardized questionnaires (the Child Behavior Checklist, Youth Self-Report, State-Trait Anxiety Inventory for Children, and etc.) and neurocognitive tests including the Continuous Performance Test (CPT).
Results
Between-group analyses revealed no significant improvements on externalizing or internalizing problems. However, the TSM group showed a significant and sustained reduction in trait anxiety. Within-group pooled analyses indicated additional improvements in self-reported internalizing problems (delayed effect) and commission errors on the CPT, accompanied by increased response times, suggesting more deliberate responding.
Conclusions
TSM exhibited selective effects on internal emotional processes, particularly trait anxiety, rather than on externally observable behavioral symptoms. These findings suggest that TSM may serve as a complementary intervention for anxiety-related difficulties in youth with ADHD, warranting further investigation in larger controlled trials.
Plain Language Summary
Why was this study done? Children and adolescents with attention deficit hyperactivity disorder (ADHD) struggle with more than just paying attention and sitting still. Many also experience anxiety, depression, and behavioral problems. While medication and behavioral therapy can help with the core ADHD symptoms, these difficulties often need additional support. Meditation programs have shown promise for helping children and adolescents manage their emotions, but evidence remains limited. We examined whether a specific approach, True Self Meditation, could help. This meditation approach teaches children and adolescents to identify and release negative thoughts and emotions from past experiences. What did the researchers do? We studied 40 children and adolescents (ages 6 to 18) with ADHD. We randomly divided them into two groups: 20 received weekly online meditation sessions for 12 weeks, while 20 were placed on a waiting list. We measured emotional, behavioral and attentional outcomes before the program, after it ended, and again 12 weeks later to see if improvements lasted. What did the researchers find? The meditation program did not reduce the main behavioral problems that parents reported, such as aggression or rule-breaking. However, children and adolescents who did the meditation showed significant reductions in anxiety. They reported feeling less anxious in daily life. These improvements lasted for at least three months after the program ended. The adolescents also reported feeling less sad and worried over time, though these improvements appeared more slowly. On attention tests, participants became more careful and thoughtful in their responses, suggesting they were learning to think before acting. What do the findings mean? Online meditation may help reduce anxiety in youth with ADHD as a complementary treatment. Parents and clinicians should know that emotional benefits may take time to appear and children may notice improvements before adults do.
Keywords
Introduction
Children and adolescents with attention deficit/hyperactivity disorder (ADHD) face challenges that extend beyond difficulties with attention and impulse control (American Psychiatric Association, 2013). Emotional difficulties, such as depression and anxiety, occur at elevated rates in this population (Melegari et al., 2018; Wang et al., 2025). Behavioral problems, including noncompliance and aggressive behaviors, are also common (Harty et al., 2009; Saylor & Amann, 2016). The impact of ADHD extends to families, as managing hyperactivity, impulsivity, and inattention places significant demands on parents and can strain parent-child interactions, contributing to elevated parental stress (Breaux & Harvey, 2019; Theule et al., 2013).
Although first-line treatments for core ADHD symptoms, including psychostimulant medication and behavioral therapy, are well established (Wolraich et al., 2019), secondary emotional and behavioral difficulties often require additional interventions. Meditation-based interventions have emerged as promising complementary approaches, gaining empirical support in recent years for addressing emotional dysregulation and behavioral challenges in youth (Cairncross & Miller, 2020; Oliva et al., 2021).
Meditation involves mental training aimed at enhancing self-awareness, emotional regulation, and attentional control (Lutz et al., 2008). These interventions encompass a wide range of approaches, from physical practices such as yoga to structured therapeutic methods such as mindfulness-based cognitive therapy (Evans et al., 2018), but all share the core principles of cultivating mindful attention and self-awareness. By promoting the ability to calm physiological arousal and direct focused attention to present-moment experiences, meditation is fundamentally conceptualized as a self-regulatory practice (Househam & Solanto, 2016). Given that deficits in self-regulation are core features of ADHD and contribute to emotional and behavioral difficulties (Murray et al., 2025), meditation-based interventions may be particularly beneficial for youth with ADHD.
Building on these principles, a self-reflective meditation approach known as True Self Meditation (TSM) may offer unique benefits in addressing emotional and behavioral difficulties in youth with ADHD. TSM is a structured, guided practice in which individuals are instructed to recall specific autobiographical memories and visualize them as discrete mental images. Through repeated training, practitioners learn to observe these images with detachment and intentionally let them go, a process referred to as ‘releasing’ (Yoo et al., 2023). Rather than analyzing or reframing the content of these memories, TSM treats them as discardable mental representations, with the goal of diminishing the emotional and cognitive influence they exert on present functioning. Through this process, TSM aims to enhance self-awareness by identifying cognitive distortions rooted in past experiences and releasing associated emotional charges, thereby fostering emotional clarity and deeper personal insight (Yun et al., 2019).
While TSM shares fundamental principles with approaches such as mindfulness-based cognitive therapy and cognitive restructuring, it distinguishes itself through unique therapeutic mechanisms (Kim et al., 2019; Yoo et al., 2023). Unlike cognitive restructuring within CBT, which relies on logical reappraisal to modify the content of maladaptive thoughts, TSM does not seek to change or reinterpret these thoughts but instead aims to disengage from them entirely by treating them as visualized images to be released. Likewise, while mindfulness-based approaches emphasize nonjudgmental observation and acceptance of present-moment experiences, TSM actively engages with past memories with the explicit goal of diminishing their emotional charge rather than coexisting with them. These internalized representations are thought to underlie cognitive rigidity, emotional reactivity, and reduced self-esteem, all of which contribute to psychological difficulties (Kim et al., 2019).
