
Abstract
Background
Identifying specific patterns of somatic expressions of depression among children from Global South countries may help inform health promotion, screening, referral pathways, assessments and interventions in various contexts (e.g., schools and clinics).
Method
1541 children from Barbados, Colombia and Jamaica completed the Adolescent Depression Rating Scale (ADRS) and the Children’s Somatization Iventory-24 (CSI-24). For each country, item discrimination indices (IDIs) were calculated for each item of the CSI-24 to determine which items best identified persons with the highest depression scores. Scales consisting of the six CSI-24 items with the highest IDIs in each country were then created and assessed for their association with clinically significant depression using regression analyses.
Results
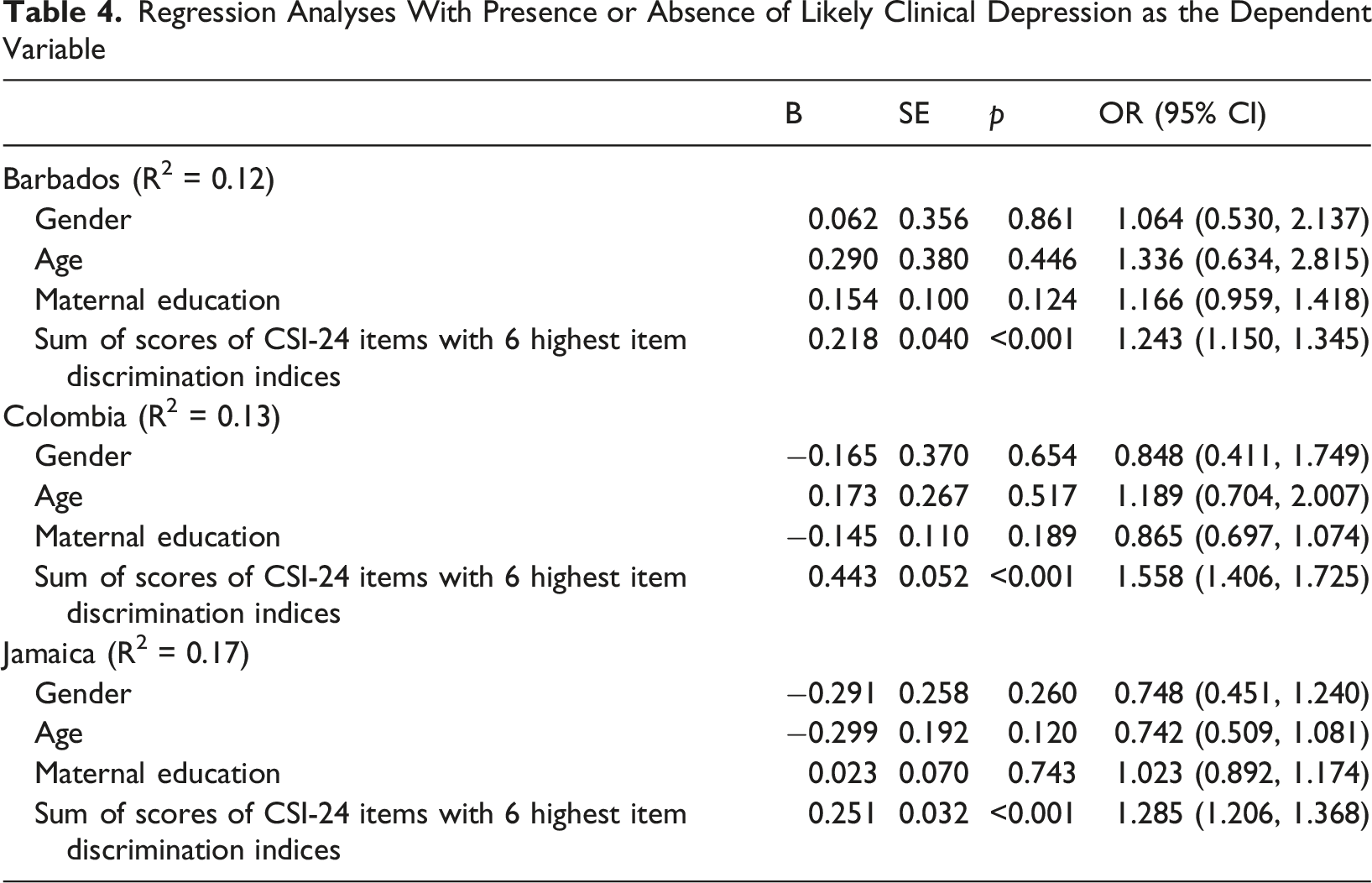
The CSI-24 items with the highest IDIs were different for each country, but with physically restrictive somatic symptoms being consistently prominent. The country-specific six-item somatic subscales were significant predictors of depression, with odds ratios (95% CI) of 1.56 (1.41, 1.73), 1.29 (1.21, 1.37) and 1.24 (1.15, 1.35) for Colombia, Jamaica and Barbados respectively.
