
Abstract
Positive body image is defined as healthy body-related attitudes that go beyond the absence of distressful symptoms. A warm and secure relationship with an important other person has been linked with attitudes of acceptance and appreciation toward one’s body as well as adaptive eating patterns. This study tested whether a warm and secure relationship with God was similarly related to positive body image. Undergraduate women completed self-report measures of religiosity, life satisfaction, body appreciation, body acceptance by others, functional orientation, and intuitive eating. Multiple regression analyses showed that relationship with God contributed variance to most of the well-being variables.
Introduction
The Hebrew word “shalom” refers to a sense of wholeness, well-being, and flourishing that goes above and beyond the absence of problems. This ancient concept parallels the basic premise of positive psychology, which states that well-being consists of more than the absence of distressing symptoms. Instead, optimal psychological health is conceptualized as positive subjective experiences such as contentment, satisfaction, hope, and optimism, as well as the presence of strengths and assets that help to build a rewarding and satisfying life (Seligman and Csikszentmihalyi, 2000). Research in health psychology has increasingly focused on positive psychological constructs (Schmidt et al., 2011), and mounting evidence shows that religion is related to many of these outcomes, including life satisfaction (Krause and Ellison, 2003), optimism and hope (Sethi and Seligman, 1993, 1994), subjective health (Karademas, 2010), post-traumatic growth (Schmidt et al., 2012), and adaptive coping with physical disfigurement (Egan et al., 2011). The purpose of the present study was to test whether a particular aspect of religiosity—one’s perceived relationship with God—would predict general well-being as well as specific aspects of well-being related to body image and healthy eating patterns.
When it comes to their bodies, most Western women do not experience shalom. The “normative discontent” that characterizes modern women (Rodin et al., 1985) is thought to stem from pervasive sociocultural messages—from the media as well as friends and family—about the desirability of extreme thinness. In response to sociocultural pressures, many women routinely scrutinize their appearance, worry about their weight, and restrain their eating. However, striving toward the thin ideal, concerns about weight and appearance, and dieting have all been shown to contribute to the development of eating disorders and depression (Stice, 2002). Various interventions have attempted to mitigate these factors, and some have been quite successful (e.g. Stice et al., 2008). Nevertheless, reduced levels of maladaptive attitudes and behaviors do not necessarily represent the positive end of the spectrum of psychological and physical health.
Within the eating disorders and body image literature, there is a growing interest in positive body image and adaptive eating. Consistent with the premise of positive psychology, these constructs involve behaviors and attitudes associated with a full and productive life that are incongruent with concerns about one’s appearance, negative feelings about the body, and dieting. Specifically, optimal body attitudes and eating behavior include body appreciation, body acceptance by others, functional orientation, and intuitive eating. Body appreciation refers to unconditional approval and respect for the body along with a cognitive rejection of unrealistic cultural ideals. Body acceptance by others involves the perception that friends, family, dating partners, and the media have indicated that one’s body is acceptable the way it is. Functional orientation refers to a focus on and appreciation for what the body can do as opposed to how it looks. Finally, intuitive eating refers to a pattern of eating that relies on internal cues—rather than emotions or rigidly imposed dietary rules—for deciding when and what to eat. Each of these constructs has been shown to inversely relate to disturbed body attitudes and eating disorder symptomatology (Avalos et al., 2005; Avalos and Tylka, 2006; Tylka and Wilcox, 2006). These constructs also emerged as themes in qualitative studies of women who endorsed positive body image (Frisén and Holmqvist, 2010; Wood-Barcalow et al., 2010). Thus, optimal psychological functioning for women likely includes elevations on each of these dimensions in addition to low or absent body image disturbance.
