
Abstract
Social capital refers to various levels of social relationships formed through social networks. Measurement differences have lead to imprecise measurement. A meta-analysis of eligible studies assessing the bivariate association between social capital and self-reported health and all-cause mortality was performed. Thirty-nine studies met inclusion criteria, showing social capital increased odds of good health by 27 percent (95% confidence intervals [CI] =21%, 34%). Social capital variables, reciprocity increased odds of good health by 39 percent (95% CI = 21%, 60%) and trust by 32 percent (95% CI =19%, 46%). Future research suggests operationalizing measures by assessing differences by race/ethnicity, gender and socioeconomic status.
Keywords
More than two decades of social capital and health research has shown to reduce mortality (Kawachi, 1999; Kawachi et al., 1997; 1999; Pollack and Knesebeck, 2004) make neighborhoods safer (Kennedy et al., 1998), and to build more socially cohesive communities (Boneham and Sixsmith, 2006; Cattel, 2001; Woolcock and Narayan, 2000). Public health researchers have employed a communitarian approach, which reflects Robert Putnam’s (1993) definition of social capital. This approach focuses on the functions of social relationships to promote an active citizenry. Public health research recommends that social capital should be separated into structural and cognitive forms because these have different relationships with health outcomes (Harpham, 2008; Harpham et al., 2002). Structural social capital refers to what people do – associational links, density of social networks, or patterns of civic engagement that can be verified objectively. Coleman (1988) conceptualizes social capital as a resource that originates from the structure of social relationships that facilitate achievement of specific goals. It is important to separate formal networks from informal networks each have different relationships with health outcomes. Also, it is important to note that all relationships can provide value, benefits, and stress.
Cognitive social capital refers to what people feel, or their values or perceptions, and is more subjective. Cognitive social capital is measured at the micro level and is considered to shape behaviors, through control of risk behavior, providing mutual aid and support, and informal means of informational exchange (Cullen and Whiteford, 2001). Cognitive and structural forms of social capital are interrelated: how people feel influences how they act, and how people behave can influence how they feel. The constructs and measures of social capital characterize both structural and cognitive social capital.
Many social capital studies seek to make examine the social capital of a geographic area and often aggregate individual-level data to an ecological level. This limits the focus of social capital constructs and measures on horizontal relationships among neighbors or community members (Kawachi et al., 1997) and less on the vertical relationships among individuals, communities, neighborhoods, organizations, and sources of power. Bourdieu’s (1985) concept of social capital addresses issues of resources and access to power. The Putnam model of social capital directly addresses neither the relevance of actual or potential resources inherent within social networks that may be used for personal or collective action, nor power dynamics, nor how people access (or may be denied access) to network-based resources (Carpiano, 2008; Wakefield and Poland, 2005).
Social capital scholars have begun to distinguish three functions of social capital according to their context and function: bonding, bridging, and linking. These categories are reformulations of network structures that provide ways to place embedded individuals or organizations within communities or neighborhoods. Szreter and Woolcock (2004) suggest that bonding social capital refers to trusting and cooperative relationships, bridging social capital refers to relationships of respect and mutuality, and linking social capital comprises norms of respect and trusting relationships. Such operational definitions also indicate that these constructs can be applied to more than one form of social capital. All three forms characterize the types of networks that individuals and groups use to confer benefits and resources upon members.
Although most social capital research hypothesizes social capital as a resource or determinant of health (Szreter and Woolcock, 2004), others argue that social capital may be determined by health (Halpern, 2005). In general, social capital research is characterized as a mechanism to improve health and the causal path cannot be determined from secondary data analysis. More research is needed to identify and understand the pathways by which social capital operates. Social capital research has developed according to the level it scrutinizes: individual, ecological, network, and multilevel.
The diversity in social capital measurement is productive in the sense of showing the range of social capital measures, but becomes detrimental in the sense that it provides imprecise measurement across the literature. A more comprehensive, systematic study of the constructs of social capital may yield fuller explanations what level of analysis capital can advance the study of social capital’s benefits for health promotion. The effect of context (e.g. geographical area) has important implications for public health initiatives such as policy interventions to improve the quality of life within a neighborhood. The level of analysis also furthers understanding of the compositional effects of social capital. A multilevel analysis cannot be appropriately implemented until it is clear what is being measured. One remedy for the lack of clarity of social capital is meta-analysis, which can combine all the indicators of social capital and compare their effects on health outcomes.
Methods
Selection of studies
There was one main inclusion criteria: studies that reported a statistical test of the relationship between the constructs of social capital (e.g. efficacy, participation, trust, reciprocity, sense of community, social support, and social networks) and either/or both self-reported health and all-cause mortality. Self-reported health and all-cause mortality were the two leading outcome measures found in the social capital literature and the search strategy was limited to these variables to limit the number of outcomes being compared for analysis.
