
Abstract
Two purposive case studies illustrate the role of habits and routines in illness management and how they are addressed in the clinical encounter. We argue habits and routines are related, but distinct constructs, and that by overlooking habits and routines, providers may be missing key opportunities to influence behaviour change. Utilization of ‘habit-changing’ professionals or health coaches who have the opportunity to communicate with patients on a regular basis in their daily living environment is proposed.
Although effective medical and life-style management of hypertension can reduce the risk of adverse outcomes, uncontrolled hypertension remains a persistent problem. Currently, 32 million Americans are at risk for the serious consequences of uncontrolled hypertension. Positive hypertension self-management includes adherence to medication regimens and life-style recommendations such as engaging in moderate intensity exercise, reducing smoking, decreasing alcohol intake, reducing sodium and losing weight (Egan et al., 2010). Interventions have not been sufficient to promote sustainable behavioural change because they focus primarily on the individual, assume that people make conscious and intentional choices, and neglect the ways in which patients modify and adapt health management behaviours within the context of their daily lives (Aarts et al., 1997; Chapman and Ogden, 2009). People who have chronic illnesses, such as hypertension, are asked to make changes to the daily habits and routines that have been part of their lives for years. Yet the role of habits and routines is silent in interventions designed to promote self-management of chronic diseases (Charmaz, 2002).
The dominant theories for changing health behaviour focus on social cognition- changing an individual’s health beliefs and attitudes in order to motivate the person to intentionally engage in health promoting behaviours (Marks, 2008; Marks et al. 2011). Chapman and Ogden (2009) note that behaviour change requires changing cognitions to overcome entrenched habits. Stage theories of health behaviour and self-regulation models suggest that intention and effort are essential to behaviour change. Thus, many interventions use education about the disease as a motivational strategy to change people’s decision making about their actions, their beliefs about action outcomes (health belief models) or their behaviour responses without careful consideration of their habits and socio-cultural contexts (Chapman et al., 2009; Orbell and Verplanken, 2010). These approaches assume that the problem resides with the patient, yet habits and routines are not simply internal or external to the patient (Garrison, 2002). Rather, humans acquire their habits from their context, and human habits may be understood only in their culturally situated and socially constructed contexts (Dewey, 1922).
Intervention effectiveness studies document that education about hypertension management is necessary but insufficient in changing daily behaviours to control hypertension (Kok et al., 1997). Wood and Neal (2007) argue that even when the person has clear intentions to act otherwise, actual behaviour change is often difficult because habitual behaviours are shaped by our cultural and social contexts. When habits are strong, people are less likely to change behaviour based on new information. Habits are well-practiced action sequences that are unconscious and automatically cued by stimuli in the environment. Once habits are developed, perception of the context automatically activates mental representation of the response (Aarts and Dijksterhuis, 2000). For example, familiar routines such as watching television while eating dinner may activate a habitual automatic response to overeat. Thus, routines and habits are difficult to change.
Although routines have been addressed in literature related to specific populations (e.g. older adults and their caregivers, people with cancer or HIV), explicit attention to routine and habit change is remarkably absent from interventions for improving control of hypertension (Zisberg et al., 2007). The goal of our research is to understand how patients manage their hypertension in their everyday lives. In this article we examine how habits and routines mediate patients’ self-management of hypertension. We present two illustrative cases to argue that these constructs are central to patients’ self-management of chronic disease. We analyze excerpts from patient interviews and patient-provider interactions to examine the extent to which providers consider habits and routines in disease management and suggest that by overlooking habits and routines, providers may be missing key opportunities to influence patients’ behaviours and improve hypertension control.
Habits and routines
Habits and routines are distinct, yet, interrelated constructs. The two constructs are often confused and used interchangeably to describe repetitive, predictable patterns of behaviour in daily life. Adding to the confusion, both terms are conceptualized and used differently across disciplines (Clark et al., 2007; Wood et al., 2002; Zisberg et al. 2007). Routines are more typically viewed as “organized activities with purpose, direction, sequence, outcomes, and repetition, but at least for a time, they may require considerable attention. Yet, routines are not always habitualized modes of responses and not all habits are routines” (Charmaz, 2002: 31S). Zisberg et al. (2007) suggest that “routines are used to coordinate activities along different axes of time, duration, social and physical contexts, sequence and order” (442). Routines are considered to be essential to everyday life and to managing chronic illness. Fiese’s (2005) research with families provides one example of the link between routines and health outcomes. She documented that routines help families create structure to develop effective asthma management strategies, which contribute to improved adherence to recommended medication protocols and quality of life.