According to some scholars, a sense of unconditional positive regard from an important other person is the starting point for the development of positive body image and intuitive eating (Avalos and Tylka, 2006). This acceptance model is based on the principles of client-centered therapy (Rogers, 1961), which asserts that people have a tendency toward personal growth and flourishing when they are not constrained by the expectations of others. In contrast, when women do not experience unconditional acceptance, they may turn to societal ideals for direction regarding what is important and how to behave. The pervasive cultural message for women is that appearance—particularly a thin body—is of utmost importance (Ahern et al., 2011). Thus, women who lack a sense of acceptance by others are more likely to internalize the cultural thin ideal and to focus on their appearance. Furthermore, as they strive to achieve a thin body, they are likely to attempt to ignore their internal hunger and satiety signals, and instead, eat according to external dieting rules or in response to negative emotions. Conversely, women who feel accepted and secure in their relationships with significant others are less likely to try to earn approval through a thin body. In the absence of perceived pressure from others to lose weight and eat a certain way, they are likely to be more appreciative of their bodies and more in touch with their inner experiences. These ideas have received initial empirical support (Augustus-Horvath and Tylka, 2011; Avalos and Tylka, 2006).
Religious people often perceive that they have a personal relationship with God, and this relationship may offer the ultimate source of unconditional acceptance. It has been argued that an individual’s relationship with God serves many of the same psychological functions as a human attachment relationship (Kirkpatrick and Shaver, 1992). According to attachment theory (Bowlby, 1969/1982), people who have an enduring emotional bond with a loving relationship partner develop an internalized sense of worth and are not dependent on others for approval. They expect others to be emotionally available and to respond consistently. Similarly, people with a secure attachment to God are confident that they are loved and accepted by God. They have an assurance that God is available and willing to provide help in time of need (Kirkpatrick and Shaver, 1992). In this regard, a secure attachment with God provides a constant source of unconditional acceptance. As a result, we hypothesize that women who feel loved and accepted by God are less likely to turn to external sources of approval that would include cultural and interpersonal messages about appearance and eating. Furthermore, it is reasonable to expect that women who are less dependent upon external standards of approval will be more in touch with what their bodies can do and how they feel.
Previous research provides preliminary support for these ideas. As far as human relationships, insecure adult attachment has been shown to inversely correlate with body satisfaction, body appreciation, and intuitive eating (Cash et al., 2004; Iannantuono and Tylka, 2012). In regard to religion, a short-term longitudinal study found that women with a secure God attachment experienced reduced levels of several important sociocultural risk factors for eating disorders, including perceived pressure from others to lose weight, internalization of the cultural thin ideal, body dissatisfaction, and dieting (Homan and Boyatzis, 2010). An experimental study found that secure God attachment buffered women from the negative effects of viewing thin-ideal promoting media (Homan, 2012). Although these findings indicate that secure God attachment can function as a protective factor, the absence or reduction of pathology is not synonymous with optimal psychological health and so it remains to be seen whether secure God attachment promotes body-related well-being. Furthermore, one limitation of these studies is that they did not rule out the possibility that a more general sense of being accepted might explain the observed relationships.
Contemporary scholars describe adult attachment along two orthogonal dimensions: anxiety and avoidance (Brennan et al., 1998). The anxiety dimension includes fears about abandonment or rejection and need for reassurance and approval. The avoidance dimension includes an unwillingness to maintain closeness in a relationship and reliance on self. Because of the hypothesized importance of acceptance in the nurturing of positive body image and intuitive eating, we expected that the anxiety dimension would show stronger associations with our body-related well-being variables because it taps themes of unconditional acceptance and relationship security. However, each dimension theoretically captures unique features of an attachment relationship (Brennan et al., 1998), so we explored the simultaneous contributions of each dimension.
The purpose of this study was to investigate the relationships between the two attachments to God dimensions, subjective well-being, and body-related well-being. In order to rule out the possibility that a general attachment style underlies the relationship between God attachment and well-being, we statistically controlled for parent attachment. Finally, because the vast majority of research on eating behavior and body image has used female samples, we restricted our sample to female undergraduates. Thus, we hypothesized that secure God attachment would show positive associations with subjective well-being, body appreciation, body acceptance by others, functional orientation, and intuitive eating. (This set of variables is hereafter referred to as well-being variables.) We hypothesized that the attachment anxiety dimension would show associations with more of the well-being variables than attachment avoidance. Furthermore, we hypothesized that these associations would remain significant when parent attachment was controlled.
