
Abstract
Individuals with medical conditions report more depressive symptoms than those without such conditions. This study assessed whether physical activity (PA) plays a mediational role in the association between medical conditions and depressive symptoms among Latino adults. Adjusting for socioeconomic factors, those who reported having been diagnosed with diabetes, cardio-related disease, hypertension, high cholesterol, arthritis, or sleep problems endorsed more symptoms of depression. Vigorous PA mediated the relation between depressive symptoms and hypertension. In other words, people with hypertension who engaged in vigorous PA reported less depressive symptoms. PA may be a promising avenue for improving hypertension and depressive symptoms.
Recent years have witnessed a dramatic increase in the number of Latinos residing in the United States. Latinos comprised 12.5% of the U.S. population in the 2000 Census, and they are predicted to comprise 25% of the U.S. population by 2050 (Current Population Reports P25-1130, 1996). This dynamic growth underscores the need for a more comprehensive understanding of health and mental health needs among Latino communities in the U.S. Research to date suggests that Latinos in the U.S. are at comparable risk for many mental health problems as are non-Latino Whites and at higher risk for certain physical health problems (Mendelson, Rehkopf, & Kubzansky, 2008; Ortega, Feldman, Canino, Steinman, & Alegría, 2006; Urizar & Sears, 2006). With respect to mental health disorders, national data indicate that lifetime prevalence of any depressive disorder is 15.4% among Latinos, and lifetime prevalence of major depressive episodes is 15.2% among Latinos (Alegría et al., 2008). A recent meta-analysis found that prevalence of major depression did not differ significantly between Latinos and non-Latino Whites; Latinos reported significantly more depressive symptoms than non-Latino Whites but the magnitude of this difference was small (Mendelson, Rehkopf, & Kubzansky, 2008). Latinos have been found to experience high rates of chronic physical disorders such as hypertension and diabetes (CDC, 2004). Some data suggest diabetes is twice as prevalent among Latinos as non-Latino Whites (Harris, Klein, Cowie, Rowland, & Byrd-Holt, 1998). Understanding associations between physical and mental health among Latinos may help us identify mechanisms that can inform interventions aimed at enhancing positive health outcomes for Latino populations.
The intersection of physical and mental health difficulties can confer significant functional limitations (Chapman, Perry, & Strine, 2005; Moussavi et al., 2007). Major depression and depressive symptoms have been found to occur with higher frequency among persons with long-term medical conditions than in the general U.S. population (Gagnon & Patten, 2002; Patten, 2005; Whooley, 2006). Among Latinos in the U.S., depression was found to be associated with a history of asthma (Ortega, et al., 2006), and qualitative data suggest that the lack of management of diabetes is associated with symptoms of depression and anxiety (Cherrington, Ayala, Sleath, & Corbie-Smith, 2006). 1 Co-occurring physical and mental health problems have been found to increase risk for premature mortality risk (van Melle et al., 2004) and to increase treatment costs (Ciechanowski, Katon, & Russo, 2000) and decrease treatment adherence (Ciechanowski, et al., 2000). Associations of physical and mental health are of public health importance because poor functioning in one of those domains may exacerbate difficulties in the other (Lu, 2011). Conversely, intervention strategies that promote improvements in physical health may have positive impacts on mental health, and vice versa.
There is growing interest in the relation between medical conditions and depression through the study of potential mediating mechanisms. These include biological factors, such as hypothalamic pituitary axis activity and heart rate variability (Carney et al., 2005), psychosocial factors such as self efficacy (Netz, Wu, Becker, & Tenenbaum, 2005) and behavioral factors, such as smoking, alcohol use and physical activity. By targeting the mediators, behavioral scientists can target potential pathways by which interventions work.
Physical activity is increasingly recognized as an important mediator of the relation between physical conditions and depression. For instance, a recent cohort study found that the link between depressive symptoms and cardiovascular events was largely explained by physical inactivity (Whooley, 2006). Data also suggest that depressive symptoms and physical inactivity may interact to increase cardiovascular mortality risk (Kamphuis et al., 2007). Sedentary behavior was found to partially mediate the relation between depressive symptoms and mortality from coronary heart disease (Brummett et al., 2003). Studies that examine the role of physical activity as a mediator are important because findings can inform the development of intervention programs that incorporate physical activity with the goal of improving physical and mental health.
