
Abstract
Introduction
Children’s services are struggling to meet increasing demand for neurodevelopmental (ND) assessment and support. Early identification enhances the appropriate delivery of services tailored to meet the needs of children and families. In the face of increased waiting lists, the integration of digital tools may improve efficiency, but only if they are acceptable to the people using them.
Methods
We qualitatively explored the views of parents/carers of neurodivergent children about the potential introduction of digital assessment tools and related data governance. All had lived experience of navigating ND assessment services with their child.
Results
Participants’ experience of the assessment process was of fragmented service delivery, and they welcomed the possibility of a holistic, streamlined approach. Most participants trusted the NHS to keep their information safe but sought greater transparency and sensitivity, about both digital and non-digital data. The introduction of digital tools was welcomed, but participants highlighted accessibility considerations.
Conclusion
Parents and carers are open to the use of digital tools to support child ND assessment, but to be effective they must be safe, accessible and inclusive. They valued the prospect of a holistic efficient approach to understanding neurodivergence.
Plain Language Summary
The NHS has been criticised for being slow to introduce new ways of working such as online questionnaires. Services for neurodivergent children have very long waiting lists. They often only consider one aspect of neurodiversity at a time, for example autism but not ADHD. These problems often co-exist. This research is important as new ways of working might lead to children’s needs being identified earlier and them getting better support. Getting parents and carers views about this could lead to positive changes in the NHS. We wanted to know what parents and carers thought about filling in questionnaires online. We also wanted to know if they thought their details and the information they put in would be kept securely. We told them about a new online questionnaire tool which asks about all areas of development. We interviewed people who volunteered to take part, either on their own or in groups of 2 or 3. They were given our questions in advance. We recorded these interviews and then looked at the written accounts to see what themes could be identified. This sort of analysis is good for projects which involve small numbers and are finding out about people’s views or opinions. The people we asked to take part were parents or carers of neurodivergent children whose child had been referred to health services for assessment. Some worked at charities offering support, others volunteered or attended for support themselves. They told us that they had found the assessment process stressful and fragmented. They welcomed the possibility of a holistic, streamlined approach. Most participants trusted the NHS to keep their information safe but wanted more information about what happened to it. They were worried that not everyone would find this easy or be able to access the questionnaire.
Keywords
Introduction
Neurodivergent children and their families can benefit from early assessment, which supports earlier access to health, educational support and social care tailored to their needs (Guillon et al., 2022). We use the term neurodivergent to refer holistically to areas of difference as described within diagnostic frameworks; it includes, autism, attention-deficit/hyperactivity disorder, (ADHD), developmental language disorder, developmental coordination disorder, intellectual disability, and tics/Tourette’s syndrome. A thorough neurodevelopmental (ND) assessment can aid the understanding of the child’s strengths and identify areas where extra support may be required. Yet children’s services in the UK, and internationally, have faced growing demands for ND assessment and support (Lang et al., 2024), and waiting times have rapidly increased. One proposed solution to streamline assessments, while better supporting families, is the integration of digital tools into ND assessment pathways. There is some evidence to suggest that digital tools, generally, may improve access (Istepanian & AlAnzi, 2020), provide time-efficient screening (Adiani et al., 2019) and reduce stigma, by enabling families to input information privately or remotely (Halldorsson et al., 2021; Tuijnman et al., 2019). Specific to ND assessment, some evidence suggests that digital tools may offer an objective approach to support earlier identification of neurodivergence (Mukherjee et al., 2024). However, much of the digital health research focuses on autism or ADHD only (Boulton et al., 2025), missing out the occurrence or crucially the co-occurrence of other forms of neurodivergence (Gillberg, 2010). If digital tools are to be both efficient and effective, then they must address the longstanding problem of single diagnostic silo-ed pathways, which likely exacerbate waiting times and leave families feeling passed from pillar to post.
There are only two neurodevelopmentally related digital tools, to the best of our knowledge, which support clinicians to gather parent information holistically i.e. questions relate to all areas of neurodivergence, on one platform. These are the Development and Wellbeing Assessment (DAWBA) (Ford et al., 2013) and the ESSENCE-D (Landberg et al., 2025). The DAWBA can be used to support decision-making around neurodevelopmental and mental health diagnoses, and the ESSENCE-D has been developed from the principles of the ESSENCE (Early Symptomatic Syndromes Eliciting Neurodevelopmental Clinical Examinations) framework (Gillberg, 2010). ESSENCE emphasises that in neurodivergence co-occurrence is the norm, but also that parents’ observations and concerns should be central to early identification. Parents are often the first to notice neurodevelopmental differences, yet their perspectives are not always prioritised within assessment processes. When parents’ voices are sidelined, opportunities for timely recognition and support can be missed (Boshoff et al., 2018). A shift toward holistic assessment models has the potential to reflect the lived realities of families and provide earlier, more coordinated support.