Method
Procedure and participants
Participants were recruited from undergraduate courses at a private Christian liberal arts college. Prospective participants heard a brief description of the study in their regular classes, including details related to informed consent. Interested participants received an envelope of materials which they completed privately and independently at their own convenience. They dropped off the completed materials in a box located in a central area of the Psychology department. All students received extra course credit in exchange for participation. The study was approved by the Institutional Review Board, and all participants were treated in accord with the ethical guidelines of the American Psychological Association.
The sample included 104 women who ranged in age from 18 to 22 years (M = 20.00, standard deviation (SD) = 0.88) with an average body mass index of 21.9 (SD = 3.01). Most identified themselves as Caucasian American (95.2%); the remainder identified as African American, Asian American, or Latino. They identified themselves as upper middle class (51.9%), middle class (46.2%), or working class (1.9%). Most of the women (62.6%) described themselves as “very religious,” 28.4 percent as “somewhat religious,” 4.0 percent as “extremely religious,” and 5 percent as “not at all religious.” The majority attended religious services weekly (53.8%) or more than once a week (27.4%). The remaining participants attended 2–3 times per month (11.3%), once a month (3.8%), or less than once a month (3.8%).
Measures
The Attachment to God Inventory (AGI; Beck and McDonald, 2004) was used to assess individuals’ relationship with God. Participants indicated agreement with 26 items using a 7-point scale (1 = disagree strongly, 7 = agree strongly). The 14-item Anxiety subscale (AG-Anxiety) tapped themes of anxiety about one’s relationship with God (e.g. “I often worry about whether God is pleased with me,” “Sometimes I feel that God loves others more than me.”) Because all but one of the AG-Anxiety items were worded in the insecure direction, two items were reworded to reflect greater security. Specifically, “I fear God does not accept me when I do wrong” was restated as “I feel that God still accepts me when I do wrong,” and the item, “I worry a lot about damaging my relationship with God” was reworded as “I don’t worry about damaging my relationship with God.” These two items were reverse scored for consistency with the rest of the subscale. High scores on this subscale reflect an anxious, insecure relationship with God, while low scores reflect greater security. The 12-item Avoidance subscale (AG-Avoidance) assessed themes involving an unwillingness to draw close to God (e.g. “I just don’t feel a deep need to be close to God,” “I believe people should not depend on God for things they should do for themselves”). High scores on this subscale reflect greater avoidance. The AGI showed good factor structure and construct validity in a multisample study (Beck and McDonald, 2004).
We used the Parental Trust subscale of the Inventory of Parent and Peer Attachment (Armsden and Greenberg, 1987) to assess women’s relationship with the parent to whom they felt closest. Development of this scale was based on Bowlby’s (1969/1982) descriptions of attachment behavior and felt security toward attachment figures. Thus, it tapped themes of perceived parental respect of needs and desires, sensitivity, and responsiveness (e.g. “My parent respects my feelings,” “My parent accepts me as I am,” “When I’m angry about something, my parent tries to be understanding”). Participants responded to each of 10 items using a 5-point scale (1 = never, 5 = always). This measure showed strong internal consistency, test–retest reliability, and convergent and divergent validity among male and female undergraduates (Armsden and Greenberg, 1987).
Subjective well-being has been defined as a multidimensional construct including overall life satisfaction, positive affect, and reduced negative affect (Diener, 1994). Thus, we measured subjective well-being with the Satisfaction with Life Scale (Diener et al., 1985), which includes five statements about general life satisfaction (e.g. “In most ways my life is close to ideal”). Participants indicate agreement with each statement using a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree). Higher scores indicate higher life satisfaction. This widely used measure demonstrated strong internal consistency and test–retest reliability among college students and older adults (Diener et al., 1985). Positive and negative feeling states were measured using the Exercise-Induced Feeling Inventory for Chronic Training (Rejeski et al., 1999). This scale presents 12 mood adjectives and asks participants to indicate the extent to which they felt each mood in the past month using a 6-point scale scored from 0 (none of the time) to 5 (all of the time). The scale has demonstrated validity and sensitivity in middle-aged adults and college students (Blanchard et al., 2004; Rejeski et al., 1999).
