
Abstract
Dialectical behavior therapy-informed (DBT) techniques have shown efficacy in reducing emotional dysregulation incidents among pediatric inpatient populations. In this study, a DBT-informed training intervention was administered to elementary school educators to assess its efficacy in reducing dysregulation incidents in the classroom and increasing confidence in de-escalation. A 60-min de-escalation training equipped educators with evidence-based strategies to reduce dysregulation incidents among elementary-aged children through early non-confrontational intervention. Participants tracked the number of dysregulation episodes three weeks before and after the intervention. Additionally, pre- and post-training surveys assessed the impact of the intervention on educator knowledge and confidence in de-escalation techniques. Data demonstrated a 22% improvement in educators’ confidence in addressing emotional dysregulation in students, a 52% increase in knowledge of trauma-informed care, 100% increase in knowledge of DBT principles, and 41% increase in knowledge of trauma presentations. There was also a 50% reduction in the number of post-training dysregulation incidents in the classroom. Most participants found the training valuable (89%) and were likely to recommend the training to others (94%). This pilot study suggests that a de-escalation training for educators may be effective in improving educator confidence in supporting students and reducing dysregulation incidents in the classroom.
Plain Language Summary
Why was the study done? Young children, especially those who have experienced childhood trauma, are emotionally vulnerable. This can manifest as emotional dysregulation and outbursts in inappropriate settings, such as the classroom. DBT is a type of psychological therapy that helps patients understand and manage strong emotions, handle stress in healthy ways, and improve communication. DBT has been successfully used with children in clinical settings. As such, we believe that it has the potential to be applied in school settings. Many NYC elementary students come from traumatic backgrounds and struggle to manage emotions in school, leading to challenges for educators. Training educators in DBT may equip them to better handle such incidents. What did the researchers do? We created a 1-hour training that taught educators at a NYC elementary school how to use DBT and trauma-informed skills to help calm a student who is having an emotional outburst, and to proactively prevent them from happening. We surveyed these educators weekly for 3 weeks before and after the training to see if it had an impact on these classroom outbursts. What did the researchers find? Nineteen teachers completed the training surveys, and ten completed the weekly surveys. After the training, there were half as many emotional outbursts occurring in classrooms as before the training. Many teachers reported feeling more confident in addressing outbursts after the training. Many also reported gaining knowledge in DBT and how to recognize and accommodate the consequences of traumatic life events in the classroom. Almost all teachers found the training valuable and were likely to recommend the training to others. What do the findings mean? This study suggests that DBT-informed trainings may help educators support vulnerable students in managing strong emotions in school. Such trainings can be widely implemented across public schools through integration with staff development programming.
Introduction
Emotional dysregulation is defined as difficulty in regulating the intensity, duration, and type of emotional reaction in an adaptive, contextually appropriate manner (Paulus et al., 2021). Dysregulation is a common reaction to early adversity such as familial instability, neglect, abuse, or trauma exposure (Keeshin et al., 2021). In childhood, emotional dysregulation may present as heightened emotional reactivity, irritability, mood instability, impaired cognitive functioning, and increased use of maladaptive coping strategies. Furthermore, research suggests that emotional dysregulation in early childhood is an important risk factor for the development of a range of psychiatric conditions, including anxiety and depression (Murray et al., 2025). This impact highlights the potential benefits of targeting emotional dysregulation early on to promote healthy development throughout childhood and into adulthood.
Dialectical behavior therapy (DBT) is a form of psychotherapy initially developed to treat borderline personality disorder (BPD) that targets emotional dysregulation through both acceptance-based and change-oriented strategies. It was later adapted for adolescents with success (Rathus & Miller, 2002). Today, studies increasingly demonstrate the promising use of DBT in the pediatric population to reduce incidence of general emotional dysregulation across care settings (Perepletchikova et al., 2017; Rizvi et al., 2024); a systematic review found it to be an effective method for regulating emotions and treating internalizing problems such as self-harm in children (Boustani et al., 2024). As such, there has been a parallel effort focused on providing de-escalation training, both DBT-informed and general conflict resolution-based curriculum, for healthcare staff interacting with this patient population, particularly in the inpatient setting (Forbat et al., 2017; Grundy et al., 2024; Hoffmann et al., 2023; Lelonek et al., 2018; Miles et al., 2023). Increased adoption of DBT techniques has resulted in improved emotional regulation and interpersonal functioning, amongst other positive impacts in children (Boustani et al., 2024).