Conclusions
“Difficulty moving forward” was symbolically represented in the restrictive somatic symptoms with high IDIs. The different findings among countries may reflect unidentified cultural nuances. Depression screening strategies that consider relevant somatic symptoms could be valuable.
Plain Language Summary
Bodily complaints are common among children with depression. Identifying which specific patterns of these complaints are most associated with depression among children from low and middle income countries may provide information that is useful for strengthening the ability of various stakeholders to identify children from these populations who are depressed and get them needed help. To identify these patterns, 1541 children from Barbados, Colombia and Jamaica were asked to answer questionnaires that assessed both depression and the presence of bodily complaints. Statistical analyses were applied to determine which patterns of bodily complaints were most associated with depression. Specific patterns were identified and, although there were some differences among the countries, a common feature was that the symptoms symbolically represented difficulties with moving forward with life. The differences that were found may be related to cultural nuances, but the strong associations between specific patterns of bodily symptoms and depression across countries suggest that this information could be utilized to enhance screening for depression.
Introduction
The presence of prominent physical complaints as a response to emotional distress is a common phenomenon among both adults and children (Chang et al., 2017; Kim Donnelly et al., 2021; Wazir et al., 2023). This may occur in the context of difficulty in understanding or processing emotional distress and may involve some psychodynamic symbolism (Gubb, 2013). Also, cultural norms and expectations often influence the extent to which this somatic expression of mental experiences occurs. For example, Chang et al. (2017) observe that the extent to which depressed persons from Asian societies identified with the cultural norm of collectivism predicted the presence of somatic complaints.
Previous research has suggested that different types of somatic symptoms may be relevant for different types of emotional distress, e.g., Weersing et al. (2012) observe that headache and fatigue were clearly associated with depression, but abdominal and chest pain were more closely associated with anxiety. In addition to the type of mental distress being experienced, there may be cultural factors that determine which specific somatic features are manifested. Somatic experiences may be viewed as an idiom for emotional distress (Wazir et al., 2023), and cultural factors may play a role in the manner in which emotional distress is expressed somatically.
The Diagnostic and Statistical Manual for Mental Disorders (DSM-5) (American Psychiatric Association, 2013) defines cultural idioms of distress as cultural groups’ shared ways of experiencing and communicating personal and social concerns. It further states that there is variability across cultures in how distress is perceived, experienced, communicated and mitigated. Kirmayer and Young (1998) report that somatization is common across cultures and, in addition to its role as a culturally-coded (although often fragmented and tentative) expression of distress, they describe it as embodying other systems of meaning including the psychodynamic symbolism and correspondence to specific psychopathological states that were previously mentioned. This study explores whether somatic expressions of depression vary among children from three different countries: Barbados, Colombia and Jamaica. In the study, the perspectives of somatic symptoms corresponding to a specific psychopathological state (depression), representing culturally-coded expressions of distress, and reflecting psychodynamic symbolism are all brought to bear on the findings.
A strong association between depressive and somatic symptoms in general among children of the three countries has previously been reported (Gibson et al., 2024). However, there has not been much more research on the subject as it relates to these countries. On the other hand, studies on Hispanic children in North America have identified that they tend to have more somatization experiences than European American children (Choi et al., 2006), and that their expression of somatization is more likely to be found among girls, in first generation immigrants, and in instances where stigma towards mental illness is high (Der Sarkissian et al., 2022). Studies from other settings have also indicated that when somatization is associated with depression in adolescents, both a greater number and higher intensity of somatic symptoms predict a greater severity of depression (Bohman et al., 2010).
Knowledge of the association between somatization and depression is helpful for clinicians and caregivers because the presence of prominent somatic complaints among children under their care may prompt them to inquire more deeply about the presence of depressive symptoms. However, more profound knowledge about the specific patterns and types of somatic symptoms that are most strongly associated with depression may be even more valuable in identifying children with depression. This, in turn, could help to decrease the risk of the under-detection and underdiagnosis of depressive illnesses, which are an ongoing public health challenge, particularly in Latin America and the Caribbean (Kohn et al., 2018) as well as other regions of the Global South (Pumariega et al., 2024).
In these settings, specialist mental health services are limited and the ideal and most efficient pathways for optimizing children’s mental health involve networks of interconnected services (World Health Organization and United Nations Children’s Fund, 2024). Parents, schools, primary care facilities, pediatric services and specialist mental health service all play a role. These various entities interface with each other to achieve health promotion, early identification of mental health issues (e.g., depression), treatment and rehabilitation. Schools in particular are an essential element of this mental health network as they often play a role in identifying children with mental health issues and helping their parents or guardians to access appropriate treatment services. Primary healthcare workers also play a salient role in identifying children with mental health issues.
