
Abstract
We examined the hypotheses that proposing higher levels of emotional intelligence (ability test and self-report) and lower neuroticism, extraversion, and agreeableness associate with lower levels of disordered eating. In a correlational study, 126 Israeli college students completed two measures of emotional intelligence, a brief five-factor personality test, demographic data questionnaires, and questionnaires assessing food preoccupation, namely, the Body Weight, Image and Self-Esteem Scale and the Appearance Schema Inventory. Results suggested that ability emotional intelligence is associated with disordered eating beyond gender and personality. Self-reported emotional intelligence did not associate with any of the outcomes after controlling for personality. Implications and applications are briefly discussed.
Keywords
Introduction
The scientific study of eating disorders (EDs) is a relatively new field, which gained momentum in the 1960s, and revealed alarming spread and increasing prevalence of the phenomenon ever since (Hudson et al., 2007; Polivy and Herman, 2002). Research provides worrying evidence suggesting that EDs can be a dangerous life-time burden and might afflict persons of all ages and both genders (Collier and Treasure, 2004; Krug et al., 2012; Robinson et al., 2013). Moreover, recent surveys show that most EDs, especially anorexia and bulimia can be seen more as a continuum of behavioral patterns rather than a specific pathological condition (Fairburn and Bohn, 2005; Hudson et al., 2007; Yost and Smith, 2012). This means that beyond diagnosed individuals, many more suffer patterns and symptoms causing psychological and physical distress, and are potentially at risk, without being diagnosed or properly attended to.
The term “disordered eating” is used in the literature to describe behaviors on the ED-continuum such as excessive dieting, excessive worries around food and food consumption, excessive exercise, vomiting to lose weight, and so on (Striegel-Moore et al., 1989; Yost and Smith, 2012). Disordered eating is increasing in prevalence, far beyond the recorded prevalence of EDs, especially among young persons, specifically young women (White et al.,2011). Treatment of ED is not always consistent, and authors in the field express the need for standards and evidence-based practice. Current evidence points to the complexity of treatment, equivocal outcomes, and the life-long struggles of individuals with EDs (e.g. Allen and Dalton, 2011; Keel and Brown, 2010). Moreover, EDs are often reported to coincide with psychological comorbidities that take a heavier toll on the individual and make coping and treatment even more challenging (De Bolle et al., 2011).
Studies have identified numerous correlates and antecedents of disordered eating, spanning from genetics to family dynamics and cultural values (Collier and Treasure, 2004). Most often cited factors are gender, exposure to objectifying norms and messages (e.g. through the popular media), and family and social dynamics (Croll et al., 2002). Recent studies have also explored emotional factors such as stress, negative emotion, and anxiety and suggested that they play a major role in disordered eating (Levine, 2012; White et al., 2011). Based on the above-mentioned, this study explores the associations between two major factors related to emotion regulation and disordered eating: personality and emotional intelligence (EI).
Personality and disordered eating
We adopted one of the most universal definitions for “personality” as stable behavioral patterns, persisting beyond temporal and situational restrictions (Pervin et al., 2005). Existing research has linked some personality traits with higher risk of developing EDs: Trait anxiety, novelty seeking, perfectionism, and perceived expectations of others have been systematically associated with various EDs (De Bolleet al., 2011; Keel et al., 2004). Recent studies have explored other personality models, the Five-Factor Model (FFM) being the most dominant (Costa and McCrae, 1992). There is evidence linking certain aspects of the FFM, such as neuroticism, openness, and so on to EDs (Keel et al., 2004; Sutin et al., 2011).This study examined the role of the FFM in disordered eating not necessarily falling within the clinically diagnosed range.
EI and disordered eating
A relatively new concept introduced into this field is that of EI. The concept refers to individuals’ abilities regarding emotion recognition, processing, and regulation in self and others (Mayer et al., 2000). The conceptual and empirical associations between EI and emotional regulation are evident in the literature (Mayer et al., 2000; Mikolajczak et al., 2008; Zysberg, 2012). Recently, two separate studies have suggested an association between EI and disordered eating or emotional eating patterns (Markey and Vander Wal, 2007; Zysberg and Rubanov, 2010). Evidence remains at this point scarce and anecdotal. EI may play a pivotal role as a factor in ED-related behaviors and thus is tested here alongside personality factors as a correlate of disordered eating.