The Body Acceptance by Others Scale (BAOS; Avalos and Tylka, 2006) was used to assess the extent to which participants perceive that significant others (such as family, friends, and dating partners) as well as society and the media accept their body shape and weight. Participants rate 10 items (e.g. “My family has sent me the message that my body shape and weight are fine”) on a 5-point scale ranging from 1 (never) to 5 (always). The BAOS demonstrated excellent internal consistency and test–retest reliability in a sample of undergraduate women (Avalos and Tylka, 2006). It also showed a significant inverse relation to pressure for thinness and was unrelated to impression management.
The 13-item Body Appreciation Scale (BAS; Avalos et al., 2005) was used to assess participants’ acceptance and appreciation of their bodies (e.g. “Despite its flaws, I accept my body for what it is”). The items are rated on a 5-point scale ranging from 1 (never) to 5 (always). Higher scores reflect greater body appreciation. The BAS showed strong internal consistency and factor analysis supported its single dimensional structure. The scale was positively correlated with an alternative measure of positive body image and negatively correlated with aspects of disturbed body image and eating disorder symptoms in college women (Avalos et al., 2005).
We used the Body Surveillance subscale of the Objectified Body Consciousness Scale (McKinley and Hyde, 1996) to assess functional orientation. This scale was originally developed to measure the extent to which a woman monitors her body and thinks of her body in terms of how it appears to others rather than how it feels or functions. Participants indicate agreement with eight statements using a 6-point scale (1 = strongly agree, 6 = strongly disagree). In the original scoring procedure, six of the eight items are scored in reverse such that the total score reflects greater body surveillance (e.g. “I think more about how my body feels than how my body looks”). However, for the present study, all items were scored such that higher scores reflect higher functional orientation. The internal consistency, test–retest validity, and convergent validity of the scale have been supported (McKinley and Hyde, 1996).
The Intuitive Eating Scale (IES; Tylka, 2006) was used to assess adaptive eating. This scale consists of 21 items that tap three aspects of healthy eating, including unconditional permission to eat (e.g. “If I am craving a certain food, I allow myself to have it”), eating for physical reasons rather than emotional reasons (e.g. “I stop eating when I feel full (not overstuffed)”), and reliance on internal hunger and satiety cues (e.g. “I trust my body to tell me how much to eat”). It is possible to compute subscale scores for each of these three elements; however, the subscales have been shown to load on a single higher order intuitive eating factor (Tylka, 2006). Thus, we used the IES total score. Participants respond to each item using a 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). The IES showed strong internal consistency and test–retest reliability among college women, and its construct validity was supported by significant negative relationships with eating disorder symptomatology (Tylka, 2006).