The value of this collaborative approach is reflected in ongoing public health initiatives to strengthen these networks. In Jamaica, for example, the Ministry of Education recently implemented a screening referral and early interventions pathway for children (United Nations Children’s Fund Jamaica, 2025). Also, in Colombia, recent reforms introduced through Law 2460 of 2025 (Congreso de Colombia, 2025) seek to strengthen pathways to care by expanding the role of educational institutions in mental health promotion and early detection, improving access to psychological and psychiatric services, enhancing intersectoral coordination, and increasing support for children and adolescents. These changes may improve the identification, referral, and treatment of children experiencing depression.
Many more children with depression can be referred to appropriate treatment if they are identified and they can thus avert the adverse long-term sequelae such as suicide (Gili et al., 2019), substance use (McKowen et al., 2013), and delinquency (Kofler et al., 2011). In addition, previous research has shown that somatic symptoms often persist throughout childhood and adolescence and are associated with substantial impairment, particularly when they co-occur with depression and anxiety (Romero-Acosta et al., 2013). Therefore, efforts to identify these symptoms as early as possible may improve access to care and contribute to better mental health outcomes Early identification may be enhanced by exploring and sharing with all elements of the collaborative network knowledge about the role of culturally relevant somatic features, which may be more apparent than emotional ones, among children with depression.
Method
This study sought to explore patterns of somatic symptoms that were associated with depression among children from three Global South countries and, in so doing, to inform different aspects of practice (e.g., help-seeking, referral pathways, assessments and interventions) in various contexts (e.g., homes, schools, primary care facilities, pediatric services and specialist child mental health services).
Research Design
Data for this study come from a three group (Country of Residence – Jamaica, Barbados & Colombia) by two group (Type of school – Private and Public School) by three wave of data collection (October, February and April; all of which occurred within a single academic year) longitudinal quasi-experiment. For this paper, data from the second wave of data collection were used.
Ethical Considerations
Ethical approval for the study was obtained from Mona Campus Research Ethics Committee of The University of the West Indies. All participants and their parents provided assent and consent respectively for their participation in the study.
Research Setting
Barbados, Colombia and Jamaica are all independent nations that are located within the Americas and share a history of original inhabitation by indigenous peoples, European invasion and colonization, and the forced migration to their shores of Africans as slaves. Barbados and Jamaica, which are Caribbean islands, retain significant British and African influences and their people are mostly of African descent, while Colombia, which is on the South American content, is largely considered Hispanic, retaining a strong Spanish influence with people of mostly White or Mestizo ethnicity.
In Barbados and Jamaica, efforts have been made to link the health, educational and social support systems of children. Schools play a central role in the identification of children with mental health issues. They communicate concerns about children to caregivers and offer guidance on accessing appropriate interventions. As such, children who are identified with mental health issues such as depression are often referred to the primary healthcare clinics for management. The children are usually, but not exclusively, taken to the health facilities by their caregivers. The primary healthcare clinics collaborate closely with other specialist secondary health care providers such as polyclinics with child psychiatry outpatient services throughout both countries. This collaborative network helps children to gain access to appropriate mental health care.
In Colombia, children with depressive symptoms typically enter the mental healthcare system through primary healthcare services, pediatric care, educational settings, or, less frequently, specialized mental health services. Under Law 1616 of 2013 (Congreso de Colombia, 2013), mental health is recognized as a fundamental right, and children and adolescents are prioritized for prevention, early identification, treatment, and rehabilitation services. Nevertheless, barriers related to service availability, access, and cross-sector coordination continue to impede timely care. Fenton et al. (2024) note that Colombian mental health policy, due to years of armed conflict, has historically focused on vulnerable populations rather than population-wide mental health promotion, resulting in limited involvement of key stakeholders, such as the education sector, and weak interinstitutional collaboration. However, recent reforms have sought to strengthen these collaborations.
Sample
A representative sample of elementary schools in Kingston, Jamaica, Barbados (island-wide), and Sincelejo, Colombia was obtained. In Jamaica and Barbados, this was achieved by selecting them from listings from the Ministries of Education using a table of random numbers. A non-random method was used for selecting the schools in Colombia, but for all countries, schools were chosen in proportion to the percentage of government-funded public schools and privately funded preparatory schools. No schools which were sampled in any of the countries declined to participate. All exit grade classrooms (grade 6 in Jamaica and Barbados, and grade 5 in Colombia) in each school were sampled.
To be included in the sample students needed to meet three criteria. Firstly, they had to be present at school on the day of data collection. Secondly, their parents must have provided their written consent to take part in the study and thirdly students needed to provide their written assent. Failure to meet one or more of these criteria resulted in exclusion. All parents who were approached to participate in Jamaica and Barbados provided consent. Eighty-two percent provided consent in Colombia. All children whose parents consented also assented and participated. The only exception was in Barbados where only thirty-eight percent of children whose parents consented were available at the time of data collection and were included in the study.