Schools have long been overlooked in this research, yet this environment is highly impacted by emotional dysregulation events, particularly in areas with limited resources and a high-needs student population. In the classroom setting, the prevalence of dysregulation incidents presents significant challenges for both educators and the students themselves (Graziano et al., 2007). Increased dysregulation events, particularly at the elementary school level, are hypothesized to disrupt classroom environments, increase educator stress, and negatively impact student academic progression. In urban public schools with limited resources (such as high student-to-teacher ratios, limited staff training, and limited funding for special staff such as learning specialists), the current standard of care to address an emotionally dysregulated child is not uniform and can involve reactionary measures such as removing children from the classroom or sending them home. This can exacerbate the child’s emotional distress and disrupt the learning environment.
Furthermore, the classroom environment and the student-educator relationship provide unique opportunities for early intervention with maladaptive behavioral techniques and promotion of positive coping mechanisms. There have been a few studies emerging regarding identifying and addressing mental health concerns in students across the K-12 school system (Bohnenkamp et al., 2021; Soneson et al., 2024; Wingenbach et al., 2023). A 30+ lesson long socio-emotional learning curriculum entitled “Dialectical Behavior Therapy Skills Training for Emotional Problem Solving for Adolescents (DBT STEPS-A)” has been implemented in some American high school health classes with positive outcomes (Chugani et al., 2021). An elementary student adaptation (DBT STEPS-E) is also newly emerging. These curricula aim to empower students to build lifelong skills in emotional regulation. However, not all schools have the infrastructure to implement such a course, and teachers still cite the need for increased professional development training in the realm of acute de-escalation (Petrovic et al., 2022). Specifically, in low-income urban public schools where educators often feel overextended in a high-demand yet resource-constrained environment, a brief, low-burden training program may serve as an effective tool to enhance their confidence in addressing emotional dysregulation amongst students.
Finally, trauma in childhood can arise from witnessing or experiencing physical, psychological, or sexual abuse, immigration/refugee crises, substance use, criminal activity, homelessness, and more. In the school setting, this can significantly impact students’ ability to develop strong learning behaviors, form secure relationships with peers and teachers, and regulate negative emotions throughout the school day (Cole et al., 2013). Many educators in America do not receive training in principles of trauma-sensitive pedagogy or school practices (Alisic et al., 2012; Reddig & VanLone, 2023). This may involve integrating predictable classroom routines and non-punitive responses that prioritize safety, emotional validation, and repair over discipline (Cole et al., 2013). This training would be especially beneficial for schools with a vulnerable student body facing adverse childhood experiences, as is common in large urban cities.
No research has yet analyzed the impact of a brief training teaching educators how to promptly and effectively de-escalate acute emotional dysregulation in younger students using DBT-informed strategies and trauma-informed principles. Here, we pilot such a training for elementary school educators using evidence-based strategies, similar to those in curricula such as DBT-STEPS, in a simple format that is digestible and accessible to overburdened educators in low-resourced schools. We analyze the impact of the training on educator confidence and knowledge of DBT and trauma-informed care principles, as well as the impact of the training on the number of dysregulation incidents in the classroom.
Methods
This was a single-site, single-arm pre-post intervention study conducted at an under-resourced Manhattan elementary public school with a high-needs (i.e. high risk of emotional dysregulation based on established risk factors) student population. Most of the educators at the school had never received any formal training in de-escalation and anecdotally reported difficulty managing such incidents. This study was approved by the Mount Sinai Institutional Review Board (IRB) (24-00219) and the New York City Department of Education (DOE) IRB (5306-NYC) on June 7, 2024 and October 2, 2024, respectively.
Participants
All student-facing pre-Kindergarten (pre-K) to 5th grade educators at a New York City public elementary school were eligible to participate, including teachers, teaching assistants, and paraprofessional classroom aides. Nearly half of the educators had fewer than three years of teaching experience. Most classrooms have a paraprofessional teaching aide. About one-third of students are English-language learners, and one-third have an Individualized Education Plan (IEP). More specific demographic statistics were excluded to preserve the anonymity of the school. Written consent was obtained from willing participants. Demographic data was not collected from individual participants to protect the identities of this small population of educators, as mandated by the NYC DOE IRB.
