
Abstract
Objective
Avoidant Restrictive Food Intake Disorder (ARFID) remains under researched and there are currently no National Institute for Health and Care Excellence (NICE) guidelines, the UK body that produces national, evidence-based clinical guidelines for treatment. Our study aims to capture the qualitative experiences of carers of young people with ARFID who have received treatment, aiming to understand caregivers’ experiences of caring for a young person with ARFID and what their experience of treatment is like.
Method
Qualitative semi-structured interviews with 11 caregivers of young people receiving treatment in a national tertiary feeding and eating disorder service were conducted. Thematic analysis was used to analyse interview transcripts, following Braun and Clarke’s six-phase approach (2006, 2022a, 2022b).
Results
Four overarching themes were developed: Care with Constant Concern: the emotional and practical impact of caring for a child with ARFID; Navigating Fragmented Systems: delays, knowledge gaps, and access barriers; Balancing Survival and Safety: the complexities of implementing feeding interventions; and Building Strength Through Shared Experiences: the value of communication and collaborative support within treatment.
Conclusion
Effective management of ARFID requires clear care pathways, integrated multidisciplinary plans, and recognition of caregiver burden. Services should balance physical safety with strategies to promote oral exposure while adopting flexible, child-led approaches. Future research must amplify young people’s voices and broaden caregiver perspectives to inform responsive, evidence-based interventions.
Plain Language Summary
Avoidant Restrictive Food Intake Disorder (ARFID) is an eating disorder where children and young people avoid or restrict food, which can affect nutrition, growth, health, and everyday life. This study explored the experiences of caregivers whose children accessed a specialist tertiary feeding service. Caregivers took part in interviews about their experiences of seeking support, receiving treatment, and navigating healthcare systems. The interviews were analysed to identify common themes across experiences. Caregivers described significant emotional, practical, and financial challenges linked to caring for a child with ARFID. Many reported difficulties accessing support and experienced delays, limited understanding of ARFID among professionals, and disjointed care across services. They also described feeling misunderstood or judged by others. Caregivers valued compassionate clinicians, collaborative communication, coordinated care, and opportunities for peer support. The findings highlight both the benefits of specialist feeding services and the challenges families experience when trying to access support. The study suggests that improving professional awareness of ARFID, increasing coordination between services, and providing earlier access to specialist support may improve experiences for children, young people, and caregivers.
Keywords
Background
Avoidant Restrictive Food Intake Disorder (ARFID) is a relatively new diagnosis characterised by an eating disturbance encompassing one or more of the following: lack of interest in food, sensory-based avoidance, or concern about the aversive consequences of eating (APA, 2022). These behaviours must result in nutritional compromise (including poor weight gain, faltering growth, nutritional deficiencies, dependence on enteral feeding or supplements) and/or psychosocial impairment. Despite its inclusion in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), ARFID remains under-recognised, and prevalence estimates vary widely. A systematic review of 30 studies reported an incidence of 2.02 per 100,000 in child clinical populations, with non-clinical prevalence ranging from 0.3% to 15.5% (Sanchez-Cerezo et al., 2023). However, qualitative findings suggest both primary and secondary healthcare professionals struggle to identify and treat ARFID (Dinkler et al., 2023; Harrison, 2021), and referral pathways to specialist services are frequently unclear or delayed (Lambert et al., 2025).
Failure to identify and treat ARFID presents significant public health concerns due to associated medical complications. Nutritional deficiencies are of particular concern given the possibility of stunted growth in adolescence (Brigham et al., 2018), especially in those who have been chronically malnourished since infancy because of feeding difficulties. Low weight and stunted growth can lead to decreased cognitive capacity and cardiac abnormalities in children, not dissimilar to Anorexia Nervosa (AN) (Friars et al., 2023; Uzogara, 2016). Despite this, there are currently no NICE guidelines for ARFID (National Institute of Health and Care Excellence, 2017), so there is a need for an improved evidence base for effective care and service provision.
A key challenge in recognising and treating ARFID lies in its heterogeneous presentation. Current literature commonly conceptualised ARFID as comprising three primary maintaining profiles or ‘drivers’ consistent with diagnostic criteria: sensory-based avoidance, where individuals restrict intake due to sensory properties of food; lack of interest in eating or food, associated with low appetite, early satiety, or limited motivation to eat; and fear of aversive consequences, in which avoidance is driven by anxiety related to choking, vomiting, or other negative experiences (Thomas et al., 2017). These presentations are not mutually exclusive, and recent evidence suggests young people with ARFID more often present with a combined profile, exhibiting overlapping features across multiple domains (Sanchez-Cerezo et al., 2024). Importantly, these distinct yet overlapping mechanisms may require different therapeutic approaches, complicating treatment planning and necessitating flexible, multimodal interventions.
