
Abstract
Public knowledge of acute stroke symptoms is a goal of public health policy. Similarly, general health knowledge is a hypothesized pathway for the salutary effects of social ties. This study examined the association of stroke warning sign knowledge with the quantity (number of recent social contacts) and/or quality (perceived emotional support) of social ties in two population-based cross-sectional surveys (Ns = 33,326 and 80,454). Both higher levels of emotional support and more frequent social contacts were independently associated with greater stroke warning sign knowledge. Social isolation is a novel marker of poor knowledge of stroke warning signs.
Introduction
Stroke is the third leading cause of death in developed countries and is associated with substantial disability and healthcare expenditures. Population-based surveys reveal low awareness of both stroke warning signs and the optimal helping behavior when one suspects someone is having a stroke, that is, to call emergency medical services (EMS) (Greenlund et al., 2003; Jones et al., 2010). Prompt medical attention is essential for preventing death and disability from stroke, and the delay between symptom recognition and seeking medical care is the longest epoch between the incident stroke and treatment (Moser et al., 2006).
Public health guidelines focus on educating the public about stroke symptoms/warning signs and the need to request ambulance transport for suspected stroke victims (Centers for Disease Control and Prevention, 2008a). Consideration of social factors may facilitate this goal (Teuschl and Brainin, 2010) because stroke symptom recognition and optimal help seeking choices are embedded in one’s social environment. More so than medical professionals, friends and family are an important source of information about stroke (Muller-Nordhorn et al., 2006; Yoon and Byles, 2002). Similarly, bystanders are often the first to recognize stroke signs (Feldmann et al., 1993; Mandelzweig et al., 2006) and are more likely to contact EMS than the stroke victim (Wein et al., 2000). Thus, the social environment is an important determinant of acquiring knowledge of stroke warning signs, providing assistance for acute stroke victims, and facilitating adjustment following a stroke (Ch’ng et al., 2008).
Health knowledge is a central element of theoretical models of the social environment and health in that these theories posit that information is one pathway through which the social environment affects health (Cohen, 2004; Oakes and Rossi, 2003). Specifically, social ties are hypothesized to stratify a broad range of health resources (House, 2001) including in particular health-related information (Cohen, 2004). However, the association of health-related knowledge with the social environment has received little scrutiny and no studies to date have examined the association between social relationships and knowledge of stroke warning signs. To test predictions derived from social environmental theory (Cohen, 2004; Oakes and Rossi, 2003) I examined the association of two social relationship markers, perceived emotional support and the frequency of social contacts, with knowledge of stroke warning signs. This association was evaluated in two large, diverse representative US samples. It was expected that higher emotional support and more frequent social contacts would be associated with greater stroke warning sign knowledge.
Method
Overview
Perceived emotional support and five stroke symptom recognition questions were assessed in 13 state-specific modules in the 2007 Behavioral Risk Factor Surveillance System (BRFSS) and in the 2001 National Health Interview Survey (NHIS). The BRFSS also included a decoy symptom question (chest pain) and a question about what the respondent would do if they thought someone was having a stroke. A measure of recent social contact frequency was available in the NHIS but not in the BRFSS. Thus, these two surveys permit evaluation of the association of emotional support with stroke symptom knowledge, as well as comparison of the predictive strength of social relationship quality (perceived support) and quantity (number of contacts – in the NHIS).
Data sources
Behavioral Risk Factor Surveillance System
The BRFSS is an annual telephone survey of non-institutionalized US adults in all 50 states, the District of Columbia and several US Territories (Centers for Disease Control and Prevention, 2008b). Stroke symptom knowledge was part of an optional module fielded by 11 states, the District of Columbia and the US Virgin Islands (hereafter referred to as ‘states’). The median cooperation rate (percent of eligible contactees interviewed) for these 13 states was 71.8 percent (range 56.9–78.7) (Centers for Disease Control and Prevention, 2008c). Of the 86,573 participants in these states, 80,454 had non-missing responses to the stroke knowledge and emotional support items. All participants provided verbal consent.
Stroke knowledge was defined as the sum of correct responses to seven questions. Correct responses included: (1) affirming that five of the symptoms were stroke warning signs (sudden numbness or weakness in face/arm/leg, confusion/trouble speaking, trouble seeing, sudden trouble walking/dizziness, sudden severe headache); (2) disconfirming the decoy symptom question (chest pain); and (3) choosing ‘call 911’ if they thought someone was having a heart attack or stroke.