One distinction between routines and habits is that routines are what people do; therefore they are more easily observed. For example, we can easily observe someone’s daily routines for cooking breakfast. Habits, on the other hand, are more than repetitive actions; they are ways of being that are so automatic and without reflection that it is often difficult to observe a habit until it is disrupted. For example, we may be unaware of the habit of always “needing to plan ahead” until we are confronted by illness and unable to maintain this way of being in the world. Dewey views habits as transactional and posits that habits are “functions acquired from both natural and social dimensions of our habitats that provide a means to an end” (Cutchin, 2007: 52S).
Dewey (1922) suggests that habits are acquired predispositions that enable people to respond to their situations with economy of thought and action. As people develop within various contexts, they unconsciously internalize predispositions (or habits) inherent to the social structures and prevailing cultural schemas that guide our thoughts, values and behaviours. These predispositions are acquired through our experiences of doing and being and contribute to our selfhood. These dispositions have also been described as a combination of inclinations, sensitivities and abilities. The habit of being a perfectionist and always trying to do one’s best is an example of this view of habit.
Habits are socially constructed, acquired through experience in contexts or habitats of doing and being, with the social context being a significant influence. Thus, our knowledge, motivations and behaviours influence and are influenced by the physical, social and cultural contexts that shape the self and others. Yet, Garrison (2002: 12S) explains, “habits are not in a context as marbles are in a jar”. Rather, our habits are embedded in our context and we cannot separate ourselves from our context. As humans respond to social signals in the environment and derive meaning from social interactions, we unconsciously internalize predispositions (habits) embedded in these social structures.
In this article, we view habits as a constituent or component of routines. Habits may be described as unconscious and embedded thoughts and actions linked to our social and physical world, with routines emerging from our habits. Thus, routines may be considered a ‘kind of habit’, a higher order habit that specifies what people do and in what order. For example, we may develop a routine for reviewing the directions to an unfamiliar destination because we have a habit of being a perfectionist and strive to avoid being late when going to an unfamiliar location. We use these ideas about habits and routines to argue that managing hypertension is both habit and routine-based.
Methods
Qualitative methods are particularly well suited to exploring previously unidentified phenomena. This article is based on data collected in a study focused on understanding the roles of explanatory models, social context and patient-provider communication on patients’ self-management of hypertension. We did not set out to explore patients’ habits and routines. Rather, the importance of these constructs emerged through our analysis of the patient interview narratives. Patients were asked about their daily lives, social context and hypertension management and, through analysis of these aspects of the narratives, we identified two key constructs of habits and routines that are discussed in this article.