The current study
The current study seeks to add to the literature by exploring the associations between persontraits often used in normative populations to assess emotional and behavior patterns --the FFM (Costa and McCrae, 1992), measures of EI --and disordered eating. Based on the literature reviewed earlier, it was hypothesized that (a) neuroticism, extraversion, and agreeableness will be positively associated with increased levels of disordered eating; (b) EI will be negatively associated with disordered eating and will add to the explained variance in this variable beyond and above that explained by the personality factors; and (c) the above associations will remain stable while controlling for gender, a major demographic variable associated with the occurrence of disordered eating (Croll et al., 2002).
Method
Sample
A sample of 126 students attending college in Northern Israel agreed to participate in a “study about the life habits and thoughts of young persons.” The mean age was 24.07 years (standard deviation (SD) = 2.43 years); 31 participants (about 25%) were men and 95 (75%) were women. Sixty percent of the sample reported being single and the rest reported being in a stable relationship/married. The vast majority (92%) were Jewish, 2 percent were Muslims, and 6 percent were Christians. The participants were all attending undergraduate programs in the social sciences.
Instruments
Disordered eating was assessed using three measures associated in the literature with the following tools:
Food Preoccupation Questionnaire (Tapper and Pothos, 2010) is a 28-item self-report form assessing respondents’ rigidity, excess involvement, and preoccupation with food and food consumption. The questionnaire demonstrated good reliability and construct validity.
Body Weight, Image and Self-Esteem Evaluation Questionnaire (Awad and Voruganti, 2004) was used as a proxy of the respondents’ judgmental aspect of their assessment of their own body, food-related behaviors, and looks. It is a self-report, 12-item questionnaire relating to one’s assessment of body shape, satisfaction with looks and weight, and food consumption. Originally developed in psychiatric settings, the instrument shows good internal consistency and differentiated well between groups varying in body mass index (BMI).
Appearance Schema Inventory (Cash and Labarge, 1996) was used to assess the participants’ body image. The 14-item scale showed good internal consistency and was shown to be relatively free of social desirability biases.
EI was assessed using two separate measures. One is a self-report measure and the other is an ability format test, both representing the two most prevalent approaches to the measurement of EI (Mayer et al., 2008).
Schutte Emotional Intelligence Scale (SEIS) (Schutte et al., 1998) is a self-report, 33-item scale showing good internal consistency and evidence of criterion-related validity in existing research. Although the authors proposed it as a measure of EI based on the ability-model presented originally by Mayer et al. (2008), it has been claimed that it may be more associated with personality traits than ability-EI. Response scales are ordered so lower scores reflect higher levels of EI.
Audio-Visual Test of Emotional Intelligence (AVEI) (Zysberg et al., 2011) is a computer-based, 27-item ability test of emotion recognition and analysis, congruent with two out of the four branches of EI as defined by Mayer et al. (2000). The test presents respondents with images and short video clips depicting persons in various emotional events and requests that they identify the emotion experienced by a target person. The test showed good reliability and predictive validity in a few studies (Zysberg, 2012). A higher grade represents higher levels of EI.
International Big-5 Mini-Markers(Thompson, 2008) was used to provide a short, simple indication of the five-factor personality traits in this sample. The 40-item adjective list showed acceptable reliability and convergent validity and was chosen for its simplicity and brevity.
Demographic data were collected using a questionnaire containing items for age, gender, program and year of study, socioeconomic status, ethnic background, religion, and so on.
Procedure
Participants were recruited from various social science classes on a college campus located in Northern Israel, after obtaining the college’s Institutional Review Board (IRB) committee’s approval. Participants were granted entry into a “lottery” draw in which two monetary prizes equivalent to US$85 were given. The participants were gathered in small groups in a computer lab with private booths for each participant. Administration of the measures took 30–35 minutes. At the end of the procedure, participants interested in more information were given a short debriefing regarding the study hypotheses and purpose. None of the participants who consented to participate withdrew from the study. The data collected were then analyzed using SPSS version 19.0 and AMOS, v. 19.0.