Nevertheless, other practical challenges need to be addressed when considering use of digital tools as part of a child’s assessment. First, families have raised concerns about how sensitive data is stored and used (Rivera-Vargas, Calderón-Garrido, Jacovkis, & Parcerisa, 2024). Little attention has been paid to how parents feel about the collection and management of their children’s assessment data, particularly when the children are too young to give informed consent themselves. Second, validation, usability and generalisability remain limited. Some digital tools are tested only on narrow populations and do not consider co-occurring developmental, or environmental factors including poverty awareness and language barriers, reducing their generalisability and applicability across diverse families and settings (Adiani et al., 2019; Mukherjee et al., 2024; Ruta et al., 2017). Additionally, neurodivergence is reported to be under-recognised in minority ethnic groups (Burke, 2015), yet most assessment tools are written in English and rarely account for cultural or linguistic diversity (Bernier, 2010). There is a distinct lack of feasibility or user experience perspectives in the research literature. Third, Lord Darzi, in his independent investigation into health services in NHS England reported that institutions like the NHS are “behind the technological curve, (Darzi, 2024).” The introduction of new technologies to NHS services can be difficult and time consuming, with costs, information governance, service user outcomes and equality being cited as potential risks (NICE, 2024). However, it is less clear how the NHS is considering the voice of the users, and importantly, what matters most to them in the context of the cost-benefits of digital tool use.
Previous research has considered families’ views on “personal data privacy, security, access, control and (dis-)empowerment” (Bowyer et al., 2018) and “experiences of providing consent to share personal information” in the context of a digital health data system (Smart et al., 2022). These studies emphasised the importance of the relational and social contexts in which information-sharing takes place, with both parent-professional and interprofessional relationships being key. Bowyer et al. (2018) conclude that “organizations must support a dynamic consent model of data handling, and plan for a new paradigm of co-operative, data-based relationships with families.” Furthermore, some research has also called for the inclusion of informants and stakeholders to be involved in the digital tool design process (Bevan et al., 2020; Brett et al., 2014). In the context of ND assessments, the perspectives of the informants, the parents and caregivers who answer clinicians’ questions on behalf of their children, is missing from the literature. Implementation challenges may act as barriers to research progression and crucially, any possible benefits to families. By understanding what matters to families regarding data security, information governance and usability, we can start to address these practical issues, so that any near future use of digital tools in ND assessments is better informed.
The recent NHS England (2025) guidance for use of digital technologies in mental health (inpatients) outlined eight important principles which should inform procurement, implementation and use. These include a human rights approach, based on consent, equity of access, informed by evidence and co-production. With these principles in mind, the focus of this study was to explore the views of parents/carers with lived experience of navigating ND assessment services about digital tool use and related data governance.
Aim
Our primary aim was to explore the views of parents/carers regarding possible use of digital tools as part of a child’s ND assessment, and to foster discussion about data governance, data protection and privacy. We proposed three questions: (1) What experience have participants had of using digital technologies, generally and in healthcare contexts? (2) What are their views about the possible future use of digital tools as part of a child’s ND assessment? (3) What are their views about the digital recording and storing of information, including related data governance, data protection and privacy?
Method
We chose a qualitative research methodology to explore the views of those with lived experience of navigating current NHS ND assessment pathways. Participants were parents of neurodivergent children, who had been assessed and diagnosed with one or more neurodevelopmental difference or were on a waiting list for assessment.
Recruitment
Once university research ethics approval was obtained, we contacted two local third sector organisations to invite parents of neurodivergent children to take part.
Semi-Structured Interviews
We adopted Cote and Raz’s (2015) approach to semi structured in-depth interviews incorporating Eklund’s (2015) approach to focus group methodology. Stem and follow-up questions were developed and shared with participants prior to interview in order to provide a consistent structure (see Appendix). We chose a research method that was sensitive to participants’ stories and offered a space to openly discuss their experiences.
Procedure
Participants were interviewed and audio-recorded either in person at an agreed location or over Teams video communication software. All participants provided informed consent beforehand. Interviews were conducted jointly by two members of the research team with different professional and personal backgrounds. This supported broad enquiry and sought to ensure that all relevant information was included. Interviewers were male and female in 10 cases and both female in 3.
Participants were first asked a few icebreakers (“how many children, how old are they?”) to set a more relaxed environment before being invited to talk about their experience of the ND assessment process with their children. In focus groups, time was given for each participant to discuss their experience, and this often led to discussion between participants about their differing experiences.
