
Abstract
Limited studies have sought to describe binge drinking among adolescents and even fewer studies have attempted to examine whether family functioning, family communication and satisfaction could be associated with alcohol abuse. Our sample was made up of 726 Italian adolescents between the ages of 16 and 18. According to previous research, adolescents were categorized into non-drinkers, social, binge and heavy drinkers. Results showed that social, binge and heavy drinkers differ in terms of some drinking variables, family functioning, family communication and satisfaction.
Research has attempted to identify the cognitive factors involved in alcohol use and abuse. An important line of research has indicated the relevance of expectancies and beliefs about alcohol consumption as well (Carey, 1995; Johnson and Fromme, 1994; McNally and Palfai, 2001). Young people do not consider binge drinking as a significant problem: adolescents classified as binge drinkers define themselves as ‘occasional drinkers’.
Adolescents find it difficult to perceive binge drinking as negative (White et al., 1997) and fail to mention the long-term risks of this behaviour. This misrepresentation of alcohol misuse reduces the possibility for adolescents to understand the seriousness of drinking behaviour. Binge drinking is a dangerous activity associated with many social and health problems (LaBrie et al., 2011) and unfavourable outcomes, such as heavier use patterns, progression to other substances (Correia et al., 2003; Grant and Dawson, 1997; Gruber et al., 1996), impaired driving (DiGrande et al., 2000; Wechsler et al., 1994), dangerous sexual activity (Naimi et al., 2003), violence (Mohler-Kuo et al., 2004), crime and lost efficiency (Crawford and Novak, 2002; Hingson et al., 2006; Wersch and Walker, 2009), for example, poor academic performance (Callas et al., 2004). Although these alcohol-related harms, spirit use is a common practice among adolescents for fun, to be satisfied, to be cool, to be more extravert (social facilitation, sexual enhancement), to reduce tension or simply out of boredom (Broadbent, 1994). In particular, females tend to initiate binge drinking when they feel irritated or down and when they want to escape from their problems (Macneela and Bredin, 2010), whereas males are inclined to binge drinking when pressed by peers and to have fun (Wersch and Walker, 2009). Generally speaking, expectancies are better predictors of alcohol abuse where adolescents are concerned than they are where adults are concerned, besides, different expectancies can predict different drinking patterns (Urbàn et al., 2008).
Although research suggests binge drinking in adolescence is a relevant problem, not only young people but also adults fail to see it as a significant problem, alcohol being widely accepted in Western society and culture. The average age at which young people in Europe begin to drink has dropped as well as the quantity of alcohol consumed by youths has increased, especially in the United Kingdom (Moore et al., 2010).
Recent investigations have shown that alcohol use among adolescents is a relevant health problem in Italy where there is a continuing and growing concern regarding frequent and excessive alcohol misuse by younger people (Gallimberti et al., 2011). Recently, the Italian Government, in order to battle the growing problem of binge drinking and alcohol-related deaths, has adopted many measures, including zero tolerance for drivers and stricter controls at discos.
However, the level of risk among Italian adolescents appears to be lower than in other European countries (Beccaria and Prina, 2010). Among Italian adolescents aged 11–15 years, 18.6 percent report at least one experience of alcohol consumption in the last year, 1.4 percent experience alcohol use far from meals at least one time a week, while 2.1 percent claim an episode of drunkenness at least once in the last year. Two factors are particularly important in Italian context: 1) a slight growth (from 12.6% to 20.6% in general; from 9.7% to 16.8% for girls; from 15.2% to 20.2% for boys) in alcohol consumption far from meals among youths aged 14–17 between 1998 and 2006, and 2) the emerging change in the drinking alcohol style. Italian adolescents seem to leave the dry drinking culture to accept the wet drinking culture, in which the most important value is intoxication after high alcohol consumption (Beccaria and Prina, 2010; Scafato, 2010).
In Italy, binge drinking is not well documented yet. Little research has been conducted into binge drinking in Italy so far and those Italian studies that have focused on determinants of binge drinking have looked only at demographic variables, showing an increase of binge drinking both in boys and in girls (Gallimberti et al., 2011). Thus, state-specific estimates of binge drinking are essential to the planning and the implementation of strategies to prevent this particular form of alcohol abuse. Nevertheless, it is necessary to identify protective and risk factors involved in binge drinking phenomenon.
