
Abstract
Background
Caregivers of children with tic disorders experience substantial psychological and social burdens; however, existing research is predominantly cross-sectional, and their lived emotional experiences remain insufficiently explored through qualitative approaches.
Objective
This study aimed to explore the emotional experiences of primary caregivers of children with tic disorders throughout the caregiving process.
Methods
A descriptive phenomenological design was employed. Semi-structured in-depth interviews were conducted with 13 primary caregivers recruited through purposive sampling. Data collection continued until thematic saturation was reached. Interview transcripts were analyzed using Colaizzi’s seven-step method.
Results
Three main themes emerged: multiple caregiving burdens, emotional and psychological distress, and caregiving challenges and coping strategies. Caregivers reported persistent negative emotions, including anxiety, guilt, and emotional exhaustion, which were intensified by financial strain, family conflict, and limited access to professional medical services.
Conclusion
Caregivers of children with tic disorders experience considerable caregiving burdens and psychological distress, which may hinder both caregiver well-being and the child’s rehabilitation. Strengthening psychological support systems and improving access to professional healthcare resources are essential to address caregivers’ multifaceted needs.
Plain Language Summary
Why was the study done? Researchers conducted this study to map the emotional “lived experiences” of parents in China caring for children with tic disorders. While previous studies often focus on high-level numbers or medical outcomes, they frequently overlook the deeper, daily stories of these families. The goal was to uncover hidden emotional needs so that healthcare professionals can develop personalized support strategies. What did the researchers do? The researchers used a “descriptive phenomenological” design to focus on the emotions parents consciously perceive and express. They conducted in-depth, one-on-one interviews with 13 primary caregivers at a clinic in Shandong, China. To ensure authenticity, they analyzed these conversations using the systematic Colaizzi’s seven-step method to identify key themes. What did the researchers find? The study found that caregiver stress falls into three categories: multiple life burdens, emotional distress, and coping challenges. Parents face “social” embarrassment when symptoms are misunderstood and “personal” guilt, often blaming their own parenting for the disorder. Many caregivers also suppress their own anxiety to keep their child calm, which frequently leads to total emotional exhaustion. What do the findings mean? These findings suggest that medical care must move beyond just treating the child to supporting the whole family. There is an urgent need for professional psychological support for parents and better public education to reduce the social stigma that makes caregiving so much harder.
Introduction
Tic disorder (TD) is a neurodevelopmental disorder characterized by sudden, rapid, repetitive and non-rhythmic movements or vocalizations during childhood and adolescence (Yu et al., 2024). It includes chronic tic disorder (CTD) and Tourette syndrome (TS), with a prevalence of 0.5–1% (Conte et al., 2020). TD is also very common in China, accounting for approximately 6.1% of the child population (Tinker et al., 2022). In addition to frequent tics, affected children may also have other conditions such as attention deficit hyperactivity disorder (ADHD), obsessive-compulsive disorder (OCD), anxiety disorder, and depression (Girgis et al., 2022). The chronic course of TD seriously affects the quality of life of children with the disease, causing long-term adverse effects on their emotions, social interactions and physical health, and posing considerable challenges to the children and their families (Rizwan et al., 2022).
The etiology of TD is complex and is often the result of the interaction of genetic, environmental and psychological factors during children’s development (Liu et al., 2020; Qi et al., 2019; Yagi et al., 2021). Among them, caregivers play a crucial role in the management of TD (Lee, 2022). However, long-term care responsibilities, insufficient social support, and concerns about the future development of children patients often subject caregivers to tremendous physical and mental stress (Travis & Juarez-Paz, 2020). Compared with caregivers of children with other chronic diseases, due to the particularity of TD symptoms, they often face more severe social pressure and psychological burden (Liu et al., 2023). Studies show that these pressures are closely related to the negative emotions of caregivers (Goussé et al., 2016), and may even affect the recovery and psychosocial functions of children patients (Banihani et al., 2025). Therefore, it is crucial to understand the emotional experiences and needs of caregivers of children with TD during the care process.