In keeping with our primary aim, our main questions focused on their experience of using digital tools and their views about data security. We then delivered a short PowerPoint presentation representing the potential use of a digital tool called ESSENCE-D (Landberg et al., 2025), (see Figure 1). ESSENCE-D Parent Dashboard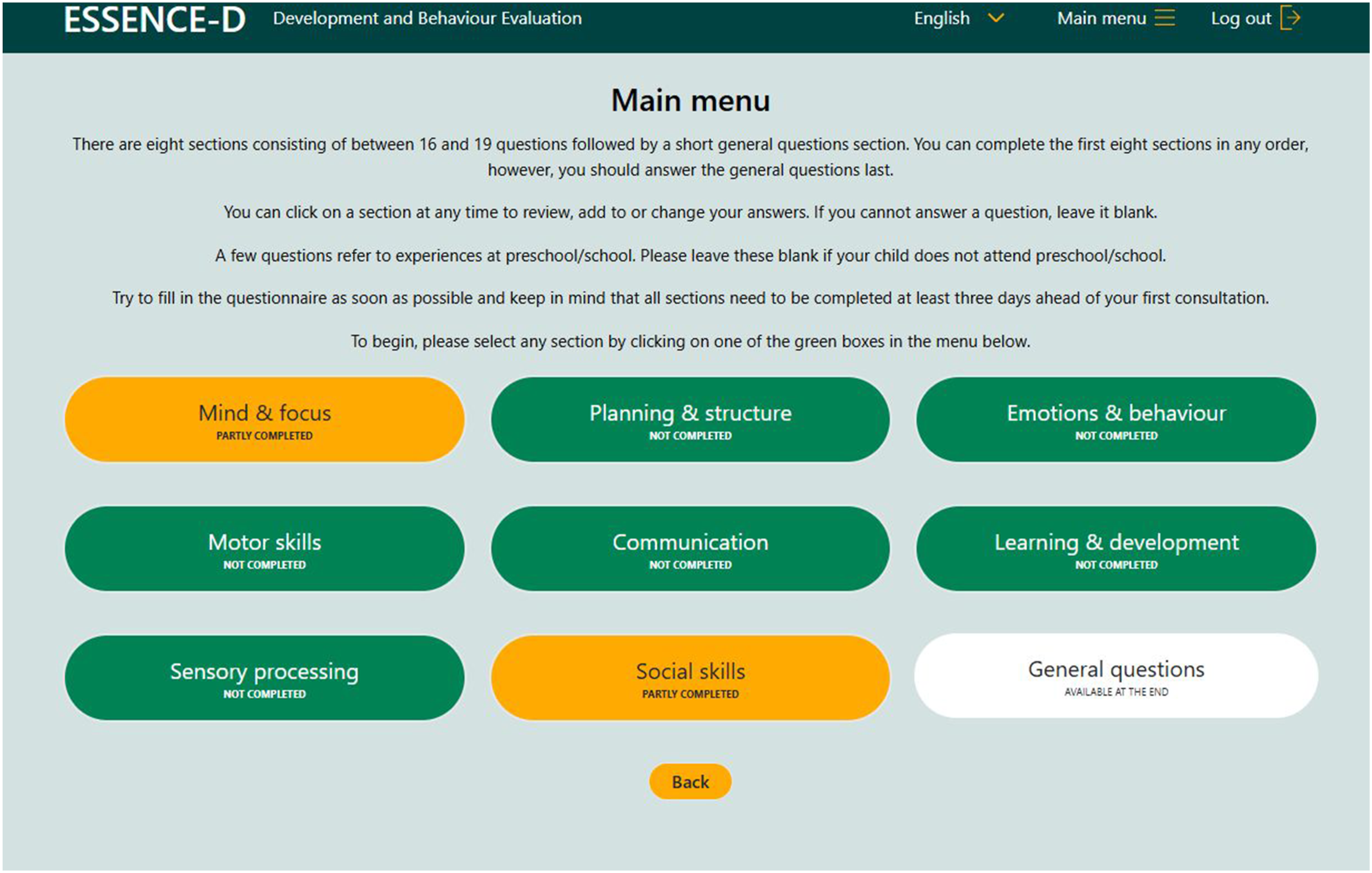
ESSENCE-D Is a browser-based digital questionnaire. It features a parent facing side which present needs-led questions regarding all areas of child development (social skills, language, sensory processing, motor coordination etc). The algorithm calculates the proportion of positive scores per question and then groups them graphically for the clinician to view under diagnostic categories such as autism, ADHD, language disorder, intellectual disability etc (clinician-facing only). It is not a diagnostic tool. It is designed to be used as an aid to holistic information gathering with clinician judgement always taking precedence. ESSENCE-D was selected for this study because of its holistic neurodevelopmental focus, without the additional mental health component offered by the DAWBA, which was less appropriate for this context.
In practice, ESSENCE-D could support clinicians by (a) providing a holistic overview of the child’s needs on one platform, without repeated questionnaires, (b) showing co-occurrence of neurodivergence and (c) identifying which clinicians need to be involved more efficiently and earlier, and therefore giving the child a more joined-up experience of the multi-disciplinary care pathway.
The researchers have not been involved in the development of ESSENCE-D but are exploring NHS clinicians’ experiences of using ESSENCE-D in a separate feasibility study.
Data Analysis
Reflexive thematic analysis was used to analyse the data (Braun & Clarke, 2021). This method considers the researchers’ worldview and background, contextualising the findings based on researcher interpretation and experience and offers transparency regarding how our backgrounds shaped the analysis.