Results
Table 1 displays the descriptive statistics and intercorrelations between the main variables. The preliminary associations between the variables reveal correlations between the SEIS, many of the five-factor personality indicators, and two out of the three indices of disordered eating. The AVEI did not associate with any of the variables with the exception of a moderate association with the body image questionnaire.
Descriptive statistics and intercorrelations between the study variables (N = 126).
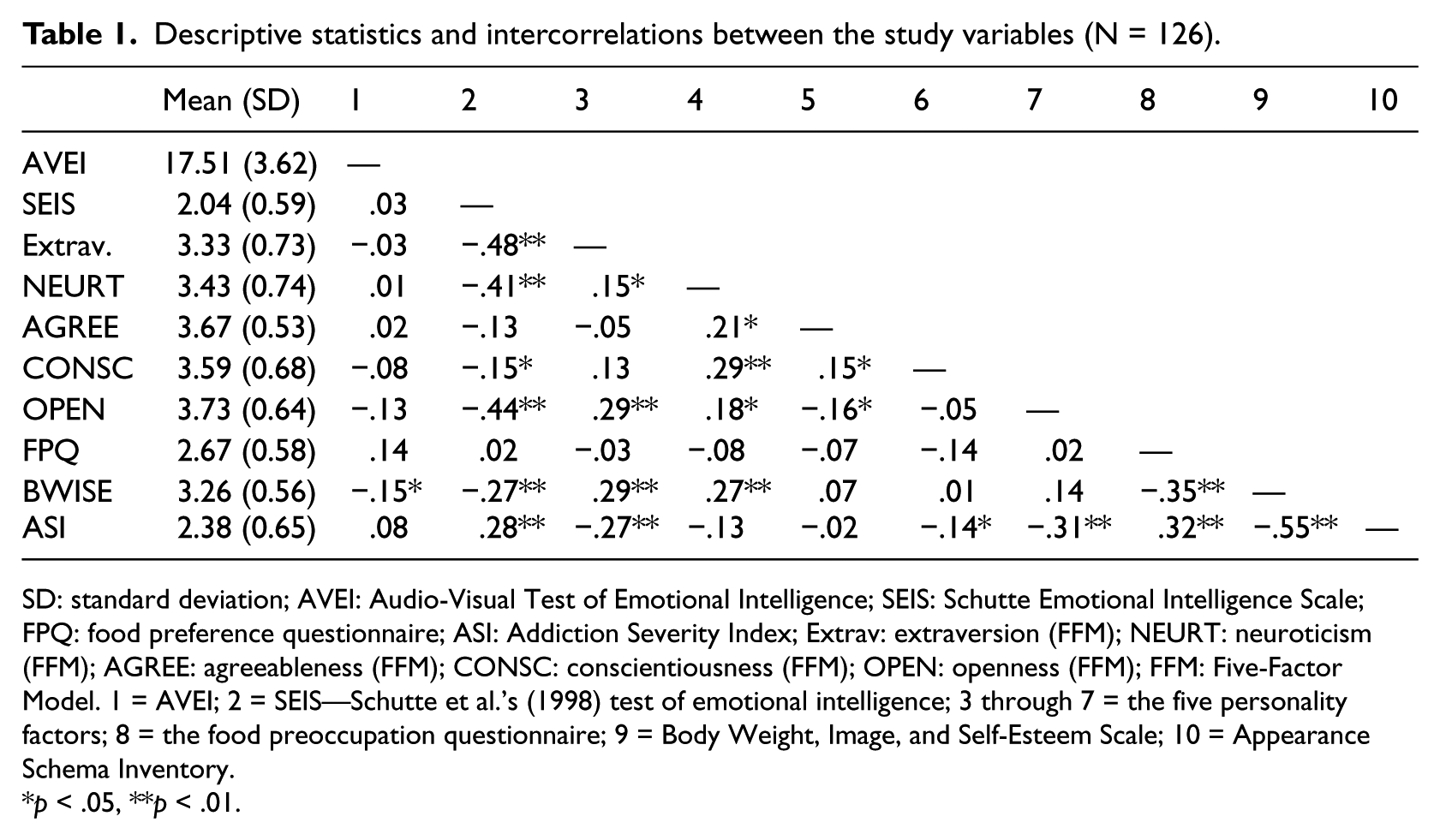
SD: standard deviation; AVEI: Audio-Visual Test of Emotional Intelligence; SEIS: Schutte Emotional Intelligence Scale; FPQ: food preference questionnaire; ASI: Addiction Severity Index; Extrav: extraversion (FFM); NEURT: neuroticism (FFM); AGREE: agreeableness (FFM); CONSC: conscientiousness (FFM); OPEN: openness (FFM); FFM: Five-Factor Model. 1 = AVEI; 2 = SEIS—Schutte et al.’s (1998) test of emotional intelligence; 3 through 7 = the five personality factors; 8 = the food preoccupation questionnaire; 9 = Body Weight, Image, and Self-Esteem Scale; 10 = Appearance Schema Inventory.