In the UK, the National Health Service (NHS) operates across three levels of care: primary care (e.g., general practitioners), secondary care (e.g., local child and adolescent mental health services (CAMHS) and paediatric services), and tertiary care, which provides specialist services for complex cases (NHS Digital, 2022). Access to tertiary care typically requires referral from secondary care, often following significant deterioration or lack of progress in standard treatment. As such, treatment approaches for ARFID vary across services, with interventions often tailored to the individual’s presentation in tertiary care.
Emerging evidence suggests the effectiveness of Cognitive Behavioural Therapy for ARFID (CBT-AR) in adult populations, and behavioural interventions coupled with caregiver training in children (Hodges et al., 2023; Thomas et al., 2021). While CBT-AR has demonstrated positive outcomes in children (Willmott et al., 2024), they may not always be appropriate given high rates of comorbidities, and family-based treatments may be utilised in these cases (Bourne et al., 2020; Lock et al., 2019). However, the complexities of ARFID remain inadequately addressed within existing service models, emphasising an urgent need for well structured evaluation frameworks to better understand the effectiveness of current interventions. Although most research to date has focused on quantitative measures, qualitative studies suggest that current treatment settings often fail to meet the specific needs of young people, impacting overall treatment satisfaction and adherence (Mitrofan et al., 2019). These limitations are frequently attributed to a lack of ARFID specific knowledge among healthcare professionals and fragmented service provision, particularly across primary, secondary, and tertiary care levels (Harrison, 2021). There is a pressing need for qualitative evaluations to better understand the lived experiences of those affected by ARFID, providing richer insights to inform service development and policy. As such, this service evaluation seeks to add to the evidence base by capturing the perspectives of families undergoing treatment in a tertiary feeding service, helping to identify strengths and gaps in current service provision.
This qualitative service evaluation was conducted within a national tertiary feeding disorder service in the UK, supporting children and adolescents with Avoidant Restrictive Food Intake Disorder (ARFID) and other feeding difficulties. The study aims to explore: (1) parents’ experiences of caring for a child with ARFID, and (2) their experiences of treatment within a tertiary feeding disorder service. Interventions offered include the Parent Intervention Programme (PIP), a six-session online group providing psychoeducation and behavioural strategies to enhance parental understanding and confidence, alongside Cognitive Behavioural Therapy for ARFID (CBT-AR), exposure-based approaches, and family-based treatment tailored to individual presentations and developmental stages. School education and training are also provided to create supportive environments for behavioural and exposure work where appropriate. By examining caregivers’ lived experiences, this evaluation seeks to identify facilitators and barriers to accessing support, assess the emotional and practical impact of ARFID on families, and explore perceptions of service responsiveness and effectiveness.
Methods
Design and Materials
The study employed a qualitative design using semi-structured interviews to explore the experiences of caregivers. Semi-structured interviews were chosen to allow for an in-depth exploration of participant’s perspectives while maintaining a flexible structure to accommodate individual experiences (Adeoye‐Olatunde & Olenik, 2021).
A semi-structured guide used to facilitate caregiver interviews was developed collaboratively with the research team and clinicians within the service, drawing on clinical expertise and informed by consultations with healthcare professions. The interview included nine open ended questions focusing first on what carer’s experiences are of caring for a young person with ARFID, and secondly what their experiences have been of treatment interventions. Prompts were used to explore topics in more depth and detail. The interview schedule can be found in Appendix 1.
Interviews were conducted remotely online, lasting approximately 45-60 minutes and were recorded for transcription purpose, increasing accessibility and convenience for participants. Three female clinician researchers affiliated with the service were involved in the service evaluation and had prior training in qualitative research. Interviews were conducted by two members of the research team: ZS (Assistant Psychologist) and CB (Undergraduate Research Assistant), who had no existing therapeutic relationships with the participants. One clinician-researcher, DL (Clinical Psychologist), had pre-existing therapeutic relationships with some young people and families and therefore did not conduct interviews. DL contributed to data analysis alongside the wider research team, with interpretations discussed collaboratively to support reflexivity and minimise the influence of prior assumptions. Participants were provided with information outlining the study’s purpose, procedures, and ethical considerations. Informed consent was obtained through signed consent forms prior to participation.
Participants
A total of 11 female caregivers for children aged 6-16 years who were treated at a tertiary service took part in the study. Participants represented eight NHS trusts from across the UK. Participants were recruited through convenience sampling, whereby care coordinators contacted caregivers who had expressed interest in sharing their experiences of the service. This approach enabled the inclusion of caregivers with direct experience of tertiary level intervention, though it may privilege the perspectives of families who remained engaged with services.
Demographic data included caregiver gender and child age, but ethnicity of caregivers was not collected within the scope of this service evaluation. To acknowledge their time, participants were offered a £25 voucher.