Transcripts were anonymised and screened by each interviewer independently, noting initial codes and identifying connections between them. When everyone had completed this process with the first few transcripts, the researchers met to compare codes. The researchers reflected upon their positionality, which in some cases was evident in the different emphasis given to the patterns identified. To give one example, the first author highlighted the clinical challenges and barriers experienced in the service pathway, while the second author identified more practical challenges related to data management. Nonetheless there was agreement among all the interviewers regarding the emerging themes. We refined and organised these into core themes and sub-themes, noting links and hierarchical connections between them. Themes were continually discussed and iterated upon throughout the analysis. Some sub-themes were later merged into core themes, as we observed overarching similarities.
Positionality Statements
First Author
I worked for over 30 years as a child and adolescent psychiatrist often assessing and treating children as part of an ND team. My younger son is neurodivergent and has had many difficulties reflecting this throughout his life.
Second Author
I have a background in computer science and a focus on design-based research methodologies. I have been working in the role of applied games for 6 years, and a total of 10 years within a computer science/human-computer interaction discipline.
Third Author
I am a digital designer with research interests in digital wellbeing, neuro-inclusive design practices, and data equality. My family are neurodivergent; I have lived experience of the assessment process as a parent.
Senior Author
I am the Principal Investigator. My research interests are neurodivergence and maltreatment-associated presentations. I am also a Speech and Language Therapist, working in a neurodevelopmental assessment team for a child and adolescent mental health service.
Results
Participants
Thirteen mothers of twenty-five neurodivergent children took part. Participants comprised a mixture of staff and volunteers who were parents to ND children and parent-clients attending the services who had ND children. Participants were predominantly white British women. Despite efforts to recruit broadly, no male participants volunteered. Two participants were non-native English speakers. Although we did not ask explicitly about parents’ own neurodivergence, three participants self-identified as neurodivergent.
Participants talked about diagnosis and appeared to value its purpose. Children had a range of diagnoses and notably had received these between 1 and 23 years after concerns were first described.
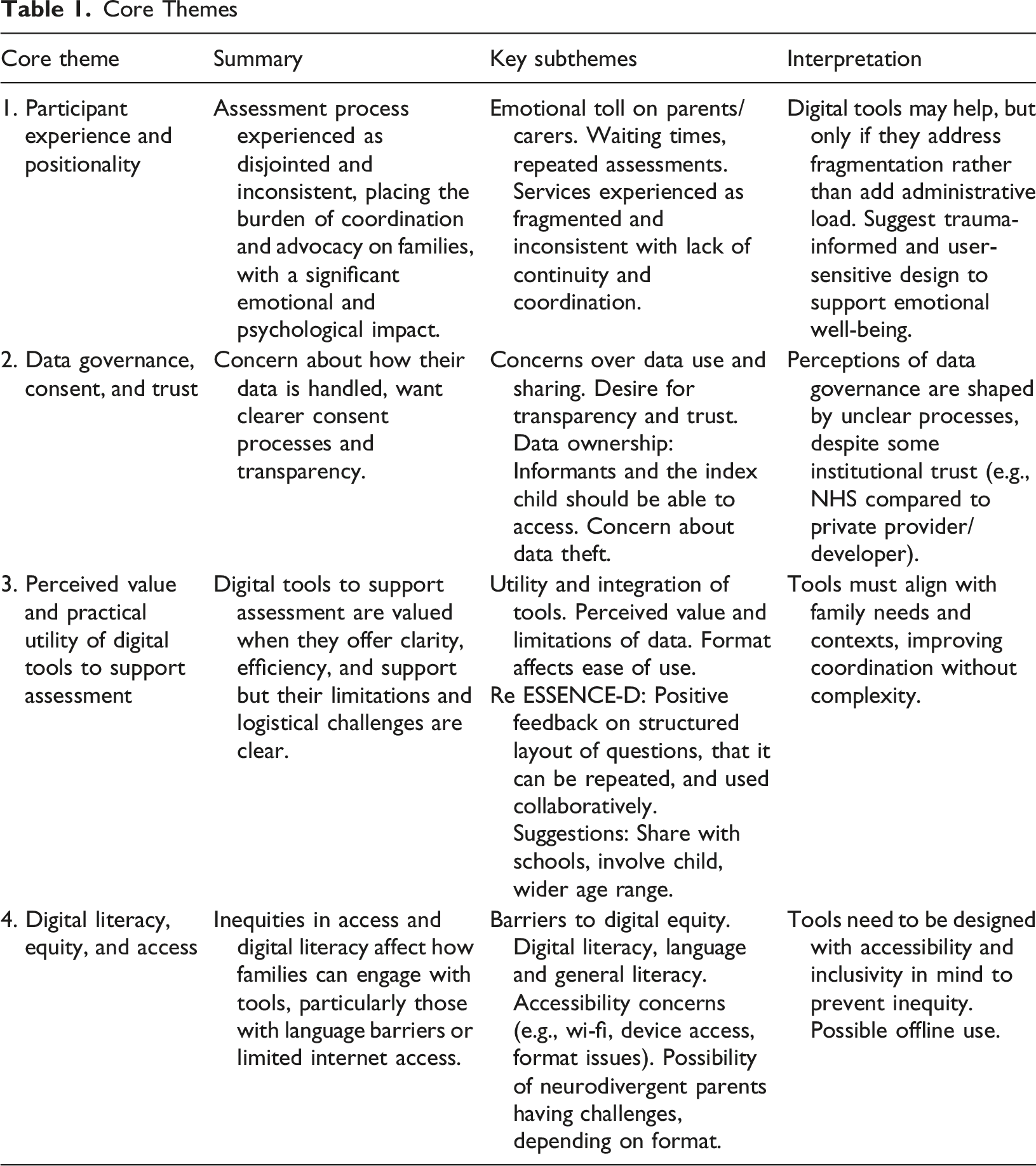
Core Themes
Core Themes
Participant Experience and Positionality
Participants’ experience of services was not the primary focus of our inquiry. However, in the process of engaging with participants, it felt important to hear and record their experience of the ND pathway as a contextual background. Participants consistently described assessment pathways as fragmented and incoherent, with little coordination between services. They reported referrals to different specialists, e.g. speech and language, autism or ADHD teams, without a clear sense of how these linked together. Children were often placed on multiple waiting lists simultaneously. The lack of integration left many needs unidentified and created a sense of being “passed about” with a perception that there was no clear ownership of responsibility for assessment. They spoke of repeatedly telling their child’s story to different professionals and keeping detailed logs to ensure continuity where services failed to communicate.
