
Abstract
This study investigated the effect of a smoking health message on smokers’ comparative optimism. Two groups watched an anti-smoking scenario, with one group imagining being part of the scenario. Participants, including controls, completed comparative optimism ratings for four smoking-related illnesses. The intervention had negative consequences with both intervention groups reporting significantly higher comparative optimism versus the control group for all four smoking-related illnesses. It is concluded that media health messages can be powerful tools in changing comparative optimism but are influenced by peoples’ prior perceptions. Health messages need to be systematically assessed to understand prior beliefs of the target audience.
Introduction
Many models of health behaviour have risk perception as one of their predictors of behaviour. These models include the Health Belief Model (Janz and Becker, 1984), the Protection Motivation Theory (Rogers, 1975), the Adoption Process Model (Weinstein, 1998) and the Extended Parallel Process Model (Witte, 1998). Evidence from systematic reviews concluded that risk perceptions can influence future behaviour (Bish et al., 2011; Van der Pligt, 1998). In addition, there is a plethora of research investigating effective risk communication in the health arena (Berry, 2004).
Risk perception can be defined in absolute or comparative terms. When it is defined in comparative terms, it is often referred to as comparative optimism (CO). 1 CO refers to the belief that negative events are less likely to happen to us than others and that positive events are more likely to happen to us than others (e.g. Weinstein, 1987). CO has been demonstrated for many diverse health-related events including skin cancer (Eiser and Arnold, 1999; Myers and Reynolds, 2000), diabetes (Myers and Reynolds, 2000), car accidents (Perrissol et al., 2011), consequences of binge drinking (Ayers and Myers, 2011), breast cancer (Park et al., 2009), heart attack (Myers and Reynolds, 2000; Weinstein, 1982) and genetic risks (Welkenhuysen et al., 1997). Although research has suggested that CO is resistant to change (Robb et al., 2008; Weinstein and Klein, 1995), there has been some success in ‘debiasing’ comparative risk judgements. For example, when drivers were told that they would be made accountable for their decisions, their CO for having an accident as a driver was reduced (McKenna and Myers, 1997). Further studies indicated that it is possible to modify CO by requiring participants to imagine a relevant scenario with severe consequences for which the activity is to blame (McKenna and Myers, 1995; Myers and Frost, 2002).
There is strong evidence to suggest that imagining self-relevant events can influence participants’ subsequent behaviours (e.g. Ruvolo and Markus, 1992; Vasquez and Buehler, 2007). For example, a recent study using guided imagery concerning the consequences of continued smoking resulted in lower smoking rates among smokers in the month after the study (McDonald et al., 2010). However, studies have concluded that just imagining an event is insufficient for debiasing CO (McKenna and Myers, 1995). In a series of experiments using a ‘debiasing writing task’ on drivers’ risk perceptions, the event (car accident) had to have severe consequences and the individual imagining the event (the driver) had to believe that their driving was to blame for the accident for successful debiasing of CO to take place (McKenna and Myers, 1995). Drivers were asked to imagine a car accident and describe the accident indicating in which way it was severe and how they were to blame. They also wrote about the personal consequences of the accident. By involving participants in this way, drivers exhibited no CO for items such as the likelihood of having a car accident as a driver.
This method was successfully extended to media messages. Results indicated that media messages can successfully change peoples’ CO judgements and also that imagination can be powerful tool in facilitating such change. This is in the areas of driving and binge drinking.
McKenna and Myers (1995) produced a video that contained four scenes from a UK television series. These scenes involved individuals describing car accidents they had been involved in with a reconstruction of the accidents. These scenarios had originally been designed with blame and severity present. There were two intervention conditions and a control group. In a ‘watch’ condition, drivers watched the video and then answered CO questions about driving. In an ‘imagine’ condition, drivers were asked to imagine that they were the driver in the scenes they were watching. In the control condition, drivers completed the CO questionnaire. The control participants exhibited CO. Compared with the control group, the watch group exhibited significantly less CO and were partially debiased. However, the imagine group were totally debiased, with this group exhibiting no CO after the intervention.
A recent study extended this study to binge drinking (Ayers and Myers, 2012). Young adults who regularly drank alcohol watched an anti-drinking scenario (having an accident due to drinking), which had been previously aired on UK TV. The design was the same as McKenna and Myers (1995) with three conditions: control, watch and imagine. CO questions included ‘likelihood of being involved in an accident due to drinking’ and ‘having unprotected sex when under the influence of alcohol’. Both intervention groups reported significantly lower CO than the control group, with the ‘imagine’ group totally debiased for these two CO items.