Numerous neurobiological and psychosocial mechanisms have been proposed to explain the role of physical activity in the etiology and treatment of affective disorders, particularly depression (Mutrie, 2000). Data from randomized clinical trials and meta-analyses support a causal role for physical activity as a therapeutic adjunct in the treatment of depression, with a recent Cochrane review (Mead et al., 2009) reporting an effect size reduction in depressive symptoms of d = -0.82 (95% CI -1.12, -0.51), compared to control interventions. When only studies with blinded outcome assessments were included there remained a moderate clinical effect (d = -0.39 [95% CI -0.75, -0.03]). However, it is difficult to generalize findings from intervention studies (where patients may be motivated to seek treatment/help) to community based descriptive studies of participants living with chronic conditions. Epidemiologic studies of community samples provide support only for PA as a protective factor against developing depression (Camacho, Roberts, Lazarus, Kaplan, & Cohen, 1991; Farmer et al., 1988).
Although intervention evidence supports a causal role, dose response relationships appear uncertain, and underlying mechanisms remain unclear. Changes in brain neurotransmitter activity as a result of physical activity, particularly central monoaminergic activity, appear to be the most biologically plausible mechanism because altered central monoamine functioning is consistently associated with physical activity (Meeusen, 2006), mood elevation, and anxiolytic outcomes (Krishnan & Nestler, 2008). The mechanisms implicated in the relation of physical activity to affective disorders are likely to involve a complex synergy of biologic, metabolic and psychosocial pathways that may be difficult to disentangle, particularly in human models (Mutrie, 2000). Also, there is limited research on how underlying mechanisms vary across different chronic diseases (e.g., CVD, obesity, diabetes).
Prior research on the intersection of medical diseases, depressive symptoms, and physical activity has certain limitations. Many studies on mediators of the disease-depression link have focused on a single medical condition, rather than a range of medical problems. Inclusion of multiple medical conditions in one study allows for comparison of the extent to which a potential mediator, such as physical activity, may have varying levels of impact on the association of depressive symptoms with physical health conditions. In addition, assessment of physical activity has often failed to measure varying intensity levels of reported activities adequately. Data suggest the importance of taking into account the level or intensity of physical activity (walking, moderate, vigorous), as different levels of intensity may have different effects on physical and mental health (Dunn, Trivedi, & O’Neal, 2001).
To address those gaps in the literature, the present study examined the association among depressive symptoms, chronic medical conditions, and physical activity in a sample of Latinos living along the U.S.-Mexico border in San Diego County. Seven common medical conditions were assessed (diabetes, cardio-related disease, hypertension, asthma, cancer, arthritis, and sleep problems), and physical activity was assessed at two levels of intensity (leisure-time moderate and vigorous physical activity). We hypothesized that (1) individuals with medical problems will report higher levels of depressive symptoms than those without medical problems, and (2) physical activity (leisure-time moderate and vigorous physical activity) will mediate the relation between medical conditions and depressive symptoms. In other words, it is expected people who report having a medical condition and engage in physical activity will report lower depressive symptoms.
Methods
The San Diego Prevention Research Center (SDPRC) contracted with the Social Science Research Lab (SSRL) at San Diego State University to conduct a random digit dial telephone survey from July through December 2006 with Latinos from two cities in South Bay, San Ysidro and National City. Percentages of Latinos residing in San Ysidro and National City were 89% and 59%, respectively. A list of telephone numbers was purchased that included Hispanic-surname households living in five zip code regions: from this list, 13,368 names were randomly sampled. To be eligible, participants had to be between 18 and 69 years of age, self-identified as Hispanic or Latino, and live in one of the two target regions. Of the 13,368 numbers called, 36% (n = 4757) were invalid, and 29% (n = 3899) participants did not answer the phone or were never assessed for eligibility. Once contact was made, staff confirmed inclusion criteria and gave respondents a choice to be interviewed in either English or Spanish. Of those contacted (n = 4713), 51% (n = 2418) were ineligible to participate, and 33% (n = 1579) refused or terminated the call prior to completion, and 106 (2%) spoke a language other than English or Spanish. Following these procedures, the sample size reached 610; however, an additional 62 interviews were completed using a snowball technique, in which a second adult in the household completed the interview after the first respondent was finished, bringing the sample size to 672 completed interviews. The research was conducted in accordance with the standards of the Institutional Review Board of San Diego State University and the University of California at San Diego for the ethical treatment of human subjects.