Surveys
Participants were recruited to participate in a six-week study that included three pre-intervention surveys, two surveys on the day of intervention, three post-intervention surveys, and a final end-of-study survey (Figure 1). Surveys were distributed via REDCap (15.0.12), with anonymous linking. Pre-and post training confidence surveys on the day of training were distributed on paper. Wilcoxon signed-rank tests were used to assess statistical differences in pre- and post-intervention scores. Flow diagram illustrating study timeline, including various survey distribution points relative to training implementation day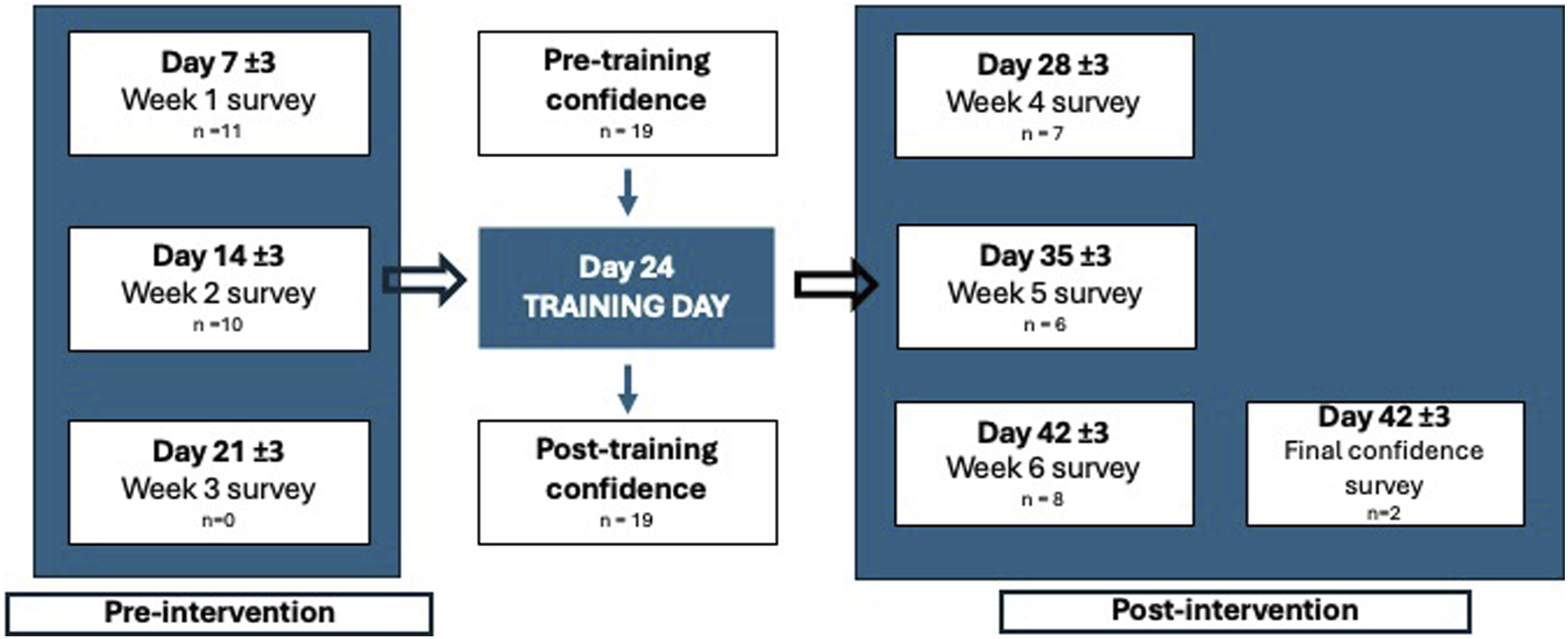
Training Day Surveys
All participants (n = 19) completed a survey right before the delivery of the training and shortly after. These surveys focused on assessing educators’ knowledge on trauma-informed care, DBT-informed strategies, and confidence levels in dealing with emotional outbursts. The post training survey also included questions aimed at assessing the favorability of the training.