Finally, respondents rated their personal religiosity on a scale from 1 (not at all religious) to 4 (extremely religious). They also indicated how frequently they attended worship services on a scale from 1 (never) to 6 (more than once a week).
Results
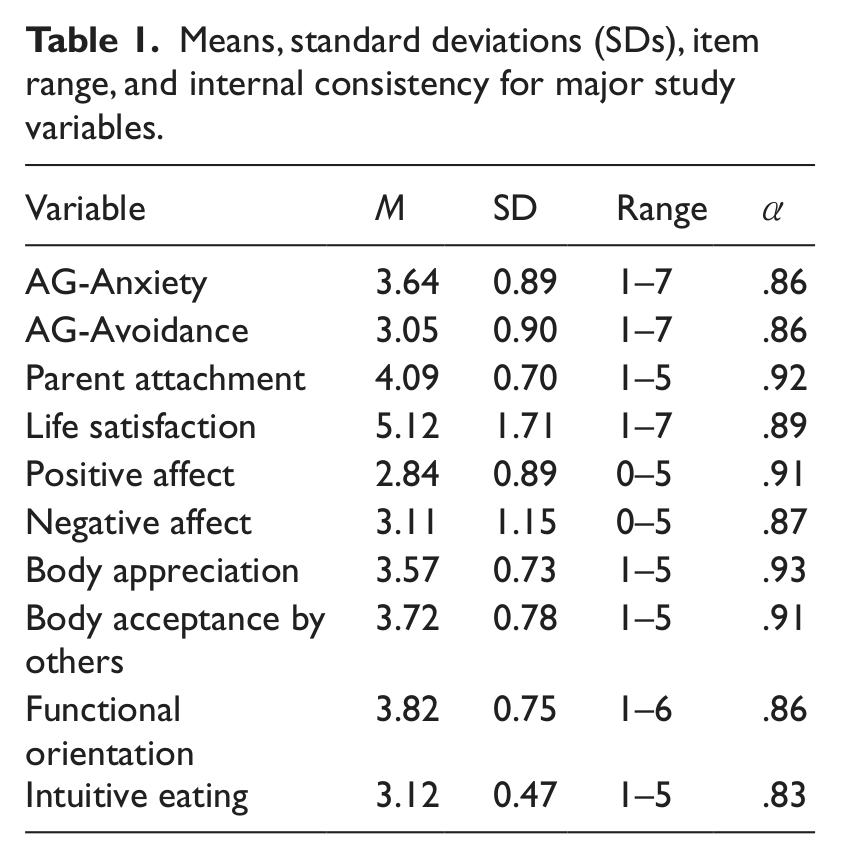
Composite scores for each measure were created by reverse-scoring items where necessary and averaging relevant items. Descriptive statistics and internal consistency coefficients for each variable are presented in Table 1. In order to demonstrate that the attachment to God measure was distinct from two standard measures of religiosity, we computed correlations between self-rated religiosity, frequency of service attendance, and the two AG dimensions. AG-Anxiety was unrelated to either of these indices, indicating that this dimension taps a unique aspect of women’s religious experience (for self-rated religiosity, r = −.16, p < .112; for attendance, r = −.15, p < .115). AG-Avoidance showed a significant negative correlation with self-rated religiosity (r = −.49, p < .001) and service attendance (r = −.47, p < .001), indicating that this dimension overlapped with standard measures of religiosity to a moderate degree. For this reason, we controlled for service attendance in subsequent regression analyses.
Means, standard deviations (SDs), item range, and internal consistency for major study variables.
As a preliminary analysis, we computed correlations among the three attachment dimensions (AG-Anxiety, AG-Avoidance, and Parent) and between these dimensions and the well-being variables. These correlations are presented in Table 2. The two God attachment variables were significantly correlated (r = .37, p < .001), indicating moderate overlap. However, they are theoretically distinct and have been shown to load on separate factors (Beck and McDonald, 2004); thus, we continued to treat them as separate constructs. Neither God attachment variable was related to parent attachment. The AG-Anxiety variable was significantly corr lated with each of the well-being variables in the expected direction. Specifically, there was a significant negative correlation between AG-Anxiety and life satisfaction, positive affect, body appreciation, body acceptance by others, functional orientation, and intuitive eating (recall that lower AGI scores indicate greater attachment security). There was a significant positive correlation between AG-Anxiety and negative affect. The other God attachment dimension, AG-Avoidance, was significantly negatively correlated with only two of the well-being variables including life satisfaction and functional orientation. Finally, parent attachment was significantly positively correlated with life satisfaction, body appreciation, and body acceptance by others (recall that higher scores on this variable indicate greater attachment security).
Correlations between attachment dimensions and well-being variables.