Measures
Medical conditions
Participants were asked several Behavioral Risk Factor Surveillance System (BRFSS) questions on physician-diagnosed health conditions: diabetes, cardio-related disease, hypertension, asthma, cancer, arthritis, and sleep problems. Response options were either 1 (“yes”) or 0 (“no”).
Depressive symptoms
The Patient Health Questionnaire-2 consists of two questions that assess the presence of anhedonia and dysphoria (Kroenke, Spitzer, & Williams, 2003). Participants are asked: “Over the last two weeks, how often have you been bothered by any of the following problems: 1) little interest or pleasure in doing things? Or 2) feeling down, depressed, or hopeless?”. The response options include: “1 = not at all” to “4 = nearly every day”. The PHQ-2 has reported to have adequate construct and criterion validity (Kroenke, et al., 2003), and it has been used with Latinos (Li, Friedman, Conwell, & Fiscella, 2007). In addition, in this study, the PHQ-2 score was cross-checked by asking respondents if they had physician-diagnosed depression (r = .29 p < .001). Because the depression variable was highly skewed, participants who reported no symptoms were categorized as ‘0’; those who reported one symptom were categorized as ‘1’ and those who endorsed experiencing both symptoms were categorized as ‘2’. The questions were translated and back-translated into Spanish by our team.
Physical Activity
The long version of the International Physical Activity Questionnaire (IPAQ) assessed the frequency and duration of moderate intensity, and vigorous intensity physical activity for occupational purposes, house and yard work, transportation, and leisure purposes during the last seven days (Craig et al., 2003). The IPAQ probes individuals to report moderate and vigorous activity level. Instructions for reporting vigorous activity state:
Think about all the vigorous activities which take hard physical effort that you did in the last seven days. Vigorous activities make you breath harder than normal and may include heavy lifting, aerobic, or fast bicycling. Think only about those physical activities that you did for at least 10 minutes at a time.
Instructions for reporting moderate activity state:
Think about the activities which take moderate physical effort that you did in the last seven days. Moderate physical activity makes you breathe somewhat harder than normal and may include carrying light loads, bicycling at a regular pace, or doubles tennis.
Because of its aggregate benefits compared to non-leisure time physical activity (West Suitor & Kraak, 2007), the current study focuses on leisure time moderate and vigorous intensity physical activity. Because a large percentage of participants reported not engaging in any activity, thereby impacting the distribution of the variable, physical activity was categorized into engaging in any activity (‘1’) or not (‘0’), for each intensity level.
Data analysis
Polychotomous logistic regression models were estimated to examine associations between depressive symptoms (dependent variable) and medical conditions (independent variables). Because significant differences in medical conditions between people who reported no depressive symptoms and those reporting two symptoms emerged, follow up logistic regression analyses were conducted with these two groups. Thus, the dependent variable was categorized into having no symptoms (‘0’) or endorsing both symptoms (‘1’). We assessed whether physical activity mediated the relation between medical conditions (predictors) and depressive symptoms (criterion variable) using a series of logistic regression models. Following the procedures recommended by Baron and Kenny (Baron & Kenny, 1986), mediation was identified as present if the relation between the independent and dependent variables was significantly attenuated when the potential mediator was entered into the model. All analyses were adjusted for socio-demographic characteristics (i.e. employment status, income, education, and age), and an alpha of .05 was used in all analyses. Analyses were conducted in SAS 8.02 (SAS, Cary).
Results
Approximately 61.01% of participants reported engaging in leisure time walking, 42.71% reported engaging in leisure time moderate levels of physical activity (vs. 57.29% who did not report any moderate leisure time PA), and 35.42% reported engaging in leisure time vigorous physical activity (vs. 64.58% who did not report any vigorous leisure time PA). Close to 40.33% of participants reported having no depressive symptoms and 31.48% (n = 210) report having two symptoms. The depression variable was dichotomized according to the guidelines (Whooley, 2006).