Family relationships and parents’ behaviours are central influences on adolescent activities and on the timing of alcohol use (Malkus, 1994; Laghi et al., 2009; Moore et al., 2010; Paxton et al., 2007; Spoth et al., 2002). Di Grande et al. (2000) argue that two factors are particularly important in predicting binge drinking in adolescence: a) onset of drinking in the family context and b) drinking outside the family context. These authors suggest that parental behaviour is relevant in explaining adolescent alcohol use and abuse. Adolescents who perceive their families to be extreme on cohesion and adaptability are more likely than adolescents from balanced and mid-range families to use alcoholic and drug substance (Smart et al., 1990).
According to Thomas and colleagues (2000), the availability of an income out of parental control is a potential risk factor for binge drinking. On the contrary, living with the family and having adequate parental monitoring are protective factors for adolescent binge drinking (Odo et al., 1999; Thomas et al., 2000). Furthermore, the effects of parenting style on adolescent drinking seem to vary across gender. In particular, the excessive parental control may increase alcohol use more in boys than in girls (Crawford and Novak, 2002).
The present study is aimed at thoroughly analysing the phenomenon and understanding the factors most frequently associated with binge drinking among adolescents. To sum up, this study intends to lay some groundwork for future research on student risk-taking behaviours and to provide example procedures for the investigation of these constructs.
The purpose of the study is to determine a drinking profile useful in discerning binge drinkers from social drinkers and heavy drinkers. The broad prediction is that a combination of alcohol positive expectancies and family functioning will be necessary in order to discriminate binge drinking adolescents from social and heavy drinking adolescents.
Methods
Participants and procedures
The sampling consisted of 726 participants (182 females; 544 males) between 16 and 18 years (M = 17.11; SD = .31). The subjects of the sample lived at home with their parents and were selected from high-schools in Rome, Italy, as well as voluntaries. High schools in Italy are divided into distinct educational and occupational fields and include five grade levels. In terms of type of high school, 23.4 percent of students were enrolled in science-focused schools, 20.7 percent were in technical-industrial arts schools, 22 perccent were in liberal arts-focused schools and 33.9 percent were in teacher-training schools. Participation was preceded by an informed-consent procedure that required active consent from both students and parents. The questionnaires were administered in the classroom during a regular class period and took approximately 40 minutes to complete. Instructions stated that the questionnaires were voluntary and that responses were anonymous and confidential. This survey was reviewed and approved by the Ethics Commission of the Department of Developmental and Social Psychology of Sapienza, University of Rome.
Measurement
Demographics and alcohol use/severity
An Identifying Information Form was used to collect demographic information. Drinking quantity and frequency were assessed using different questions: a) frequency of alcohol consumption, b) average number of drinks consumed per occasion in the last month and c) age when alcohol was first tried outside the family. Another item yielded information about drinking practices of friends and finally, the amount of alcohol friends who drink regularly was calculated. The specific wording of the question concerning binge drinking was as follows: ‘Considering all types of alcoholic beverage, did you have 5 or more drinks (4 if you are female) on one single occasion during the past month?How many times in the last month?’ Respondents were categorized as ‘binge drinkers’ (one to eight binge drinking episodes in a month) and ‘heavy drinkers’ (more than 8 binge drinking episodes in a month) (D’Alessio et al., 2006; Vik et al., 2000). According to previous research (Baiocco et al., 2010; D’Alessio et al., 2006; Morawska and Oei, 2005), respondents were categorized as non-drinkers (consuming alcohol less than twice per year), social drinkers (drinking ranging from three/four times a year to three/four times per month), binge drinkers (at least one but less or equal than 8 binge drinking episodes in a month), and heavy drinkers (more than eight binge drinking episodes in a month).
Drinking expectancies profile
The Positive Drinking Expectancy Scale (PDMS; D’Alessio et al., 2006), consisting of 12 items on a Likert scale (1 = disagree, 5 = agree), was used to assess beliefs concerning the positive effects of alcohol. Factor analysis revealed three different positive functions of alcoholic drinks: (a) sexual and behavioural disinhibition, (b) relief from pain, anxiety and stress, and (c) social confidence. Internal reliability of the PDMS ranges from 0.80 to 0.86.