Participants and recruitment
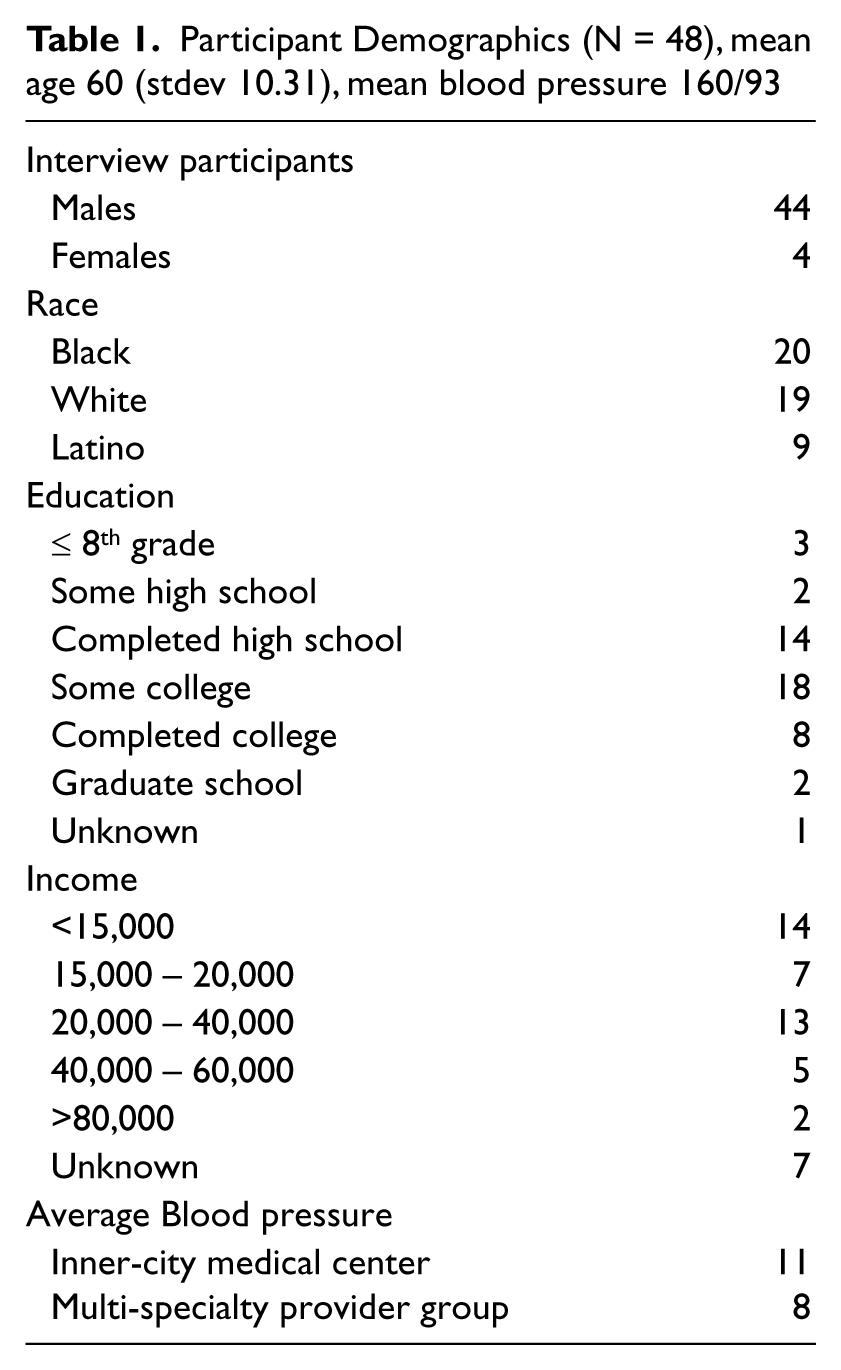
A purposeful sample of adults with uncontrolled hypertension and their primary care providers were recruited from two Veterans’ Affairs Medical Centers, one in the Northeast, one in the Southwest (see Table 1 for demographics). The institutional review board at each site approved the study.
Participant Demographics (N = 48), mean age 60 (stdev 10.31), mean blood pressure 160/93
Based on the assumption that they regularly treated adults with hypertension, all primary care providers at each site were eligible to participate. A study investigator presented the study to providers at staff meetings at each clinical site, asked for participation and obtained informed consent. The providers were told that the study focused on how patients understand and manage hypertension and on the patient- provider communication about hypertension.
Eligible patients were identified via the healthcare system’s electronic medical record and were eligible if they had one documented instance of high blood pressure (BP) (140/90 or above) in the six months before their participation in the study and had a BP reading above 140/90 on the day of the clinic visit. A research assistant (RA) called patients prior to their next appointment to invite participation. The patients were told that the study focused on how providers talk to patients about high-blood pressure and how they understand and manage their hypertension. When the patients came to the clinic for their appointments, the RA assessed BP, administered eligibility screening, demographic questions, took blood pressure readings and obtained written informed consent. The study was conducted between February 2007 and June 2008.
Data collection
We audio-recorded the clinical encounter between the patient and provider via a digital recorder set up in the exam room during regular primary care visits. Patients were given a $5.00 gift card for their initial participation.
Within two weeks of the clinical visit at which the patient was recruited, the RA conducted semi-structured qualitative interviews with each patient. Patients were given another gift card for an additional $20.00 for their participation in this interview. During the one and a half hour semi-structured interview, patients were asked to describe their family, a typical day, experiences living with a hypertension, their beliefs about hypertension, their last appointment with their provider, and the medications and strategies they used to manage their hypertension. All recorded interviews were transcribed verbatim by a professional transcription service. The interview transcripts were then reviewed by the research assistant to ensure accuracy and entered into the NVivo software program for organization and coding of interview manuscripts.