Demographic characteristics
Table 1 displays the demographic characteristics of those who were included in the analysis (n = 479; endorsed no depressive symptoms vs. endorsed two symptoms of depression) compared to the entire sample (n = 672).
demographic characteristics of study participants who were included in the analyses compared to the larger sample
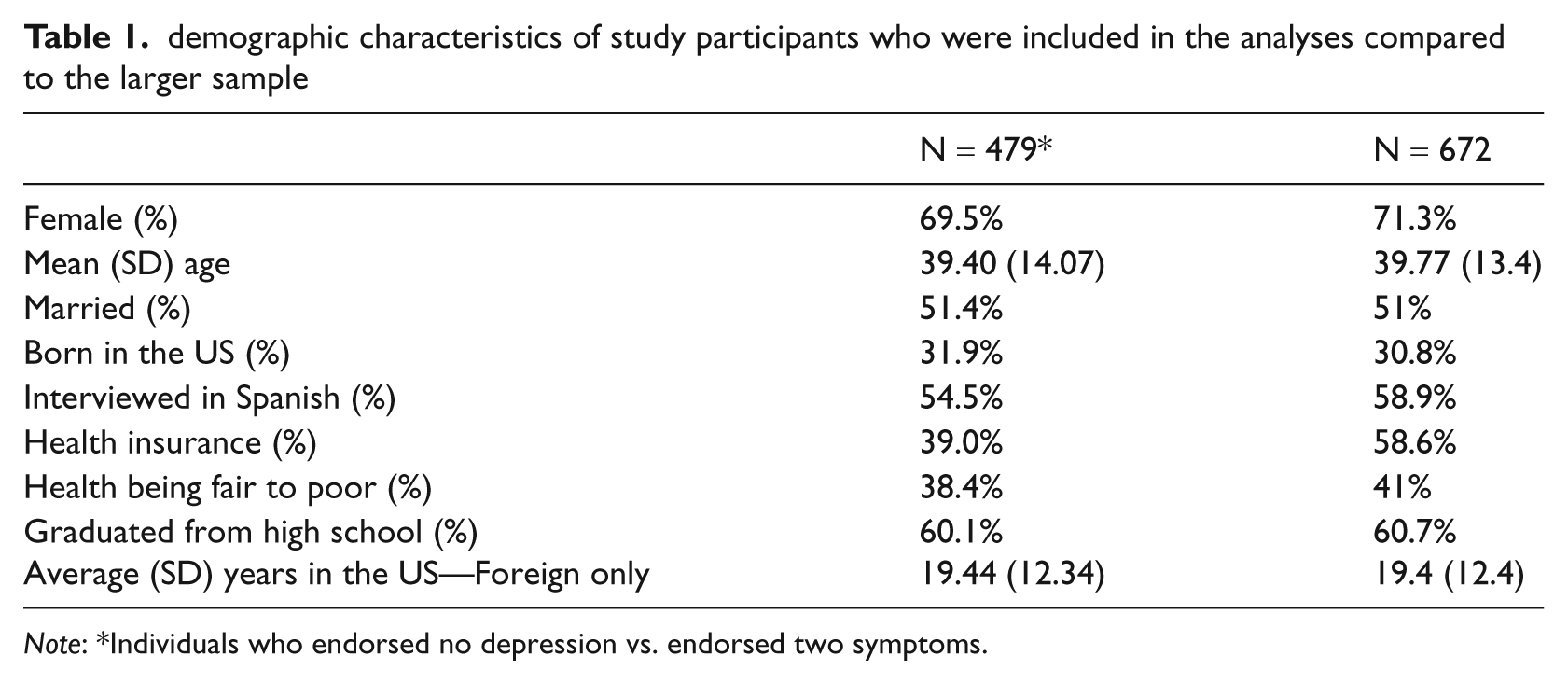
Note: *Individuals who endorsed no depression vs. endorsed two symptoms.
Are depressive symptoms related to medical conditions adjusting for socio-demographic characteristics?