A detailed search using Medline (via Pub Med, OVID), Sociological Abstracts, The Cochrane Database of Systematic Reviews, The Cochrane Library, the ISI Web of Knowledge, and PsycInfo was conducted. The searches were conducted using the following search terms: ‘social capital’, ‘health’, ‘self-reported health’, and ‘mortality’. Limitations included ‘English only’.
Study coding
Several methodological and conceptual issues are of concern in the social capital literature and were the dominant themes of the coding strategy. Studies were read for themes from the 39 eligible studies and from the broader social capital literature. A process of random checks with a second member of the research team helped to further identify themes and errors in coding and data entry. The coding strategy involved examining studies iteratively and reviewed for:
(1) co-variables reported,
(2) how the independent variables (social capital variables) were measured and conceptualized (e.g. at the individual, neighborhood, community, state, or national levels),
(3) how the dependent variables (e.g. self-reported health measures and/or all-cause mortality) were measured and conceptualized (e.g. at the individual, neighborhood, community, state, or national levels).
After coding each study, a second process of coding the social capital variables was performed. The breadth of social capital measures within these 39 studies was vast, which reflected the following larger constructs of social capital: participation, trust, efficacy, sense of community, social support, social networks, bonding, bridging and linking forms of social capital. For the purpose of analyses, each of the social capital measures reported were coded to reflect the larger social capital constructs and improved the ability to combine more studies for comparative analyses. Similarly, most studies did not report social capital measures according to the three forms of social capital: bonding, bridging, and linking. These forms were assigned to the measures according to: bonding (constructs such as participation, trust, and reciprocity), bridging (constructs such as social networks, political or electoral participation) or linking (measures such as voting and trust in legal, political, or government institutions). A number of studies also included a combined social capital measure, constructed by each study author as a social capital index.
Data analyses
The data analysis occurred in five steps. First, the mean effect size estimates for each study were calculated by averaging the effects across all studies. Second, an overall effect was estimated by outcome (e.g. self-reported health or all-cause mortality). Third, theoretical and methodological characteristics were tested as moderators of the overall effect. Fourth, an overall effect was estimated by each social capital variable. Fifth, an overall effect was estimated by one of the three forms of social capital (e.g. bonding, bridging, and linking). Cochran’s Q-statistic was calculated to assess statistical heterogeneity (p ≤ 0.05). Sensitivity analyses were performed to identify potential outliers and other threats to validity of results. Mixed-effects models were reported for tests of heterogeneity and moderation. Data management and analyses were performed using Comprehensive Meta-Analysis (version 2) sponsored by the National Institutes of Health (Biostat, Englewood, NJ). Effects of this meta-analysis are reported as odds ratios measured at the 95 percent confidence level. In most cases, we entered data in the form they appeared in each individual study, correlation coefficients, t-values, p values, odds rations, and confidence intervals. In certain cases, a p value and sample size (e.g. studies reporting regression analyses) were entered and the software calculated an effect size.
Initially, 13 potential moderators were identified to explore the variability in effect sizes. However, as a result of the non-independence of effects, the constructs of social capital and the three forms of social capital (bonding, bridging, and linking) could not be tested as moderators. Instead, the overall effect estimate for each social capital construct was calculated and described to determine its influence on effect size variability. This meta-analysis cannot determine if the independent effects on health of these constructs differ significantly from each other. Three potential moderators met the criteria of effects of dependency and were tested: (1) country (national status of the data: international (one country outside of the United States)), multinational (multiple countries), US (data from the United States only); (2) level of analysis (individual, ecological, multilevel); (3) outcome (self-reported health, all-cause mortality) and social capital survey methods (studies focusing on social capital only versus studies were constructs of social capital were analyzed secondarily).
Publication bias was assessed by computing a ‘fail-safe’ N. This value is an estimate of the number of irretrievable or unpublished studies with null results that would be required to render the observed effect non-significant. In the present analysis, the fail-safe N indicated we would need to locate and include 287.7 missing studies for every observed study for the effect to be nullified, thereby suggesting a low probability of publication bias.
Results
Search strategy
More than 500 studies were identified using this initial search strategy. Upon reviewing titles and abstracts of these, 500 studies were reviewed andthe sample of articles was narrowed to 158 based on the inclusion and exclusion criteria. Other potential articles were reviewed from the reference sections of the articles selected from the database search. Using these search methods and carefully reviewing the 158 studies, a total of 39 studies were identified meeting the inclusion criteria.