Data analysis
We used qualitative analytic techniques informed by grounded theory (Corbin and Strauss, 2008). A research team of five investigators (authors) began by open coding five transcripts together, identifying content and themes grounded in the language used by the participants. Through this process we generated a coding dictionary, which was refined and enhanced with coding of subsequent interviews. We then collapsed codes into broader categories informed by the instances in which patients discussed their daily behaviours with regards to hypertension and beliefs about hypertension and medications. Each subsequent interview was coded and reviewed by two investigators. We developed individual patient summary templates in which we described each patient’s beliefs about hypertension, social context, hypertension management behaviours and perceptions of clinical encounters. Each template was completed by two investigators and then reviewed by the entire team to establish consensus and conduct constant comparison analyses across cases to explore similarities and differences in patients’ reported routines and beliefs about hypertension.
In the analyses for this article, we identified segments in which patients made statements about the actions and activities related to how they live their daily lives. We call these activities the ‘daily-lived experience (DLE)’. We then identified descriptions of daily routines and habitual ways of being in the world. For example, in one person’s interview, we coded his daily activity of eating at restaurants as a routine because eating at a restaurant is an organized activity, with an outcome and a behavioural sequence that can easily be observed. When he said “We all lived together, families lived together. You saw each other all the time, you had contact”, we coded this passage as habit. Later in the same interview, this patient told us “I’m not going to live like a monk”. This passage was also coded as habit. These descriptions of behaviour were coded as habit because they describe automatic ways of being in the world. We further analysed these passages to understand the roles of habits in mediating illness management and shaping daily behaviours or routines.
Subsequently, we conducted an analysis of the patient-provider interactions to examine the ways in which the interactions unfolded. Two investigators coded each transcript to develop consensus in identifying segments where patients or providers discussed the patients’ DLE, including routines and habits. We then compared the information and perspectives provided in the patient-provider interactions with information and perspectives provided in the patients, interviews.
These cases are situated within a setting, limited by time and place, and are not representative of all patients with uncontrolled hypertension. Rather than suggesting generalizability, we present these cases as examples to illustrate a way of thinking about the role of habits and routines in the daily management of hypertension. These cases were selected because they both provide examples of the role of routines and habits in managing hypertension, yet the provider’s response to the patient’s contextual cues varied.
Findings
Patients described a range of daily life styles and hypertension management behaviours, including structured lifestyles, living and working on a boat, or avoiding medications while drinking alcohol and then doubling up on medications while not drinking. In most recordings of the clinical encounters, providers reminded patients to take medications and warned of the dangers of uncontrolled hypertension. Patients’ daily routines for managing hypertension were discussed in only a few instances, primarily focusing on routines for medication taking, avoiding salt or the benefits of exercise. In contrast, in the interviews with veterans we recurrently heard stories that illuminate the habits and routines that interfere with hypertension management.
The social role of habits is evident in Dale’s story. A 72-year-old veteran with uncontrolled hypertension, Dale lives alone in an urban environment. He was an art director whose job was eliminated the previous year. Since that time, he reported that he “hasn’t been doing anything”. When asked to describe a typical day, Dale said:
I really don’t do any designing anymore. I was always coming up with ideas, always. But once they let me go it was like I felt that I became impotent. When you’re an art director, you know, you’re in charge. You set up shoots, you hire models, you hire photographers. And people come up to you and call you up and want to take you out. They want to schmooze with you. Then all of the sudden, you’re not doing anything. So I’m not working. I would like to be doing something productive. I’d like to be doing something creative, which I’ve done all my life. I have nothing, there’s nothing to be creative about. It’s very boring. And so now, I get up late. Well I tell you what; I play poker at night, mainly because I am bored because I have nothing else to do. And you meet people there. … I socialize a little bit.
When asked about his diet, Dale’s response implied that he is cognizant of the recommendation to reduce salt intake to manage his hypertension:
If I cook for myself, which is very rare, I don’t use salt. But, when I go to restaurants, sometimes there’s no control of what you’re eating. I will tell them, like when I go to the club to play poker, we have food there, ‘Don’t put any salt on my food’.