This study explored the effect of a similar media message on smoking using the same method as used for binge drinking (Ayers and Myers, 2012). In smoking research, CO for smoking-related diseases has been reported, in that, smokers assess their risk of contracting smoking-related disease as significantly less than the average smoker (e.g. Segerstrom et al., 1993).
In an earlier intervention study, the debiasing writing task was extended to smokers’ perception of their smoking-related health risks (Myers and Frost, 2002). Smokers were asked to rate the likelihood of three events happening to them compared with the average smoker of the same sex and age. These events were lung cancer, heart disease and bronchitis (time 1). Results were not clear-cut, with no overall CO for any of the three health events. Responses were divided into two groups for each health event: (a) those responses that exhibited CO and (b) those responses that did not exhibit CO. Between 1 and 3 months later, participants were invited back to take part in the second part of the study, which involved completing the debiasing writing task, based on the driving manipulation, with participants being asked to imagine a smoking-related disease happening to them, due to their smoking (i.e. they were to blame), and to describe the [severe] consequences. The intervention was successful for those who exhibited CO at time 1, and the groups originally exhibiting CO for lung cancer, heart disease and bronchitis were totally debiased after the intervention at time 2.
However, for those who did not exhibit CO at time 1, the debiasing intervention had a different effect. At time 2, the groups either shifted to CO or in the direction towards CO. These results have important potential ramifications for media messages. If smokers exhibit CO, an intervention that involves engaging individuals about the severe consequences of their smoking behaviour and blame may be successful in motivating smokers to quit. However, if a smoker does not exhibit CO about their chances of contracting smoking-related diseases, such an intervention may have the opposite effect to the intended one (Myers and Frost, 2002).
These findings are relevant to a number of TV health messages developed for the UK Department of Health, which are designed to aid quitting. This study investigated whether a smoking scenario would affect CO judgements, using two experimental conditions, imagine and watch, similar to the previous driving and binge drinking interventions (Ayers and Myers, 2012; McKenna and Myers, 1995).
It was believed that a smoking intervention would have detrimental effects on smokers’ risk perception of contracting smoking-related diseases. It was hypothesised that participants in the watch condition would exhibit more CO for smoking-related illnesses (lung cancer, heart disease, bronchitis and stroke) compared to a control condition. Participants in the imagine condition would exhibit more CO for lung cancer, compared to both the watch and control conditions. This was hypothesised as lung cancer was the topic of the health message being watched.
Methods
Participants
Participants were 120 young adults from two universities in the United Kingdom. Inclusion criteria were being a smoker and aged between 18 and 30 years. There were 63 males and 57 females. Their age ranged from 19 to 30 years, mean = 24.45 and standard deviation (SD) = 2.34.
They had smoked between 1 and 15 years, mean = 4.76 and SD = 2.66, and smoked between 5 and 30 cigarettes per day, mean = 15.67 and SD = 6.25. There were 40 participants in each condition (imagine, watch, control). There were no significant group differences for age (F(2, 117) = 0.49, ns) and gender (χ2 = .60, degree of freedom (df) = 2, ns). All participants agreed to take part in the study.
Measures
CO was measured for four smoking-related illnesses: lung cancer, stroke, bronchitis and heart disease. The questions were compared to the average smoker of the same age and gender: how likely do you think you are to (a) develop lung cancer? (b) Have a stroke? (c) Get bronchitis? (d) Develop heart disease? Ratings were on a 5-point scale. The choices were very likely, likely, neither likely nor unlikely, unlikely and very unlikely, where (5) was anchored at ‘very likely’ and (1) was anchored at ‘very unlikely’. The wording (very unlikely–very likely) has been used in previous research, for example, for CO for alcohol consumption (Ayers and Myers, 2012) and skin cancer (Myers, 1999).
Demographic information collected were age, gender, number of cigarettes smoked per day and number of years the participant had smoked.
Health message was previously aired on UK national TV. It is approximately 1 minute and depicts a scenario of a young teenage girl discussing with a woman who is off-screen about her father contracting lung cancer. Severity (of the illness) and blame (lung cancer due to her father’s smoking) are clearly part of the scenario. At the end of the scenario, there is ‘quit smoking’ information. At the time of the experiment, this advert was not being aired on UK national TV.
Procedure
Ethics approval was given by Brunel University Psychology Department Ethics Committee. All participants gave informed consent. Participants who smoked were identified on campus when viewed to be smoking or after purchasing cigarettes at an on-campus newsagent. Participants were randomly divided based on the three conditions. Control participants completed the questionnaire. Participants in the two health message conditions ‘watch’ and ‘imagine’ completed the experiment in a quiet lab, where they sat on a chair facing a personal computer (PC), and then completed the questionnaire.