TSM has been applied across diverse settings, including schools, clinics, and community-based programs, and its effects have been preliminarily explored in several empirical studies. Among children and adolescents, prior studies suggest that TSM is associated with improvements in self-reflection and academic attention in middle school students (Yun et al., 2020), as well as reductions in social anxiety, aggression, and stress among elementary school students (Yoo et al., 2016). Studies of adult populations report similar positive effects, including reductions in anxiety and depression as well as improvements in somatic symptoms such as fatigue and sleep disturbances among college students and cancer survivors (Yoo et al., 2023; Yun et al., 2017).
Despite these promising findings, several important research gaps remain. First, no study has specifically examined TSM’s effectiveness in children and adolescents with ADHD, as most studies have focused on general pediatric or adult populations. This gap is notable given that systematic reviews of meditation-based interventions have reported limited effects on externalizing and internalizing symptoms in youth with ADHD (Evans et al., 2018; Lee et al., 2022), highlighting the need for targeted investigation of specific meditation approaches in this population. Second, the existing TSM literature is limited by a lack of randomized controlled trials, with most studies employing non-randomized designs that limit causal inference. Third, little is known about the long-term maintenance of treatment effects following meditation-based interventions in pediatric populations.
Therefore, the present randomized controlled trial aimed to evaluate the effects of a 12-week online TSM-based program on emotional, behavioral, and attentional outcomes in children and adolescents with ADHD. Building on prior evidence of TSM’s positive effects in general pediatric populations, this study explored whether these benefits extend to youth with ADHD. Additionally, this study examined TSM’s impact on attention-related variables, as attentional deficits are among the most persistent ADHD symptoms. Finally, this study assessed whether the effects were maintained over a 12-week follow-up period, addressing the largely unexplored question of sustainability, which is essential for determining clinical utility. Through this comprehensive design, this study sought to provide preliminary evidence for TSM as a complementary intervention for youth with ADHD.
Methods
Participants
Participants were recruited through the outpatient clinic of a tertiary university hospital between April and September, 2023. Inclusion criteria were (1) a primary diagnosis of ADHD and (2) an age between 6 and 18 years. The diagnosis was confirmed through a semi-structured diagnostic interview with parents using the Korean version of the Schedule for Affective Disorders and Schizophrenia for School-aged Children-Present and Lifetime version (Kaufman et al., 2016). Exclusion criteria were (1) a history of brain injury; (2) seizure disorders or other neurological illnesses; (3) uncorrected sensory impairments (e.g., vision or hearing); (4) planned changes in psychiatric medication during the subsequent 12 weeks; and (5) insufficient device access for online participation. After excluding one participant who withdrew consent, 40 children and adolescents with ADHD were enrolled in this study (mean age = 10.85 years, SD = 2.81; 37 boys, 3 girls).
Study Design and Procedures
Participants were randomly assigned to either the experimental group or the wait-list control (WLC) group using stratified block randomization based on age (6–12 and 13–18 years). Randomization was conducted using a web-based randomization system. Recruitment and randomization procedures are illustrated in Figure 1. CONSORT flow diagram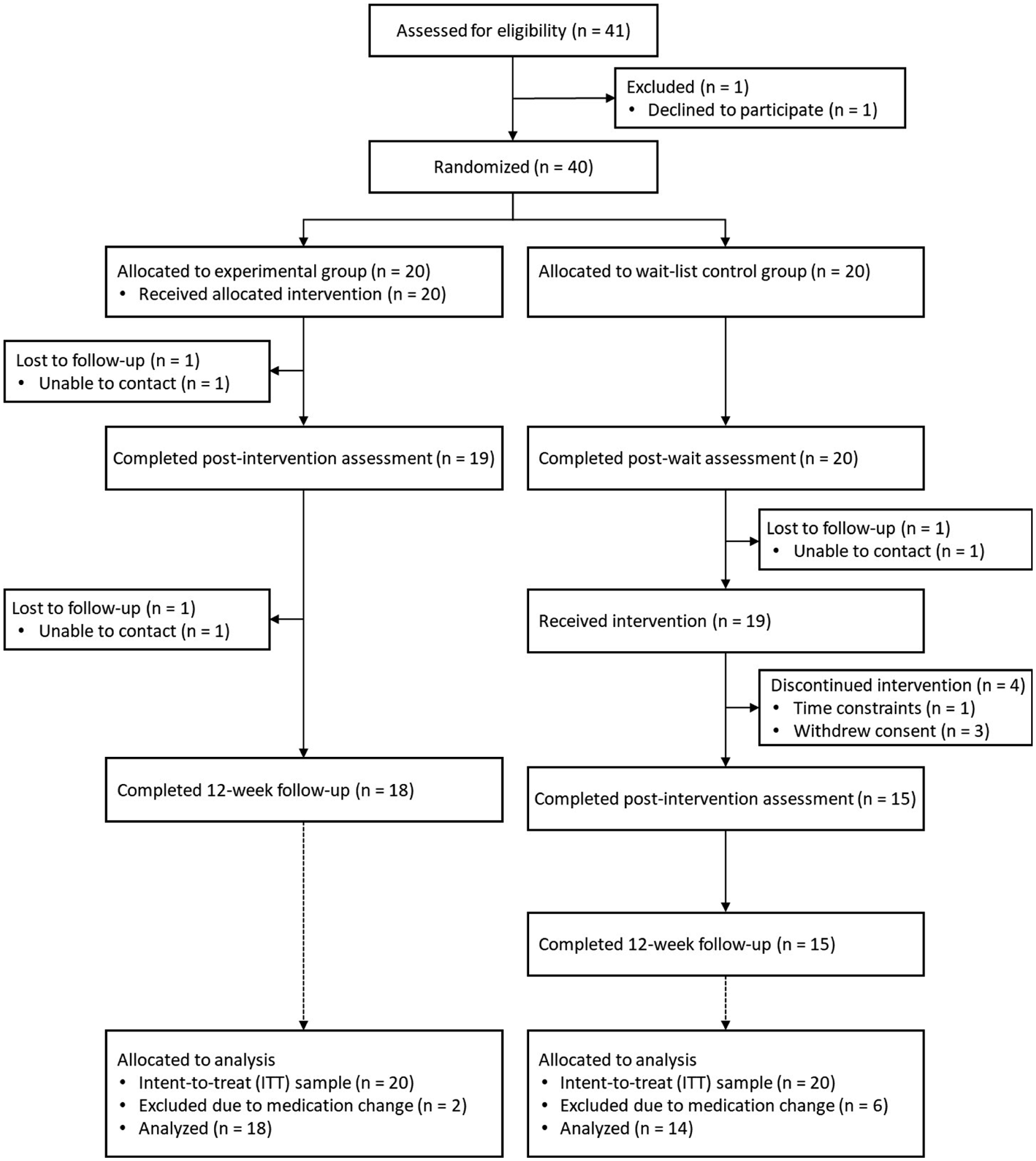