Dale’s story highlights that his former habits arose from his everyday activities and were patterned through his social relationship and work routines. His habitual way of being in the world is marked in his discourse by the way he uses words in the following sentences:
When you’re an art director, you know, you’re in charge. You set up shoots, you hire models, you hire photographers. And people come up to you and call you up and want to take you out. They want to schmooze with you. (our emphasis)
In these sentences Dale is talking about himself, but using a generic ‘you’. Rather than a pronoun, he uses the word you as a stative verb. Stative verbs describe a state or condition of someone or something; they have no distinguished endpoint, and they denote a state rather than an action. Even though Dale no longer works as an art director, he vividly describes the experience of being an art director. Dale does not use the first person, such as “I used to hire models” to tell the interviewer what actions he performed as an art director. Rather, the generic form of ‘you’ conveys his habitual state. Linguists might call this form of language a “durative aspect marker”, “a form that means that an action or event is a regular event, happens over and over, and is characteristic or typical” (Gee, 2011: 3). Dale’s use of ‘you’ is his way of communicating his expectation of work life, which in turn helps to dramatize the change in his circumstances in his narrative—he is now unemployed and is yearning for engagement in meaningful activity. Dale’s language conveys his enduring habitual and characteristically social way of being in the world. Over the years, Dale was habitualized to working with others- being social, being in charge, being potent and being creative. Once he stopped working, these habitual and long standing ways of being in the world disappeared. He has established new routines, activities directed toward meeting his ingrained lifetime social habits. He plays poker to interact and “schmooze” with other people, which sustains his habit of socializing. Yet this routine, playing poker to socialize, conflicts with his hypertension management and ability to control the sodium in his food, a recommended strategy to lower blood pressure. Beyond poker, Dale has few opportunities to socialize. Thus, playing poker is an important and meaningful activity for Dale. Perhaps, at this moment in Dale’s life, playing poker and socializing is more important than managing his hypertension.
Dale’s interaction with his provider offers an instructive view of how routines enter into the clinical dialogue without sufficient attention to Dale’s daily-lived experience. The provider conveys compassion in his interaction with Dale and probes to understand Dale’s routines. The provider opens his interaction with Dale by asking a broad open-ended question, “How are you today?” Dale responds by explaining that he “doesn’t understand what’s going on with his blood pressure”. The conversation then shifts to a review of when Dale last took his medicine. After the provider checks Dale’s blood pressure and explains that it is high, he asks Dale numerous questions about his daily routines, including medication-taking, diet and exercise routines. He asks Dale, “Tell me exactly what medicines you are taking and when and how many time a day”. Later in the encounter, the provider asks Dale what he has been eating lately, what his diet looks like and if he is adding salt to things. Dale explains that he never adds salt to anything but that he eats out a lot. The provider responds, “Okay, there it is, yes. That’s where a lot of salt might be coming from”. Dales explains his routine further:
I’ll say, ‘Don’t put the salt on it’. And then I do play poker at a place that has food, or that makes food. And I ask them, ‘Do not put any salt on anything you make me.’
The conversation then shifts to Dale’s blood pressure log, and the provider stops short of discussing Dale’s daily-lived experience and routine of playing poker. Later in the encounter the conversation returns to Dale’s medication routine as he explains that he gets up in the morning, takes his blood pressure and then takes his medication. As the appointment is coming to a close, the provider makes one more attempt to understand Dale’s hypertension management routines by asking Dale if he has been walking. Dale responds by sharing his former habitual way of being social in the world when he reveals:
I started a little while. You know, when my friend was in town I walked a little more than I usually do, but I haven’t really.
The provider than educates Dale by telling him that 30 minutes a day will get his heart rate up and that will be good for his blood pressure.