Participants
Demographic Characteristics of the Sample
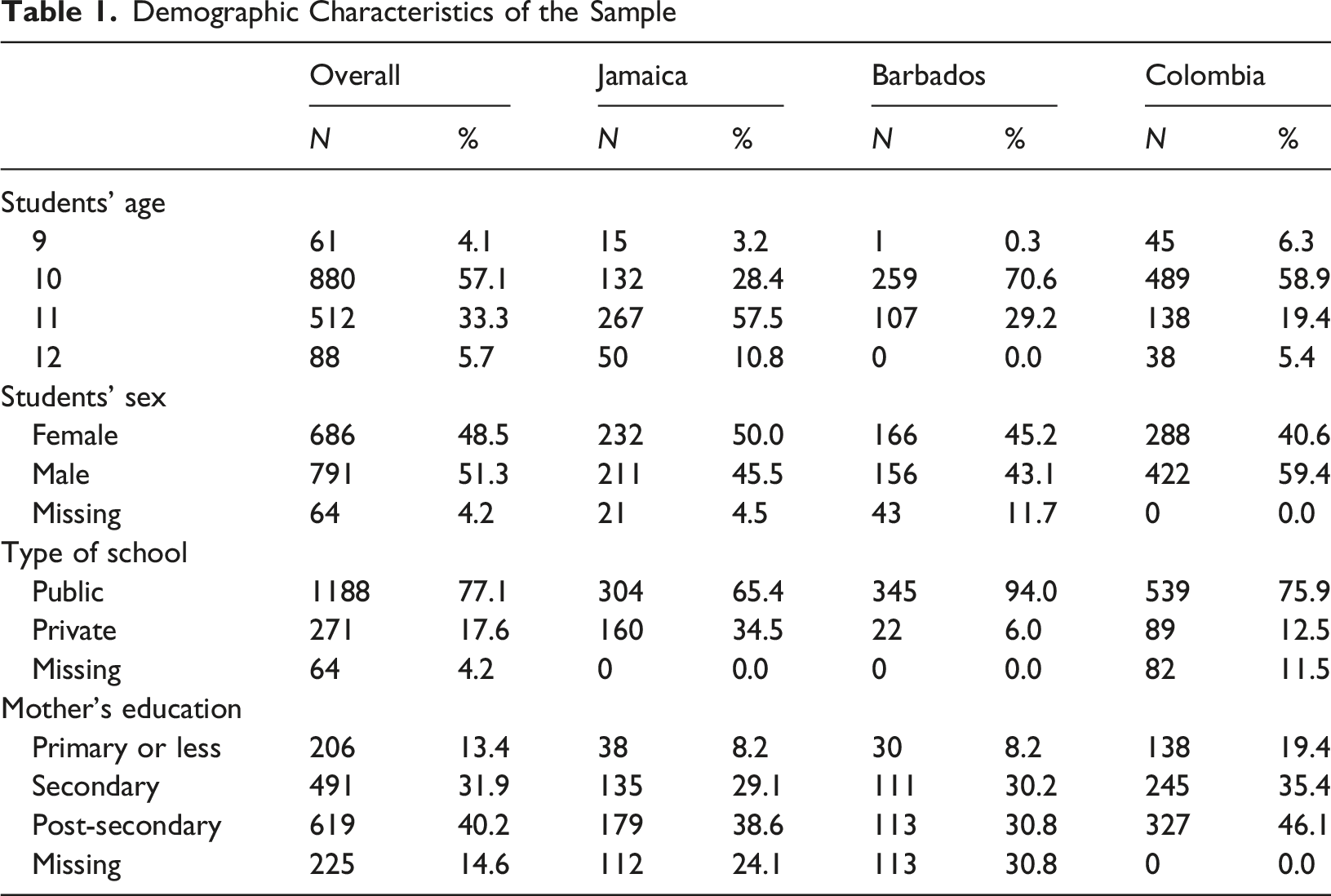
Additionally, the majority of students were male (n = 791, 51.3%) and attended public school (n = 1188, 77.1%). About four out of every ten students’ mothers had attained post-secondary education (n = 619, 40.2%).
Measures
Adolescent Depression Rating Scale (ADRS)
The Adolescent Depression Rating Scale (Revah-Levy et al., 2007) is a 10-item measure of depressive symptoms for use with children ages 13 to 19 years. The ADRS assesses the cognitive, affective, and somatic symptoms of depression. Respondents are asked to indicate whether each item is true or false for them. The scale was developed using a three-step procedure. In the first step, a review of the literature on adolescent depression was conducted to conceptualize the manifestation of depression among adolescents. Next, separate interviews with child psychiatrists and with depressed adolescents were conducted to identify depressive symptoms and how they clustered. From this process, an initial 44-item self-report depression measure was created for adolescents. A factor analysis of the measure was then used to create a ten-item, unidimensional measure of depression. Scores range from zero to ten, and a score of four or more corresponds to DSM-IV criteria for major depressive disorder with a sensitivity of 0.80 and a specificity of 0.60. The creators of the ADRS report acceptable levels of internal consistency reliability (α = 0.74 to 0.79) as well as good concurrent validity as demonstrated by fairly strong correlations with the Hamilton Depression Rating Scale (r = 0.56), the Beck Depression Inventory - 13 (r = 0.82) and the Clinical Global Impression Severity Scale (r = 0.52). The validity of the ADRS among children in Colombia (Romero-Acosta & Gómez-de-Regil, 2019) as well as Jamaica and Barbados (Lipps et al., 2021) has been demonstrated in previous research.