Following enrollment, all participants completed a pre-intervention assessment at the participating institution. To minimize bias, two investigators blinded to group assignment administered all assessments. Within one week of this pre-intervention assessment, the experimental group began a 12-week online meditation program. The program consisted of weekly 50-min one-to-one sessions delivered through Zoom, scheduled individually for each participant. Sessions were led by 10 certified instructors, with each instructor assigned to four participants. To ensure intervention fidelity, instructors followed standardized manuals and worksheets, completed detailed session logs, and attended weekly supervision meetings.
To evaluate the effects of the program, the experimental group completed assessments at three time points: pre-intervention, post-intervention, and a 12-week follow-up. The WLC group maintained usual treatment and completed assessments before and after a 12-week waiting period. Afterward, they received the same meditation program as the experimental group and subsequently completed post-intervention and follow-up assessments. Throughout the study period, both groups were allowed to continue any treatment they had been receiving prior to enrollment.
Intervention
The online meditation program was adapted from the school-based TSM curriculum developed by the Academic Society for Human Completion in Korea. This curriculum integrates TSM techniques with developmentally appropriate methods and has received formal accreditation from the Korean Ministry of Education. For this study, the program was modified to meet the needs of children and adolescents with ADHD and to support online delivery. The program comprised 12 sessions, including eight core sessions delivered to all participants and four additional sessions tailored for younger (under 13 years) and older adolescents (13 years and above). Each session followed a structured format: (1) brief psychoeducation on meditation principles and techniques; (2) reflective exercises designed to help participants identify maladaptive thoughts and emotions; and (3) guided practice in recognizing and releasing maladaptive cognitive-emotional response patterns. Detailed session content is provided in the Supplementary Material.
Measures
A range of standardized measures assessed emotional, behavioral, and attentional functioning. Primary outcomes evaluated emotional and behavioral problems, while secondary outcomes assessed ADHD symptoms and neurocognitive functioning.
Primary Outcomes
Secondary Outcomes
Statistical Analyses
All analyses were conducted using IBM SPSS Statistics version 29.0. Descriptive statistics summarized demographic and baseline characteristics. Normality was evaluated using the Shapiro-Wilk test, and baseline group differences were examined using independent samples t-tests or Mann-Whitney U tests for continuous variables and chi-square or Fisher’s exact tests for categorical variables. Differences between study completers and non-completers were also examined.
Analyses followed a modified intent-to-treat (ITT) approach with participants analyzed according to original group assignments. However, eight participants with unplanned ADHD medication changes (2 in the experimental group and 6 in the WLC group) were excluded because these changes could confound intervention effects. The final analysis sample included 32 participants (18 experimental, 14 WLC). Participants with incomplete data but without medication changes were retained, and missing values were handled using generalized estimating equations (GEE).
Between-group differences in pre- to post-intervention changes were tested using GEE models, controlling for age, gender, and full-scale IQ. Each model included group (experimental vs. WLC), time (pre- vs. post-intervention), and group × time interaction terms, with post hoc pairwise comparisons (Bonferroni-adjusted) for significant interactions.
To examine intervention effects across the full intervention period and to assess sustainability, additional within-group GEE analyses were conducted using pooled data from both groups across three time points: pre-intervention, post-intervention, and follow-up for the experimental group; and post-waiting, post-intervention, and follow-up for the WLC group. This approach increased statistical power and allowed a comprehensive evaluation of both immediate and maintained effects, addressing limitations associated with small sample sizes.