p < .05, **p < .01.
The association patterns also suggested correlations between the SEIS and the personality factors. We therefore tested the study hypotheses using path analysis, which allowed controlling for shared variances between our main variables. Since the three indicators of disordered eating were intercorrelated, we represented them in the model as three indicators of a latent variable we dubbed “eating and food-related worries.” The model and the results are summarized in Figure 1.
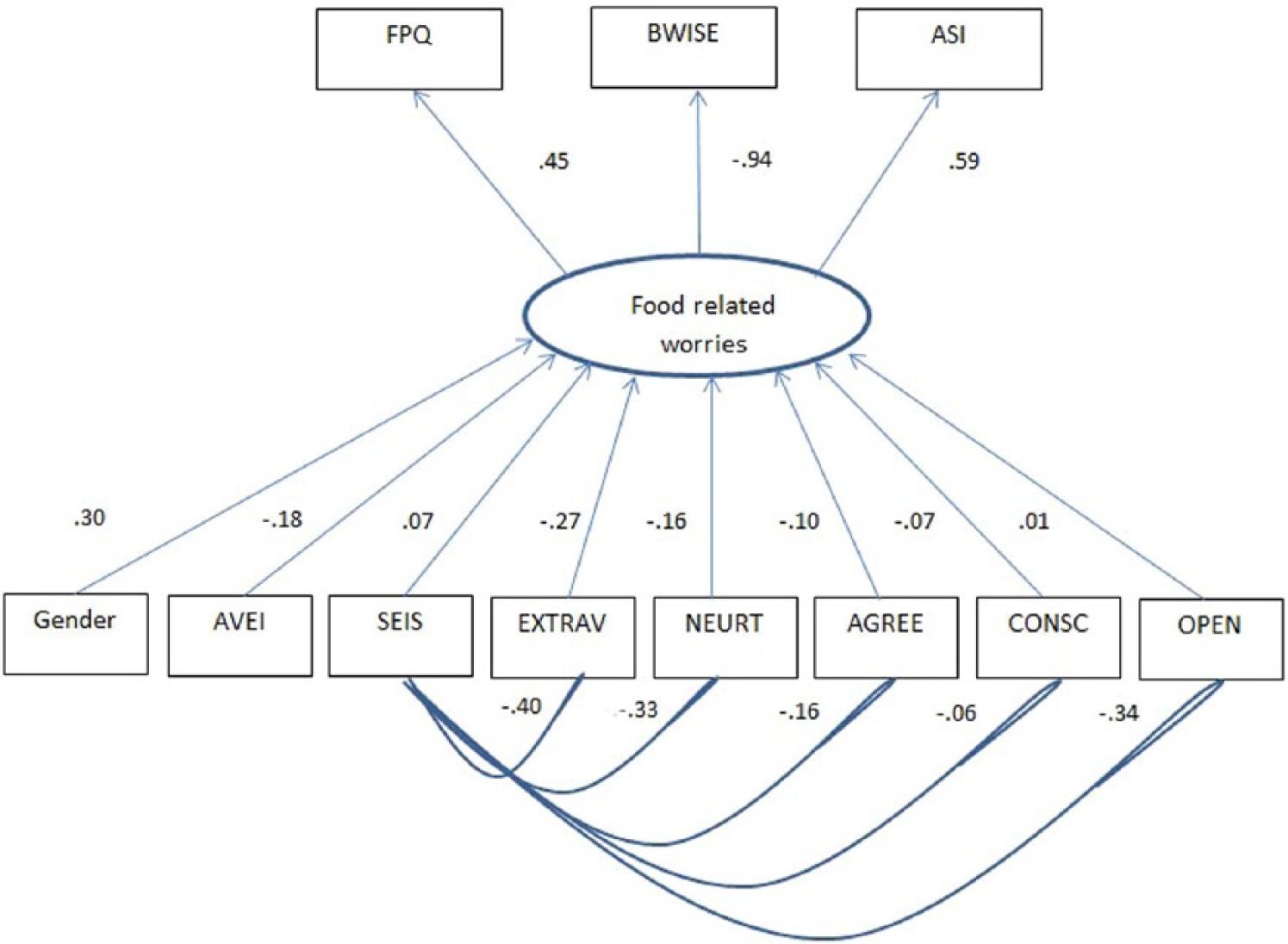
The study model including the path coefficients.
The path analysis revealed a more intricate pattern of associations between the study variables: first, the data confirmed that all three outcome indices loaded on a single factorand second, the SEIS EI scores correlated significantly with four of the five personality factor scores. After controlling for shared variances between the SEIS and the FFM mini marker scores, the association of the SEIS with disordered eating was nonsignificant. Two of the five personality factors, namely, extraversion and neuroticism associated significantly with disordered eating, while the AVEI showed a moderate but statistically significant addition to the explained variance in disordered eating beyond that accounted for by personality and gender. In interpreting the coefficients, higher levels of EI, neuroticism and extraversion, and being male were associated with less food-related worries and preoccupation. These results support the study hypothesis.
Discussion
Numerous social and psychological factors have been empirically studied as antecedents and correlates of disordered eating patterns (including clinically diagnosed EDs). Gender and personality traits have long been associated with dysfunctional food consumption and contemplation (Cervera et al., 2003; Collier and Treasure, 2004; De Bolle et al., 2011; Sutin et al., 2011). EI, a concept consistently associated with effective emotion regulation and sporadically associated with health-related outcomes (Schutte et al., 2007; Zysberg, 2012), may play an important role in the etiology of disordered eating.