Children’s Somatization Inventory – 24 (CSI-24)
The Children’s Somatization Inventory - 24 (Walker et al., 2009) is a 24-item measure that assesses the perceived severity of twenty-four somatic symptoms. The measure was constructed using items from the Somatization sub-scale of the Hopkins Symptom Checklist along with symptoms of Somatization Disorder from the DSM III - R. The original measure (Garber et al., 1991) consisted of 36 items which were subsequently pared down to 24 items. Using the item stem from the Hopkins Symptom Checklist, children were asked to report “How much were you bothered by (Specific Symptom)” during the past two weeks. In the current study, the item stem was modified to read “In the last 2 weeks, how much were you bothered by each symptom?” Students recorded their answers to these questions using a five-point Likert-type response format with 0 representing “Not at All”, 1 “A Little”, 2 “Sometimes”, 3 “A Lot”, and 4 “A Whole Lot”. Total scores were converted into standardized scale scores using the instructions of the authors of the scale. The original CSI has acceptable concurrent validity as demonstrated by strong correlations (r = 0.76) with another measure of somatic sensations (The Pennebaker Inventory of Limbic Languidness; Pennebaker, 1982), and acceptable predictive validity as demonstrated by moderate correlations with the Children’s Depression Inventory (r = 0.37; Kovacs, 1981) and the Spielberger Trait Anxiety Scale (r = 0.43; Spielberger, 1973). The CSI-24 has acceptable internal consistency reliability as reported by the authors (α = 0.87; Walker et al., 2009) and as found in the current study (α = 0.90 across all three countries).
Procedure
As a quality control measure, think-aloud interviews were conducted to assess children’s ability to understand each question within each questionnaire before they were used. Following this process, amendments were made to the questionnaires to ensure that the children correctly understood each question.
Participating schools identified regular class sessions during the normal school day for the administration of the instruments. At the start of the session, research assistants provided a brief introduction to the project. The project was described as an investigation into the psychosocial factors associated with mood and social relationships. Participants whose parents provided their consent were informed that their participation was completely voluntary and that they could withdraw from the project at any time. Questionnaires containing the scales were then distributed for completion. Completed questionnaires were returned to one of the investigators at the end of the session. For each completed CSI-24 questionnaire, items were summed and converted to standard scores using the Rasch measure scores (Walker et al., 2009).
Statistical Analyses
The data were entered into SSPS (Version 21) for analysis. On a question-by-question basis, missing data, for all variables, except gender and type of school, were substituted using the Expectation Maximization procedure in SPSS.
Item analyses were conducted to determine which somatization items best differentiated depressive symptoms using item discrimination indices. There were separate item analyses for each country. In each instance, the upper quartiles for both the CSI-24 item scores and the ADRS total scores were first determined. Next, considering the CSI-24 items individually, of the participants who scored in the upper quartile on each CSI-24 item, the proportion who also scored in the upper quartile of the ADRS (PU) was determined. Then, still considering the CSI-24 items individually, of the participants who did not score in the upper quartile on each CSI-24 item, the proportion who scored in the upper quartile of the ADRS (PL) was determined. The item discrimination index for each CSI-24 item in each country was calculated by subtracting PL from PU.
For each country, the CSI-24 items with the six highest item discrimination indices were identified and compared. For each country, a scale consisting of these six items was created. To test for any clinically relevant association between depression and the six selected CSI-24 items for each country, binary logistic regression analyses were undertaken. In these analyses, an ADRS variable with categories representing the presence (ADRS ≥ 4) or absence (ADRS < 4) of depression of likely clinical significance was utilized as the dependent variable, and the sum of the scores of the relevant six CSI-24 items, as well as gender, age and maternal educational level were included as independent covariates.