The ‘watch’ group were verbally given the following information:
You will now watch a short video clip about smoking. When it has finished can you please turn over the questionnaire and complete it. You can cease the experiment at any time.
The ‘imagine’ group were verbally given the following information:
You will now watch a short video clip and I would like you to imagine that it is personal and involves you. When it has finished can you please turn over the questionnaire and complete it. You can cease the experiment at any time.
The health message was then played using the PC. After completion of the questionnaire, the participants were fully debriefed.
Results
Means and SDs for CO ratings can be seen in Table 1. Initially, one-way analysis of variance (ANOVA) was performed with Student–Newman–Keuls (SNK) used for all post hoc comparisons (see Table 1). As hypothesised, for all four health events (lung cancer, bronchitis, heart disease and stroke), there were significant main effects of conditions (control, watch and imagine), with CO ratings in the watch and imagine conditions being significantly lower than the control condition, that is, participants in the two experimental conditions were significantly more comparatively optimistic than the control condition. In addition, for lung cancer and bronchitis, the CO ratings in the imagine condition were significantly lower than the watch condition, that is, participants in the imagine condition were significantly more comparatively optimistic than the watch condition as well as the control condition.
Self-ratings of means and standard deviations for comparative optimism estimates for control, watch and imagine conditions.
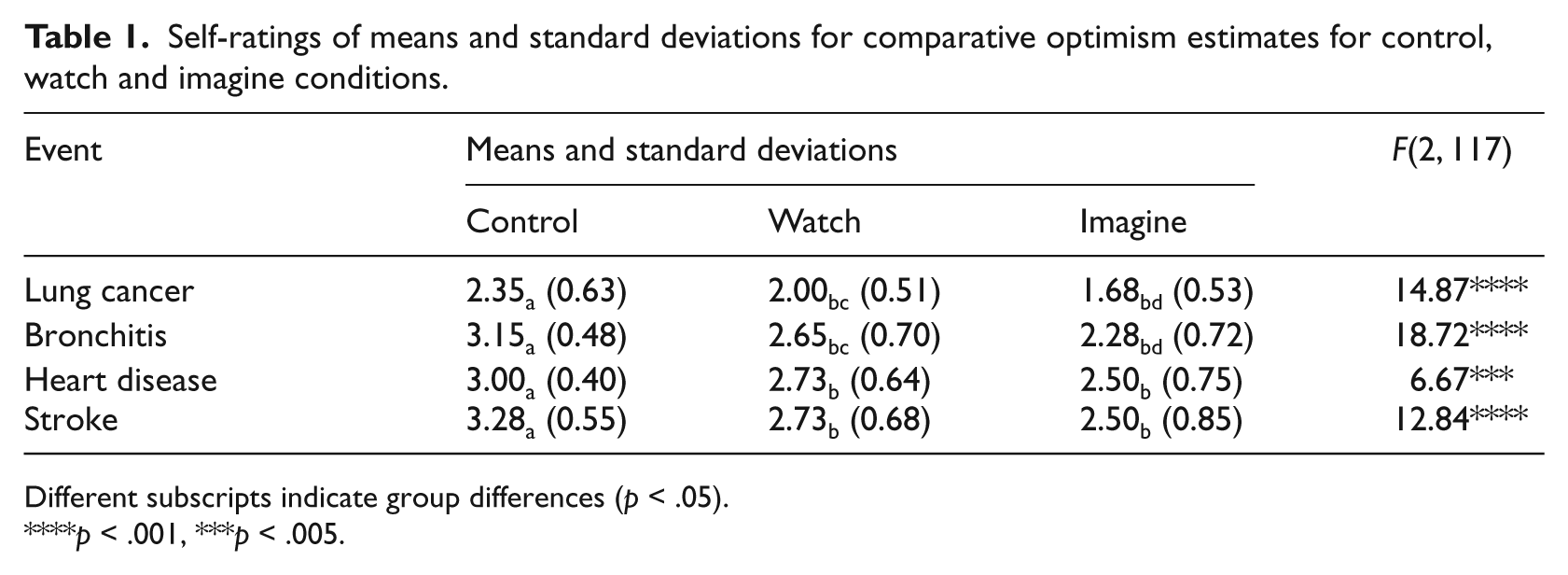
Different subscripts indicate group differences (p < .05).
p < .001, ***p < .005.