In recent years, the mental health of caregivers of children with chronic diseases has gradually attracted the attention of scholars (Holmes et al., 2024; Zonta et al., 2024). However, most of the studies on the emotions of caregivers of children with TD are cross-sectional studies, and qualitative research on their emotional experiences remains limited (Stewart et al., 2015; Wattanarojjanakit et al., 2023). Compared with quantitative research, qualitative research methods are more suitable for in-depth exploration of the challenges, difficulties and emotional experiences faced by caregivers (Jika et al., 2021). A deep understanding of these feelings can help medical staff implement targeted interventions, improve the mental health of caregivers, reduce related care obstacles, enhance care capabilities, and ultimately promote the recovery and growth of children patients.
Therefore, this study adopts qualitative research methods, aiming to deeply explore the emotional experiences of TD child caregivers and provide empirical evidence for formulating targeted intervention strategies.
Methods
Study Design
This study adopts a descriptive phenomenological design to explore the emotional experiences of the primary caregivers of TD children. This method is based on Husserl’s phenomenology of psychology and focuses on understanding the emotional experiences that participants consciously perceive and express. The research conducted in-depth interviews following standard descriptive phenomenological procedures to elicit the emotions and experiences of caregivers.
Study Population
Participants were recruited at the psychosomatic medicine clinic of a hospital in Shandong Province from July to September 2025. To ensure the heterogeneity of participants in terms of demographic characteristics such as age, gender, education level, occupation and income, this study adopted a purposive sampling strategy with maximum variability. The sample size is determined based on data saturation, that is, no new topics appear during the interview process.
Inclusion criteria were: (1) parents of children meeting the DSM-5 diagnostic criteria for TD (American Psychiatric Association, 2013); (2) parents of children aged 3–12 years; (3) serving as the primary caregiver for at least three months; (4) caregivers under 65 years of age, alert, and able to communicate clearly.