Weekly Surveys
Pre- and post-intervention weekly surveys gathered information on the number of emotional outbursts in the classroom per week, the outcome of those incidents (e.g. return to classroom activities vs sending student out of the classroom or home), and the impact of the incidents on the educators’ mental health. An emotional outburst was defined for respondents as incidents (e.g., tantrums or episodes of crying, yelling, or physically aggressive behaviors such as throwing objects or pushing peers) that required the teacher to intervene.
During the six-week study period, each consented participant received one reminder email on Friday to submit the weekly survey. All participants who had not responded by Monday received an additional reminder email. A final reminder email was sent by the middle of the week to non-responders. Figure 1 outlines the number of participants who responded to each weekly survey. The lack of responses during Week 3 (n = 0) was likely due to a school holiday that coincided with the study period.
Intervention
The primary intervention was a 60-min in-person training focused on applying principles of trauma-informed care and DBT in the classroom setting, adapted to the needs of elementary school educators. The training was developed by graduate-level trainees and reviewed by a board-certified child psychiatrist. It was delivered by graduate-level trainees who received orientation on teaching this session prior to implementation. The session followed a structured format to support consistent delivery in future iterations.
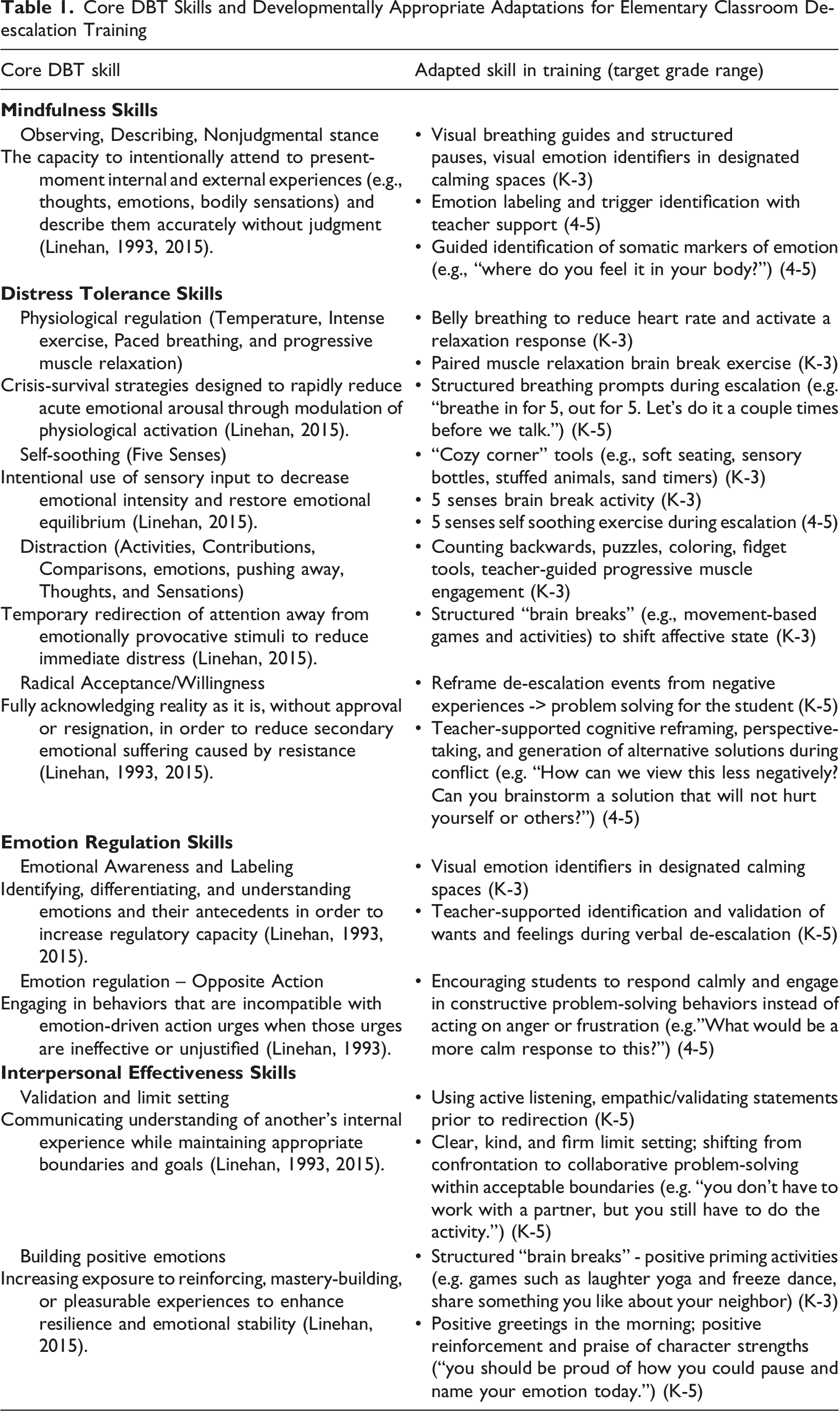