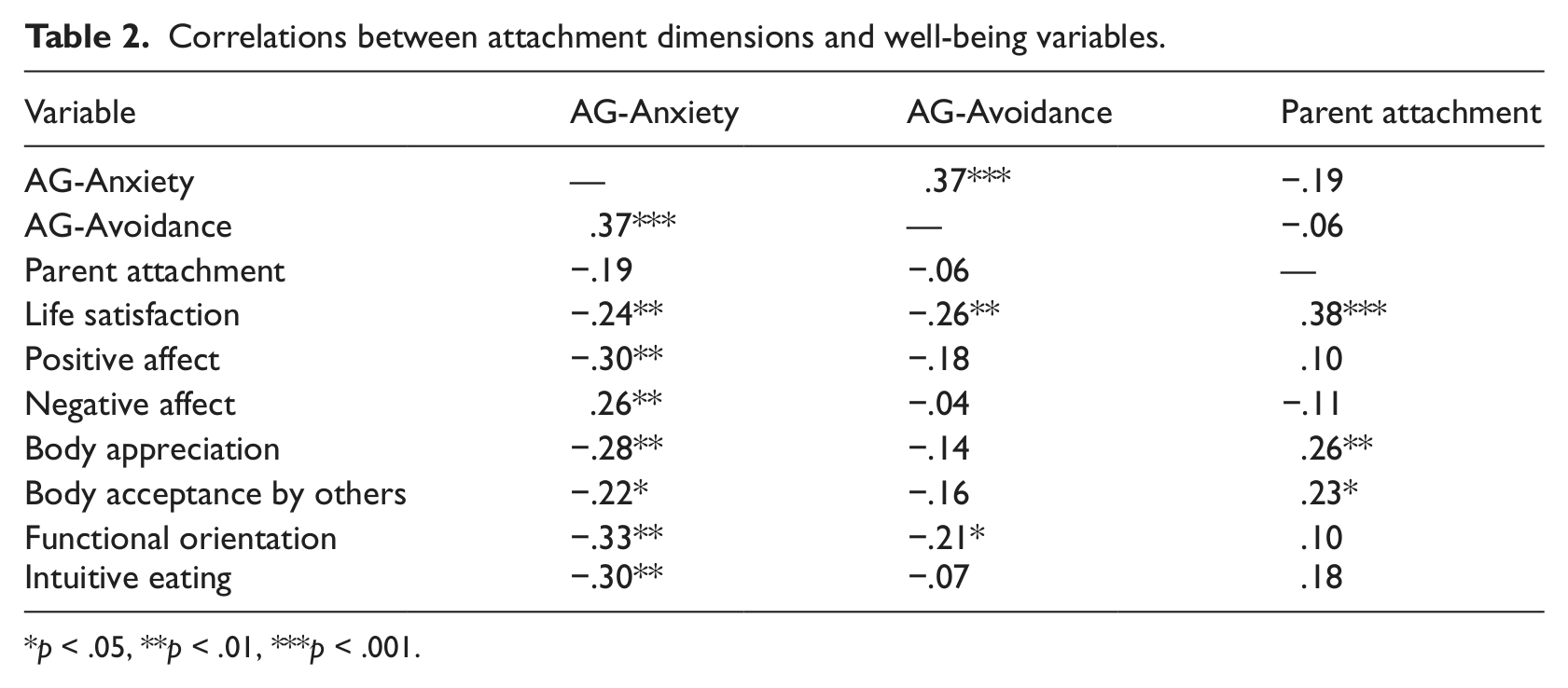
p < .05, **p < .01, ***p < .001.
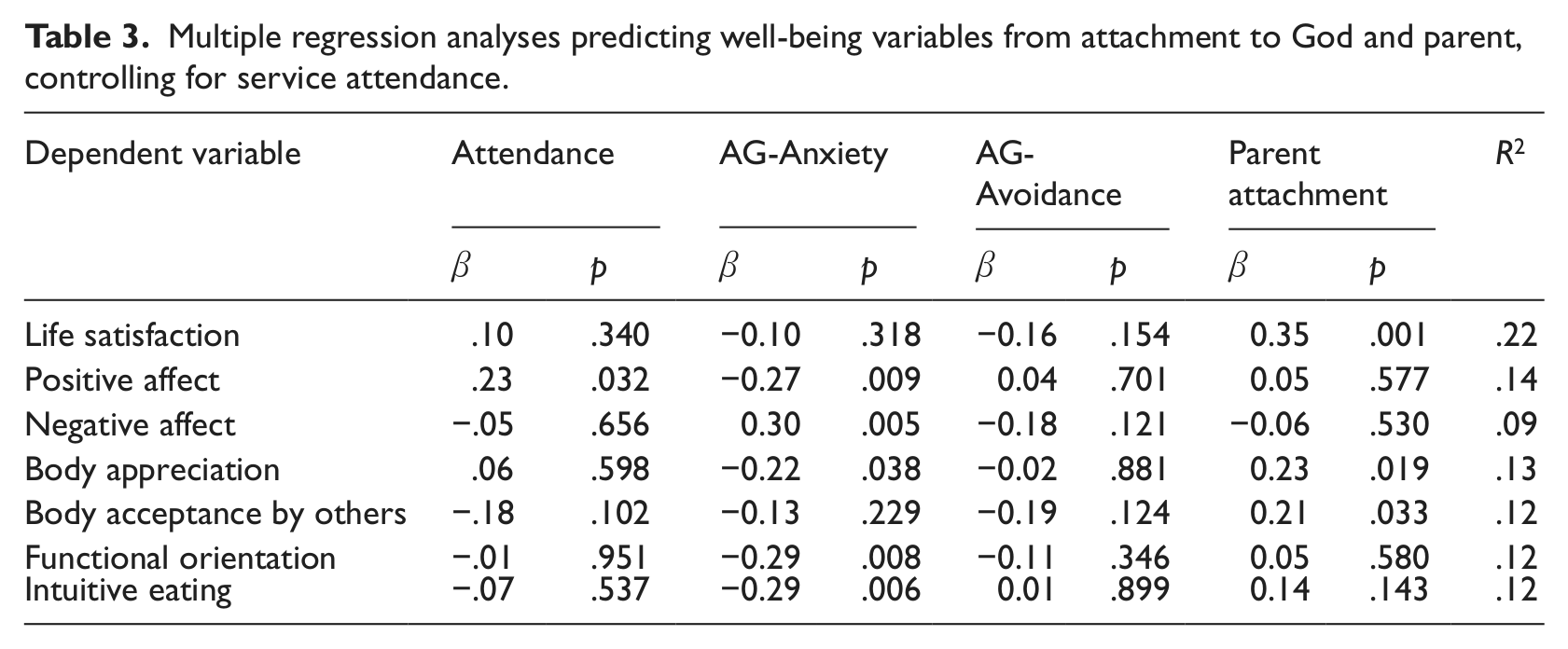
In order to test the relative contributions of the attachment dimensions to the well-being variables, we performed a series of simultaneous regression analyses. For each analysis, the criterion variable was regressed on service attendance, AG-Anxiety, AG-Avoidance, and parent attachment. A summary of these results is presented in Table 3. AG-Anxiety contributed unique variance to most of the well-being variables, above and beyond the contributions of AG-Avoidance, parent attachment, and service attendance. Specifically, AG-Anxiety predicted positive affect, negative affect, body appreciation, functional orientation, and intuitive eating. AG-Avoidance did not contribute unique variance to any of the well-being variables. Parent attachment significantly predicted life satisfaction, body appreciation, and body acceptance by others. Of note, parent attachment was the only significant predictor of body acceptance by others. Effect sizes (as indicated by R2) were moderate based on Cohen’s (1992) criteria.
Multiple regression analyses predicting well-being variables from attachment to God and parent, controlling for service attendance.
Discussion
We hypothesized that secure attachment to God would predict subjective and body-related well-being above and beyond attachment to a parent. We also predicted that nonanxious God attachment would relate to more of the body-related well-being variables than nonavoidant God attachment. Both these hypotheses were supported.
These results are consistent with two important theoretical positions. First, the acceptance model of intuitive eating (Avalos and Tylka, 2006) posits that unconditional positive regard from a significant other fosters a sense of acceptance and appreciation toward one’s body. This study showed that a perceived warm and secure relationship with God can serve as an important source of acceptance, which presumably reduces a woman’s tendency to turn to cultural messages about what is important. Second, according to attachment theory, mental representations of the self and the attachment figure tend to be complementary (Bowlby, 1969/1982). Thus, when women perceive that God is accepting, caring, and responsive, they believe that they themselves are acceptable and worthy of care. Our results are consistent with this interpretation, as they show that women with secure God attachments are more appreciative of their own bodies, are not overly concerned with their external appearance, and are attuned to their bodies’ physical capabilities and internal states.