Results
ADRS Scores by Country

Item Discrimination Indices of CSI-24 Items by Country
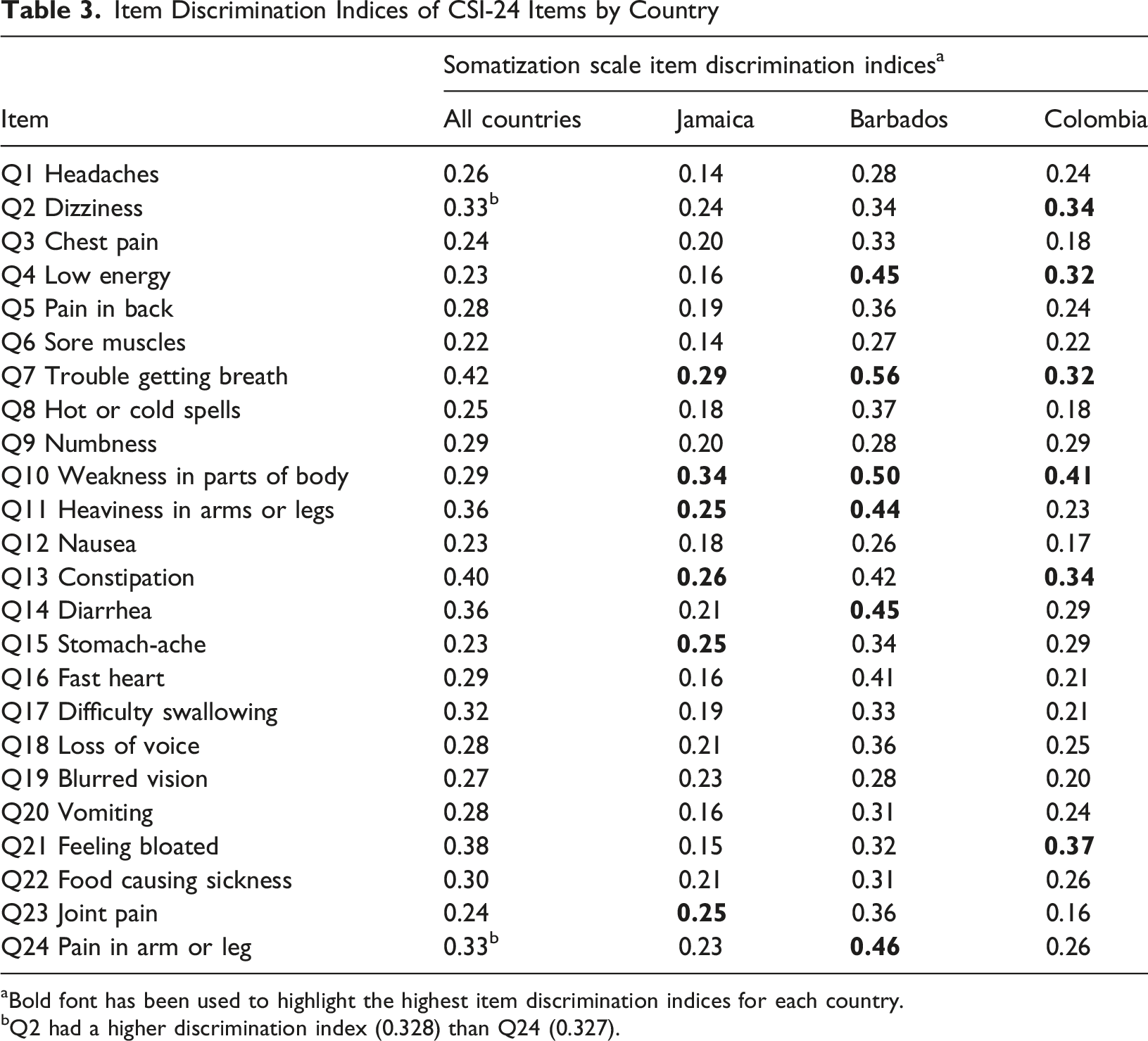
aBold font has been used to highlight the highest item discrimination indices for each country.
bQ2 had a higher discrimination index (0.328) than Q24 (0.327).
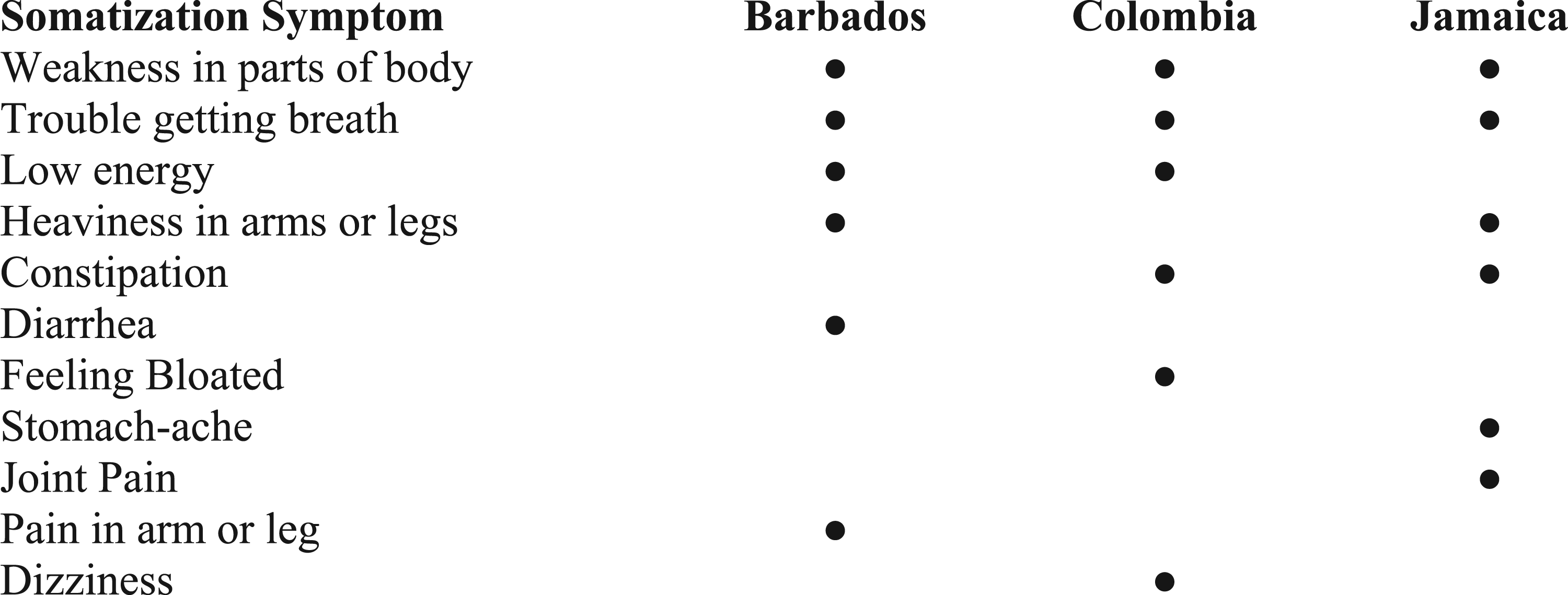
CS1-24 items with the highest item discrimination indices for each country
Weakness in parts of the body and trouble getting a breath were among the CSI-24 items with the six highest item discrimination indices for all three countries. Two out of three countries had low energy, heaviness in arms and legs, or constipation among the CSI-24 items with the highest item discrimination indices. Other gastrointestinal symptoms of diarrhea, feeling bloated and stomachache were among the items with the highest indices in one country each, as were pain in the arms or legs and dizziness (Figure 1).
Regression Analyses With Presence or Absence of Likely Clinical Depression as the Dependent Variable
Discussion
The “speechless mind” and the “speaking body” are common psychoanalytic conceptualizations of the somatic expression of emotional distress (Gubb, 2013). They relate to persons who are unwilling or unable to process distressing experiences, and of the body taking on the communication of distress of which the mind is incapable. Difficulty with processing and communicating about personal distress is especially likely to be present among children, given their developmental stage.
Persons with lived experiences of depression report that feeling overwhelmed is a core feature of the condition (Fusar-Poli et al., 2024). Such an emotional state may impede affected individuals from moving forward with life. Trouble getting a breath and weakness in parts of the body may be viewed as “the speaking body” communicating an inability to move forward or acknowledging the presence of obstacles to engaging with everyday life. These somatic symptoms were significantly associated with depression in each of the countries that were studied (Barbados, Colombia, and Jamaica). Of note, Vaccarino et al. (2008) and Li et al. (2023) have also found weakness in parts of the body to be linked to depressive states. We theorize that the difficulty moving forward that characterizes depression is symbolically represented in the prominent somatic symptoms that the children who were likely to have depression of clinical significance experienced. Further investigation of this concept with appropriate research methodologies is warranted.