Inclusion criteria for interview participants were: (1) aged 18 years or older, (2) fluent in English, and (3) had a child who had previously received assessment and intervention within the Feeding and Eating Disorder Service (FEDS). Exclusion criteria included caregivers who were not fluent in English or whose child had not yet received any intervention within FEDS.
Analysis
Data were analysed using reflexive thematic analysis, following the six-phase process outlined by Braun and Clarke (2006, 2022a, 2022b) and without the use of qualitative analysis software. Reflexive thematic analysis conceptualises themes as actively generated through the researchers’ interpretative engagement with the data, rather than as patterns that passively emerge. This approach prioritises depth of engagement, transparency, and reflexivity, rather than notions of data saturation. The phases included familiarisation with the data, systematic coding, development of initial themes, incremental refinement of themes, defining and naming themes, and producing the final report. The consolidated criteria for reporting qualitative research were followed and adhered to throughout (Tong et al., 2007).
Coding was conducted using an inductive approach. While analysis was conducted at a semantic level, focusing on participants’ personal accounts, interpretative engagement from researchers supported the exploration of underlying meaning at a latent level. Themes were actively generated through researchers’ interpretative engagement with the data, rather than emerging organically. An initial coding framework was developed collaboratively by three members of the research team, ZS, CB, and DL, and refined through continued engagement with the transcripts Regular meetings were held to enhance reflexivity throughout the process and deepen analytical insight. The researchers’ positionality as clinician-researchers working within the service was acknowledged and reflected upon as an analytical resource rather than source of bias, consistent with a reflexive approach. Transcripts were manually transcribed and reviewed for accuracy and were not returned to participants for comment or correction. In line with reflexive thematic analysis, analytic sufficiency was prioritised over data saturation. While the sample size was relatively small, it enabled rich engagement with caregiver accounts and the development of coherent, theoretically meaningful themes.
Ethical Considerations
The following study was registered and approved as a service evaluation project by the Great Ormond Street Hospital Research and Development Service. Informed consent was obtained from all participants prior to data collection, and they were informed of their right to withdraw their data at any point up until publication.
Results
A total of four main themes and twelve sub-themes were developed through researchers’ interpretative analysis of carers’ interviews. Each theme is presented below with embedded supporting quotations to illustrate the findings. See Figure 1 for thematic map. Thematic Map.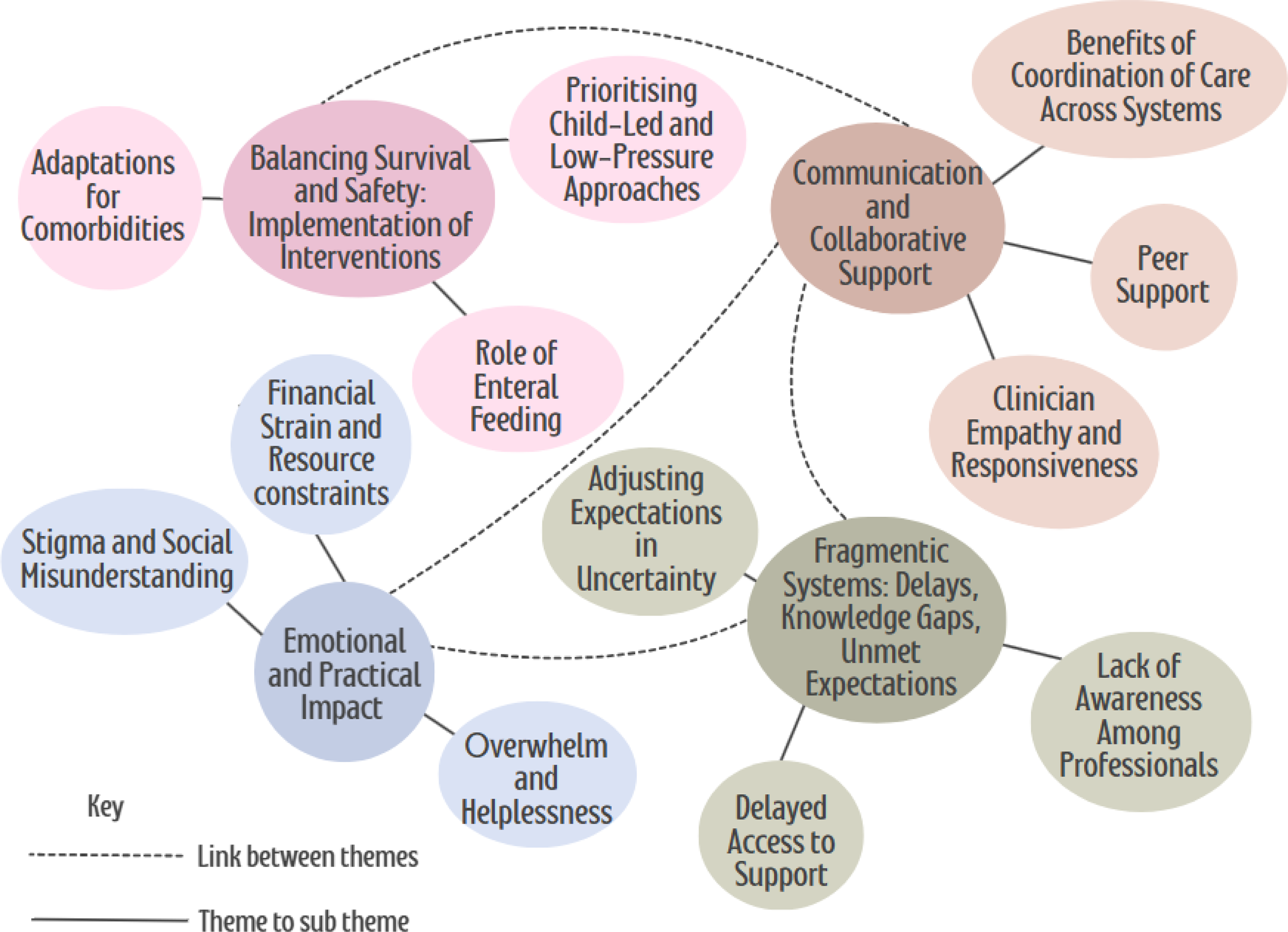
Participant Characteristics
All caregivers (n = 11) were female parents. Over half (54%, n = 6) had a female child. Children’s ages ranged from 6–16 years (M = 9.9, SD = 3.1). Most children were White British (64%, n = 7), with others from mixed ethnic backgrounds (18%, n = 2), Asian or Asian British Indian (9%, n = 1), and White Other (9%, n = 1).
Research Question 1: What Are Carers’ Experiences of Caring for a Young Person With ARFID?