Results
Preliminary Analyses
Demographic Characteristics of the Participants
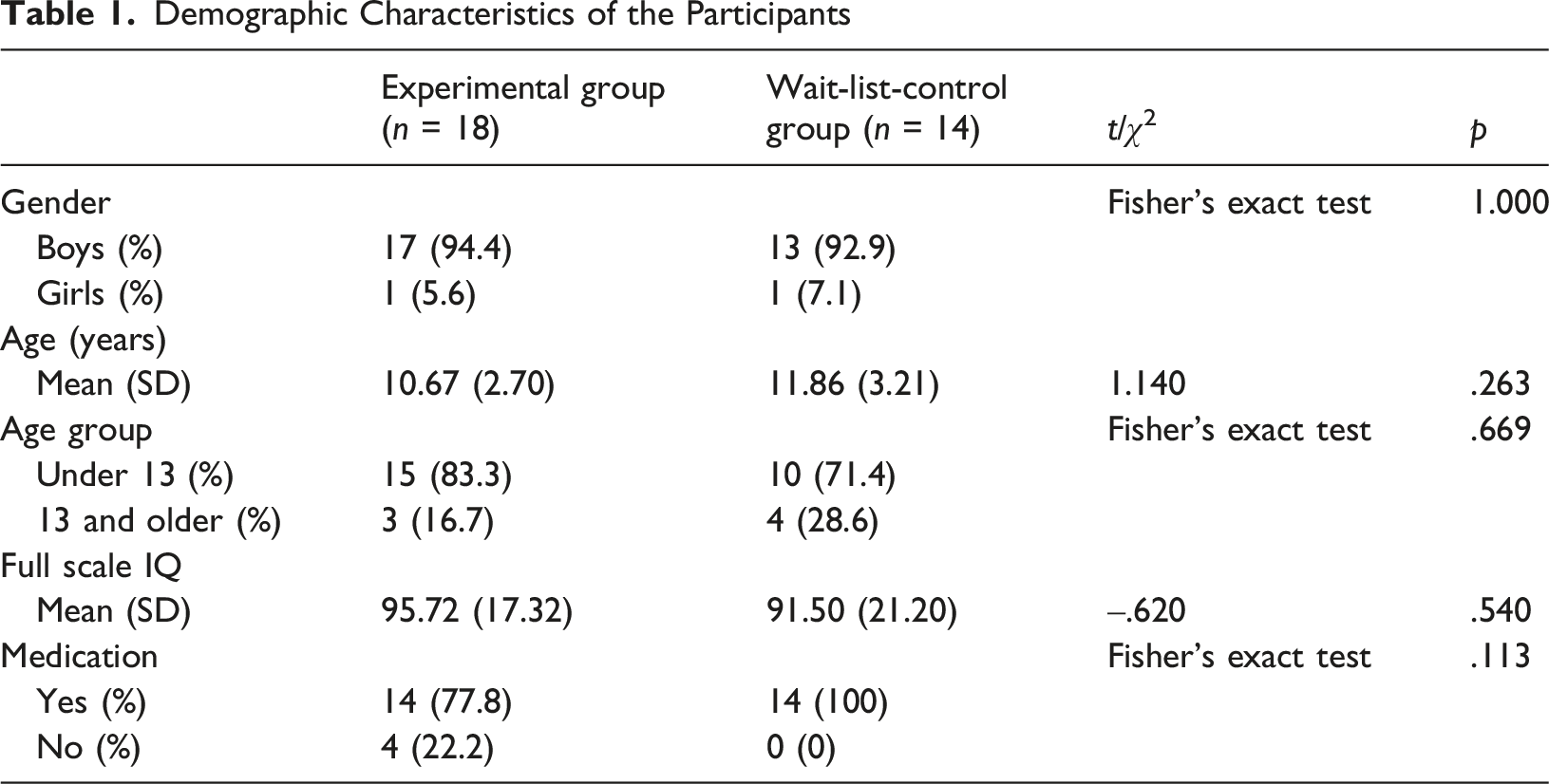
The overall dropout rate did not differ significantly between the two groups (χ2 = 2.789, p = .095), although it was numerically higher in the WLC group (35.7%, 5 out of 14 participants) than in the experimental group (12.5%, 2 out of 18). Participants who discontinued the study did not differ from those who completed it on any demographic characteristics or baseline outcome variables (p = .320–.923).