The more prevalent diseases reported by the participants included sleep disorders (22.36%), hypertension (22.35%), high cholesterol (19.94%), cardiovascular diseases (5.52%), arthritis (19.55%), diabetes (11.31%), and asthma (8.04%). Approximately 3.28% reported being diagnosed with cancer; due to the low prevalence of this disease, cancer was excluded from the logistic regression analysis. To examine the association between medical conditions and depressive symptoms, logistic regression models were estimated separately for each of the seven most prevalent diseases. Table 2 shows that the odds of various medical conditions were greater among those endorsing depressive symptoms: diabetes (OR = 3.63, 95% CI = 1.72–7.66), cardio-related diseases (OR = 3.17, 95% CI = 1.13–8.92), hypertension (OR = 1.78, 95% CI = 1.01–3.14), high cholesterol (OR = 2.54, 95% CI = 1.40–4.63), arthritis (OR = 2.33, 95% CI = 1.28–4.23), and sleep problems (OR = 2.99, 95% CI = 1.75–5.09).
Associations between medical conditions and depressive symptoms

Note: Analyses adjust for employment status, income, education, and age.
Is physical activity related to depressive symptoms adjusting for socio-demographic characteristics?
Leisure time vigorous physical activity (OR = .57, 95% CI = .35–.93) was inversely related to depressive symptoms. In other words, those who endorsed depressive symptoms were half as likely to engage in leisure-time vigorous PA. In contrast, depressive symptoms were not significantly associated with leisure time moderate physical activity. As a result, we only examined vigorous activity as a mediator.
Are medical conditions related to physical activity adjusting for socio-demographic characteristics?
The associations between vigorous activity and the following health problems: diabetes, cardiovascular-related diseases, hypertension, high cholesterol, arthritis, and sleep problems were assessed adjusting for employment status, income, education, and age. Only, hypertension (OR = .52, 95% CI = .29–.94) and arthritis (OR=.53, 95% CI=.28-.99) were significantly associated with leisure time vigorous physical activity.
Analysis of mediation
To test the hypothesis of mediation, four multiple regression models were estimated with the criterion variable (depressive symptoms), adjusting for socio-demographic factors. The same series of models were estimated separately for hypertension and arthritis. In the first step, the likelihood of experiencing depressive symptoms was regressed on having been diagnosed with a medical condition (hypertension or arthritis). In the second step, leisure time vigorous physical activity was regressed on depressive symptoms. In the third step, leisure time vigorous physical activity was regressed on having been diagnosed with a medical condition (hypertension or arthritis). The final model tested whether the association between having a medical condition (hypertension or arthritis) and depressive symptoms was mediated by leisure time vigorous physical activity. When vigorous physical activity was entered in the model, the association between hypertension and depressive symptoms was no longer significant, suggesting full mediation. Leisure time vigorous activity did not mediate the relation between arthritis and depressive symptoms (see Figure 1).
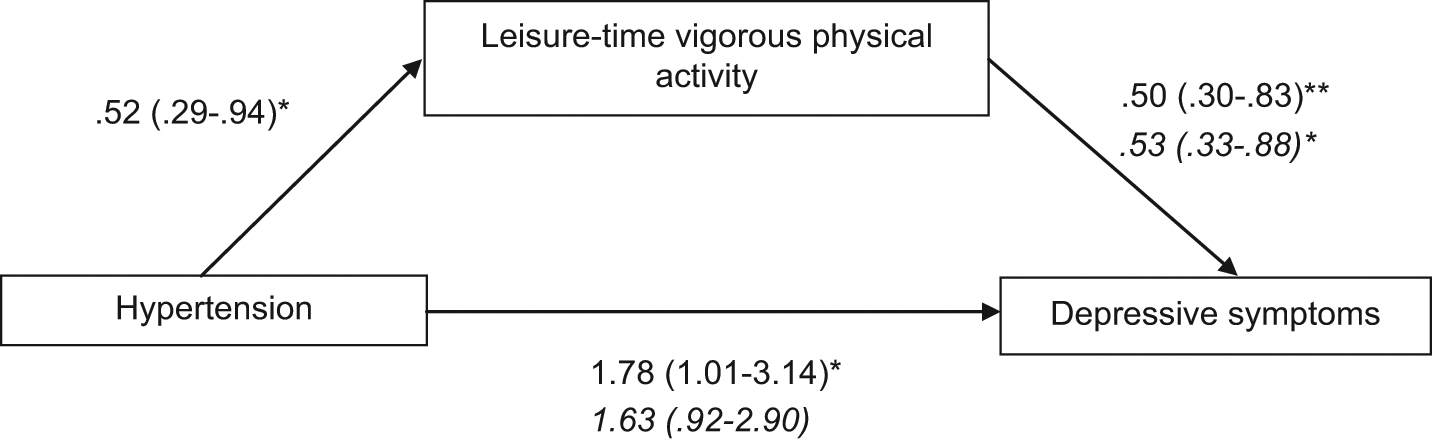
Mediation
Discussion
Chronic medical conditions are associated with depressive symptoms and physical activity may have beneficial effects on mental and physical health outcomes. However, mechanisms linking physical health problems, depressive symptoms, and physical activity have only recently begun to be elucidated in the research literature (e.g., Whooley et al., 2006), and those factors have not previously been explored among U.S. Latino populations to our knowledge. Our findings suggest that a range of common physical health problems are associated with depressive symptoms among Latinos, findings consistent with prior research (Lu, 2011). Reduced vigorous leisure-time physical activity also mediated the relation between hypertension and depressive symptoms in our sample.