Parents shared experiences of significant emotional, social and financial burdens, as well as the challenges, stresses and relief to access treatment.
Theme 1: Care With Constant Concern: The Emotional and Practical Impact of Caring for a Child With ARFID
Carers’ Experiences of Emotional Overwhelm and Helplessness
Across the interviews, the emotional toll on parents and caregivers was a dominant theme. Many described feeling overwhelmed by stress, helplessness, and exhaustion: I’m just lying awake at night worrying and crying… how can I help him? I don’t know what to do—I don’t have the tools to know how to help him. And I think that is the hardest thing.
Another parent shared constant anxiety that accompanies caring for a child with ARFID: It’s anxiety. Constant anxiety, you know, always. And I feel myself triggered at certain point in time, when I know that she’s not had a lot for maybe a few days, a couple of days, whatever, and I can feel myself wanting to lose it at her.
Additionally, caregivers often struggled with others’ lack of understanding, compounding their sense of isolation. One parent shared: Your worst nightmare is what happens if they get seriously sick and you’re living with that possibility all the time. You end up becoming quite resilient, you don’t need people undermining that worry because it just is what it is. You’re worried.”
These reflections illustrate how ARFID profoundly affects family well-being and parents’ sense of competence. The emotional strain was frequently linked to uncertainty and the perceived lack of knowledge and resources surrounding ARFID, leaving caregivers feeling unsupported and ill-equipped to manage their child’s needs.
Managing Financial Strain and Resource Constraints
Alongside the emotional burden, parents frequently described significant financial pressures associated with caring for a child with ARFID. These challenges were primarily linked to the cost of preferred or “safe” foods, reliance on specific brands, and expenses incurred for travel to specialist appointments. For many families, following clinical advice or implementing dietary recommendations was complicated by budget constraints. One parent explained: I will go to the shop and buy him anything if he’ll eat it… my food bill is over one and a half thousand pounds a month.
Others highlighted the unsustainable nature of preferred foods: I know lots of parents that have got stuck going to McDonald’s seven days a week and that’s not financially viable.
One parent also noted that travel for specialist care added further strain: Appointments at… take 10 minutes, but the travel costs and time off work are huge.
These findings demonstrate how financial strain permeates everyday life for families managing ARFID. For many, these pressures limited their ability to follow clinical recommendations, forcing difficult decisions about which strategies were affordable. This financial compromise often intensified feelings of guilt and stress, illustrating how practical constraints intersect with the emotional burden placed on carers.
Navigating Stigma and Social Misunderstanding
Parents frequently described experiencing judgment from others, both in public settings and within their extended families, regarding their child’s feeding difficulties. Social scrutiny often intensified feelings of isolation and defensiveness, compounded by a widespread lack of awareness about ARFID. One parent expressed frustration: It’s seen as a middle-class affectation in the press, like parents being dramatic.