Exclusion criteria were as follows: (1) caregivers currently receiving other psychological interventions; (2) caregivers with severe medical, surgical, or neuropsychiatric conditions; (3) caregivers with difficulties in reading or comprehension; (4) paid caregivers; (5) caregivers who withdrew during the study; and (6) children with life-threatening organic diseases.
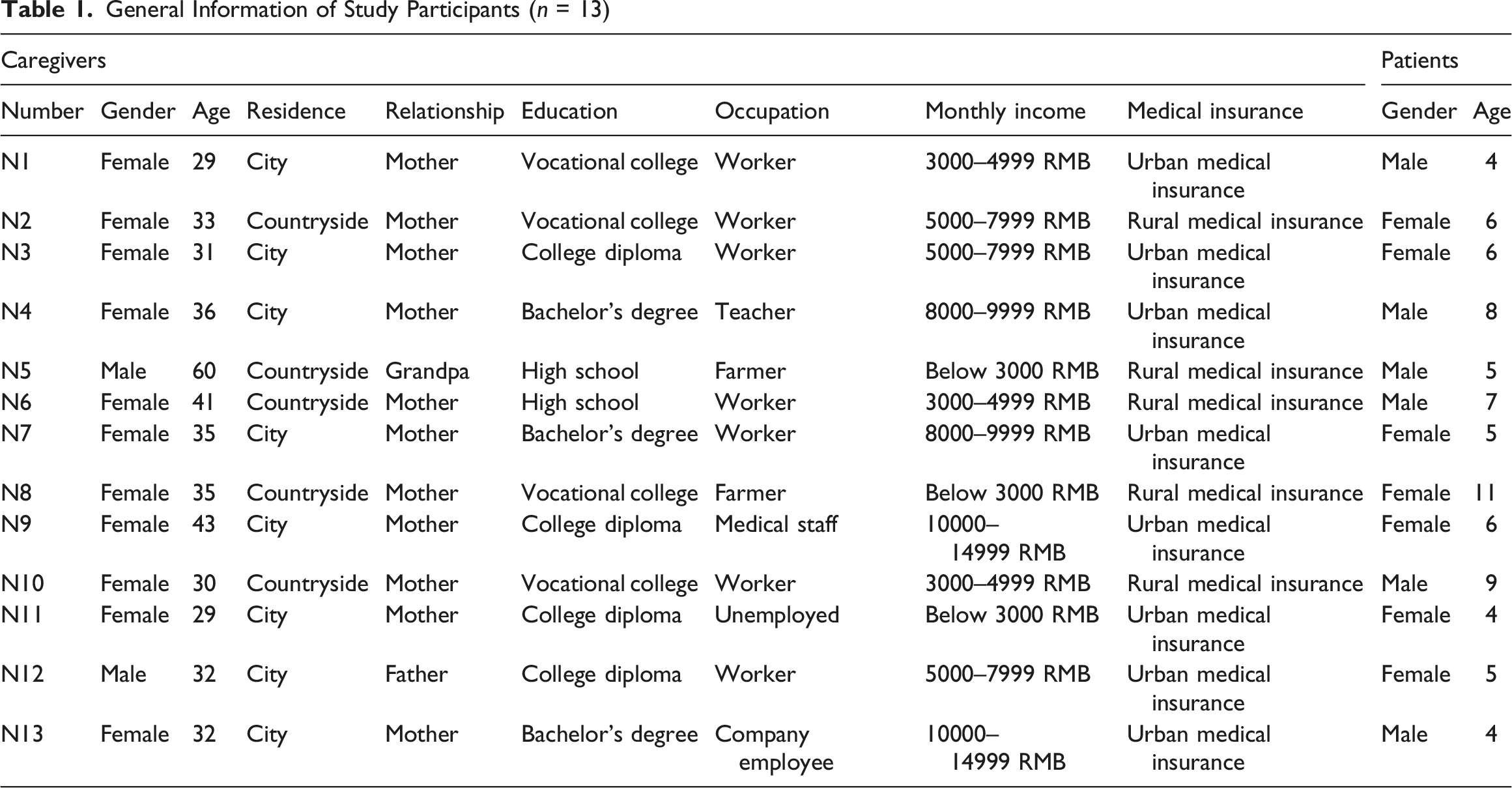
General Information of Study Participants (n = 13)
Determination of Research Outline
The interview outline was formulated based on the literature review (Kallio et al., 2016; Yu et al., 2022) and the preliminary discussion consistent with the research objectives. Pilot interviews were conducted with two caregivers to assess the clarity and relevance of the questions. The team discussed the feedback from the pilot interviews to refine the interview outline. The data from the pilot interviews were not included in the final analysis.
The final version of the interview outline mainly includes the following questions: 1. What changes have occurred in the children’s emotions since their diagnosis, and provide examples to illustrate? 2. What are the main causes of these emotions? 3. How do they usually deal with these emotions? 4. How do these emotions affect their interactions with their children, their daily lives, and their work? 5. What types of support or assistance do you most hope to receive during the care process? 6. Talk about your expectations or concerns for your child’s recovery and future life.
Data Collection
Researchers recruited participants at the outpatient department. During the period when the caregivers were waiting for medical treatment, the researchers explained the purpose and process of the study to the caregivers and emphasized that all information would be strictly confidential. All participants signed a written informed consent form before participating and were informed that all research results would only be used for research purposes and would not affect the clinical treatment of their children.
Conduct one-on-one interviews in quiet and private places, such as meeting rooms, consultation rooms or doctors’ offices. The interviews follow a semi-structured interview guideline and each session lasts approximately 30 minutes. All interviews were recorded. The interviewer listened attentively, encouraged the caregiver to express themselves freely during the process, and adjusted the wording or the order of the questions when necessary. Keep collecting data until the topic is saturated, that is, no new topics emerge.