Pre-Post Comparison Between Groups
Pre- and Post-intervention Scores for Outcome Variables by Group
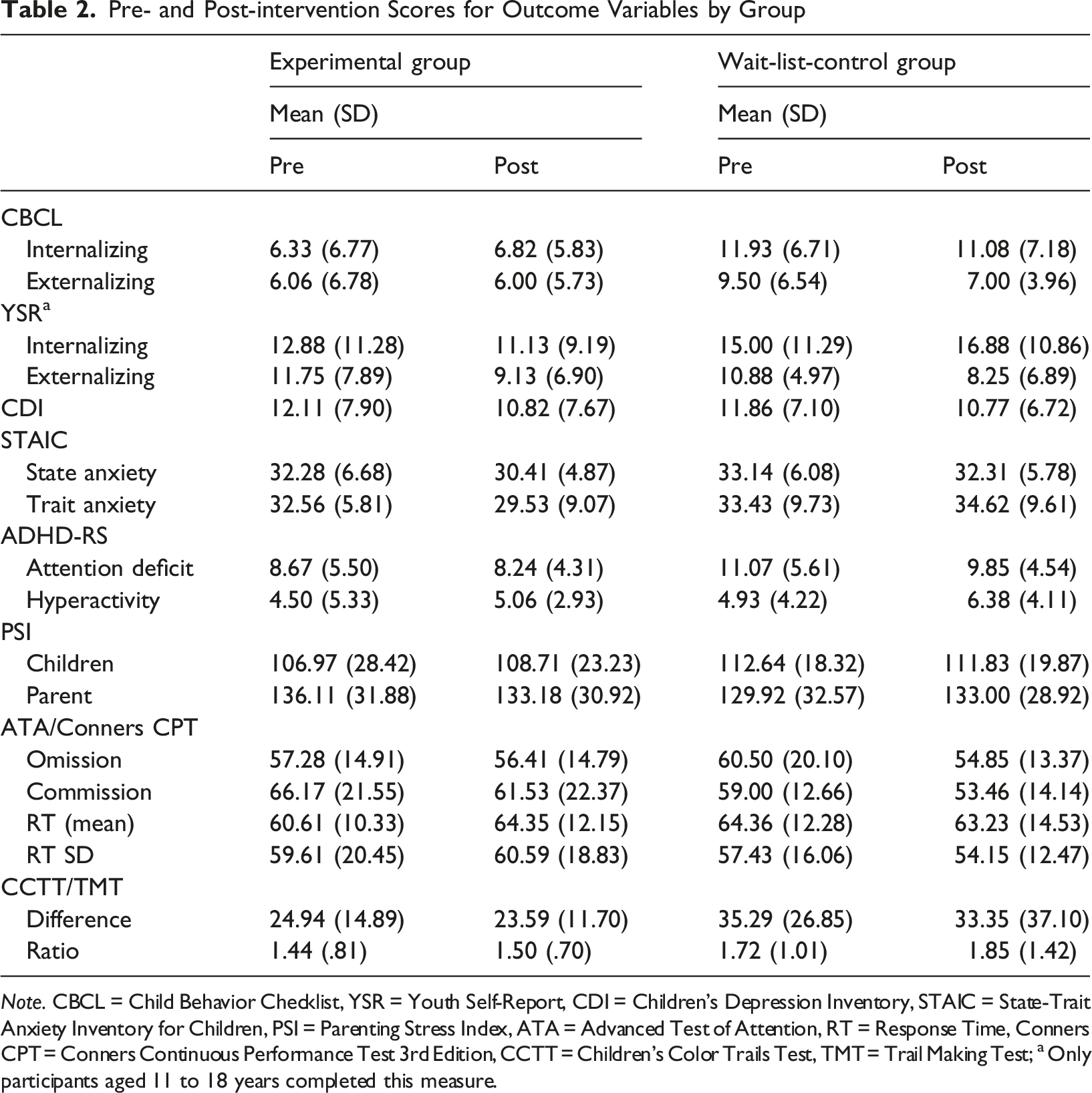
Note. CBCL = Child Behavior Checklist, YSR = Youth Self-Report, CDI = Children’s Depression Inventory, STAIC = State-Trait Anxiety Inventory for Children, PSI = Parenting Stress Index, ATA = Advanced Test of Attention, RT = Response Time, Conners CPT = Conners Continuous Performance Test 3rd Edition, CCTT = Children’s Color Trails Test, TMT = Trail Making Test; a Only participants aged 11 to 18 years completed this measure.
Findings of Generalized Estimating Equations for Outcome Variables
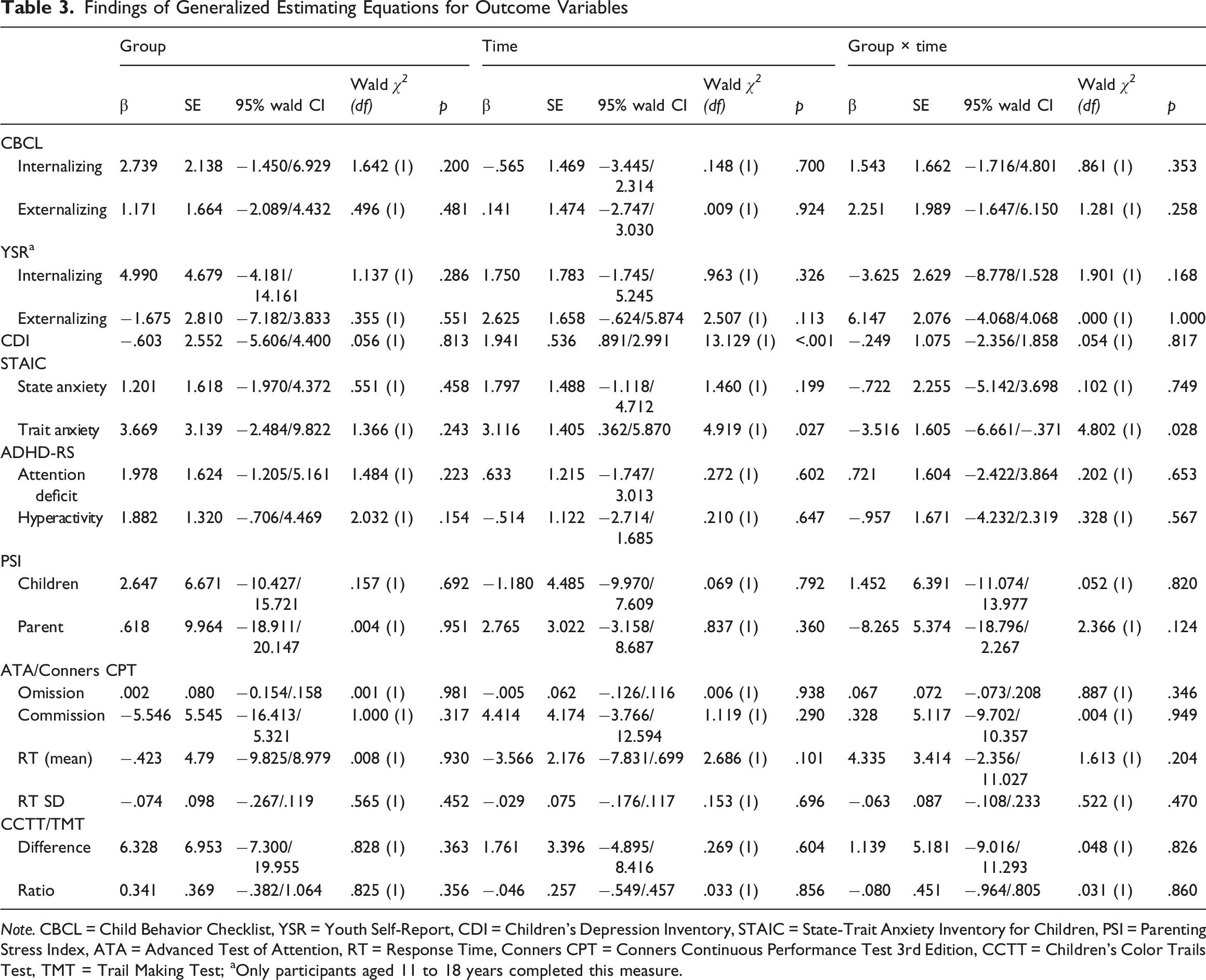
Note. CBCL = Child Behavior Checklist, YSR = Youth Self-Report, CDI = Children’s Depression Inventory, STAIC = State-Trait Anxiety Inventory for Children, PSI = Parenting Stress Index, ATA = Advanced Test of Attention, RT = Response Time, Conners CPT = Conners Continuous Performance Test 3rd Edition, CCTT = Children’s Color Trails Test, TMT = Trail Making Test; aOnly participants aged 11 to 18 years completed this measure.
Within-Group Analysis of Intervention Effect and Maintenance Using Pooled Data
Generalized Estimating Equations Results for Within-Group Changes Across Times (Pooled Data)
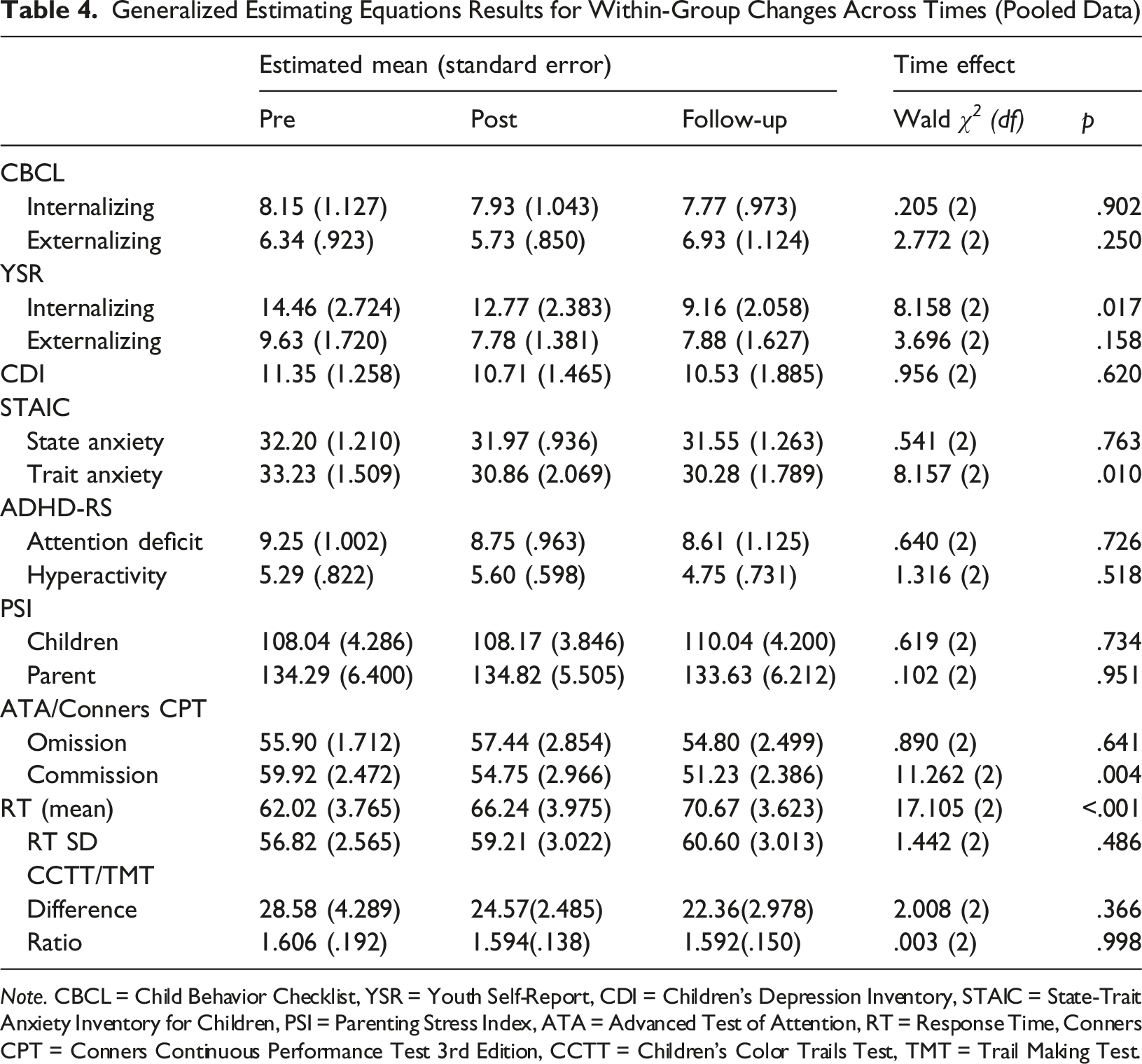
Note. CBCL = Child Behavior Checklist, YSR = Youth Self-Report, CDI = Children’s Depression Inventory, STAIC = State-Trait Anxiety Inventory for Children, PSI = Parenting Stress Index, ATA = Advanced Test of Attention, RT = Response Time, Conners CPT = Conners Continuous Performance Test 3rd Edition, CCTT = Children’s Color Trails Test, TMT = Trail Making Test.