It is noteworthy that the experience of weakness in parts of the body, as opposed to the more generalized concept of “low energy” (which was another of the CSI-24 items), was exhibited across all countries by children who were most likely to be depressed. Among children with a greater likelihood of depression the more generalized “low energy” was restricted to Barbados and Colombia only. This is useful information because, overall, simply asking children about weakness may be less helpful in an assessment for depression than inquiring about weakness that is restricted to some body parts.
For the Barbadian sub-sample, besides trouble getting a breath, weakness in parts of the body, and low energy, the strongest somatic predictors of depression severity were heaviness in the arms or legs (which was also one of the strongest predictors among Jamaican children and may be yet another manifestation of difficulty moving forward), diarrhea, and pain in the arm or leg. Diarrhea has previously been shown to be associated with depression severity among adults (Ballou et al., 2019; Wang et al., 2024). Pain and depression are frequently comorbid (Harte et al., 2024) with some possible mechanisms being depression preceding the onset of pain, depression following the onset of pain, or a shared predisposition to both depression and pain (Fishbain, 2002).
Colombian children who reported dizziness, or the gastrointestinal symptoms of constipation or feeling bloated were likely to have greater depression severity than other Colombian children. Lorente-Piera et al. (2024) observe that it is common for clinicians to view dizziness in children as being psychosomatic in origin, although they caution that, in clinical practice, the possibility of vestibular dysfunction should not be overlooked. Similarly, the association between depression and gastrointestinal symptoms is well known, with the influence of stress on the brain-gut axis being one possible mechanism (Ballou et al., 2019).