Parents and carers described feeling vulnerable, judged, and unsupported as they navigated the system. Assessments were often experienced as emotionally taxing, with questioning, for some, feeling like an “interrogation.” Some participants doubted their parenting and others felt exposed by a lack of sensitivity or explanation. The absence of clear preparation or forewarning about the process intensified distress, with many participants stating they were “totally unprepared.” Participants discussed how the experience impacted their mental health, while others spoke of the strain it placed on family relationships and the feeling that they had to advocate for their child alone. This “regurgitation” of information was described as exhausting and often left them feeling isolated. Yet, for the majority of those whose child did eventually receive a diagnosis, the support offered was experienced as appropriate and much needed, with only a minority remaining concerned that their child’s needs would remain unmet as they progressed through school.
Data Governance, Consent and Trust
Most participants used smart phones and/or other digital devices, with some regularly using social media platforms. In this context they were aware of the potential for their data to be mined or stolen and opportunities to be caught up in scamming activities.
However, participants generally expressed trust in the NHS to safeguard their data. This appeared to be linked to a perception of health professionals, e.g. health visitors and doctors, as knowledgeable and supportive. Some parents and carers stated explicitly that they were “not worried about information security”, indicating strong confidence in public services.
However, many also described a lack of clarity about what they had consented to during their child’s neurodevelopmental assessment, almost all of which did not include use of digital tools. This was particularly evident for the parents for whom English was not a first language, who reported difficulty understanding the content and implications of forms and questionnaires. Several participants questioned whether they had truly grasped what they had “signed away,” in fast, short appointments. They described a lack of transparency and communication regarding how personal and sensitive data was handled during the ND assessment process. Families described an assumption that the “NHS was confidential”, [and] “assumed data was kept secure”. In some cases, data had gone missing leaving them asking “where did that go?” In a few cases, consent was described as formally requested, for example, to share information with the Education Authority. More often, consent appeared informal and lacking in detail: “It was just, like, ‘are you okay with us sending this copy to whoever?’” Such exchanges left some parents feeling uncertain about the implications of their agreement. Over half wanted to know from the outset exactly how their data would be used, who would have access to it, and where it would be stored. The sensitive nature of the information which related to their child sparked concerns about its long-term implications: “What if this affects their future, like a job?”
Parents’ reflections regarding data security and consent currently, enabled deeper reflection regarding the possible use of digital tools in a child’s neurodevelopmental assessment and related governance. Views were mixed. Some participants believed that digital data was more secure than paper records, citing password protection and encryption. Several admitted to not being overly concerned regarding digital data if the NHS used their data appropriately, i.e. confidentially, securely stored and seen only by those who needed to see it. When they heard that private third-party partners were often involved in developing digital tools and data storage, some expressed concern. They voiced fears about sensitive data being sold, mishandled, or exposed through cyber-attacks. The perceived safety of digital platforms appeared linked to digital literacy. Participants were concerned that families who were less confident with technology or lacked reliable access to Wi-Fi, laptops, or mobile devices might face more significant challenges, including understanding the implications of digital data collection.
Participants acknowledged that their primary focus was getting help for their child, which often overshadowed immediate concerns about data governance. However, this did not diminish their expectations for ethical standards. They wanted professionals to treat sensitive information with care, maintain clear boundaries around access and use, and provide greater transparency about what data is collected and why, regardless of whether data was collected digitally or not.
Perceived Value and Practical Utility of Digital Tools to Support Assessment
Parents welcomed the ESSENCE -D tool’s capacity to capture co-occurring difficulties and present a “broader view” of the child’s needs. One parent appreciated how a clinician could “hit a few markers for something else as well,” avoiding the scenario where a family must “start again on the next one” for each potential different neurodevelopmental diagnosis.