Study characteristics
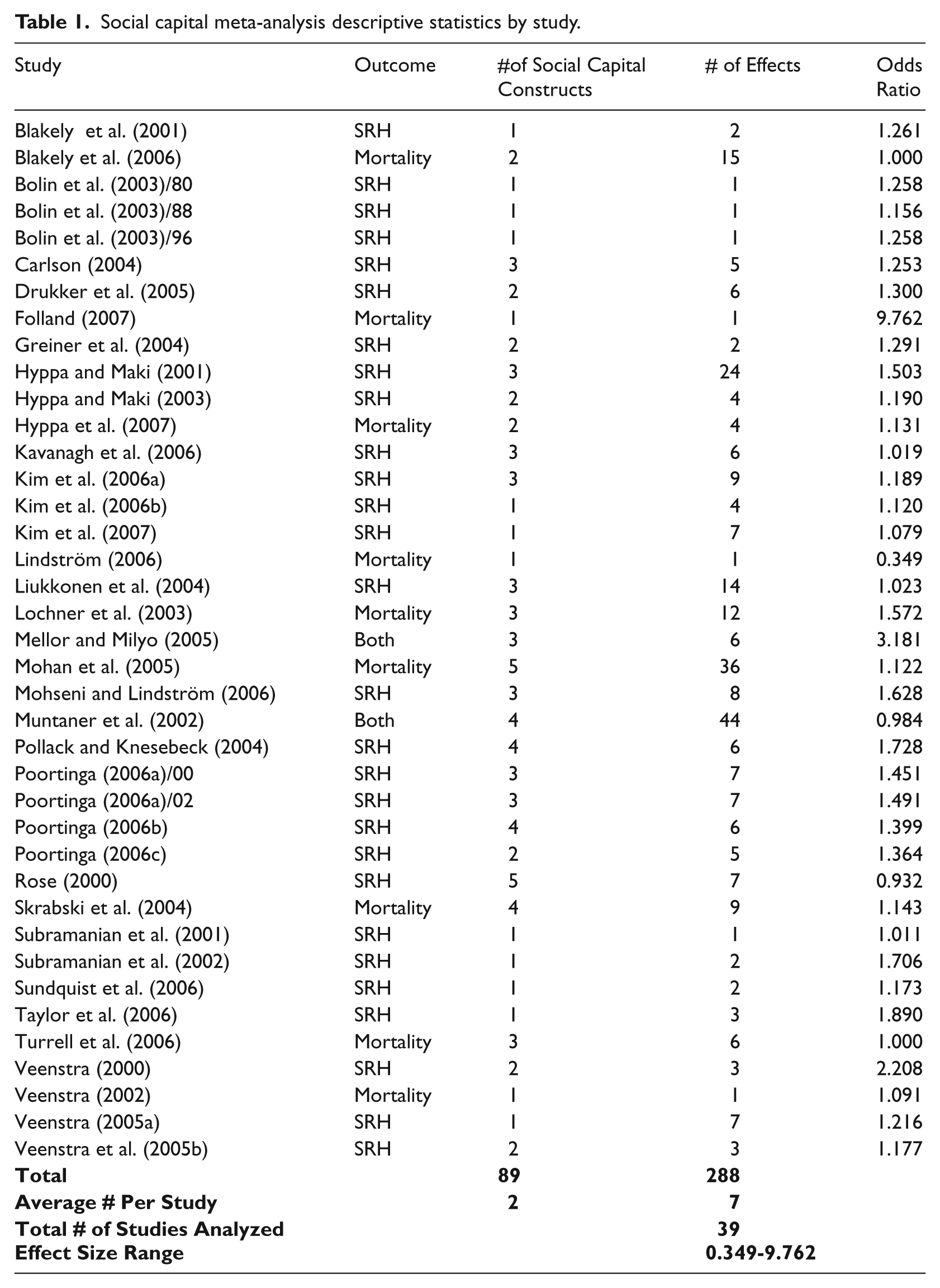
Table 1 contains descriptive statistics of the total sample of studies included in this metaanalysis and reports the overall effect size for each study. A total sample of 39 studies met the inclusion criteria outlined in the methods. These 39 studies yielded 288 effect size estimates. The average number of effect size estimates tested within each study was seven. Self-reported health was an outcome in 28 social capital studies, mortality was the outcome in nine studies, and two studies reported both self-reported health and mortality as outcomes. These studies measured the constructs of social capital using 102 different indicators (specific measures) across social capital constructs. Each of the 288 effect sizes were coded with a social capital construct according to how they were operationally defined within their respective studies. The average number of social capital constructs per study was two.
Social capital meta-analysis descriptive statistics by study.
Overall effect size estimates
The overall weighted effect size estimates and methodological characteristics for each study are presented in Table 1 and Figure 1, while Figure 2 shows moderator analysis. Results showed that an estimate for the overall weighted effect size for the relationship between social capital and health is OR=1.27 (95% confidence interval [CI] 1.21–1.34) and is significantly different than zero (p = 0.0001). The mean effect size within each study estimate ranged from OR = 0.35 (95% CI = 0.07–1.83) to 9.76 (95% CI = 2.80–37.13). The two largest effect sizes were omitted because both were almost three times larger than the next largest effect and were therefore considered to be outliers. These results suggest that on average, a one-unit increase in social capital increases the odds of having good health by 27 percent.