In contrast to Dale’s interaction with his provider, James’ provider does attend to his daily-lived experience and considers the role of habits and routines in his management of hypertension. When asked to tell us about his life, James, a 61-year-old Vietnam war veteran, immediately told us that his “life has been a terrible mess from the start”. His father died when he was three years old and his mother raised James and his siblings by doing whatever she could to make money to support her family. At the age of 15, James began to contribute to the family by learning to drive an 18-wheeler and helping out his stepfather. At 18, James’ girlfriend became pregnant, and, demonstrating his commitment to his family, he married her before he left for a tour of duty. When he returned from Vietnam he worked numerous jobs to support his wife and son. Now, James’ habitual disposition to help out his family creates a dilemma which makes it challenging to manage his hypertension. James explained the dilemma this way:
My son needs me a lot. He don’t pay me … but, I never know when he is going to need me. So, it seems like every time I’ve tried to make a schedule for anything, about that time he’ll get so busy and then I have to help him run a crew somewhere. Every time I try to schedule [exercise] he’s got 16 million things he needs me to do for him. And we do whatever we can for my son.
In this example, we learn that James’ predisposition to help his family developed at an early age because of the commitment to family his mother made. This predisposition has become of habitual way of being that guides James’ thoughts, values and behaviours. Helping his son interferes with his intention to schedule time for exercise (a routine) or meet with someone to address his weight. James makes a decision to work for his son rather than exercise because his overarching habit is to support his family above all else.
In contrast with Dale’s interaction with his provider, James begins his interaction by telling his provider about the pain he experiences while working on his house. He explains:
It hurts like crazy. I’m working on the house, and everything on me hurts. I feel like my eyelids hurt. I’m trying to rent my house, and I have to get ready for that and oh, I get up and down that stupid ladder. And I can’t do that but I am having to do it.
Rather than directing the conversation to James’ medical concerns and pain, his provider attends to James’ daily-lived experience by responding, “So, you want to rent your house?” James’ response illustrates, once again, the enduring influence of his habitual predisposition to help his family. He explained that he is renting his house because he moved in with his 90-year-old father-in-law. The provider, continuing to probe about James’ social world and daily life asks, “And, how is your daughter doing?” James tells the provider all about his daughter’s divorce and how he helped his daughter paint the bathroom in her new house. After more conversation about his daughter’s divorce, the conversation shifts to James’ medical concerns when the provider asks, “How are you feeling today?” He also asks James if he is taking his medication. Yet, rather than educating James about necessity to take his medication, monitor his diet and exercise, his provider appears to take into account the complexity of James, daily-lived experience and recommends that James attend a blood pressure clinic and work with a case manager.
Discussion
The case examples illustrate the enduring influence of habits and routines on behaviour. Dale’s habitual way of being social interferes with his ability to monitor his sodium intake. James’ habitual ways of helping his family create a dilemma. Helping his family trumps developing a schedule to exercise. Moving beyond a discussion of routines for managing hypertension, James’ provider attends to elements of the habits surrounding James’ daily life. Initially it is unclear that the conversation about James’ children might be relevant to this hypertension management. Yet, James’ provider allows him the time to discuss his current life situations, offering clues about his habits and routines. The provider then makes a recommendation to a case manger that can co-construct an intervention with James that considers how to integrate recommendations into his daily life.
Examining the role of both habits and routines in mediating the daily activities of persons with hypertension illustrates a conceptual link between habits and routines and disease self-management. We argue the patients’ habitual modes of being in the world will influence their daily routines, which may support or interfere with disease self-management.
These findings provide a novel perspective for considering alternative approaches to intervention. Education falls short because, at best, it only addresses routines in a superficial way. Rather than providing more education about the value of diet, exercise and medication, the task expands to understanding patients’ habitual modes of being in the world and attending to patients’ daily routines to understand their hypertension management behaviours. When hypertension management is explored in relation to routines and habits, providers have an opportunity to support patients to develop health-promoting routines congruent with their habitual way of being in their world. However, given that habits are contextually embedded and patients’ daily-lived experiences occur at home and in the community, intervention delivered in the hospital or outpatient clinic may be too disconnected from the realities of daily life. In order to build habits and routines into everyday activities, we must recognize that habits occur in a context and that health care professionals must attend to the context as well to the person. The patient-provider communication noted in Dale’s story is congruent with recent findings that document higher error rates when physicians do not attend to individual patient context and behaviours. Weiner et al. (2010) describe these errors as “contextual errors”—failures to tailor intervention care plans to a patient’s individual circumstances. Similarly, in their study of patient counselling by physicians on hypertension, Bell et al. (2008) noted that counselling about lifestyle was limited in value. Thus, we propose that viewing habits and routines in the context of the broader daily-lived experience is essential to promoting sustainable change. In addition to the biomedical tasks of managing the disease symptoms and prescribing the proper medications, we recommend listening for instances of habitual behaviour that may conflict with disease management. Once the behavioural patterns are identified, primary care providers can refer patients to interventionists who can collaboratively work with patients to design individualized long-term interventions that are embedded in their socio-cultural contexts (Haslbeck and Schaeffer, 2009).