Data Analysis and Rigor
Data analysis was managed using NVivo 11.0 software and conducted in accordance with Colaizzi’s seven-step phenomenological method (Colaizzi, 1978). This rigorous process included repeatedly reading the transcript to gain an overall understanding, extracting important statements, encoding recurring meaning units, summarizing and distilling potential meanings, formulating detailed descriptions, summarizing the topic into broader concepts, and finally feeding the results back to the participants for inspection and verification.
We adopted a variety of strategies to enhance the rigor and credibility of the research. Experienced clinical interviewers first establish a harmonious relationship with the participants to help them discuss sensitive experiences candidly. We prepared an interview outline in advance and recorded the relevant background information of the participants. Interviewers consciously avoid leading questions when asking questions to minimize the impact to the greatest extent. After the interview, two researchers encoded the data, compared the results with the original interview records, and resolved any differences through team discussions. Finally, the participants verified the results. Throughout the entire research process, we also employed the practice of constantly reflecting on and improving the interview strategies to ensure the authenticity and validity of the data.
This study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Tong et al., 2007).
Ethical Considerations
This study was approved by a local hospital’s Institutional Review Board and conducted in accordance with the Declaration of Helsinki. Prior to each interview, participants were informed that their involvement was entirely voluntary. Audio recordings and transcripts were kept strictly confidential, and participants were free to withdraw or decline to answer any questions at any time without consequences. During the interviews, special attention was paid to participants’ negative emotions, and empathetic support was provided when necessary to prevent potential psychological distress.
Results
Multiple Caregiving Burdens
High Caregiving Load
Most caregivers reported that, due to the young age of children with tic disorders, daily care-giving required substantial time and effort. To avoid increasing the child’s psychological burden, caregivers often suppressed their own anxiety, which further contributed to physical exhaustion. “Administering medicine is so difficult. Just giving my child medicine takes two hours every day—I feel like I’m about to collapse [N1].” “During that period, I focused entirely on curing my child. I would consult doctors or even try traditional remedies—anything that could help my child recover. I accompanied my child in avoiding nearly forty foods he could not tolerate, gave him bitter herbal medicine, took him to play and get sunlight every day, all while enduring psychological anxiety and distress. I couldn’t show it, fearing it would scare him. I felt completely drained [N7].” “Most children with this condition have allergies, which makes caregiving extremely demanding. My child is allergic to so many foods that preparing meals is nearly impossible. I spend every day researching suitable recipes and trying to make grains and beans appealing, to avoid foods he cannot eat due to wheat allergies [N9].”
Financial Burden
Due to the need for repeated medical visits, many caregivers have to take unpaid leave to accompany their children, and the high medical costs also impose a heavy economic burden on the caregivers. This often leads to a vicious cycle of “treatment - poverty”. “The monthly medication cost for my child alone exceeds 4,000 RMB, and it cannot be reimbursed [N8].” “Since my child became ill, we have spent nearly 70,000 RMB on medications. At this rate, we simply cannot afford it [N6].” “After learning how serious this illness could be, I resigned from my job to care for my child full-time. Our household income decreased further, and we had to cut everyday expenses to cover treatment [N11].”
Barriers to Accessing Care
Many caregivers point out that seeking medical treatment in China faces numerous challenges. The shortage of specialist doctors leads to limited consultation time, difficulty in making appointments, and uneven distribution of medical resources, forcing patients to seek medical treatment across regions multiple times. Once the child patient is in the acute stage of the illness, it further intensifies the pressure and sense of helplessness of the caregivers. “Appointments with good specialists are extremely hard to get. Online or phone booking never works, so we have to buy expensive tickets from scalpers. Even then, sometimes we can’t get one. We wait in line at the hospital, clinging to the hope of getting timely treatment [N10].” “When we come to the provincial capital, the queues are so long that consultations are very brief. Even if we finally see the doctor, it lasts only three minutes. Good specialist resources are extremely limited [N8].” “Children with this disorder are mostly treated as outpatients, with no hospitalization arranged. Multiple follow-up visits are necessary, and the queues are very long [N3].”