Family Adaptability and Cohesion Evaluation Scales
Family Adaptability and Cohesion Evaluation Scales (FACES IV; Olson, 2011) is composed of 42 items on a Likert-type scale divided into six scales: two balanced scales (Cohesion and Flexibility) assessing central-moderate areas and four unbalanced scales (Rigid, Chaotic, Enmeshed and Disengaged) assessing the lower and the upper ends of Cohesion and Flexibility (Olson and Gorall, 2006). While the two balanced scales, Balanced Cohesion (sample item: ‘Family members are supportive of each other during difficult times’) and Balanced Flexibility (sample item: ‘My family is able to adjust to change when necessary’) are similar to previous FACES III scales, the four Unbalanced Scales; Enmeshed (sample item: ‘Family members feel guilty if they want to spend time away from the family’), Disengaged (sample item: ‘Family members seem to avoid contact with each other when at home’), Chaotic (sample item: ‘Our family feels hectic and disorganized’), Rigid (sample item: ‘There are clear consequences when a family member does something wrong’), represent an original improvement (Olson, 2011). The two Balanced Scales assess normal functioning, while the other scales are related to problematic functioning. A further improvement brought on by the Balanced and Unbalanced ratio score is that it offers a method to assess the curvilinearity of Cohesion and Flexibility dimensions. These scales proved to be valid, reliable and discriminatory among both problematic and no problematic families and the range of reliability in the six scales is between .78 and .90 (Olson, 2011).
Family Communication Scale
Family Communication Scale (FCS) is based on the Parent-Adolescent Communication Scale (Barnes and Olson, 1985); the PACs is a 20 item scale developed to measure communication in families with an adolescent. The FCS is a shorter 10 item scale on a Likert-type scale based on the longer 20 item version that can be used with a variety of family forms and families at various life cycle stages related to the Circumplex Model. The internal consistency reliability of the scale is .92.
Family Satisfaction Scale
Family Satisfaction Scale (FSS; Olson, 1995) assesses the degree of satisfaction with aspects related to family cohesion and flexibility. The current version of the Family Satisfaction Scale contains 10 items on a Likert-type scale and is based on the original 14 item scale. Based on a sample of 2,465 family members, the 10 item family satisfaction scale has an alpha reliability of .92 and test re-test of .85. In this study internal consistency reliability is .90.
Results
Individual correlates of social, binge and heavy drinkers
The sample was composed of 31 non-drinkers (4.26%), 228 social drinkers (31.40%), 375 binge drinkers (51.65%) and 92 heavy drinkers (12.67%). The frequency of 4.26 percent of no drinkers is slightly higher than other studies (Baiocco et al., 2008; Morawska and Oei, 2005).
Drinking groups differed according to sex [χ2 = (2) = 109.66, p <0.001]. Males were more likely to be classified as binge drinkers (60.3% of male versus 32.9% of females) and heavy drinkers (16.9% of males versus 1.2% of females), while females were more likely to be classified as social drinkers (22.8 of males versus 65.8% of females).
Social, binge and heavy drinkers differed as to the age when they first tried alcohol [F(2,692) = 79.62, p<.001] and the number of friends who regularly drink alcohol [F(2,692) = 151.93, p<.001]. Post hoc analyses revealed that heavy drinkers (M = 12.15, SD = 1.8) were younger than binge drinkers (M = 13.40, SD = 1.31) and binge drinkers were younger than social drinkers (M = 14.39, SD = 1.51) when they first tried alcohol. Heavy drinkers (M = 4.16, SD = 1.06) appeared to have more friends who drink alcohol on a regular basis than binge drinkers (M = 3.93, SD = 0.75); social drinkers reported the lowest number of friends who drink alcohol (M = 2.49, SD = 1.42).
Family functioning and drinking patterns
Drinking groups differed according to the Circum-plex Total Ratio [χ2 = (2) = 36.95, p < 0.001]. The Circumplex Total Ratio provides a summary of a family’s balanced and unbalanced characteristics in a single score (Olson, 2011) and is calculated by dividing the average of the two balanced scales of FACES IV (Cohesion and Flexibility) by the average of the four unbalanced scales (Disengaged, Enmeshed, Chaotic and Rigid). Families of heavy drinkers were more likely to be classified as unbalanced (problematic) (34.6% unbalanced versus 10.4% balanced). No significant differences were found between social and binge drinkers.