Participants valued the possibility of completing assessments flexibly, for example, logging on a mobile device and completing separate sections, when convenient, was seen as helpful when juggling childcare. They also felt it allowed them to document observations “in the moment” by logging on and recording when something was in their mind.
For many, digital tools were seen to ease the emotional intensity of assessments. They felt this would support them to “take as much time as you want” and better process emotionally difficult or complex questions. Several parents contrasted this with their experience of interviews, noting that written formats felt “less intrusive,” easier to manage emotionally and reduced that sense of being judged in face-to-face encounters.
Two participants suggested that digital tools could provide a means of communication and feedback between parents and clinicians. They anticipated a digital tool might be able to send reminders about where they were in the assessment process, confirming that they were still on the service’s “radar”.
Many parents wanted a copy of their responses; this being seen as a way of supporting a feeling of being “in control”. It was noted that keeping track of paper copies was difficult and a digital record which they were able to keep might help. Self-documentation was recurringly noted by many participants who kept “logs” of their child’s behaviours to avoid forgetting important details. Some suggested that having a dedicated section to record specific observations would be a “highly beneficial” development and expressed enthusiasm for the idea that a digital tool could support and centralise this work, despite the fact the ESSENCE-D tool demonstrated did not offer that. Others reported that they found open-ended unstructured questions difficult so this development may not have been welcomed by all.
Digital tools appeared to be valued not only for their practical efficiencies, but also to support earlier intervention, and reduce the burden on families of navigating complex, fragmented systems. In this context, digital tools were seen as a way to “streamline” and “process patients and children as quickly as possible.” The ability to have “everything in one place” was especially valued.
Digital Literacy, Equity, and Access
Most participants thought that inequities in digital access and literacy might significantly constrain families’ ability to engage with digital tools during the ND assessment process. This introduced a conflict for participants; while digital formats were mostly welcomed as a way to streamline data sharing and to provide a more holistic picture, there was a notion that the digital tool might not be wholly accessible. Participants were concerned that families who were less confident with technology or lacked reliable access to Wi-Fi, laptops, or mobile devices might face significant challenges in using these tools effectively and understanding the implications of digital data collection. The absence of connectivity was also a concern for those families from rural areas. Participants wondered if offline completion could be supported. Without due consideration digital tools could introduce new barriers, which could compound existing inequities.
Three participants reflected on how easily they could log in and fill out forms online, but acknowledged this was not the case for many neurodivergent parent/carers whom they supported. They felt that a parent’s own neurodivergence might affect how they engaged with standardised digital forms. Yet, different participants noted that the structured Likert scale format of the questions, offered within ESSENCE-D, was of benefit for neurodivergent individuals. For any tool, user-friendly, neuro-diverse design is clearly an important consideration. Concerns also surfaced around digital literacy and understanding of consent about data storage. “But do they really understand what they're saying?” reflecting a wider anxiety about informed consent and the invisibility of data storage and handling practices.
For parents whose first language was not English, digital interfaces could feel exclusionary and unmanageable. One such participant shared that when completing paper questionnaires, they required support from another person “It’s easier when someone is reading slowly and explaining the sentences.” One parent recalled how their health visitor had to help them fill out a paper questionnaire because they “didn’t know how to do it.”
Such challenges raise questions as to the possible accommodations required for a tool like ESSENCE-D which has many questions and is designed to be completed at home.
Other participants suggested that such digital tools might be more helpful as they could be completed collectively, allowing input from multiple family members: “You know, the husband, the grandma, siblings—they all notice different things.” The ESSENCE-D presentation had highlighted this possibility.
Without consideration of language diversity, neurodivergence, and digital accessibility and literacy, digital tools could add additional challenges for users. Hands-on support for whatever reason was highly valued by participants, for completion of paper questionnaires, and in the future for digital ones. Overall, while there was recognition that digital tools, such as ESSENCE-D or other digital technologies, could offer efficiencies but there were concerns about equity, usability, and trust.
The Reflective Process
A key principle of reflexive thematic analysis (RTA) is acknowledging “How did I shape what I observed?” Our positionality as researchers may have influenced our assumptions as we familiarised ourselves with the data and began our analysis. Through the lens of RTA, we did not attempt to match participant experience with researcher experience, but instead we collectively reflected upon our findings, and identified four main influences which may have shaped the analysis and interpretation of data. First, two of the researchers had personal experience of the ND assessment pathway. This may have led them to follow up on participants’ account of the emotional aspects of their assessment journey. Second, those with clinical experience may have inadvertently been more focused on the presentation of neurodiversity than participants’ experience of digital tools. Third, participants became more invested in data security once we had raised the issue of potential risks and concerns. Finally, three of the researchers are women as were all the participants. We acknowledged the gendered perspective that female researchers and participants might bring to the discussion as women are largely responsible for caregiving in Western society. We also considered their status in terms of gender, race, ethnicity and neurodivergence.