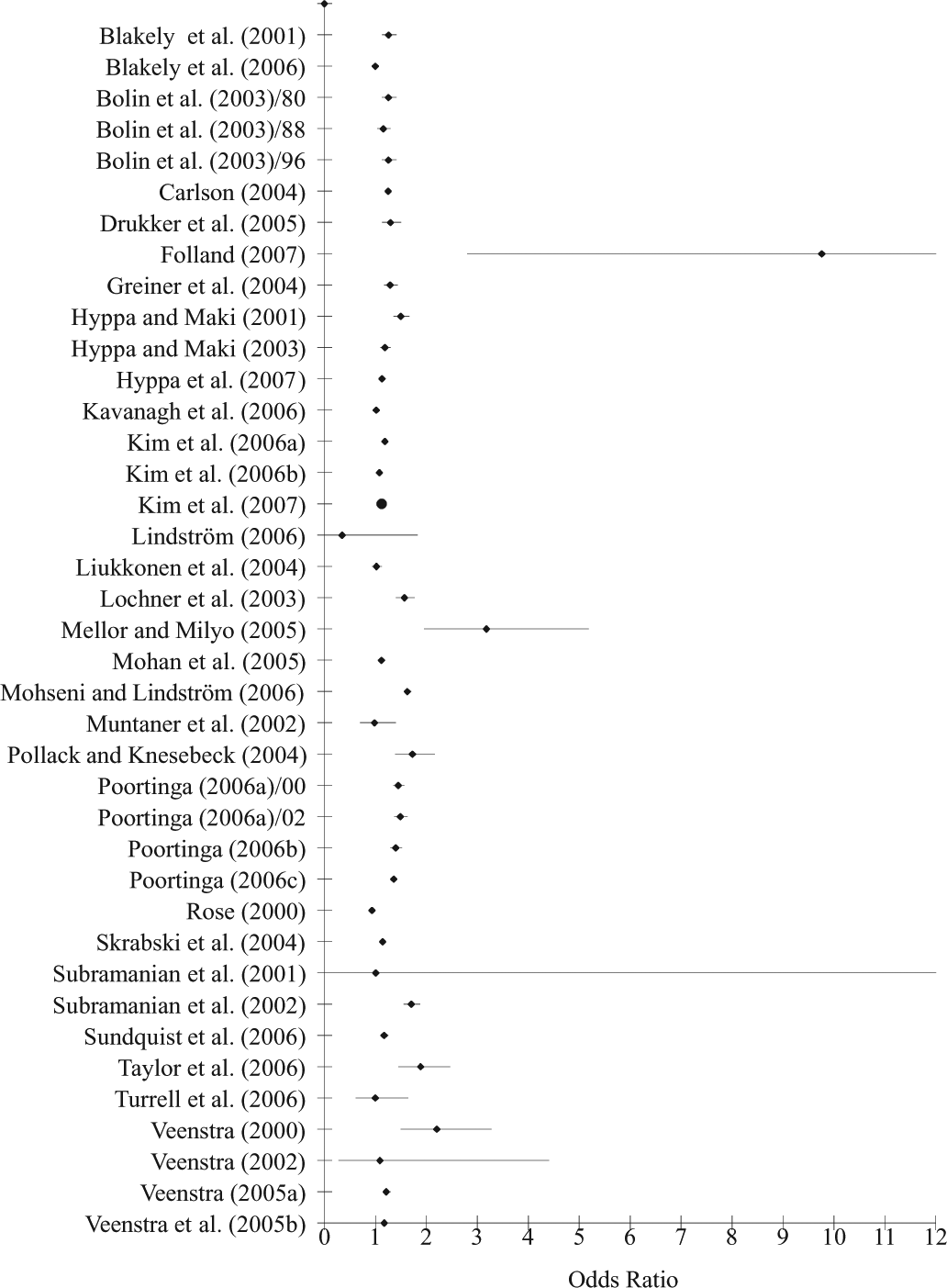
Distribution of effect sizes by study.