We found that diabetes, cardiovascular-related diseases, hypertension, hypercholesterolemia, arthritis, and sleep problems were all positively associated with depressive symptoms, consistent with prior literature (Patten, 2005). It is unclear whether an association between asthma and depressive symptoms would become evident with a larger sample size. Physical activity was inversely associated with depressive symptoms and with hypertension and arthritis. Those associations remained after adjusting for potential confounders, such as employment status, income, education, and age. Studies have consistently shown that individuals from low socio-economic backgrounds and who are older are at greater risk for health problems (Lorant et al., 2003).
Observational and quasi-experimental studies have demonstrated that leisure-time physical activity has mitigating effects on depressive symptoms and that these effects may vary based on the level and frequency of physical activity in which an individual engages (Dunn, et al., 2001). In this study, vigorous leisure-time physical activity fully mediated the association between depressive symptoms and hypertension among Latinos. In other words, lower levels of vigorous physical activity accounted for the association between hypertension and depressive symptoms. Research identifying reasons why hypertensive individuals are not currently engaging in more vigorous physical activity is critical for understanding the mechanisms involved and for developing interventions to promote increased physical activity. Moderate physical activity did not mediate the relation of hypertension and depressive symptoms, suggesting that it may be important to target more vigorous levels of activity when promoting enhanced physical and mental health among hypertensive Latinos. One disconcerting finding from this study was the low percentage of participants engaging in any leisure time physical activity. Our data are consistent with national trends of physical activity among Latinos (Ham, Yore, Kruger, Heath, & Moeti, 2007) and highlight the need for programs to promote physical activity among Latino populations.
It is noteworthy that physical activity did not mediate the association between other physical conditions (e.g., arthritis, cardio-related disorders) and depressive symptoms in analyses controlling for demographic factors. Prior studies in which physical activity mediated or moderated the disease-depression used clinical samples (Brummett, et al., 2003; Whooley, 2006) or assessed 10-year longitudinal outcomes among elders (Kamphuis, et al., 2007). Physical activity may play a more active role in the disease-depression link among medically ill or elderly samples than community samples. Future research should explore other potential mediators that may explain the associations we observed between depressive symptoms and medical conditions other than hypertension. Rejeski and colleagues (2001) found that satisfaction with physical appearance and self efficacy mediated the relation between physical activity and self report well being. To impact the relation between physical activity and health, interventions may also consider targeting the mediating mechanisms between these two factors. In addition, vigorous physical activity was negatively associated with arthritis and hypertension. It may be that individuals who engage in vigorous activity are more physically fit and less likely to have arthritis or hypertension. Additional studies are needed to examine this hypothesis.