The perception of misunderstanding extended beyond strangers to immediate social networks. Families reported that even well meaning relatives and friends frequently offered simplistic explanations or advice, often minimising the complexity of ARFID. Another parent reflected: We needed strength to block out the noise from society, and I’m gonna include family in that as well. They keep saying give her this and that… It’s about educating—it is not just a fussy child.
Research Question 2: What Are Carers’ Experiences of Treatment Within a Tertiary Feeding Disorder Service?
Carers reflected on their experiences of treatment, including both medical and psychological treatment within the service. Analysis highlighted three core themes:
Theme 2: Navigating Fragmented Systems: Delays, Knowledge Gaps, and Unmet Expectations
Encountering Delays in Accessing Support
Caregivers consistently described significant delays in accessing appropriate support for their child’s feeding difficulties. Carers reported being passed between services, such as secondary care services and paediatrics, without clear guidance or recognition of ARFID: We were ping-ponged between CAMHS and paediatrics for over a year.
These delays often occurred despite evident clinical need, contributing to emotional distress and a sense of helplessness: Even though she was clearly struggling, CAMHS said she didn’t meet the threshold.
The frustration was further echoed by another parent: I thought, how low does his weight have to go before we get help?
These accounts underscore the urgent need for streamlined referral pathways and the absence of clear criteria for ARFID, which left families without timely intervention.
Confronting Lack of Awareness Among Professionals
Caregivers frequently reported that healthcare professionals in primary and secondary care lacked awareness of ARFID, further contributing to delays in diagnosis and appropriate support. Parents described feeling compelled to educate clinicians themselves, often encountering professionals who had never heard of the condition: I had to educate the clinicians myself because they had never heard of ARFID.
This lack of recognition often resulted in misdirection to services that were not equipped to manage feeding difficulties, hindering early engagement and prolonging distress. As one parent explained: Primary care services haven’t heard of it… or where to go when you feel this concern for your child, and how to find the right help within the care system.
These accounts underscore a systemic gap in professional knowledge, highlighting the need for targeted training alongside clearer referral pathways to ensure timely and appropriate support for families.
Adjusting Expectations in the Face of Uncertainty
Given these systemic knowledge gaps and fragmented referral pathways, setting realistic expectations emerged as a critical component of care. Parents emphasized that, in the absence of clear information from professionals, they often entered treatment hoping for rapid improvement, only to experience frustration and self-blame when progress was slow: You think you’re doing something wrong every day because nothing changes quickly.
However, parents noted that honest conversations about the likely long-term nature of ARFID were essential for reducing anxiety and fostering resilience: Don’t expect this is going to be your answer, it is a lifelong journey… let’s hope one day he does expand his diet, but I think that if you know beforehand you will not get him miraculously eating again, it is quite useful.
Taken together, these accounts suggest the importance of managing expectations as part of an early intervention, particularly alongside ongoing systemic barriers and an overall lack of awareness of ARFID.
Theme 3: Balancing Survival and Safety: Implementation and the Complexities of Feeding Interventions in ARFID
Negotiating the Role of Enteral Feeding
Alongside psychological interventions, parents expressed complex and often conflicting feelings about enteral feeding interventions. While many acknowledged its critical role in safeguarding neurological development and overall health, they also questioned whether it was always necessary:
I sometimes think, could I have gotten away without that PEG (percutaneous endoscopic gastrostomy)? But then I think, I don’t know if developmentally that would have been putting her at risk.
Despite recognising its protective role, several parents reported that once their child became reliant on tube feeding, oral exposure to food often declined or ceased altogether. One parent noted: It was sort of sold as a bit of a lifeline when really, I felt it should have just been like it's there as your safety net. Because it was used as her main food source for everything, I felt like the rest of it kind of got put to the side and got in the way of oral intake.
This reflects concerns that enteral feeding, if not paired with ongoing oral exposure strategies, may inadvertently hinder progress toward oral feeding.
Parents also spoke about the stigma surrounding feeding tubes and the lack of understanding from others. One parent expressed frustration: There’s already, like, there’s a negative approach anyway, I think around feeding tubes, to then be compounded by seeing a child with a feeding tube, is eating pasta, well, actually, you have no idea how we got to the bowl of pasta, this is Olympic gold standard for us.
This quote illustrates how outsiders may misinterpret milestones, overlooking the immense effort behind small achievements and reinforcing stigma.
Prioritising Child-Led and Low-Pressure Approaches
A prevalent subtheme across interviews was the positive impact of interventions adopting a child-led approach. Parents consistently described how prioritising the child’s voice, pacing enhanced engagement, and adapting interventions based on developmental stages strengthened the therapeutic alliance and improved treatment outcomes: The sessions were amazing because it was at [child’s] pace, but also with that mindfulness—of yes, I know you want to play, but it’s going to bring in a bit of tasting.