The training began with a case study aimed at introducing the concept of how early adversity impacts childhood development and classroom behavior. Multiple causes of child trauma were discussed through the lens of their subsequent manifestations, specifically within the classroom environment. The training then moved into de-escalation strategies. The first section described general principles emphasizing the importance of modeling regulation, kindness and positivity, and dissuading negative language. The next section focused on classroom-wide activities that could be incorporated into daily routines to create mindful habits that may mitigate emotionally dysregulated incidents in students. This section offered multiple types of “brain breaks” designed to promote positive energy and mindfulness in the classroom, so students can practice these skills while regulated and thus more readily access them during moments of dysregulation. Examples include laughter yoga, progressive muscle relaxation, and belly breathing.
Core DBT Skills and Developmentally Appropriate Adaptations for Elementary Classroom De-escalation Training
Results
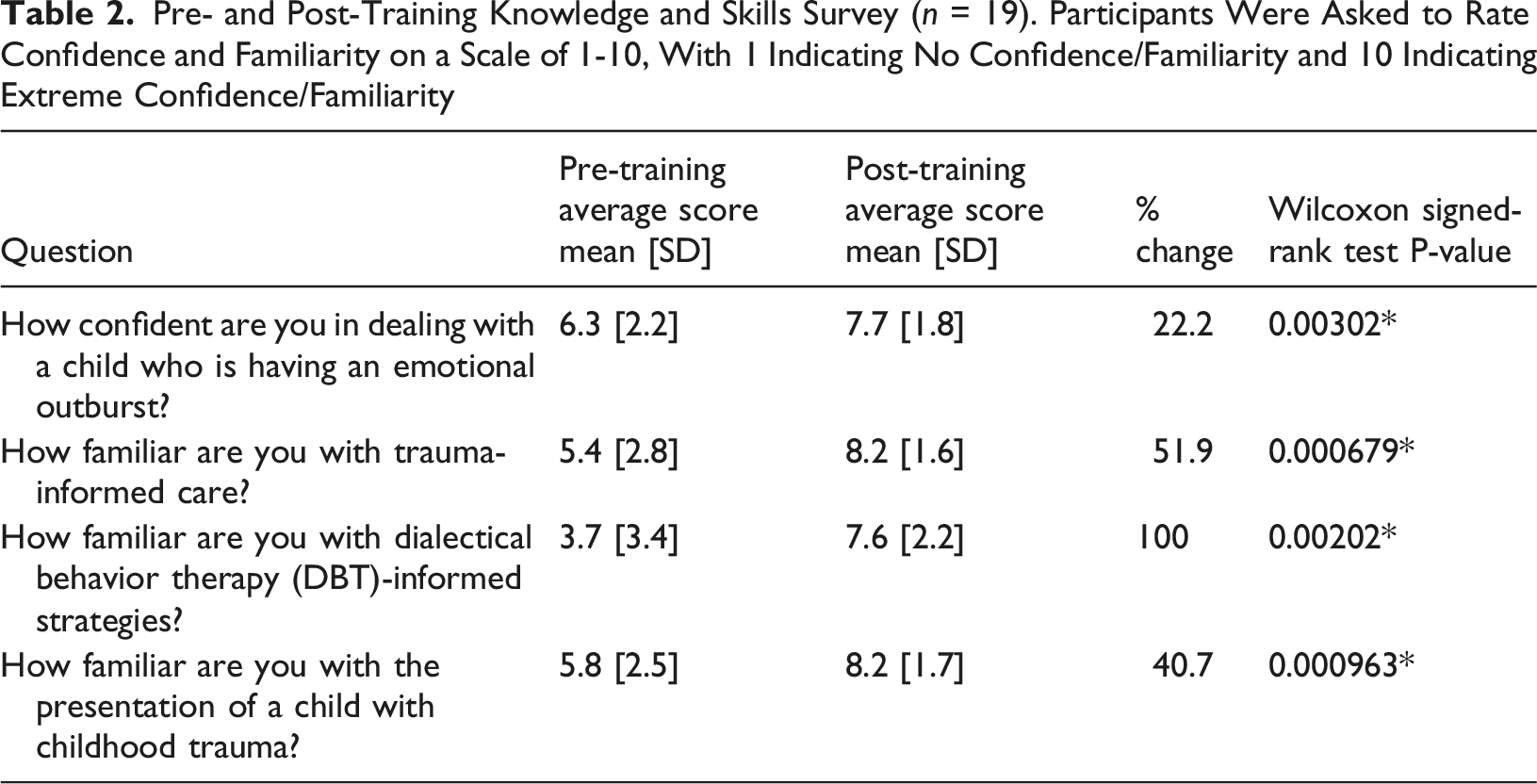
Pre- and Post-Training Knowledge and Skills Survey (n = 19). Participants Were Asked to Rate Confidence and Familiarity on a Scale of 1-10, With 1 Indicating No Confidence/Familiarity and 10 Indicating Extreme Confidence/Familiarity
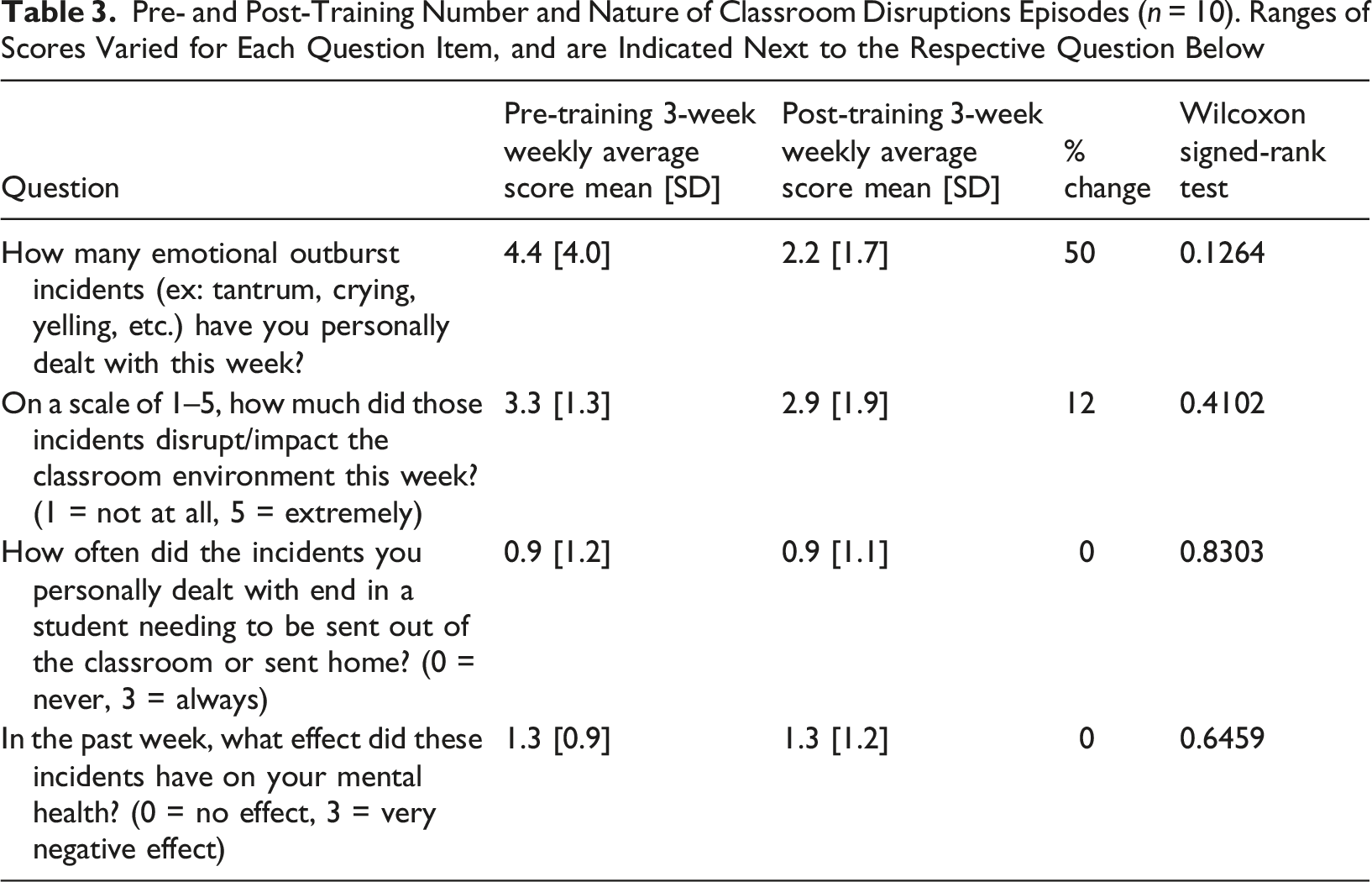
Pre- and Post-Training Number and Nature of Classroom Disruptions Episodes (n = 10). Ranges of Scores Varied for Each Question Item, and are Indicated Next to the Respective Question Below