National Health Interview survey
The NHIS is an annual in-person population-based survey of non-institutionalized US residents (National Center for Health Statistics, 2003). The present study utilized the sample adult respondents from the 2001 survey (N = 33,326). All participants provided written, informed consent. The conditional response rate for the sample adult component was 73.8 percent. Of these 98 percent (32,604) had non-missing values for analyses including stroke knowledge, emotional support, and the frequency of social ties.
Stroke knowledge was the sum of ‘yes’ responses to five stroke symptoms (see above). Items with refused (< 1%) or ‘don’t know’ responses were scored as incorrect. Social ties reflected the sum of six binary questions regarding contact with friends or relatives, over the phone or in person, as well as attending a group social activity or a religious service. Social contact questions referred to the past two weeks and specifically excluded interactions with household members. Items with refused (< 1%) or ‘don’t know’ responses were scored zero.
Emotional support
In both surveys emotional support was assessed with the question: ‘How often do you get the social and emotional support you need?’ Response options were always, usually, sometimes, rarely, or never.
Statistical analyses
Multiple logistic regression incorporating the complex survey design (Stata software version 10.1) was used to assess the association of stroke knowledge with social environment variables. These analyses are representative of their respective state (BRFSS) and national (NHIS) referent groups. Stroke knowledge was defined as either 100 percent correct or not (Greenlund et al., 2003). Knowledge was regressed on social ties and then adjusted for age, gender, race/ethnicity, marital status, education, previous stroke, heart attack or coronary heart disease, diabetes, hypertension, and smoking. Missing values on covariates reduced the sample sizes for multivariate analyses by less than 4 percent.
The social ties variables violated an interval measurement assumption (ps < .001) (Long and Freese, 2003) so dummy codes were used to represent categories of emotional support and social contact frequency. The most isolated categories (e.g. 0/1 social contacts; never/rarely receiving emotional support) were collapsed to accrue reasonable cell sizes (> 5% of the sample) for analyses. Sensitivity analyses revealed generally consistent associations across logistic analyses, ordinary least squares and right-censored Tobit regression models.
No institutional ethical review was required for this study because it involved secondary analysis of publicly available data that lacked identifying information.
Results
Demographic and social environmental characteristics for the two samples are presented in Table 1. Substantially fewer respondents answered all knowledge items correctly in the BRFSS (17%) versus the NHIS (59%).
Sociodemographic characteristics and stroke symptom knowledge in the 2007 Behavioral Risk Factor Surveillance System and the 2001 National Health Interview Survey.

Note: Proportions are weighted to represent the 13 states that used the optional heart disease and stroke module in the Behavioral Risk Factor Surveillance System or the US population in the National Health Interview Survey. Variable percentages may not sum exactly to 100 due to rounding.
Higher perceived emotional support was associated with greater knowledge across both surveys. This association was somewhat attenuated after adjusting for age, race, ethnicity, gender, education, the presence of stroke risk factors, and prior stroke. The magnitude of the association was most consistent for the usually and always levels of perceived support and in the NHIS this association was independent of social contacts (see Table 2). For example, those reporting always receiving the emotional support they need were more likely to answer all of the stroke questions correctly (BRFSS odds ratio [OR] = 1.32; 95%CI = 1.10–1.58, p < .001; NHIS OR = 1.27; 95%CI = 1.13–1.42, p < .001).
Logistic odds ratios (95% CIs) predicting binary stroke knowledge, 2001 National Health Interview Survey and 2007 Behavioral Risk Factor Surveillance System.