Parents also described how adopting a child-led approach themselves reduced pressure and reframed expectations around mealtimes. This approach was viewed as essential for promoting gradual progress and reducing anxiety for both children and caregivers: Maybe just have that understanding. Yeah, your child doesn’t need to finish everything on that plate. You know, not to be as fearful.
Alongside this, carers highlighted the importance of continued exposure and repetition, recognising that ARFID interventions often require revisiting strategies over time as developmental stages and motivation shift. One parent reflected: I tried to learn as much as I can. If I’ve tried something, it didn’t work and I’ve forgotten about it—if I revisit it at a later stage, she’s potentially going to respond differently because she is older and bigger.
Taken together, these quotes illustrate that ARFID treatment may benefit from a dual focus: child-led, low-pressure approaches tailored to developmental readiness.
Adapting Interventions for Comorbid Conditions
Given the high prevalence of co-occurring conditions such as autism and ADHD among children with ARFID, parents consistently highlighted the need for tailored service adaptations. These adaptations were seen as essential for ensuring interventions are effective and sensitive to neurodivergent needs.
One parent described a negative experience with an inaccurate social story, a tool commonly used to prepare children for upcoming appointments by providing a simple, visual narrative of what will happen and what is expected: Some of the information on the social story didn’t happen in real life when we got there… Now in our case, this wasn’t a big deal… But I would say more broadly speaking, for families, it’s important if it’s on a social story, it happens—for some kids, it’s a deal breaker.
This underscores the importance of predictability and routine for children with autism, where discrepancies between expectations and reality can significantly impact engagement and trust in the service.
Another parent emphasised the value of structured approaches, specifically the use of graded exposure, a technique within CBT encompassing gradual exposure to feared situations, and scaling techniques within therapy to reduce anxiety Grading was useful… I think his autistic brain uses that to help anxiety. If you can put a number to something, it feels like how his brain works, and that helps
Lastly, one parent stressed the need to recognise diverse communication methods within the service, ensuring that a child’s voice is not overshadowed by adult assumptions: If you were a grown adult, you wouldn’t be allowing me to make a non-informed choice. If I’m clearly communicating in whatever means a child chooses to communicate, like non-verbal… I think that actually any action is a form of communication, and that’s being lost.
Theme 4: Building Strength Through Shared Experiences: The Value of Communication and Collaborative Support Within Treatment
The Value of Clinician Empathy and Responsiveness
Carers consistently emphasised the importance of clinicians who are responsive, empathetic, and able to build trust through clear communication. Responsiveness was described not only in terms of timely action but also in the ability to listen and validate concerns. Empathy was seen as a cornerstone of effective care, reducing parental anxiety and fostering a sense of partnership: I was so grateful when we got to you guys because you understood. I felt listened to, he felt listened to, and he formed a really good relationship with (therapist)—the only one he’s ever really formed. You hear a lot of people trying to make things better for you when actually you just want to feel validated. Listening to me was sometimes just having a platform to speak and someone listen and understand. And that took away that parent guilt for me.
Additionally, one carer highlighted the value of timely and responsive digital communication with their named clinician through the service’s messaging platform: She’s amazing. Anything I need to know, or I am confused about, I just go onto the app and ask. And I’m so glad. I feel like someone’s listening.
Such reflections suggest that timely, empathetic communication, both face-to-face or via digital platforms, was viewed as essential for building trust within the service.
Finding Strength Through Peer Support
A further sub-theme identified was the availability of peer support throughout the service, particularly in relation to the Parent Intervention Programme (PIP). Parents described the significant emotional impact of connection with others who shared similar experiences. Additionally, being part of a structured intervention helped normalise their experiences and reduced feelings of isolation, which are often exacerbated by the invisibility of ARFID: When you get there (PIP), it makes sense that you’re not the only parent or your child isn’t the only one suffering. Meeting other parents was invaluable; you don’t feel so alone.
However, a gap in peer support provision was noted for young people themselves: He’s never met anybody else with ARFID. I’m on a Facebook group… and we support each other. (He) has asked if he could meet somebody else with ARFID.
Although PIP fostered a sense of community among caregivers, children with ARFID might continue to feel isolated in their experiences. Parents expressed a desire for future service development to facilitate safe peer connections, recognising the potential psychosocial benefits of knowing they are not alone.
The Benefits of Coordinating Care Across Systems
Carers highlighted the importance of ongoing collaboration between the service and wider professional networks, including schools and local healthcare providers. Given the complex and often comorbid nature of ARFID, effective communication across agencies was seen as essential for ensuring consistent care.
When coordination was facilitated, parents described feeling supported and reassured: We had a multi-agency meeting that was really beneficial for me… it was with our GP and our local CAMHS. When school was fully aware of what truly is happening to that child, it made such a difference. They knew what was safe and what to avoid.
Such proactive communication helped align strategies across settings, reducing the burden on families to advocate alone and ensuring that interventions were reinforced beyond the tertiary service.