Discussion
This study examined the effectiveness of a 12-week online TSM-based program in improving emotional, behavioral, and attentional outcomes in children and adolescents with ADHD, as well as the maintenance of effects over time. No significant between-group differences were observed in the primary outcomes (CBCL and YSR internalizing and externalizing problems). These findings align with prior reviews reporting limited effects of meditation-based interventions on internalizing and externalizing symptoms in youth with ADHD (Evans et al., 2018; Lee et al., 2022).
However, the TSM program significantly reduced trait anxiety. The experimental group exhibited greater reductions than the WLC group, with effects maintained at the 12-week follow-up. Delayed improvements were also observed in adolescents’ self-reported internalizing symptoms. These findings are consistent with previous studies reporting reduced emotional difficulties among youth following TSM interventions (Park et al., 2024; Shin et al., 2019; Yoo et al., 2019).
These findings suggest that TSM may exert selective effects on internal emotional processes, such as emotional vulnerability, rather than on externally observable behavioral problems. The reduction in trait anxiety may reflect the program’s emphasis on identifying and releasing distorted thoughts and emotions. It is plausible that the program’s cognitive-emotional restructuring preferentially addressed internalized negative self-perceptions and rigid thinking patterns that contribute to chronic anxiety. TSM principles posit that internalized psychological structures underlie emotional over-reactivity and instability, closely related to trait anxiety. This interpretation is consistent with STAIC trait anxiety items, which assess stable emotional tendencies through self-related statements (e.g., “I worry about making mistakes”), whereas state anxiety items reflect momentary emotional states. Therefore, the TSM’s subtraction approach, which targets underlying psychological processes, may have been better captured by trait rather than state anxiety measures.
The delayed improvements in adolescents’ self-reported internalizing problems, reaching significance only at follow-up, warrant further consideration. This pattern aligns with prior findings of delayed internalizing-symptom improvements after mindfulness interventions in adolescents with ADHD (Haydicky et al., 2015). The difference in timing between immediate trait-anxiety improvements and delayed broader internalizing changes may reflect differences in measurement sensitivity, construct complexity, or other methodological factors. As the present study was not designed to examine these temporal relationships directly, further research is needed to clarify these mechanisms.
Significant improvements were observed in adolescent self-report measures (STAIC and YSR), whereas parent-report measures (CBCL) exhibited no significant effects. This discrepancy may suggest that TSM’s effects on internal emotional processes are more readily perceived by adolescents themselves than by external observers. However, differences in perspectives, measurement characteristics, or potential reporter bias may also contribute. Future research employing multiple informants, more frequent assessment points, and process-oriented measures may clarify how emotional domains respond to TSM over time.
Regarding neurocognitive outcomes, within-group analyses exhibited reduced CPT commission errors and increased response times. These changes may indicate the adoption of more cautious and deliberate response strategies, potentially reflecting reduced impulsivity associated with repetitive meditation practices. This interpretation aligns with prior studies reporting improvements in self-control and attention among youth following TSM interventions (Choi et al., 2020; Yoo et al., 2024; Yun et al., 2020). However, because these effects were not significant in the between-group RCT analysis, they may also reflect practice effects, developmental changes, or other non-specific influences. Future studies with larger sample sizes are needed to clarify whether TSM produces reliable improvements in attention-related cognitive functioning in youth with ADHD.
This study provides several contributions. To our knowledge, it is the first randomized controlled trial to examine the efficacy of TSM in youth with ADHD. Sustained reduction in trait anxiety suggests that TSM may serve as a complementary intervention for anxiety-related difficulties commonly comorbid with ADHD. The maintenance of the effects over 12 weeks indicates that benefits may persist beyond the intervention period, providing clinicians with guidance on treatment duration and outcome monitoring. Additionally, the discrepancies between adolescent and parent reports highlight the importance of multi-informant assessment and suggest that meditation may have stronger effects on internal emotional regulation than on externally observable behaviors.