Findings from this study are consistent with other work showing that physical activity has important links to mental and physical health (Penedo & Dahn, 2005). Engagement in physical activity has been found to reduce chronic disease incidence (Kruk, 2007; Stewart et al., 1994). Physical activity may also help to alleviate depressive symptoms directly or indirectly through improved self-care behaviors (Taylor, Sallis, & Needle, 1985) and increased endorphins (Fraioli et al., 1980). Evidence suggests that physical activity has benefits for reducing depression and emotional distress among samples of different ages and cultures (Adams, Moore, & Dye, 2007; Brown, Ford, Burton, Marshall, & Dobson, 2005; Camacho, Roberts, Lazarus, Kaplan, & Cohen, 1991a; Lindwall, Rennemark, Halling, Berglund, & Hassmén, 2007; Wise, Adams-Campbell, Palmer, & Rosenberg, 2006). Preliminary evidence suggests that physical activity may also have beneficial effects on emotional well-being and depression among Latino adolescents (Brosnahan, Steffen, Lytle, Patterson, & Boostrom, 2004) and youths (Crews, Lochbaum, & Landers, 2004). Among Latino adults, physical activity has been associated with positive health behaviors, including fruit and vegetable consumption (Kieffer et al., 2006), and successful management of diabetes (Wood, 2004). Health promotion programs that aim to promote physical activity among underserved communities may tailor the health promotion strategies to the needs of the target population (Hardy & Grogan, 2009). The health care setting may be an effective setting to encourage individuals with medical conditions to engage in physical activity. Previous research has found that primary care staff can influence the physical activity of patients (O’Sullivan, Fortier, Faubert, Culver, Blanchard, Reid & Hogg, 2010).
This study has certain limitations. Given the cross-sectional study design, we cannot determine the etiology or causal direction of the observed effects. It may be that depression diminishes physical activity, in which case the association between hypertension and physical activity would be mediated by depressive symptoms. This seems equally plausible and there is ample empirical and clinical data to suggest that people who are depressed, due to their lack of motivation, engage in less physical activity (Roshanaei-Moghaddam, Katon, & Russo, 2009). In fact, there appears to be a bi-directional relation between physical activity and depression in general. Furthermore, physical activity may be enabled by better health. Post hoc analyses of the present data suggest that depression did not mediate the association between hypertension and vigorous physical activity. However, our data cannot address whether physical conditions gave rise to depressive symptoms or vice versa, or whether other variables (e.g., genetic or behavioral risk factors) may have caused both the physical and mental difficulties. Future research using prospective longitudinal designs should explore those questions among Latino samples. Moreover, the use of a two item measure of depression and categorization of the physical activity question may have reduced the power to detect the association between physical activity and depressive symptoms as well as compromised the validity of the instruments. Also, self-reporting of medical conditions and depressive symptoms may be subject to misclassification or bias (Wu, Li, & Ke, 2000). Similarly, social desirability factors may result in an overestimation of engagement in physical activity by study participants (Marin & Marin, 1991). This study examined physical activity as a potential mediator of the relation between medical conditions and depressive symptoms but did not assess other potentially important mediators, such as social support, self efficacy, quality of life, or biological factors. Our findings cannot be assumed to generalize to all Latinos in the U.S. given that the response rate in the study was low, and recruitment methods precluded the enrollment of individuals without land-line phones, who are more likely to be low income. Those factors may have biased the composition of our sample, arguably resulting in the exclusion of the most disadvantaged individuals (e.g., the most depressed and/or most medically impaired).
These limitations notwithstanding strengths of this study include a large community sample of Latinos in the U.S. To our knowledge, this is the only study to examine the relation between multiple chronic medical conditions and depressive symptoms among U.S.-dwelling Latinos, as well as the potentially mediating role of physical activity at different levels of intensity. Our findings suggest associations between physical and mental health among Latinos, as well as an inverse relation of physical activity with depressive symptoms and with certain chronic physical problems (hypertension, arthritis). Mediation of the relation between hypertension and depressive symptoms by vigorous physical activity suggests that interventions focused on increasing vigorous physical activity may be effective for addressing those problems among Latinos.
Footnotes
Acknowledgements
The San Diego Prevention Research Center is a member of the Prevention Research Centers Program, supported by the Centers for Disease Control and Prevention cooperative agreement 5-U48-DP-000036.