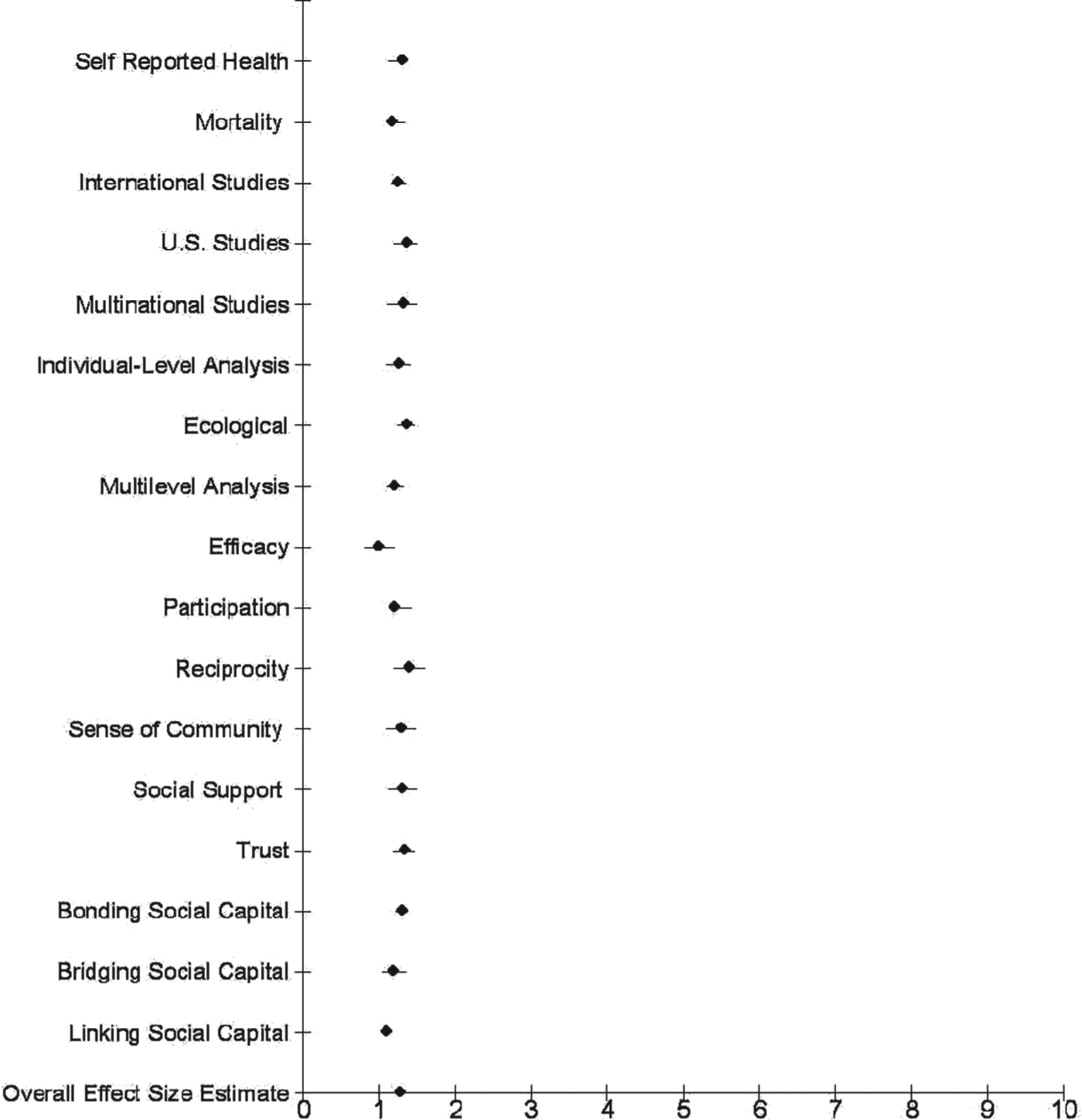
Distribution of effect sizes by moderator.
When the overall effect was recalculated for a sensitivity analysis, with each study removed, all of the overall tests of significance remained significant (p < 0.05). Cochran’s Q-test showed that the effects were significantly heterogeneous (Q = 862.2, d.f. = 38, p = 0.0001). As a result of the significant difference of effect sizes across studies (having significant variability), moderation was tested.
Relationship between social capital, self-reported health and all-cause mortality
Nine studies examined the relationship between social capital and mortality outcomes and 28 tested the association between social capital and self-reported health. A moderator test showed that the relationship between social capital and self-reported health and the relationship between social capital and mortality were marginally different from one another (Q = 3.55, d.f. = 1, p = 0.0597). Because of this marginal difference, results for each set of studies are reported separately in the next section.
The overall weighted effect size for mortality studies was found to be OR = 1.17 (95% CI = 1.20–1.33) and for self-reported health OR = 1.29 (95% CI = 1.21–1.37). These results indicate that an average one-unit increase in social capital will increase the odds of survival by 17 percent and increase the odds of reporting good health by 29 percent. Sensitivity tests showed that no one study in either set of outcome studies significantly influenced the overall effect estimate. Regardless of which study was removed for self-reported health studies, the overall estimated effect size range was OR = 1.27–1.30 and for mortality studies OR = 1.12–1.15.