Family Tension
Differences in understanding of diseases, dietary management and parenting concepts often lead to internal conflicts within families. Parents have different expectations for their children’s future growth, and it is also very common for young parents and grandparents to have differences in parenting concepts. “My husband and I have different expectations for our child. He wants better academic performance, while I just hope the child grows up healthy [N2].” “It’s difficult to coordinate dietary restrictions with the elders. They spoil the child and sometimes buy foods he is not supposed to eat [N4].” “I also have to calm the family, whose concerns are even greater than mine. For instance, my husband constantly asks whether this is hereditary and whether it can be cured. I have to manage my own stress while responding to family emotions, which sometimes makes me lose my temper [N1].”
Emotional and Psychological Distress
Disease-Related Anxiety
Caregivers frequently worried about symptom recurrence and potential comorbidities, including ADHD, OCD, anxiety, depression, and sleep disorders (Girgis et al., 2022). This persistent uncertainty undermined their psychological stability. “We’ve been treating this for over two years, but the problem remains. I keep asking myself whether this illness can really be cured. What will happen to my child in the future [N5]?” “I’ve read that many children with this disorder also have attention deficits and learning difficulties. Although my child hasn’t shown any signs yet, I worry about school [N10].” “The symptoms have almost disappeared recently. I hope this treatment works and that they never recur. My child is growing more aware, and I worry that relapses could leave lasting psychological scars [N11].”
Stigma and Social Embarrassment
As children with tic disorders entered school, caregivers expressed heightened concern about the social repercussions of their child’s symptoms. They worried that peers, teachers, and the broader community might misunderstand or judge their child, which contributed to anxiety, social withdrawal, and protective behaviors on the part of the caregiver. “When he reached third or fourth grade, he realized his condition and kept making faces and gestures in class. This affected his self-esteem over time [N8].” “I’m worried he’ll be mocked by classmates for blinking or making noises [N10].” “When my child first developed the disorder, I was reluctant to take him out for fear of being asked questions. On a few occasions, I said it was a tic disorder, but people assumed it was epilepsy or some other condition, so later I just said he had allergies [N2].” “A friend’s child played with mine, and I noticed him constantly clearing his throat and shrugging. When I asked if my child had a tic disorder, the friend denied it and seemed upset, claiming it was just a bad habit. Later, I learned she knew about it but didn’t want to admit it [N13].”
Guilt and Self-Blame
Many caregivers reported experiencing persistent feelings of guilt, often attributing their child’s disorder to their own parenting practices, emotional responses, or personal characteristics. This self-blame contributed to ongoing psychological distress and heightened anxiety about their caregiving effectiveness. “Honestly, I still feel very guilty today. I am not a competent mother and feel I’ve let my child down [N8].” “I may have been too strict or impatient with him. After I lost my temper, he felt frustrated, and his symptoms appeared. Since the diagnosis, I have been very self-critical [N11].” “Sometimes his symptoms reappear after I scold him for not doing homework. I feel extremely guilty [N2].”
Emotional Exhaustion
Prolonged caregiving for children with tic disorders imposed significant psychological and physical strain on caregivers, often leading to chronic stress, heightened anxiety, fatigue, and, in some cases, thoughts of collapse or hopelessness. “At that time, I felt completely broken and hopeless; sometimes I even thought of giving up with my child [N3].” “Helping him with homework was the hardest. Yesterday, he didn’t write a single word in half an hour, and nothing I did worked. I thought I’d be driven crazy [N4].” “I watched him show symptoms but had to pretend not to notice, feeling anxious inside but hiding it so as not to scare him [N13].” “His teacher contacted me about his inattention in class. I explained the disorder to the teacher to gain understanding, but I felt completely helpless [N9].”