To explore any effects of covariates, a series of four analyses of covariance (ANCOVA) were then performed, with condition as the independent variable and CO ratings as the dependent variables, and age, gender, number of years smoked and number of cigarettes smoked per day as covariates. For lung cancer and heart disease, none of the covariates reached significance (CO: lung cancer, F(2, 113) = 15.51, p < .0001; heart disease, F(1, 113) = 6.22, p < .005). For bronchitis, age and number of years smoking were significant (F(1, 113) = 4.47, p < .05) and (F(1, 113) = 10.00, p < .01), respectively, with CO for bronchitis remaining significant (F(2, 113) = 19.72, p < .0001). For stroke, number of years smoking was significant (F(1, 113) = 4.53, p < .05), with CO for stroke remaining significant, (F(2, 113) = 12.84, p < .0001). A series of one-sample t-tests investigated whether each group were comparatively optimistic for each event (see Table 2).
One-sample t-tests for comparative optimism estimates for control, watch and imagine conditions.
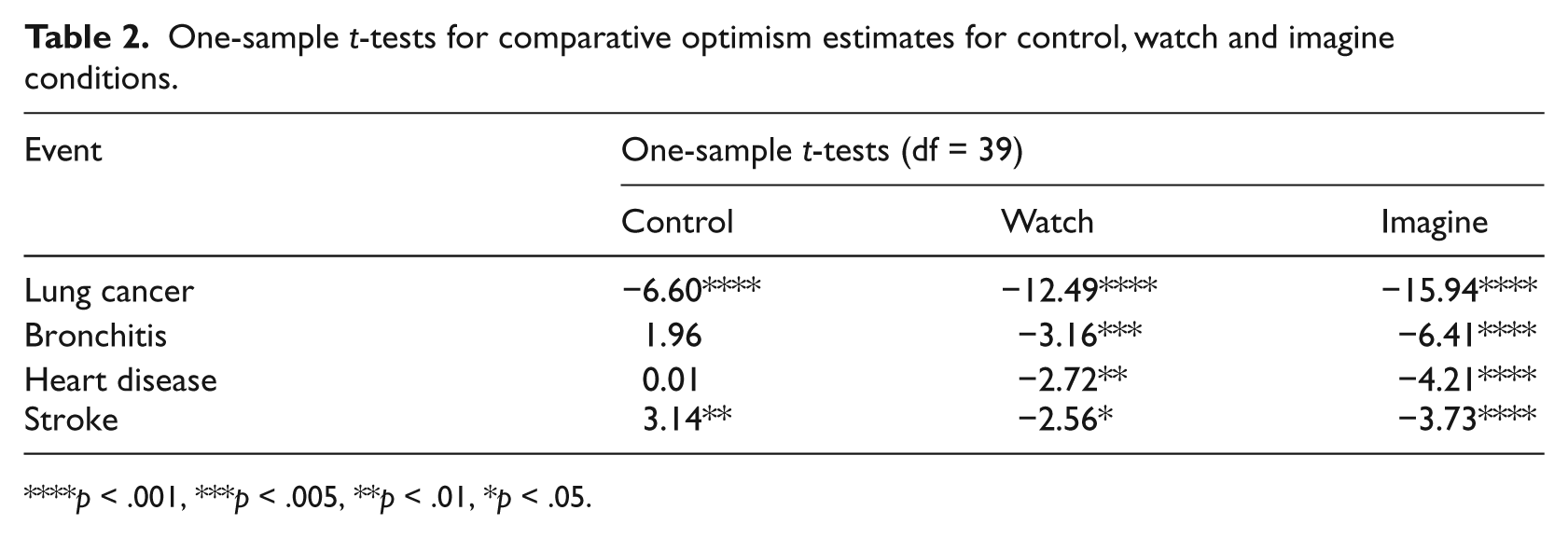
p < .001, ***p < .005, **p < .01, *p < .05.
All groups exhibited significant CO for lung cancer. However, the control group exhibited no CO for bronchitis or heart disease and were comparatively pessimistic for stroke, reporting that they were more likely to suffer from a stroke than other smokers of the same age and gender, that is, they were ‘debiased’ for three out of four smoking-related illnesses. For the other two groups, watch and imagine, participants reported CO for bronchitis, heart disease and stroke.
Finally, for the control group, participants were divided into those who exhibited CO (optimists) and those who did not (non-optimists). Optimists accounted for 53 per cent (N = 23) for lung cancer, 5 per cent (N = 2) for bronchitis, 7.5 per cent (N = 3) for heart disease and 5 per cent (N = 2) for stroke.