Level of analysis
The purpose of this analysis was to test whether or not the effect size variability across studies is influenced by the conceptual level and statistical analysis of social capital (e.g. individual versus community/ecological). Thirty-nine studies were analyzed at three different levels of analysis: individual (N = 12), group or ecological (N = 16), and multilevel (N = 11). Studies were characterized by level of analysis according to how each analyzed the relationship between social capital and health. Cochran’s Q-test for moderation showed that the effects were not significantly different across these subgroups of studies (Q = 4.48, d.f. = 2, p = 0.11). The three average effect sizes estimated for each level of analysis were not statistically different from each other. Group studies, or studies measured at the ecological level, had a higher OR = 1.36 (95% CI = 1.26–1.47), followed by social capital studies measured using individual analyses, OR = 1.25 (95% CI = 1.11–1.40); the lowest overall effect size estimate was for multilevel analyses, OR = 1.20 (95% CI = 1.11–1.31). These results indicate that, on average, studies that examine communities, neighborhoods, states, and nations show that a one-unit increase in social capital increases the odds of having good health by 36 percent. Studies that examine social capital at the individual level show that a one-unit increase in social capital increases the odds for good health by 25 percent. Finally, studies that examine social capital using a multilevel framework show that a one-unit increase in social capital increases the odds of good health by 20 percent. Sensitivity tests show that no one study in any of these sets of outcome studies significantly influences the overall effect estimate.
Country
Data were categorized according to each study’s country of origin. Three categories emerged: International (N = 24), Multinational (N = 5), and United States (N = 10). Results showed that country was not a significant moderator (Q = 1.69, d.f. = 2, p = 0.430). Estimates for the overall weighted effect size for the relationship between social capital and health as moderated by country were OR = 1.24 (95% CI = 1.16–1.33), 1.31 (95% CI = 1.12–1.50), and 1.35 (95% CI = 1.22–1.50), respectively for international, multinational, and US studies. The US studies’ effect size estimate is larger but not statistically different than the international and multinational effect size estimates. On average, studies that examined the relationship between social capital and health in one international data found that a one-unit increase in social capital increases the odds of having good health by 24 percent. Studies that examined the relationship between social capital and health with data based in multiple countries found that a one-unit increase in social capital increases the odds of having good health by 31 percent. Studies examining the relationship between social capital and health with data based in the United States showed that with every one-unit increase in social capital the odds of having good health increased by 35 percent.
Constructs of social capital
Efficacy
Four studies and 17 effect sizes tested the effects of the social capital construct of ‘efficacy’ and health. These studies comprize two social capital indicators: self-efficacy (e.g. measured by individuals’ level of control over their lives) and collective efficacy (e.g. measured by informal social control). Collapsing these social capital constructs into one proffered one group for comparison, for which the fixed-effects model was an appropriate test of heterogeneity. Cochran’s Q-test for fixed effects showed that these effects were significantly heterogeneous (Q = 13.4, d.f. = 3, p = 0.004), whereas the overall effect size was OR = 0.995 (95% CI = 0.82–1.20), ns, not significantly different than zero. These results indicated that on average, people with high levels of efficacy had odds of reporting poor health almost equal to people with lower levels of efficacy. Of the four studies that reported effects of the social capital construct efficacy, two were not significant at the p < 0.05 level, one study had a p-value of 0.05, and one had a p-value of <0.05. Sensitivity analysis showed that the overall effect size estimate did not change significantly with each study removed. When Skrasbski et al. (2004) and Rose (2000) wre individually removed, the overall estimated effect size increased slightly above OR = 1.00; howeer, this non-significant finding suggests that neither study was a significant outlier.
Participation
The overall estimated effect size for participation was calculated from 124 effect sizes that yielded 51 different indicators of participation in 26 studies. These measures of participation included whether individuals had associational memberships, belonged to organizations, attended church or volunteered. Cochran’s Q-test for fixed effects showed these effects to be significantly heterogeneous (Q = 124.2, df = 25, p < 0.05). The overall weighted effect size was OR = 1.20 (95% CI = 1.25–1.41), with a range of OR = 0.309 (95% CI = 0.092–1.04) to OR = 3.35 (95% CI -8.10). With every one-unit increase in participation, the odds of having good health increases by 20 percent. Results remained significant after sensitivity tests.
Reciprocity
Five studies reported measures of reciprocity (with a total of 12 effect sizes) and five indicators were used to measure reciprocity (e.g. willingness to help others in certain situations, altruistic activity, and giving). Using the fixed-effects model, Cochran’s Q-statistic showed these results to be significantly heterogeneous (Q = 24.1, d.f. = 4, p < 0.05). These results are significantly different than zero (p < 0.05). The overall effect size estimate was OR = 1.39 (95% CI = 1.21–1.6). With every one-unit increase of engagement in reciprocal activities, the odds of having good health increased by 39 percent. Sensitivity tests showed that regardless of which study was removed for reciprocity studies.
Sense of community
Six studies measured sense of community, using 19 indicators such as individuals’ perceptions of neighborhood safety, social cohesion, and friendliness of neighbors. A total of 21 effect sizes were derived. Using the fixed-effects model, Cochran’s Q-statistic showed these results to be significantly heterogeneous (Q = 47.17, d.f. = 5, p < 0.05). They are significantly different than zero (p = 0.001). The overall effect size estimate was OR = 1.28 (95% CI = 1.10–1.49). With every one-unit increase in a positive sense of community, the odds of having good health increases by 28 percent. Sensitivity test showed that regardless of which study was removed, these results remain significant.