For the Jamaican children, the most significant predictors of depression that were not also common to all three countries were heaviness in the arms and legs (which was also a strong predictor in the Barbadian children); constipation (which, as previously discussed, may possibly be a manifestation of mechanisms involving the brain-gut axis); and pain in the stomach or in joints, such as the knee or elbow. As mentioned before, there are several pathways that may connect depression and pain.
Overall, physical symptoms that impeded one from moving forward, as well as gastrointestinal and pain symptoms were the most prominent somatic predictors of depression across all three countries. The possibly universal theme of the psychodynamic symbolism of difficulty moving forward, the influence of the brain-gut axis, and the generally common comorbidity of depression and pain have already been discussed. However, the reasons for the differences across countries, with regard to the somatic symptoms that best predicted depression, are more difficult to explain. While “cultural differences” constitute an intuitive explanation, the details of the specific cultural characteristics that lead to specific somatic manifestations are much less obvious, and warrant further exploration with anthropological research. Although no firm conclusions can be drawn about, for example, what cultural features make dizziness strongly associated with depression in Colombia but not in Jamaica or Barbados, it is clear that differences between the countries exist and this should be taken into account when probing depression with a somatic lens.
In addition to supporting the concepts of psychodynamic symbolism and cultural variability in the somatic expression of depression among children of the three countries, the study’s findings also point convincingly to specific somatic symptoms as being representative of a specific psychological state (depression). This is potentially very useful clinical information because in practice, the identification of childhood mental disorders is challenging and many children with these conditions are not identified until the symptoms become severe (Gómez-Restrepo et al., 2021). Sensitizing relevant stakeholders such as children, parents, teachers, primary healthcare workers and other health professionals about the association of depression with specific somatic symptoms may lead to earlier and better identification of children at risk for depression who may otherwise go unrecognized.
Inquiring about the six CSI-24 items that were most predictive of depression in each country may function as an effective way of screening for depression among children in the respective countries. It is also plausible that with further refinement and validation testing, screening instruments based on the six CSI-24 items per country could be developed. Integrating somatic symptom screening into routine health and educational assessments may enhance early detection and facilitate timely intervention. Furthermore, recognizing somatic symptoms as potential markers of depression may strengthen pathways to care by prompting earlier referral for mental health assessment and treatment, thereby reducing delays in accessing appropriate services. This may be particularly valuable in settings where specialized mental health resources are limited, and children are more likely to encounter primary care providers, pediatricians, or school personnel before mental health professionals. Future research should examine whether incorporating somatic symptom assessment into existing pediatric and school-based screening pathways improves referral processes, service utilization, and treatment outcomes for children and adolescents.
One potential obstacle to the implementation of screening or other interventions based on the study’s findings is that the relevant stakeholders may not intuitively appreciate that somatic symptoms may be so reliably linked to depression. Sensitizing these individuals to the evidence for the association between depression and specific somatic symptoms in specific local contexts would therefore be important. A useful approach to this sensitization would be to utilize elements of the same networks that are depended upon to direct children to mental health services. For example, in school settings, existing interfaces between teachers and caregivers such as Parent Teacher Associations (PTAs) may be used to educate teachers and parents about the association. In addition, healthcare professionals could be reached for sensitization and training through existing in-service training opportunities or continuing medical/professional education activities. Both the recognition of depression with somatic presentations as well as the best approaches to this type of clinical scenario would be valuable areas for training. The conventional approach for managing patients with prominent somatic complaints would be worth pursuing, bearing in mind that both the child and their caregiver would need to be engaged clinically. Thus, clinicians could be educated or reminded about issues such as the value of developing strong rapport (with both the child and the care-giver); exploring the presence of both mental and physical illnesses; explaining (to the child and the caregiver) that physical symptoms may be simultaneously from different causes, some of which are emotional; treating the underlying depression; and having regular follow-up (Henningsen, 2018). The sensitization activities for teachers and caregivers could also incorporate the explanation aspect of the clinical approach. Using highly relatable examples of how somatic symptoms may reflect underlying emotional states may help to convince stakeholders in both health promotional and clinical settings about the relationship between somatic symptoms and depression. For example, it could be explained that just as how being scared may cause the heart to race, being very sad may cause bodily feelings of being able to move forward.
Limitations
Some limitations apply to the study. The cross-sectional design precludes the formation of causal inferences about cultural characteristics and depressive or somatic symptoms. As previously noted, neither does the study’s methodology facilitate the exploration of the association between specific cultural characteristics and the differences in somatization patterns that were observed across countries. It should also be considered that the participants in each of the countries studied did not constitute homogenous samples and that this further constrains conclusions that can be made about culture. Finally, although the CSI-24 has been widely used internationally, investigations into its cultural validity for the study’s participants were not conducted.
Footnotes
Ethical Considerations
Ethical approval for the study was obtained from The University of the West Indies’ Ethics Committee. (Approval Number: ECP 173, 13/14). All parents and children provided their written informed consent and assent for their data to be used in the research prior to the collection of their responses.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by University of the West Indies.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.