To examine differences in family functioning dimensions between the three groups, a MANCOVA model with Bonferroni’s correction was conducted using ‘alcohol use’ group as the fixed factor (heavy versus binge versus social); effects of gender and age were adjusted as covariates. The α level was divided by the number of statistical tests performed (the adjusted P values were α = 0.001). For this multivariate analysis, Wilks’s λ criterion was used.
Concerning family functioning, MANCOVA revealed the main effects for the groups [Wilks’s Lambda = 0.40, F = 67.14, p<.0001]. Age and gender did not show significant covariations with groups for the FACES-IV dimensions [Wilks’s Lambda = 0.98, F = 1.60, p =.87; Wilks’s Lambda = 0.8, F = 1.57, p =.45, respectively). Post hoc analyses revealed that groups differed on Cohesion [F(2,692) = 360.90, p < .001], Flexibility [F(2,692) = 9.74, p < .001], Disengaged [F(2,692) = 10.80, p < .100], Enmeshed [F(2,692) = 8.42, p < .001], Rigid [F(2,692) = 7.22, p < .001] and Chaotic [F(2,692) = 7.79, p < .000]. Post hoc analyses revealed that heavy drinkers showed lower mean scores in the scales of Cohesion and higher mean scores in the scales of Disengaged and Chaotic. Social drinkers showed higher mean scores in the scale of Flexibility and lower mean scores in the scale of Rigid and no differences were found between binge and heavy drinkers in either scale. Heavy drinkers showed higher mean scores than binge drinkers and binge drinkers showed higher mean scores than social drinkers in the scale of Enmeshed. Drinking groups differed regarding Family Communication [F(2,692) = 4440.93, p < .001] and Family Satisfaction [F(2,692) = 2974.39, p < .001]: heavy drinkers showed lower mean scores than binge drinkers; social drinkers showed higher mean scores than binge and heavy (Table 1).
Differences between groups on the FACES-IV subscales
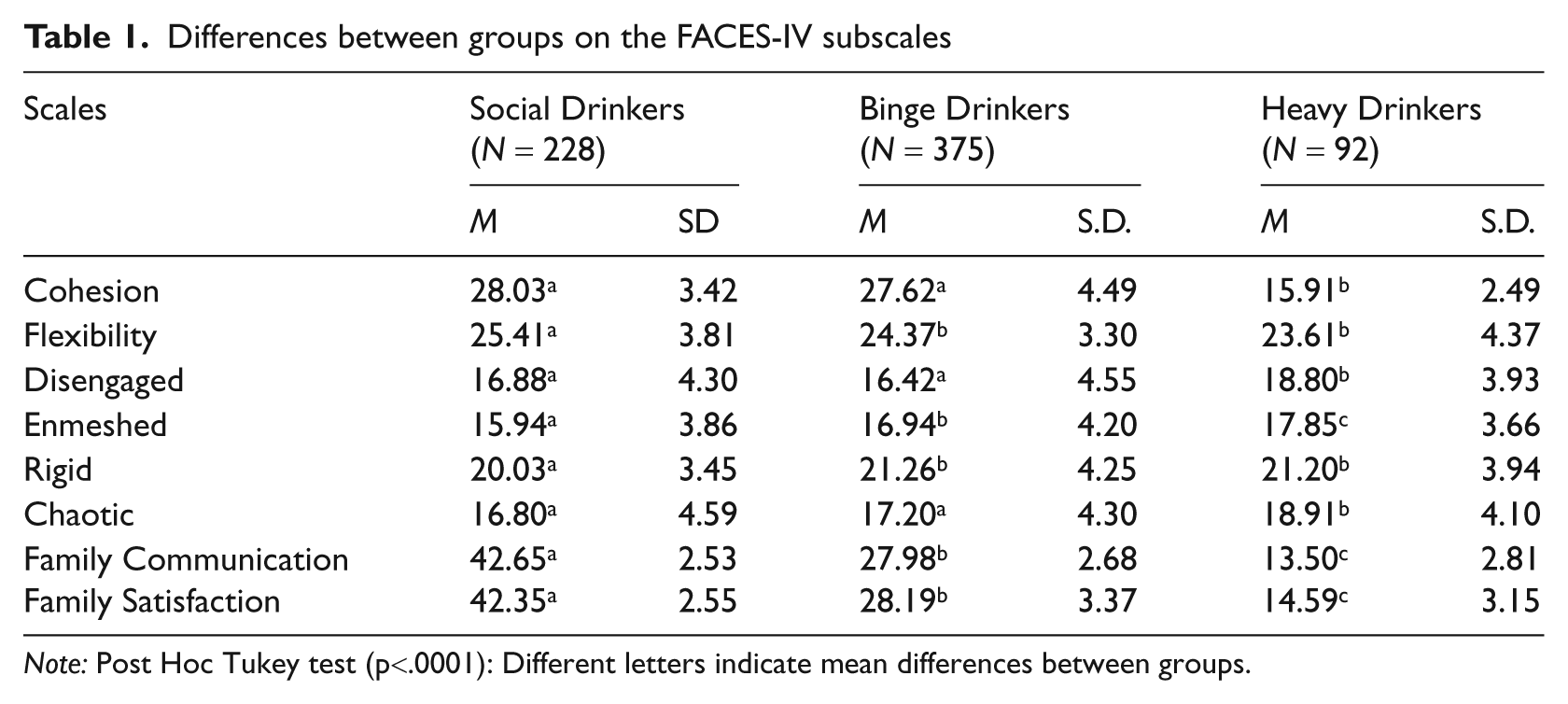
Note: Post Hoc Tukey test (p<.0001): Different letters indicate mean differences between groups.
Social, binge and heavy drinkers: Multivariate findings