Caregiving Challenges and Coping Strategies
Knowledge-Related Anxiety
Most caregivers initially lacked awareness of tic disorders. They turned to the internet for information, but inconsistent and sometimes alarming information often increased anxiety. “Why does my child have these symptoms? Where did it come from? I still don’t understand [N5].” “I’ve been searching online, but every source gives different timelines for recovery—some say by 12, others 14. I don’t know which to trust [M8].” “I learned more about the disorder, but knowing more actually made me more worried [N1].”
Parenting Cognitive Restructuring
Over time, caregivers adjusted expectations, communicated more gently, and prioritized the child’s health, psychological security, and daily development over academic performance. “I’ve learned to let things go naturally. Even if his grades are not great, he will be fine as he grows up [N6].” “As long as my child grows up healthy, I am grateful [N2].” “I accept everything about my child now and try to provide a relaxed environment to promote healthy psychology and character [N3].” “I just hope he can live like a normal child, and that his life and school are not affected [N7].”
Emotion Suppression and Avoidance
Without professional psychological support, caregivers often managed emotions independently. Temporary emotional release or self-persuasion helped maintain surface stability but might conceal delayed psychological crises. “After crying for two days, I gradually convinced myself to move on [N1].” “I never thought about how to relax. I just suppressed everything and didn’t consider releasing my emotions or seeking help [N6].” “I dealt with it myself, checked information online, and comforted myself mentally [N12].” “I’ve read some psychology books in the past, but they didn’t help much [N7].”
Discussion
This study employed a descriptive phenomenological approach to systematically collect and analyze the emotional experiences and caregiving challenges of primary caregivers of children with tic disorders. Through inductive thematic analysis, three core themes were identified: (i) multiple stressors, (ii) emotional and psychological distress, and (iii) caregiving challenges and coping strategies. These themes comprehensively reflect the diverse difficulties faced by caregivers during prolonged caregiving, including sustained physical and psychological strain, emotional distress, and limited coping strategies.
The findings indicate that primary caregivers of children with tic disorders commonly experience multiple burdens spanning physical, economic, medical, and family domains. Given the young age and low cooperation of children with tic disorders, daily care requires substantial time and energy. Moreover, because tic symptoms are easily influenced by environmental emotions (Ruhrman et al., 2023), caregivers must maintain a stable environment and deliberately suppress their own anxiety, presenting a calm exterior to prevent symptom exacerbation, which further increases physical and mental fatigue, consistent with previous studies (Johnson et al., 2023; Yang et al., 2019). Economically, high medical costs and income disruption due to caregiving place many families in a vicious “treatment-poverty” cycle, aligning with findings by Buckle et al. (Buckle et al., 2023). Additionally, scarcity of specialist resources and barriers to timely medical consultation pose significant challenges for caregivers seeking professional guidance, further confirming difficulties in the current healthcare environment (Walkowiak et al., 2024). According to Murray Bowen’s family systems theory (Calatrava et al., 2022), families function as interdependent systems, and interactions among members profoundly affect individual psychological states and behaviors. In this study, caregivers frequently needed to manage conflicts arising from differences in disease understanding, parenting approaches, and expectations among family members, which further diverted their attention and energy—a phenomenon consistent with prior research highlighting the negative impact of family conflict on chronic disease caregiving (García-Marín et al., 2023). These factors interact and collectively contribute to the heavy physical and psychological burden on caregivers (Wattanarojjanakit et al., 2023; Wellen et al., 2023).