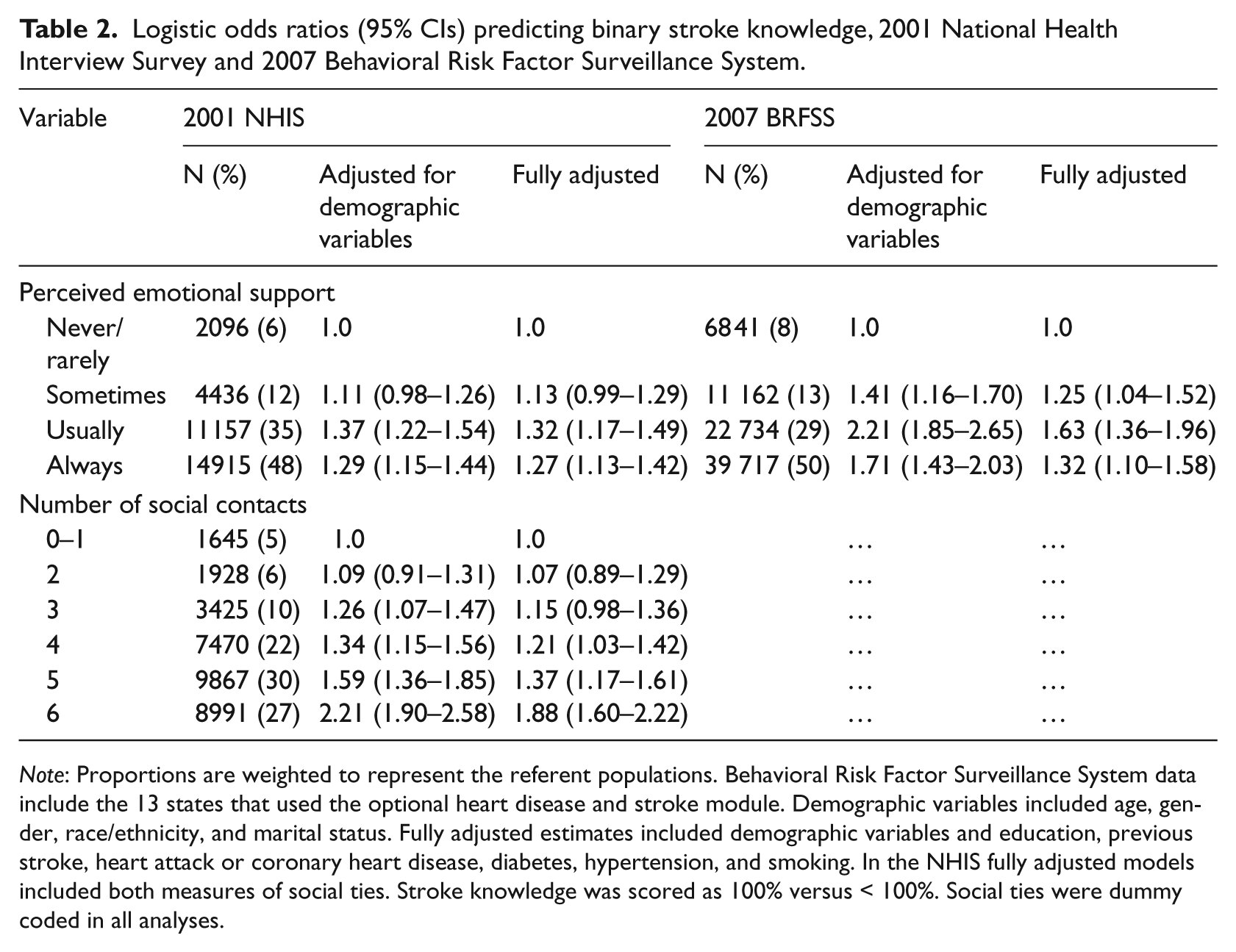
Note: Proportions are weighted to represent the referent populations. Behavioral Risk Factor Surveillance System data include the 13 states that used the optional heart disease and stroke module. Demographic variables included age, gender, race/ethnicity, and marital status. Fully adjusted estimates included demographic variables and education, previous stroke, heart attack or coronary heart disease, diabetes, hypertension, and smoking. In the NHIS fully adjusted models included both measures of social ties. Stroke knowledge was scored as 100% versus < 100%. Social ties were dummy coded in all analyses.
In the NHIS more frequent social contacts showed a strong association with stroke knowledge and this association was independent of perceived emotional support. For example, those with five or six recent social contacts were more likely to classify all stroke warning signs correctly (ORs = 1.37 [95%CI = 1.17–1.61] and 1.88 [95%CI = 1.60–2.22], respectively, ps < .001). Generally the knowledge difference emerged at the middle levels of social integration, that is, reporting more than three social contacts or perceiving emotional support sometimes or usually. The size of the associations between social environment variables and stroke knowledge were consistently higher than gender (adjusted ORs 1.12–1.18, NS) and previous stroke (adjusted ORs 1.12–1.17, NS) and were comparable in magnitude to having a high school education versus less than high school (adjusted ORs 1.32–1.61, ps < .05).