Conversely, when communication broke down, parents reported significant challenges obtaining accurate records of their child’s food intake at school, and in one instance, this was despite the child being in a small class with additional support. I look at a class of eight children, and I still can’t get written into a book what she actually ate. There hasn’t been communication between school and any department… I think that is probably needed for any child with issues.
This lack of integration left parents feeling isolated and concerned about gaps in care, particularly when schools or local services were unaware of the child’s needs or feeding plan. Overall, these accounts highlight that multiagency communication and shared understanding is essential for a child with ARFID, reducing risk of interventions being undermined.
Discussion
This study evaluated the experiences of young people and their families as they navigated a UK tertiary feeding and eating disorder service, identifying four overarching themes and twelve sub-themes related to clinical practice and service engagement. Given the limited research on service-level experiences of ARFID, this evaluation addresses a critical gap by centring the family voice to provide a nuanced understanding of caregiving challenges and treatment experiences within a specialist setting.
When discussing carers’ experiences of caring for a child with ARFID, an important theme related to the emotional and practical impact emerged. This reflects the profound burden experienced by parents of children with ARFID. Feelings of stress, helplessness, and exhaustion echo the broader eating disorder literature, where parental distress and perceived blame can negatively impact treatment (Hillege et al., 2006; Mitrofan et al., 2019). Consistent with these findings, parents in this study emphasised the importance of being listened to by professionals, identifying this as a potential buffer against carer burden. Similarly, further research found that emotional distress was intensified by limited-service availability, societal misunderstanding, and caregiver responsibility (LaMarre et al., 2023). Brimo et al. (2025) highlighted that parenting a child with ARFID was described as exhausting and all-consuming, often dominated by persistent worry and societal misunderstanding. This study adds to existing evidence by identifying financial strain as a significant and underexplored barrier. Specifically, the cost of specialised or preferred food was seen as unsustainable. Understanding these financial pressures is crucial, as they may influence parental capacity to persist with interventions. Addressing both emotional and economic burdens could improve parental wellbeing and the overall feasibility of ARFID service provision.
Specifically related to carers experience of treatment within a tertiary service, an important theme of “Communication and Collaborative Support” emerged, which encompasses not only professional’s interaction with the family but also the broader systemic exchange between services, young people, and support networks. Given the complexity of ARFID and common comorbidities such as ASD, anxiety, and gastrointestinal conditions (Bourne et al., 2020), these findings align with research and support the need for a multidisciplinary approach across services (Perez & Pesce, 2025; Winten et al., 2024). However, multi-agency communication is often hindered by systemic and organisational barriers, such as medical based language and resource allocation (Salmon, 2004), and so our findings emphasise the importance of consistent and clear communication between both professionals and families. This is in line with qualitative findings highlighting the importance of validation, clear communication, and collaborative clinician-family relationships (Brimo et al., 2025; Young et al., 2024). As children spend a substantial portion of their time in school, it is important to consider the positive impact school environments may have on progress. Importantly, teachers believe they would benefit from further training related to autism and feeding difficulties (Adams & Matsimela, 2023).
The perceived gaps in knowledge and lack of awareness across professional systems was felt to have direct consequences on recognition, referral, and continuity of care. This is common throughout eating disorder literature: that treatment isn’t often accessible until physical risk becomes severe (Johns et al., 2019; Regan et al., 2017). Research indicates that professionals often struggle to identify ARFID early, citing a general lack of knowledge and unclear pathways, causing a difficulty accessing care (Harrison, 2021). This is further echoed in qualitative research describing the difficulties caregivers experience navigating healthcare systems when caring for a child with ARFID, particularly related to diagnostic uncertainty and systemic barriers accessing care (Young et al., 2024). The delay in identification poses a significant risk given the potential impact on a child’s development, such as faltering growth and disruptions to milestones (Brigham et al., 2018; Tanner & Richmond, 2024). Within services, it is likely to have a negative impact on therapeutic relationship and thus quality of care provided, highlighting an important need to increase awareness throughout healthcare systems.
While ARFID has been recognised in the Diagnostic and Statistical Manual of Mental Health Disorders (DSM) since 2013, clinical practice has yet to catch up in terms of nationally standardised care pathways. The heterogenous nature of ARFID further complicates this and calls for highly individualised care plans tailored toward their specific presentation and comorbidities. Given the long-term nature of ARFID, particularly in the context of ASD (Fisher et al., 2023), carers felt that it was essential to manage expectations to allow them to plan for the future.