Caregivers commonly experienced significant emotional and psychological distress. Concerns about the uncertainty of the disease, symptom recurrence, and comorbidities such as ADHD and OCD eroded caregivers’ psychological stability, with prolonged anxiety often accompanied by increased depressive symptoms (Fjermestad et al., 2024), echoing findings by Wellen (Wellen et al., 2023). As children reached school age, tic symptoms were frequently misunderstood by peers, potentially leading to social exclusion. This sense of stigma not only arises from external judgment but also from caregivers’ self-blame for perceived obstacles in their child’s social development, exacerbating psychological burden, consistent with prior studies (Suh et al., 2022). Notably, many caregivers attributed the disorder to their own parenting or genetic factors, resulting in persistent guilt and self-blame, consistent with Hu et al. (Hu et al., 2024). This reflects cognitive distortions stemming from a lack of scientific understanding of the disease, which can influence treatment decisions. Under such chronic stress, accumulated emotional distress sometimes led to heightened tension, sleep disturbances, and even suicidal ideation, underscoring the severity of psychological health risks.
Most caregivers in this study had limited educational backgrounds and insufficient professional knowledge of the disorder. They often resorted to online resources for self-education, yet the abundance of inconsistent and low-quality information frequently amplified catastrophic thinking and anxiety, consistent with Liu et al. (Liu et al., 2024). Caregivers’ attitudes toward their children gradually shifted from “achievement-oriented” to “health-oriented” and from “authoritative control” to “collaborative management,” a pattern commonly observed in families dealing with chronic pediatric conditions (Dandy et al., 2024; Spurr et al., 2023). However, this shift often represents passive adaptation to perceived helplessness rather than a rational cognitive restructuring, implicitly limiting the child’s developmental potential. Furthermore, most caregivers lacked effective means for emotional release (Brandão et al., 2024); in this study, caregivers primarily relied on brief venting or avoidance to manage negative emotions, without structured social or professional psychological support. While such strategies can temporarily stabilize emotions, unresolved negative emotions may accumulate over time, increasing the risk of depression and anxiety.
Given the multifaceted challenges faced by caregivers of children with tic disorders, constructing effective support systems is crucial. Future interventions should leverage these findings to develop targeted support strategies. For instance, patient-centered care could be extended to family-centered care, integrating routine psychological assessment of caregivers and timely counseling for those experiencing emotional crises. Improving access to specialist resources and reducing the burden of cross-regional medical visits are also essential. Digital platforms, such as official hospital WeChat accounts and short-video services like Douyin, could disseminate systematic knowledge, offer Q&A sections with professional guidance, and provide accurate caregiving resources, reducing uncertainty and fear among caregivers. Additionally, school- and community-level health education can enhance public awareness, reduce stigma, and foster a supportive social environment. Policy measures could include expanding insurance coverage for long-term treatment of tic disorders and offering flexible employment support to parents who interrupt work, alleviating financial and caregiving burdens.
This study has several limitations. First, participants were recruited from the outpatient department of a single hospital’s psychosomatic medicine clinic, and the sample size was relatively small, limiting generalizability across different regions and cultural backgrounds. Second, most participants were mothers, with few male caregivers included, potentially constraining understanding of gender-specific caregiving experiences. Future research should expand sample diversity, including more male caregivers, to provide a more comprehensive understanding and inform tailored interventions.
Conclusion
The findings indicate that primary caregivers of children with tic disorders experience significant gaps in disease knowledge, emotional regulation, and coping strategies. Caregivers commonly face physical and psychological stress, disease-related anxiety, stigma, and self-blame, yet lack systematic psychological support and caregiving guidance. These results underscore the urgent need for evidence-based education and psychological interventions for caregivers. Optimizing family caregiving models, establishing information support platforms, and promoting inclusive social education can enhance caregiving quality and improve recovery outcomes for children.
Footnotes
Acknowledgments
The authors sincerely thank the investigators for their assistance in the study conduct and the participants for generously sharing their experiences and insights, which were pivotal to the completion of this research. Gratitude is extended to all individuals and institutions that contributed to this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Doctoral Research Start-up Fund of Shandong Second Medical University (Grant No. 041176).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.