Social capital indices
Social capital indices were captured by various composites of social capital measures such as trust, participation, collective efficacy, and reciprocity. Trust and participation were the two predominant social capital measures, included across 11 studies. Using the fixed-effects model, Cochran’s Q-statistic showed these results to be significantly heterogeneous (Q = 154.28, d.f. = 10, p < 0.05). They are significantly different than zero (p < 0.05). The overall effect size estimate was OR = 1.27 (95% CI = 1.12–1.43). With every one-unit increase in a composite measure including multiple indicators of social capital, the odds of having good health increases by 27 percent. Sensitivity test showed that regardless of which study was removed, these results remained significant.
Social support system
The social support system analysis was compiled by aggregating social support and social network effect sizes. Measures of social support included having someone to rely on when ill and a sense of support from family, friends, and co-workers. Social network measures included the diversity of friendship networks, having a friend of another race or ethnicity, and the frequency of individuals meeting locals in their areas. There were a total of 38 effect sizes, 22 indicators of social support systems, and 10 studies reporting social support system measures. Using the fixed-effects model, Cochran’s Q-statistic showed these results to be significantly heterogeneous (Q = 139.29, d.f. = 9, p < 0.05). The overall effect size estimate was OR = 1.30 (95% CI = 1.13–1.50). With every one-unit increase in social support, the odds of having good health increases by 30 percent. Regardless of which study was removed, sensitivity tests showed the range of overall estimated effect sizes regardless of which study is removed was OR = 1.24–1.35.
Trust
Twenty-two studies reported measures of trust, as measured by 20 different indicators, yielding 58 effect sizes. Using the fixed-effects model, Cochran’s Q-statistic showed these results to be significantly heterogeneous (Q = 447.07, d.f. = 21, p < 0.05). These results were significantly different than zero (p < 0.05). The overall effect size estimate for trust measures was OR = 1.32 (95% CI = 1.19–1.46). With every one-unit increase in trust, the odds of having good health increases by 32 percent. Sensitivity tests showed no significant outliers regardless of which study was removed.
Bonding
Thirty-seven studies and 249 of the 288 total effect sizes captured bonding social capital. Using the fixed-effects model, Cochran’s Q-statistic showed these results to be significantly heterogeneous (Q = 718.43, d.f. = 36, p < 0.05). These results are significantly different than zero (p < 0.05). The overall effect size estimate for trust measures was OR = 1.30 (95% CI = 1.22–1.37). With every one-unit increase for those with horizontal or homogenous social capital sources, the odds of having good health increases by 30 percent. Sensitivity tests showed that regardless of which study was removed there were not any significant outliers.
Bridging
Eleven studies and 26 effect sizes captured bridging social capital. Using the fixed-effects model, Cochran’s Q-statistic showed these results to be significantly heterogeneous (Q = 196.36, d.f. = 10, p < 0.05). These results are significantly different than zero (p = 0.007). The overall effect size estimate for trust measures was OR = 1.18 (95% CI = 1.05–1.34). With every one-unit increase in both horizontal and vertical social networks, the odds of having good health increases by 18 percent. Sensitivity tests showed that regardless of which study was removed, no one study was a significant outlier.
Linking
Fourteen effect sizes and eight studies reported measures of linking social capital such as electoral and political participation, as well as trust in institutions such as government, the legal system, or other political institutions. Using the fixed-effects model, Cochran’s Q-statistic showed these results to be significantly heterogeneous (Q = 84.63, d.f. = 7, p < 0.05). However, these results are not significantly different than zero (p = 0.14). The overall effect size estimate was OR = 1.10 (95% CI = 0.97–1.24). With every one-unit increase for those with high levels of linking social capital, the odds of having good health increased by 10 percent. Sensitivity tests showed that no one study was a significant outlier.
Discussion
This is the first meta-analysis to show the overall statistical relationship between social capital and health. There have been other systematic reviews reporting an overall positive relationship between social capital and health (Islam et al., 2006; Kawachi et al, 2004) by conducting systematic reviews and graphically examining individual studies of social capital. Kim and colleagues (2008) investigated how social trust and associational memberships relate to statistical associations between higher social capital and the relative odds of fair/poor health, life expectancy, and mortality. This study reported the results of individual studies, not the cumulative effect of all studies reporting a social capital variable and a relationship between a general health outcome such as self-reported health and mortality. This study reports the cumulative effects of multiple constructs of social capital and the odds of good health.