A multinomial logistic regression analysis was performed where the dependent variable ‘alcohol use’ has three categories with ‘non–drinkers’ category serving as the reference group. A step-wise approach determined the final model, both before and after adjusting for gender and age. The estimation of a multinomial logistic, regression model tested whether adjusted odds ratios of explanatory variables would be significantly different between the categories of binge, social and heavy drinkers. Specifically, explanatory variables included in the final multinomial logistic regression model were Circumplex Total Ratio, age of alcohol initiation and number of friends who drink alcohol. With respect to family functioning, the significant difference was between heavy drinkers and non-binge (OR = 3.78; CI = 1.13,5.24; p≤.01). Adjustment for gender and age did not reduce the associations. In addition, both heavy and binge drinkers were significantly more likely to be more younger when they first tried alcohol than social drinkers (OR = 5.86; CI = 2.23,7.84; p ≤ .05 and OR = 4.24; CI = 2.36,6.54; p ≤ .01, respectively). Adjustment only for gender attenuated the association with little differences. Analyses further revealed that heavy drinkers were significantly more likely to have a greater number of friends who drink alcohol (OR = 3.78; CI = 1.40,5.48; p ≤ .01) than binge and social drinkers (OR = 2.44; CI = 1.20,5.32; p ≤ .01 and OR = 2.22; CI = 1.12,4.48; p ≤ .01, respectively), compared to non-drinkers. Adjustment for gender and age did not reduce the associations.
A discriminant function analysis was conducted to determine the variables that enabled us to differentiate between the three groups. Two significant functions emerged [χ2 (12) = 681.03, p < .000; χ2 (5) = 117.80, p < .000]. The first function accounted for most of the variance (87.2%). Structure matrix (Table 2) shows that function 1 was principally explained by outcome expectancies about alcohol use like social disinhibition, sexual disinhibition, anxiety relief and by the age when the subjects first tried alcohol. This function was termed alcohol expectancies.
Function 2 was explained by two social variables: the number of friends who regularly drink alcohol and the Circumplex Total Ratio of FACES IV. The second function can be defined as parents/peers influence.