There was strong parental support for child-led approaches that prioritise emotional readiness and pacing to improve outcomes. This aligns with Kim et al. (2022) who found forceful caregiver strategies to be retrospectively viewed as unhelpful in ARFID. However, this must be considered in light of emerging structured models, such as Family-Based Therapy (FBT) for ARFID, focusing on parental empowerment and direct behavioural change (Lock et al., 2019; Rosania & Lock, 2020). While direct comparative evidence between child-led and parent-led approaches remains limited, FBT has shown to be effective in symptom reduction and weight restoration (Willmott et al., 2024). It may be that parent-led interventions become more urgent in contexts where the child is nutritionally at risk, presents with low motivation, or child-led approaches have failed to incite change.
Findings emphasise the need for individualised care and considering comorbidities, particularly those with intellectual disabilities which are underrepresented in current research (Bourne et al., 2020), neglecting support needs for a large subset of the ARFID population. Hambleton et al. (2022) similarly recommended early identification and management of comorbidities to improve outcomes in eating disorders.
Parents’ mixed relationship with enteral feeding reflects the lack of current ARFID-specific guidelines, and the potential feelings of loss around feeding their child (Royal College of Psychiatrists, 2022). While it can be lifesaving and protective in the short term, oral exposure may decline once enteral feeding is initiated. This is reflected in the literature, where feeding is perceived as sacrificed for safety (Ruiz, Fischer & Starr, 2024). Findings suggests that without a concurrent plan to manage oral exposure, enteral nutrition may delay progress, and structured guidelines are necessary to balance safety with recovery.
Strengths and Limitations
A strength of the study is that it was conducted within a national tertiary feeding disorder service, which provides a unique opportunity to capture diverse perspectives from families across the UK. Since the service accepts national referrals, the findings reflected experiences spanning different socio-demographic backgrounds and healthcare settings. This broad scope enhances the potential generalisability of the results, providing a comprehensive insight into challenges faced by families and the nature of interventions required.
It is important to acknowledge several limitations. All caregivers in the sample were mothers, and caregiver ethnicity was not collected, which restricts understanding of diverse caregiving perspectives, including fathers. While child ethnicity was recorded, the sample was predominantly White British, with limited representation from other ethnic backgrounds. This lack of diversity may reduce the applicability of findings to more varied populations. Additionally, all participants were drawn from a tertiary care setting, where secondary input is required for acceptance, meaning the sample may not reflect families managed solely in primary or secondary care. Finally, convenience sampling, while useful for targeting specific perspectives, may introduce selection bias. However, the inclusion of families from multiple NHS trusts may provide valuable, transferable insights to similar feeding and eating disorder services within the UK. As participants were recruited from a tertiary service using convenience sampling, findings may be less transferable to families supported exclusively in primary or secondary care, or those who disengaged prior to tertiary input.
Clinical Implications
Our findings highlight an urgent need for enhanced professional and public awareness to facilitate early identification and treatment of ARFID. Clear, standardised pathways, ideally embedded in national guidelines, would provide much-needed clarity in the recognition and management of ARFID.
Clinical teams should prioritise integrated care plans that balance the immediate physical safety with strategies that encourage sustained oral exposure, such as coordinated input from psychologists, gastroenterologists, and dieticians to optimise timing and methods for tube weaning. Developing clear, evidence-based guidelines on the role of enteral feeding in ARFID is critical to improve outcomes and reduce parental distress. Professionals should adopt a family-centred approach that recognises the emotional, financial, and social burdens parents face and provide regular psychosocial support, including peer support, as a result.
Lastly, while child-led approaches are valued for their emphasis on emotional safety and engagement, further research is needed to understand which treatment model, is more effective in cases of severe nutritional risk or low motivation.
Future Directions
Further qualitative research that captures the voices of young people is necessary to deepen our understanding of ARFID. It would also be useful to hear the voices of a broader range of caregivers, including fathers and siblings, and understand how we can continue to improve and develop innovative and responsive services to enhance outcomes for young people and their families. ARFID is recognised as a heterogeneous diagnosis, with presentations commonly characterised by sensory sensitivity, lack of interest in eating, and fear of aversive consequences, often with overlap. Further qualitative research may usefully explore whether caregiver burden, perceptions of risk, and experiences of intervention differ across ARFID presentations, as this may help inform more nuanced service pathways. Whilst current research focuses on the evidence base for different psychological interventions, it is important to consider other external factors, such as improving communication and addressing carer burden, to assess how they contribute to the effectiveness of treatment interventions.
Conclusion
The present study has highlighted key considerations for services supporting young people with ARFID. Effective management relies on communication with the wider multi-disciplinary team, recognising the complexity and comorbidities often present in this population. Similar to other mental health difficulties, families favour open and collaborative dialogue, particularly because of the overall lack of awareness of ARFID and the burden placed on caregivers. The increasing recognition of ARFID diagnoses suggests an urgent need for greater awareness and consistent care pathways across the UK. Given the mixed relationship with enteral feeding, further research should investigate the potential impact on oral feeding progress for young people and their caregivers.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is (partly) funded by the NIHR GOSH BRC. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.