The results of this meta-analysis suggest a strong positive relationship between social capital and health as measured by self-reported health and mortality. This meta-analysis aimed to compile the social capital literature to determine whether social capital has a positive relationship with health. The results from this meta-analysis do provide evidence of a strong positive relationship between social capital and health. The association presented in this meta-analysis could be strengthened, but this study, like many social capital studies, are burdened by several factors, discussed later. These factors have long plagued the social capital literature. Social capital, a complex phenomenon, is a result of social relationships based upon reciprocal exchanges between residents of the same neighborhood, family and friend networks, or members of social, religious, or political organizations. Results from this meta-analysis imply that research about the relationship between health and social capital might be better assessed by self-reported health measures. The practice of using self-reported health to predict future health status and mortality, as many social capital studies do, may also be a function of secondary data analyses of cross-sectional data in which self-reported health appears as an available health outcome in many studies.
Another goal of this meta-analysis was to examine the relationship of each social capital construct with health. Its results show that the construct of reciprocity has the largest effect on health, followed by trust. The lowest effect size found was for efficacy. This meta-analysis cannot determine if these effect size estimates are significantly different.
The heterogeneity tests from this meta-analysis showed that certain factors do account for the previously unexplained differences among the targeted studies. Testing for moderators became a function of how best to categorize or combine the social capital literature based on both theoretical and a priori assumptions. Upon careful review of the literature, 14 categories emerged as possible moderators. However, not every social capital construct could be tested as a potential moderator because of the non-independence of effects. Thus, the ability of this meta-analysis to test the significance between social capital constructs, bonding, bridging, and linking forms of social capital was limited.
Limitations
One possible explanation the overall effect size estimate between social capital and health is not larger may be a lack of social capital studies to identify mediators, confounders, and moderators. The inability of these studies to systematically discuss the possible influence of mediators, confounders, and moderators is a major limitation within the literature that reduces the capacity not only of this meta-analysis but also of future meta-analyses. The use of multiple indicators of social cohesion has been encouraged in the literature (Kim and Kawachi, 2006) to avoid measurement error that leads to a downwardly biased of effect estimates (Kim et al., 2008). This analysis was unable to adequately test for moderation stratified by race/ethnicity, gender, age, income, education, or to test each of the social capital constructs and the interaction effects among them. Islam et al. (2006) found the association between social capital and health was more consistently reported in less than egalitatiran countries, or those countries marked by high concentrations of inequities such as poverty and racial segregation. A weaker or unobserved association was found for more egalitarian countries such as Canada and Sweden. Kim et al. (2008) suggest that inegalitarian countries have more safety nets such as more spending on public goods for example, health care, education, and unemployment insurance, which may make social capital less salient. Resulting from this argument, social capital matters more for inegalitarian countries, and by extension less egalitarian communities within these countries. To be able to more clearly suggest why and for whom social capital matters more, social capital research will need to more clearly articulate how social capital operates differently within and across communities, neighborhoods, states, and countries, especially in environments where inequality persists.
Social capital research as an approach to health promotion contains several limitations that can be broadly described as a lack of conceptual development in theory and measurement. Because social capital research lacks clear distinctions between social capital as an attribute of a geographic space or as an individual attribute, it also suffers from the problematic operation of variables and offers limited theoretical exploration of causal linkages (Carlson and Chamberlain, 2003). Research interests in social capital and health promotion stem from strong motivation to discover a mechanism to help explain the association of income distribution with mortality, psychosocial mechanisms, and a particular psychosocial mechanism that specifically operates at an ecologic level (Moore et al., 2006).
One of the many limitations of this meta-analysis was to be able to distinguish differences in social capital by SES, race, and gender. Social capital has become useful to explain how social relationships can increase human capital (Coleman, 1988), but in a nonspecific manner. However, a possible gradient effect rather than a threshold effect may indicate that one’s social positioning along various social and economic hierarchies affects income as well as health (Marmot and Feeney, 1997). Others have suggested that income inequality can lead to increased mortality by causing individuals to disinvest in social capital (Kawachi et al., 1997). Baum and Ziersch (2003), who refer to the ‘darker side’ as social ‘exclusion/inclusion and equity’, argue that these problems are relevant because they link the social elements of exclusion to material deprivation and poverty and emphasize the processes of marginalization, providing further evidence that individuals’ and communities’ access to elements of social capital can vary according to characteristics such as race, gender, and socioeconomic status.
Future research
At best, social capital may be an essential but not a sufficient ingredient for health improvement (Lochner et al., 2003). This conclusion is drawn from both the extensive limitations of, and opportunities for, social capital development in the field of public health. To determine if social capital is necessary and sufficient, researchers and practitioners will need to understand how to encourage the development of social ties and to strengthen existing social ties through increased participation in various contexts that can ultimately improve health behaviors and health outcomes. Finally, future studies should focus on the vast array of indicators for social capital to better understand how existing studies specifically measure each construct, and determine where measurement for future secondary analyses should focus and how best to develop data collection methods for observational studies.
Footnotes
Acknowledgements
The authors want to thank Michael Marshal, Rashawn Ray, Arjumand Siddiqi, Ronald Stall and Allan Steckler for reading drafts of this manuscript and providing invaluable feedback.