The associations of emotional support and social contacts with stroke knowledge were generally consistent across White, Black, and Hispanic subgroups. However, emotional support did not achieve conventional significance levels for Black and Hispanic subgroups in fully adjusted models in the NHIS (data not shown).
Educational categories representing some college or more had the strongest associations of any predictor, with odds ratios from 1.3–3.2. Stroke symptom knowledge was examined within education categories by levels of emotional support and social integration (Fig. 1). Regardless of education level, high emotional support was associated with greater stroke awareness (BRFSS). This graded association for emotional support was replicated in the NHIS data and also observed for the frequency of social ties (Fig. 1).
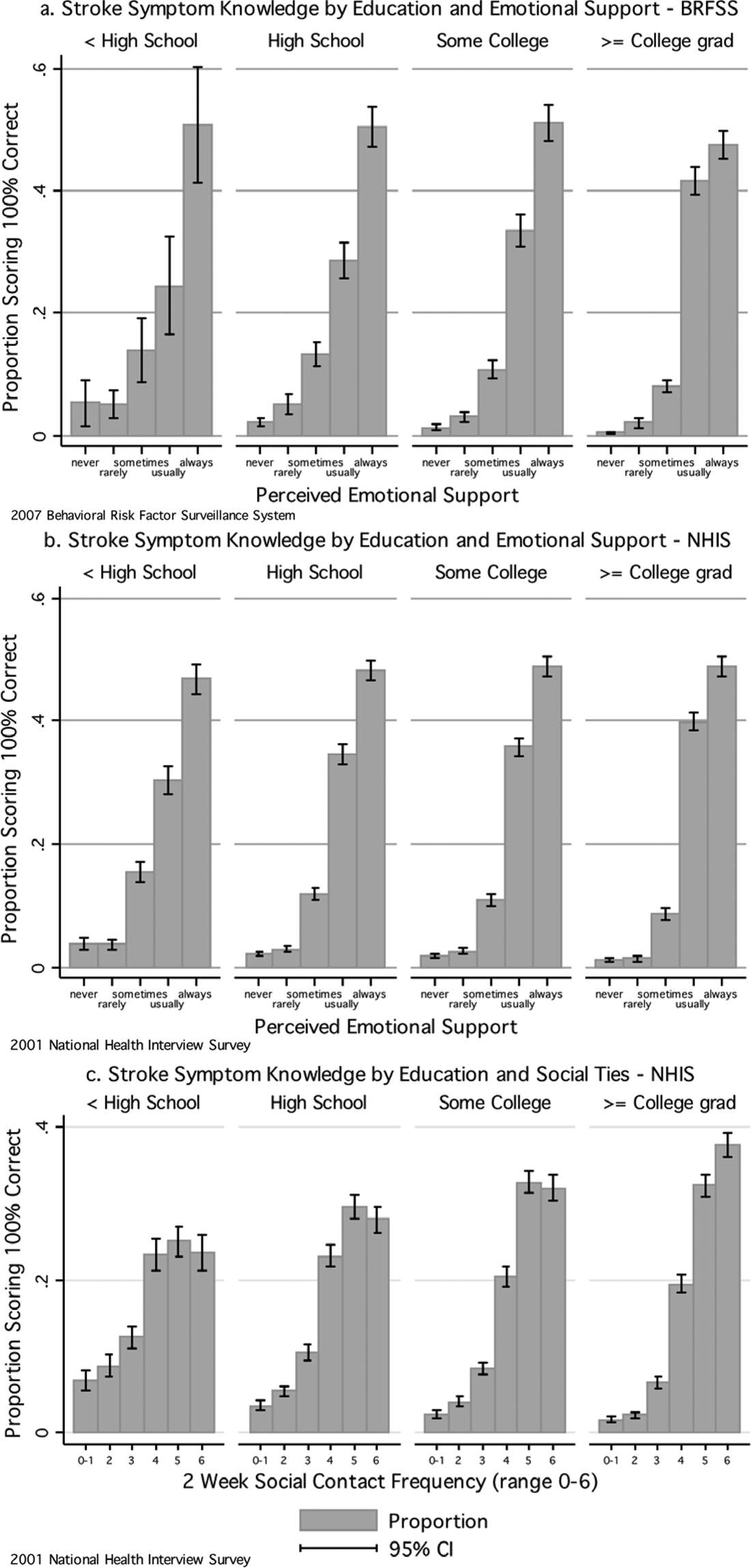
Stroke symptom knowledge by education level and social ties.