Multiple discriminant function: structure matrix
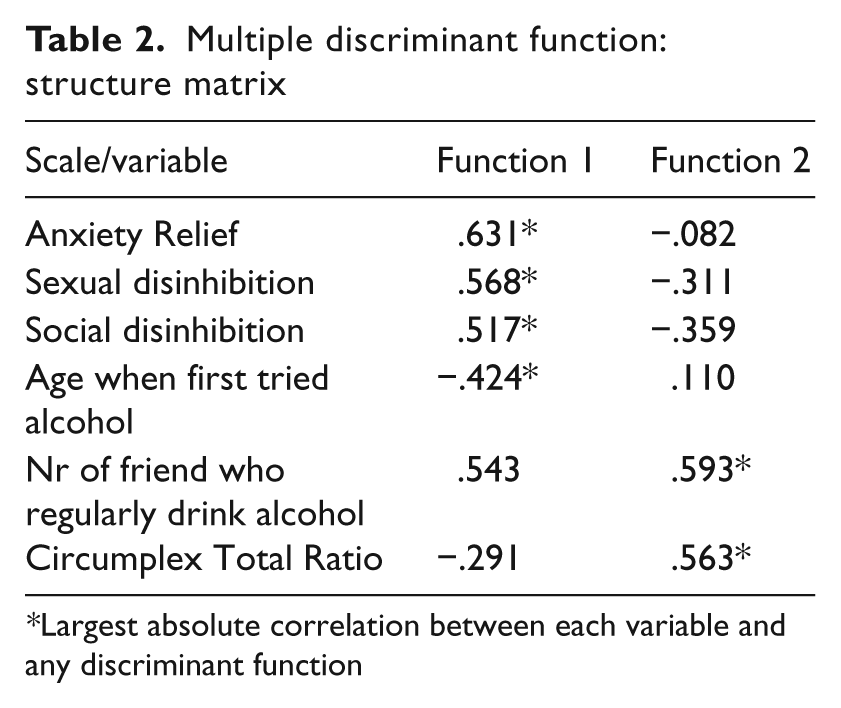
Largest absolute correlation between each variable and any discriminant function
An evaluation of the group centroids showed that function 1 best separates social drinkers from heavy drinkers whereas function 2 adds to differentiate social and binge drinkers from heavy drinkers. The results of discriminant classification show 70.2 percent of the subjects correctly classified (75.7% of social drinkers, 67 % of binge drinkers and 69.6 % of heavy drinkers).
Discussion
Two were the principal aims of this study: first one was evaluating the relevance of binge drinking among Italian adolescents, second one was verifying the possibility to determinate some dimensions, expectancy variables and family functioning variables that can discriminate social drinkers from binge drinkers and heavy drinkers.
The higher percentage found in the sample was classified as binge drinkers (51.65%), who were prevalently males while females described themselves as social drinkers. The data – also consistent with other national estimates (Gallimberti et al., 2010) – confirmed that binge drinking and heavy drinking is indeed widespread among adolescents, especially among males. Researches in the cultural factors connected to drinking habits show that more binge and heavy drinkers are found in Northern, Western and Eastern Europe than in Southern Europe (Smith and Foxcroft, 2009). Data indicate that alcohol problems are less relevant in the countries in which alcohol is integrated in everyday life – as in the South of Italy – whereas they are a more severe issue when drinking on weekends and drinking during social gatherings is culturally accepted – as in the centre of Italy (Beccaria and Prina, 2010).
Social, binge and heavy drinkers were revealed to differ in terms of drinking variables, expectancy about alcohol and family functioning dimensions by means of univariate and multivariate analysis. Results indicate that heavy drinkers were younger than binge and social drinkers when they began to drink on a regular basis, and that they have more friends that regularly drink alcohol. Adolescents affiliating with friends who drink were found to be more likely to drink than those affiliating with non-drinkers (Martin and Hoffman, 1993). Studies reveal that adolescents consider getting drunk as an appropriate behaviour in social contexts such as parties. Hence, perceptions of drinking as socially normative can influence alcohol consumption by students (Crawford and Novack, 2002; Poelen et al., 2007). Some studies (Arria et al., 2008; Baiocco et al., 2010) evidenced that the percentage of drinking friends was a better predictor of adolescent drinking than parents’ or friends’ approval of drinking. Other studies show that adolescents’ perception of alcohol use among friends varies widely: alcohol users tend to overestimate alcohol use among friends and the number of friends who drink alcohol as a way to rationalize their own behaviour (Callas et al., 2004). Such misperceptions are a risk factor for alcohol use and unfavourable outcomes as heavier use patterns or progression to other substances (Beck and Treiman, 1996).