Discussion
To the best of the author’s knowledge, this is the first study that has investigated the effect of an anti-smoking media health message that has been presented on UK national TV on perception of risk (CO). Concurrent with previous research on smoking (Myers and Frost, 2002), the debiasing attempt resulted in the experimental groups who watched the message (which included severity and blame elements) rating themselves as less at risk for all four smoking-related illnesses: lung cancer, heart disease, stroke and bronchitis, compared to controls, that is, the message had the opposite effect to what would have been hoped for in such media campaigns. Further analyses (analysis of covariance) indicated that these findings could not be explained by demographic information (gender or age) or smoking behaviours (number of years smoked or number of cigarettes smoked per day). Demographic information has been explored in smoking cessation interventions. Blissmer et al. (2010) reported secondary data analyses of three behaviours including nearly 4000 participating in smoking cessation interventions. Results were similar to this study in that behaviour change was not consistently related to the demographic variables.
Detrimental health effects of smoking have been known since the 1950s (e.g. Doll and Hill, 1950). For example, a 40-year prospective study of smoking-related mortality among 34,000 male British doctors found that a number of fatal diseases were positively correlated with smoking (Doll et al., 1994). Participants in this study would have been aware of health-related risks of smoking for most of their lives. Smoking bans in public places throughout most of the developed world would also highlight risks of smoking, for example, in England, a ban on smoking in public places was implemented on 1 July 2007 (Health Act, 2006). Even smokers’ views on smoking seem to be surprisingly negative about smoking. In a recent survey of over 8000 people in the United Kingdom, around a third of smokers surveyed indicated that they would be in favour of moving towards a total ban on tobacco products (Shahab and West, 2010). Therefore, smokers are most likely very aware of the dangers – the possible (severe) health consequences due to smoking (blame). These are the elements that have previously been successful in the debiasing task (McKenna and Myers, 1995; Myers and Frost, 2002 – those exhibiting CO at time 1) and may have in this study resulted in more accurate measurements of risk in the control group than in earlier studies (e.g. Segerstrom et al., 1993). The possibility of smokers being aware of severity and blame needs to be investigated further, as well as how much they imagine the long-term consequences of smoking.
It may also be that exposing smokers, who more accurately perceive risk of contracting smoking-related diseases, to a hard-hitting message results in a defensive response. This is consistent with recent studies that suggest that high threat messages are related to defensive reactions (Brown and Smith, 2007; Leshner et al., 2009; Nestler and Egloff, 2010). A very recent study highlighted the potential importance of presentation of information in the smoking arena (Glock et al., 2012). The researchers found that when health messages on cigarette packages were presented as questions, such messages were significantly less likely to evoke a defensive response compared to other warning labels (text or graphic). These findings could be extended and explored by developing smoking scenarios where information is either formulated as a question or a warning.
For all four health events, lung cancer, bronchitis, heart disease and stroke, just watching the intervention significantly increased the amount of CO. For both lung cancer and bronchitis, imagination was more powerful than just watching the health message. It had been hypothesised that this would be the case for lung cancer, as this was a topic of the media message. However, this extended to bronchitis, which is also a disease of the lungs. This is consistent with the power of an imagination intervention (McDonald et al., 2010; Ruvolo and Markus, 1992; Vasquez and Buehler, 2007).
The control group did exhibit CO for lung cancer, with just over half of participants exhibiting CO (53%), which was higher than that reported in the study by Myers and Frost (2002), with 33 per cent exhibiting CO. How participants were recruited may have had an effect on the make-up of the groups. Myers and Frost (2002) allowed people to identify themselves as smokers or non-smokers. In this study, they were identified behaviourally, either when they were smoking or buying cigarettes. It is not clear whether it did make a difference or if it did, why it would only effect CO for lung cancer and not the other health behaviours. This should be investigated in future studies. However, the intervention had a similar effect for lung cancer risk estimates as the other three behaviours, in that it increased the amount of CO.
This study does have its limitations. First, it should be noted that although the media message had an effect on CO, it is not known what the consequences were, if any, on actual behaviour. Although viewing the media message resulted in higher CO judgements, it may still have been positive for quit attempts. It is very important to investigate this in future intervention studies. Second, this study was a between subjective design. Although this is consistent with previous CO media message studies (Ayers and Myers, 2012; McKenna and Myers, 1995), it would be useful in further studies to use a repeated measures design as in the previous smoking study (Myers and Frost, 2002) to investigate any within group changes.
This intervention study highlighted that media health messages can be powerful tools in changing peoples’ risk perception, but may be influenced by prior perceptions. Supportive of the importance of the role of prior belief, a recent study has shown that pre-existing beliefs can influence judgements of novel health information (Chang et al., 2012).
It would also be interesting in future studies to investigate the effect of these messages on non-smokers. In conclusion, caution is needed when developing such messages that should be systematically assessed to understand peoples’ prior beliefs.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not for profit sectors.