A surprising finding was that neither dimension of God attachment contributed significant variance to body acceptance by others. We had expected this variable to be strongly influenced by a perceived secure relationship with God, particularly because previous research showed that unconditional acceptance in a close relationship was related to greater body acceptance by others (Avalos and Tylka, 2006). There was a significant bivariate relationship between attachment anxiety and body acceptance by others, but when attachment avoidance and parent attachment were simultaneously considered, this relationship was no longer significant. This result indicates that parent attachment was relatively more important for explaining body acceptance by others. It should be noted that two of the questions comprising the BAOS specifically asked about familial affirmation of weight and shape. Thus, if women generally felt accepted and respected by a parent, they likely also felt that parents accepted their bodies. In other words, shared method variance at least partially explains this result. In addition, however, it has been shown that parental messages about weight and shape have a strong influence on body image (Kluck, 2010). It appears that parental acceptance fosters an environment in which women do not perceive or are less sensitive to external social pressures to conform to cultural body ideals, and this effect continues into the college years.
This study showed that a perceived warm and secure relationship with God is an asset in the sense that it is related to multiple aspects of optimal psychological functioning for women. Although the design of the study prevents conclusions regarding causal direction, the most plausible interpretation is that feeling loved by God fosters well-being rather than vice versa. This interpretation is supported by reports from former patients that faith and spirituality were important in their recovery from eating disorders (Mitchell et al., 1990). A clear application of this finding would be to teach young women that they are loved and accepted by God regardless of weight and shape. However, interventions could be reasonably applied only in settings where religious ideas can be comfortably discussed, such as religious schools, gatherings, and faith-based treatment centers. Where appropriate, teachers, youth group leaders, or clinicians could engage religiously oriented young women in discussions that reinforce the idea that God is the ultimate source of acceptance, and that they are assured of security in their relationship with God. A recent study tested the effectiveness of a short-term group psychotherapy intervention that was explicitly designed to improve clients’ attachment to God (Thomas et al., 2011). The eclectic 8-week program used psychoeducational, interpersonal, and cognitive exercises as well as bibliotherapy and art/music interventions. Results showed significant improvements in the extent to which clients experienced God as accepting, intimate and supportive, as well as reductions in their attachment anxiety and avoidance. This type of intervention could be adapted for both prevention and treatment programs.
This study contributes to the growing literature that shows that religion is related to better physical and psychological health (Koenig et al., 2012). However, it goes beyond the existing literature by showing that religion is related to both general and specific aspects of flourishing. Furthermore, some scholars have argued that specific religious beliefs deserve greater attention, especially in the context of health and well-being (Cromby, 2012; Park, 2012). This study focused on a particular set of cognitions regarding women’s relationship with God, and these beliefs seem to tap a dimension of religiosity that is distinct from standard measures such as service attendance or self-rated religiosity. Findings highlight the importance of specific beliefs, because cognitions regarding the availability, security, and acceptance of God were consistently related to healthier body image and eating practices, while beliefs about depending upon God were unrelated to those outcomes.
This study has several limitations. First, the participants were female students attending a Christian college and the majority reported that they were at least somewhat religious. Thus, it may be that this particular dimension of religiosity is relevant only for similar populations. As is typical of much of the extant body image literature, our sample consisted primarily of White, upper middle class students; thus, generalizability to other ethnic or socioeconomic groups is limited. The study design was correlational; thus, conclusions about causation remain tentative. Finally, the study relied upon self-report measures that are always a potential cause for concern.
Despite these limitations, this study extends the existing literature in several ways. The study of positive body image and adaptive eating has only recently emerged as an area of inquiry that is distinct from low levels of disordered body image and eating habits (Tylka, 2006). This study is the first to explore the potentially beneficial contribution of religion to body-related flourishing, and our results suggest potential interventions for promoting positive body image within certain settings. Findings are consistent with the recently proposed acceptance model of intuitive eating (Avalos and Tylka, 2006) as well as attachment theory (Bowlby, 1969/1982), thereby affirming the importance of warm and accepting relationships as an asset for flourishing. Finally, the psychology of religion has been increasingly recognized as a legitimate field within mainstream psychology, particularly in regard to health and well-being. The present study provides additional evidence that the study of human behavior and mental processes should continue to explore the sometimes unexpected role that religion/spirituality can play in many people’s lives.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.