Although the Italian drinking culture is different from other European countries, protective and risk factors regarding the family structures and characteristics are overlapping. Heavy drinkers, unlike social and binge drinkers, live in families characterized by a problematic functioning, with weak emotional bonds and relationship rules not very well defined. Thus, heavy drinkers perceive a low degree of satisfaction, and communication between family members is very difficult and marked by a lack of clarity and regard towards one another.
Social drinkers and their families are more able to modify their own relationship rules and structures in response to life challenges and everyday problems than binge and heavy drinkers. They perceive a good degree of family communication and satisfaction. Binge drinkers live in balanced families in which relational boundaries are less clear than those of social drinkers.
On a multivariate level, discriminant function analysis showed that positive expectancy about alcohol, variables concerning alcohol use (age when regular drinking began) and family functioning are significant in discriminating the three groups of drinkers. The model suggests that positive expectancy about alcohol best separates social drinkers from heavy drinkers while the second function, parents/peers influence, adds to differentiate social and binge drinkers from heavy drinkers. Evidence from other studies indicate that negative family characteristics are linked to alcohol misuse and other antisocial behaviours (Bird et al., 2001; Gil et al., 2000; Tafà and Baiocco, 2009). In adolescence, the tendency to imitate peer behaviours increases compared to childhood, and if the adolescent perceives limited or abnormal closeness to family members, peer influence becomes stronger than that of the family (Moore et al., 2010; Young et al., 2008). Drinking is often used as a way of being accepted by group members, especially if they misuse alcohol.
While the current study is focused on binge drinking, data also seem to give important findings on different drinking patterns. The model needs to be improved; other relevant variables – such as personal self-efficacy or peer/parent norms towards alcohol use – could be introduced to explain differences in drinking patterns. If previous studies analysed attachment, parental monitoring and family conflicts in relation to alcohol misuse (Moore et al., 2010), the present study examined family functioning, a neglected aspect in the others. However, parental descriptions about family functioning were not considered and further investigations are also needed to better understand how parental representations and their drinking behaviours affect alcohol consumption of their sons and daughters.
Moreover, expectancies about the effects of alcohol and family functioning were the strong predictors of alcohol consumption; our results concur with existing literature (Malkus, 1994; Laghi et al., 2009; Moore et al., 2010; Paxton et al., 2007). Differently from demographic or personality factors, our variables can be modified by particular preventive programmes, that is why our findings provide a basis for specific intervention programmes. Results may prove valuable to prevention specialists working with adolescents.
Although the problem of adolescents’ drinking habits is not new, its extent and effects on a national level have become far more relevant than ever before. An ecological framework for a public health prevention effort should recognize that health-related behaviours are influenced by personality and individual factors, interpersonal processes, institutional and community factors, as well as by public policies. Community programmes need to address not only individual student attitudes, but also environments that will support moderation in alcohol use (Cable and Sacker, 2008; Morawska and Oei, 2005). A long-term approach is necessary to modify the students’ alcohol use patterns, but school and community must necessarily work together. Italian high schools do not seem to give the correct attention to the binge drinking phenomenon and prevention approaches. There is a lack of programme evaluation, particularly as far as students’ alcohol use patterns are concerned, and high schools play no role whatsoever in alcohol abuse prevention even though their involvement is vital to the success of prevention efforts.
Some limitations of the study must be pointed out. First, the relation identified in the study is correlational and not causal. For this reason, this study represents only a first step in understanding the relations among binge drinking and family functioning in adolescent sample. Second, all data were collected using self-report questionnaires. Studies using behavioural self-presentation measures, observational data and other-report methodologies to assess behaviours could be very useful for this topic. The present study focused on alcohol use and family functioning in a convenience sample of adolescents. A longitudinal study would provide perspective and generate data on changes in drinking behaviours and cognitions across the years.
Despite these limitations, the present study has important implications for future empirical investigation and also for clinical intervention. To our knowledge, this is the first study to investigate the associations between binge drinking and family functioning, as evaluated with FACES IV, the current self-report questionnaire used to assess the primary dimensions of the Circumplex model. Furthermore, considering that the binge drinking is a significant risk factor for mortality, the current results could be useful for future clinical intervention efforts.
The presented results have nevertheless some important implications for prevention. Furthermore, the results here and in previous research also highlight the importance of a balanced and comprehensive approach to prevention.