The pre- and post-training confidence and skills survey found significant improvements in educators’ confidence in helping an emotionally dysregulated student (22% increase), as well as their knowledge of trauma-informed care (52% increase), DBT principles (100% increase), and child trauma presentations (41% increase) after the training (Table 2). Subject-level analysis revealed average increases of 1.4 [SD 1.5] points in confidence in helping an emotionally dysregulated student, 2.8 [SD 2.5] points in knowledge of trauma-informed care, 3.8 [SD 3.4] points in knowledge of DBT principles, and 2.4 [SD 2.1] points in knowledge of child trauma presentations on scales of 1–10.
The aggregate pre- and post-survey data revealed a 50% reduction in the number of emotional dysregulation incidents after the training; however, this difference was not significant (p = 0.126) (Table 3). There was no significant change in the overall average level of classroom disruption caused by dysregulation incidents, the frequency of students being removed from the classroom, or effect on educators’ mental health. Subject-level analysis, including responses from those who completed at least 2 pre-training weekly surveys and 2 post-training weekly surveys (n = 5), demonstrated an average of 34.2% reduction in the number of dysregulation incidents within educators’ classrooms, and a 14.3% reduction in the disruptiveness of incidents within educators’ classrooms. Of total responses, 33% indicated children being sent out ‘often’ or ‘always’ when dysregulated, before training, compared to 25% afterwards. The final study survey did not receive enough responses for analysis, but the two responses received both indicated that the skills taught were able to be applied in classrooms and with dysregulated students.
Most participants (89%) found the training valuable and informative and were likely to recommend the training to other educators (94%). Positive qualitative feedback regarding the training included appreciation for the clearly presented material and inclusion of practice cases with discussion questions. Constructive feedback noted that more time for these practice cases, and including more cases, would be beneficial. A few educators (n = 5) also suggested including videos demonstrating the highlighted de-escalation skills, or time for role-play activities.
Discussion
This was a single-site pilot study to evaluate the effectiveness of a DBT-informed de-escalation training for educators at an urban public elementary school. To our knowledge, this is the first study of its kind to teach and evaluate the teaching of de-escalation skills in an elementary school setting. Our training session was created to address events related to emotional dysregulation in the classroom, such as emotional outbursts, children being sent out of the classroom or home, and classroom disruption. The training was designed specifically for our pilot school’s population, which generally faces heightened emotional sensitivity and dysregulation in the context of unstable home environments, trauma exposure, and early adversity. Before our training, most of the educators at the school had never received any formal training in de-escalating a dysregulated student; therefore, this program sought to fill that gap.