Discussion
In two large US probability samples greater perceived emotional support and more frequent social contacts were associated with better knowledge of stroke warning signs. This association was independent of established knowledge determinants and was robust across one of the strongest knowledge predictors, educational achievement. The pattern of higher knowledge among more socially connected individuals was replicated across assessments that varied substantially in difficulty; 71 percent fewer participants correctly answered all questions in the BRFSS survey. Finally, these associations were consistent across disparate time intervals and survey methods, that is, in person or via telephone.
Disparities in stroke knowledge and appropriate help seeking behavior have been observed among men, blacks, Hispanics, and less educated persons (Centers for Disease Control and Prevention, 2008a; Greenlund et al., 2003). Social isolation, as measured by both low emotional support and infrequent social contacts, represents another marker of knowledge disparities in these data. Particularly notable is that those with less than a high school education with high levels of emotional support had greater knowledge scores than socially isolated individuals with a college degree. Public knowledge of stroke warning signs remains low and health education efforts (Centers for Disease Control and Prevention, 2008a; US Department of Health and Human Services, 2000) might be improved by incorporating communication channels likely to reach socially isolated individuals.
Social ties are broadly related to better health (Barth et al., 2010; Buchman et al., 2009; Ikeda et al., 2008) and the predictive strength of social ties with mortality is comparable to established risks such as physical inactivity and smoking (Holt-Lunstad et al., 2010). The associations reported here provide additional evidence for the broad importance of social relationships and confirm that health resource access, as defined by knowledge of stroke warning signs, are stratified by social ties (Berkman and Glass, 2000). Indeed, friends and family are important sources of stroke-related health information (Jones et al., 2010; Muller-Nordhorn et al., 2006) and there is evidence that health-related behavior is transmitted via social distance (Christakis and Fowler, 2007, 2008). These converging reports support theoretical predictions that social ties stratify health resources (see Berkman and Glass, 2000).
For acute stroke the importance of the social environment extends beyond individual-level knowledge. Bystanders are often the first to notice stroke warning signs (Feldmann et al., 1993; Mandelzweig et al., 2006) and to call EMS during suspected strokes (Wein et al., 2000). This suggests that socially integrated people who experience a stroke would be more likely to be around others, others who potentially would also have greater awareness of stroke warning signs. Although these associations would be difficult to test, the importance of bystanders in acute stroke recognition and help seeking is established (Teuschl and Brainin, 2010) and the bystander role could be elucidated by tracking social environmental variables in stroke registries (Reeves et al., 2006).
Limitations and caveats
No causal relation between social ties and stroke knowledge can be inferred from these cross-sectional data. The social ties measures in this investigation capture but two elements of a large number of potential measures of social integration, for example, the size or reciprocity of social networks (Berkman and Glass, 2000). In addition, closed-ended knowledge assessments like those used here result in higher knowledge scores relative to open-ended assessments (Pancioli et al., 1998; Rowe et al., 2001). Conversely, the associations observed in this study were robust across both relatively easy and difficult knowledge assessments, including one that evaluated whether people would contact EMS for suspected stroke victims (BRFSS).
Although knowledge is an important public health goal, knowledge assessments are also limited. Survey knowledge assessments do not resemble the context in which one must interpret spontaneously occurring symptoms/signs as a stroke (Rowe et al., 2001). Greater knowledge of stroke warning signs is not always associated with faster help seeking (Fussman et al., 2010), and acute stroke often impairs motor and communication capabilities that could increase pre-hospital delay (Moser et al., 2006). Social, cognitive, and emotional elements of stroke recognition and help seeking remain important areas for future research (Moser et al., 2006). Despite these caveats, these data confirm predictions of social environmental theory (Cohen, 2004; House, 2001; Oakes and Rossi, 2003) showing that social ties, broadly defined, stratify knowledge of a health resource prioritized by public health policies.
Conclusions
In two population-based surveys higher perceived emotional support and more frequent social ties were associated with greater knowledge of stroke symptoms/warning signs. Such patterns are consistent with theoretical predictions and suggest that these elements of the social environment are novel and independent markers of stroke knowledge. These data also suggest that public health efforts to educate the public about stroke warning signs should target socially isolated people (cf. Lawson et al., 2010), perhaps via sustained televised media campaigns (Hodgson et al., 2007) that link stroke knowledge with the contexts in which strokes occur (Teuschl and Brainin, 2010).
Footnotes
None declared.