Shared reflection and the examination of different perspectives brought a valuable lens to the analysis of qualitative data, ensuring that our interpretation could be seen as robust and replicable.
Discussion
We set out to explore the views of parents/carers with lived experience about the introduction of digital tools in ND assessment. Our aim was to identify perceived benefits and challenges, particularly in relation to data security and governance.
Participants were women, perhaps reflecting societal expectations, but also the reality of family life in the UK, where mothers/female carers are more likely to be the family members who support offspring and seek healthcare for them when required.
Current Pathways
Participants’ views were informed by their own lived and living experience as parents of neurodivergent children, having navigated their local ND assessment pathway. Consistent with previous research (Guillon et al., 2022; Nilses et al., 2019; Tait et al., 2016), participants described ND assessment as fragmented, protracted, and emotionally taxing. These findings reinforce prior work highlighting the psychological toll of ND assessment on families (Abbott et al., 2013; Rutherford et al., 2021)
The Potential of Digital Tools to help
Participants expressed optimism about the potential of digital tools to improve the assessment process. Digital tools were also valued for their capacity to give parents a voice. Completing questionnaires in their own time, outside of what they experienced as pressurised encounters with clinicians, was seen as less intrusive and allowed them to reflect before responding. Several noted that digital platforms could ease the emotional intensity experienced in face-to-face assessments, particularly where they felt judged by professionals. Features that allowed for documentation of day-to-day observations, retention of copies of responses, and progress updates (e.g. reminders of waiting list status) were strongly desired. These align with broader arguments that digital technologies can enhance agency, reduce stigma, and improve communication between families and clinicians (Halldorsson et al., 2021; Tuijnman et al., 2019)
Participants were clear that digital tools must address, rather than replicate, the fragmentation of service delivery. Without integration across departments and professionals, digital tools risk adding burden rather than alleviating it. This echoes critiques that many current digital tools are siloed and target single neurotypes overlooking the co-occurrence that characterises most ND presentations (Boulton et al., 2025; Mukherjee et al., 2024). As Gillberg (2010) argues, listening to parents’ concerns and adopting a holistic orientation to assessment are essential to facilitate earlier and more effective support. The demonstration of ESSENCE-D was generally well-received, with parents valuing its efficiency and capacity to capture a broader picture of their child’s needs. Many described the appeal of a system that could hold “everything in one place,” was accessible across services and reduced the need for repeated storytelling. Such features align with calls to streamline ND pathways and reduce duplication of effort (Ford et al., 2013; Thomson et al., 2025). However, the readiness of clinical services to adopt a holistic approach (Lang et al., 2024) and for NHS systems to embrace available digital technology (Darzi, 2024) is an area requiring further investigation. Our findings support wider calls for public health providers to engage with research and collaborate more with those with lived experience, grounding decisions about service delivery in user experience.
Designing With Accessibility and Inclusivity in Mind
A recurring theme was the importance of accessibility and inclusivity in digital design. While most in our sample were comfortable with technology, concerns were raised about families with limited digital literacy, poor internet connectivity, or lack of access to devices. These concerns echo broader literature on the “digital divide” in health care (Istepanian & AlAnzi, 2020).
Language was another barrier. The two non-native English speakers and one other participant described requiring support from others to interpret and complete forms. Literacy was also seen as important. For digital tools to be equitable, they should accommodate linguistic diversity, for example by offering translations, simplified language options, or audio support. Most assessment tools are written in English and rarely account for cultural or linguistic diversity (Bernier, 2010). This is important as neurodivergence is reported to be under-recognised in minority ethnic groups (Burke, 2015). Barriers may also extend to clinical language. Prior research shows that medicalised terminology can alienate parents (Jones et al., 2020; Nissenbaum et al., 2002). This could be particularly important as participants highlighted that many parents may be neurodivergent. They shared that, sometimes, communication differences can affect how questions are interpreted and how tools are used, highlighting the need for flexibility and sensitivity in design. Digital tools that adopt plain language, explain the purpose of sensitive questions, and provide feedback may improve engagement.
These findings reinforce calls for involvement of those with lived experience in the design of digital technologies to ensure usability across diverse populations (Bevan et al., 2020; Halldorsson et al., 2021). Furthermore, indirect benefits of co-production include service users feeling empowered and valued, and researchers/developers developing a greater understanding and insight in the area (Brett et al., 2014; Saiger et al., 2023).
Digital Data Governance
Although participants generally prioritised accessing support over questioning data governance processes, most assumed that their data was stored safely by public health services. Most participants were unaware of the storing of data by third-party partners when using digital technologies, and when this was highlighted, it raised additional concerns. These findings resonate with recent critiques about transparency in digital health (Rivera-Vargas et al., 2024) and suggest that data governance is not only a technical issue but also a relational one, tied to trust, communication, and perceived respect for families’ contributions (Bowyer et al., 2018; Smart et al., 2022).