Immediately following our training, there was a 22% increase in educator confidence in de-escalation, as well as 52% increase in knowledge of trauma-informed care, 100% increase in knowledge of DBT principles, and 41% increase in knowledge of childhood trauma presentations. This demonstrates that increased knowledge, administered in a single, 1-h training session, may enable educators to feel better prepared to handle incidents with dysregulated students. This is consistent with another study in a pediatric clinical setting that successfully taught de-escalation skills and increased pediatric residents’ confidence in addressing dysregulation through a 1-time session with case-based discussions (Kronish et al., 2024). Providing new knowledge and allowing for group discussion about student cases allows educators to share their ideas and strategies with each other, growing their de-escalation skills and confidence. This is especially helpful in a population where many participants are new educators with less than three years of experience.
We found a 50% reduction in the number of de-escalated incidents with students after the training; Although a larger sample size is required to demonstrate statistical significance, the reduction is notable and consistent with positive training feedback and reported improvements in confidence and knowledge. This is consistent with existing literature regarding teacher self-efficacy. Increased confidence in educators’ self-perceived ability to manage their classroom is linked to increased frequency of intervention and better student behavior (McLean et al., 2019). This is essential in allowing educators to sustainably de-escalate dysregulated students without removing them from the classroom. The decrease in dysregulation incidents can, in turn, enhance student engagement in the classroom and improve learning outcomes (De Neve et al., 2023). Over time, effectively teaching students how to address their dysregulation will also improve their mental and emotional well-being in the face of adversity and reduce development of future psychiatric conditions.
Moreover, our training included material about integrating ‘brain breaks’ into the school day, particularly exercises that can help students relax and focus on their breathing, or exercises to help them release strong emotions and energy. These breaks also facilitate emotional regulation and impulse control and serve as preventative strategies that can equip even young students with the space and skills needed to avoid becoming dysregulated, thereby supporting improved mental and emotional development throughout childhood (Mazzoli et al., 2021). Explaining the cognitive theory underlying these exercises, as was done in the training, may facilitate their integration into classroom practice. Most educators (n = 18) reported that they planned to implement these breaks in their classrooms, and their adoption may have contributed to the observed decrease in incidents of emotional dysregulation. However, further research is required, as the final study survey assessing the extent to which strategies were ultimately integrated into practice received an insufficient number of responses.
This study was limited by a small sample of educators and high rates of nonresponse, limiting the power of statistical conclusions. A primary reason for attrition is educators potentially feeling overextended in an under-resourced setting. Teachers may have been unable to find time to complete surveys that added to their already overburdened mental load, despite attempts to keep the weekly surveys as short as possible (3 questions). We also could not collect any additional demographics data (due to privacy concerns given the small study population) to learn more about impacts of certain educator characteristics, such as personal identities, years spent teaching, etc. on de-escalation abilities. As a cross-sectional study, we also cannot assume causality or generalizability to other populations. Furthermore, the absence of a control group limited our ability to determine whether observed changes in educator-reported outcomes were attributable to the training itself or to other factors. Nevertheless, the pre-post study design allowed educators and their classrooms to serve as their own controls and control for individual variation. The small study population also enabled us to speak closely with the staff, learn about their needs, and design the training specifically for the challenges they and other educators in similar school districts around the country face. Constructive feedback collected from this pilot cohort of educators will be used to adapt the training for future iterations.
Conclusion
This pilot study demonstrates that a brief, one-time de-escalation training for elementary school educators based on DBT principles is a feasible model that improved educators’ confidence and knowledge in de-escalation. This low-burden intervention is especially useful in low-resourced urban schools with limited infrastructure and capacity for an extended training curriculum for educators or students. This model should continue to be studied in larger samples and expanded to other under-resourced schools. The skills provided to educators may be crucial in aiding vulnerable students to gain important skills in emotional regulation at a critical period in their development and greatly assist teachers who are still early in their education career.
Footnotes
Acknowledgement
The authors have no acknowledgments to declare.
Ethical Considerations
This study was approved by the Mount Sinai Institutional Review Board (IRB) (24-00219) and the New York City Department of Education IRB (5306-NYC) on June 7, 2024 and October 2, 2024, respectively.
Consent to Participate
Participants provided written consent with signatures prior to participation.
Consent for Publication
Not applicable; no participant’s individual data is included in this submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study were collected as part of a small pilot project conducted in a single school. Data may be provided upon request to the corresponding author.