Several limitations should be considered. First, the relatively small final sample (n = 32) likely reduced statistical power to detect intervention effects, particularly for the primary outcomes. Although the original sample size (n = 40) was comparable to similar studies, ranging from 5 to 55 participants (Sultan et al., 2025), the exclusion of participants with medication changes further reduced the analytical sample size. Although significant effects on trait anxiety were observed despite this limitation, replication with larger samples is necessary to confirm these findings and assess effects on primary outcomes. Additionally, all participants were recruited from the outpatient clinic of a single tertiary university hospital, which may limit the generalizability of the findings to youth with different symptom severity or different levels of treatment-seeking motivation. The sample also had a pronounced male predominance (37 boys, 3 girls). While ADHD is more commonly diagnosed in males than in females in Korea (approximately 3.3:1; Seo et al., 2022), male-to-female ratios can be higher in clinical samples, ranging from 3:1 to 16:1 (Nøvik et al., 2006; Skogli et al., 2013). Although the 12:1 ratio observed in our sample falls within this range, such variability can be amplified in small samples. Given that only one girl per group was included in the final analysis, the present findings may not generalize to female youth with ADHD. Future studies should recruit from diverse clinical and community settings with more balanced gender representation to determine whether TSM benefits extend to youth with varying levels of ADHD severity, treatment motivation, and demographic characteristics.
Second, although stratified block randomization based on age (6–12 and 13–18 years) ensured balanced age distribution between groups, the wide age range of participants (6–18 years) introduces developmental heterogeneity. Younger children and adolescents may differ in symptom presentation, treatment response, and engagement with self-reflective practices. The small number of adolescents aged 13 and above in the final sample (n = 7) limited the feasibility of meaningful subgroup analyses comparing younger and older participants. Future studies with larger and more age-balanced samples are needed to examine whether TSM effects vary across developmental stages.
Third, some non-specific factors may have remained uncontrolled. Although the investigators were blinded to group assignment, participants and their parents were aware of the group assignments, potentially introducing expectancy effects. The modest improvements in the WLC group on some measures may reflect assessment reactivity or attention associated with study participation. Future studies should benefit from active control conditions to better isolate specific intervention mechanisms.
Fourth, although the meditation program followed a structured curriculum, intervention fidelity and participant engagement quality were not formally assessed. Low engagement can compromise effectiveness by limiting the acquisition of skills essential for therapeutic change (Montero-Marin et al., 2022). Future studies should incorporate systematic measures of engagement quality, intervention fidelity, and extra-home practice frequency to enhance accuracy in evaluating intervention effects and identifying optimizing factors. Additionally, while the online format improved accessibility, it limited control of environmental variables, and engagement varied widely because of technical challenges and inattentive behaviors. These variations could not be reliably quantified and may have diluted effects.
Several future research directions emerge. Larger and more diverse samples, along with active control groups, are needed to rigorously assess meditation effects. Earlier research suggests that neurocognitive outcomes often show smaller effects than behavioral outcomes in ADHD interventions (Evans et al., 2018), underscoring the need for adequate statistical power in studies employing task-based cognitive measures. Various active control conditions would enhance the specificity of findings related to meditation. Examples include attention-matched tasks (Robe & Dobrean, 2023) and emotional education without meditation (Zaccari et al., 2022). These approaches have been useful for isolating meditation-specific effects and may be valuable for future TSM research.
Further research is also needed to identify mechanisms by which meditation improves outcomes. Potential pathways such as executive control, emotion regulation, or cognitive flexibility should be examined as mediating factors, particularly given the current study’s findings related to emotional vulnerability. Considering TSM’s unique approach, future studies may investigate whether changes in self-referential processing underlie improvements in emotion regulation.
Finally, examining how TSM effects vary according to developmental and individual characteristics, including age, gender, and predominant ADHD symptom profiles, may help tailor interventions to specific subgroups. Comparisons of different meditation formats (e.g., MBCT, TSM, physical activity-based meditation) may also identify optimal components for specific populations. Prior research suggests that older children may benefit more from abstract, reflective methods, whereas younger children may respond better to concrete techniques incorporating visualization or physical movement (Lee et al., 2022), although empirical support remains limited. Tailoring meditation programs to developmental needs and individual characteristics may enhance therapeutic impact. Further research is required to test these hypotheses.
Supplemental Material
Supplemental Material - Emotional and Behavioral Effects of an Online Self-Reflective Meditation Program in Youth With ADHD: A Randomized Clinical Trial
Supplemental Material for Emotional and Behavioral Effects of an Online Self-Reflective Meditation Program in Youth With ADHD: A Randomized Clinical Trial by Seung Ah Lee, MiRa Yun, Hani Lee, In-Soo Lee, In Sook Jang, Soon-Beom Hong in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgments
We thank Seog-Gi Lee for administrative support and program management, Yoon Jung Shim for contributions to implementing and refining the intervention, and ChoonWon Kim, Eun Zu Oh, Heejeong Lim, Hyun Kyung Shim, Jeong Mi Kim, Jungen Cho, Mikyung Han, Se Eun Kang, and Yeon Ok Kim for their dedicated involvement in program facilitation.
Ethical Considerations
This study was approved by the Seoul National University Hospital Institutional Review Board (approval no. H-2211-085-1378) on January 10, 2023.
Consent to Participate
Written informed consent was obtained from the parents or legal guardians of all participants, and written assent was obtained from the children and adolescents prior to participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funds donated by Truebook Sinsago Co., Ltd. to the Mind the SHIM (SNUH Health In Mind) Center at Seoul National University Hospital, Republic of Korea.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed in this study are not publicly available owing to ethical considerations and privacy restrictions. The data may be made available upon reasonable request and approval from the Institutional Review Board of Seoul National University Hospital, South Korea. Inquiries regarding data access should be directed to the corresponding author and will be evaluated individually.
Trial Registration
This trial was registered with the Clinical Research Information Service of Korea (https://cris.nih.go.kr; registration number: KCT0008345).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.