At a minimum, participants expected clear explanations of how data is stored, who would have access, and for what purposes. Some wanted copies of their child’s assessment data, which they saw as empowering and as a safeguard against information loss, considering digital tools as an easier way for them to store their child’s records.
If public health services are to embrace digital innovations to better understand and inform children’s neurodevelopmental assessments, then governance teams must also listen to what families want and need regarding ethical data processing. Currently, stringent data protection laws, many of which limit or inhibit access to health information and dictate how/what information is shared across different services, pose significant barriers to the collaborative and transparent system that parents are asking for (Palfreyman & Morton, 2022). Furthermore, the 2020 national audit (National Audit Office, 2020) demonstrated that siloed and fragmented governance services also create barriers to the efficiency and effectiveness of digital innovations within the national health sector. Until such problems are directly addressed, some of the challenges raised by our participants may persist and the perceived benefits of digital tools for ND assessment will not be offered, despite the ever-increasing need (Lang et al., 2024).
Designing Tools to Align With Family Needs
Overall, our findings suggest that digital tools can play a meaningful role in ND assessment if designed to align with family needs. This requires moving beyond tools that prioritise clinical efficiency alone. Participants in this study valued tools that: • • • • •
These preferences suggest that digital tools could help to build trust, streamline pathways, and give families agency. Such design principles align with participatory and co-design approaches, which have been shown to improve usability, uptake, and long-term sustainability of health technologies (Boulton et al., 2025; Brett et al., 2014; Halldorsson et al., 2021).
Recommendations
We propose the following recommendations for researchers, developers and clinicians working towards better ways of delivering ND assessment: (1) Digital or paper forms should always be complemented by clinician-facilitated conversations to explore areas of uncertainty and ensure shared understanding. (2) Future digital developments should adopt holistic approaches. Tools such as ESSENCE-D, which capture presenting symptoms across the range of neurodivergence are better aligned with families’ experiences than single-neurotype tools. (3) Prioritise accessibility and inclusivity. Design of digital tools should consider linguistic diversity, neurocognitive differences, and digital inequalities. Where possible, tools should offer multi-language support and flexible formats. In-person support to input information should be offered where required. (4) Ensure transparency in data governance. Families should be clearly informed about how their child’s data is stored, who has access, and how it will be used, with options for parents to access their own records. (5) Integrate tools into coordinated pathways. Digital tools will only be effective if embedded in streamlined, collaborative systems that reduce fragmentation rather than adding to it.
Limitations
There was a gender imbalance in this study, with all participants and 3 out of 4 researchers being women. Despite efforts to recruit broadly, no male carers participated. This absence may reflect gendered dynamics in caregiving roles, or possible reluctance among male carers to engage with discussions about their children’s neurodevelopment. Exploring fathers’ perspectives is an important direction for future research.
The participants were recruited via third sector support organisations and included staff and volunteers as well as those receiving support. This may have led to them being more empowered to voice their views. Further, participants may have shared experiences or perspectives not reflective of all families navigating ND assessment. Moreover, participants were geographically concentrated and may have accessed services within the same locality, limiting the generalisability of findings.
Finally, the ESSENCE-D platform was selected for discussion because of its holistic orientation but is currently undergoing feasibility testing with UK ND services and being used in an international randomised control trial (see Appendix). Participants’ responses therefore reflect hypothetical engagement with the tool rather than real-world use. Longitudinal studies are needed to evaluate how families and clinicians engage with digital tools in practice, including consideration of their impact on access, efficiency, emotional burden, and family wellbeing.
Conclusion
Our findings highlight three central conclusions. First, parents’ experiences of ND assessment are characterised by distress, fragmentation, and uncertainty. Second, our participants view digital tools positively when they offer holistic, streamlined, and accessible support, but remain wary of tools that reinforce silos or inequities. Third, while parents trust public services, they desire far greater transparency and communication about how sensitive data is managed.
We recommend that developers of digital tools consider inclusive, accessible and holistic approaches and provide flexible formats for diverse end-users. The effectiveness of digital tool use in ND assessment will depend on clear data governance and integration into existing pathways that promote collaboration and reduce service fragmentation.
Footnotes
Acknowledgements
Thanks to participants and to the third sector organisations that supported recruitment.
Ethical Considerations
The research proposal received approval from the University of Glasgow Research Ethics Committee in March 2025 – see below.
Consent to Participate
Informed consent to participate was obtained in writing and witnessed.
Consent for Publication
Informed consent to publish our findings was obtained in writing and witnessed.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Office for Life Sciences and the National Institute for Health and Care Research (NIHR) Mental Health Translational Research Collaboration Mission, hosted by the NIHR Oxford Health Biomedical Research Centre.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Exploring Parents’ and Carers’ Views about the use of Digital Tools in Neurodevelopmental Assessment.
Data Availability Statement
Anonymised data is available in OSF repository which can be accessed by readers.
Author Biographies
Appendix
*OSF repository containing anonymised supplemental material. Access at https://osf.io/3t4xm/overview?view_only=0d01cefadafa49819b7916bac28b9a23