Patients with chronic conditions, such as hypertension, may benefit from collaborating with “habit and routine-changing professionals” who have the opportunity to communicate with patients on a regular basis in their daily living environment. These “habit and routine-changing professionals” could be health psychologists, nurses, or occupational therapists, as practitioners in these disciplines have extensive training in understanding human behaviour in context and mechanisms for behaviour change. Habit changing professionals can help patients by analysing and making explicit the contingencies and consequences of habitual and routine behaviours and potential conflicts with hypertension management. Intervention involves building new routines that honour patients’ habitual ways of being in the world and allow people to manage their hypertension within the context of their daily experiences.
It is important to note that a highly rational model will not work, as we cannot change habits directly by appealing to reason alone. We cannot expect rationality to prevail with statements such as “Exercise more often”. Rather, we recommend understanding underlying patterns of habits by looking for patterns of daily lived experience, that is, “understanding how behaviour reflects the intersection between habits and situations in which they are expressed”, attending to context as well as person, and considering the constellation of circumstances in everyday life and broad social patterns (Swartz, 2002: 68S). Dewey (1922), an advocate of reflective learning, suggests that habits might be amenable to change through reflection—people are not determined by their context as long as they can critique it and reconstruct it. He suggests that, to shape the course of human behaviour, we seek to understand how habits interlink with conscious reflection. Thus, we recommend coupling reflection and attention to the context in which habits and routines are performed. Clark (2000), drawing from Dewey, recommends “creating situations in which the client has the opportunity to practice skills until they become automatic—the process of habit formation” (134S).
Finally, these findings raise the question of service delivery and how to best promote change. We are reminded that healthcare encounters are not decontextualized events, but are connected to the histories and habits and daily routines of clients’ lives. Hypertension is most commonly addressed in a primary care visit with a provider. These primary care visits are constrained by the limited time and multiple demands on physicians to rapidly form partnerships with patients, address biomedical and psychosocial needs, provide preventative care, coordinate care with specialists, and ensure informed decision making with patients (Bennett et al., 2010). We argue for public and private health insurance plans that reimburse for habit and routine changing interventions to address life style redesign beyond the 15 minute clinical visit (Fiscella and Epstein, 2008; Margolius and Bodenheimer, 2010). Lifestyle or health coaches, with an opportunity to have repeated interactions with patients over time, may be able to understand patients’ broader social worlds and habits, an understanding necessary to support life-style modifications required to manage chronic illnesses. Changes in payment models to reimburse for habit-changing health coaches who can intervene in the settings where people live are indicated. The findings of the current study support the necessity of health coaches, particularly if these coaches address how enduring habits and routines impact health management behaviours. This argument is consistent with recommendations for adjunctive therapy focused on life-style modifications, particularly if these therapies address how enduring habits and routines impact health management behaviours (Egan et al., 2010).
Limitations
This study has several limitations. First, although we make no claim of generalizability, it is noteworthy that this study was conducted with veterans, mostly men, and the findings may not be relevant for non-veteran populations. This study lays the conceptual foundation for more research, using varied methods and broader samples, to advance understandings of the mediating influence of routines and habits in management of chronic illness. The data is all verbal, without observation of patients’ actual daily behaviours in context. It would be helpful to observe patients in their natural context to gain a deeper appreciation for the potential influences on medication-taking behaviour, exercise and diet. This would provide further understanding of how people with hypertension successfully develop and maintain habits and routines in the course of their everyday lives. Despite these limitations, this study highlights the need for innovative approaches to addressing the health management needs of people with hypertension.
Conclusion
We have noted that, even when motivated and knowledgeable about recommended behavioural lifestyle changes, patients with hypertension often do not make those changes. We argue that daily habits and routines are often overlooked, yet they form a foundation for the daily behaviours that may either support or interfere with health promoting behaviours. Finding ways to help patients identify and make necessary changes in habits and routines may lead to improved health outcomes.