This study investigated the potential associations of two measures of EI alongside widely accepted personality measures and gender with a range of measures representing varying aspects of eating and dysfunctional food-related perceptions and behaviors, indicating “disordered eating.” The results offer a few interesting insights into EI’s potential role in dysfunctional eating and food-related behavior: The evidence suggest ability measures of EI add moderately to the explained variance in disordered eating beyond personality and gender. The association means that higher levels of EI correlate with lower levels of preoccupation with food, and a healthier perception of the body shape and food consumption. The self-report measure of EI showed correlations with disordered eating, but those disappeared after controlling for the FFM traits, thus suggesting that the self-report measure may reflect personality more than EI. This suggestion is congruent with some of the findings in EI measurement research (Brackett and Mayer, 2003). The lack of associations between the AVEI and the FFM scores may suggest that the AVEI captures aspects of EI that are separate from personality, congruent with existing models of ability-EI (Mayer et al., 2000).
Another result, not originally within the framework of the study hypotheses, may be of interest, regarding the factorial structure found in the “disordered eating” measures. Although theoretically associated, food preoccupation; body weight, image, and self-esteem; and the Appearance Schema Inventory were not empirically tested for shared variance before. In this study, we found correlations between the three. They were therefore entered into the analyses as proxies of a single factor: the analyses showed all three loaded on the same factor dubbed “eating and food worries.” Obtaining empirical support for the associations between different measures assessing various aspects of dysfunctional food-related thoughts and consumption may lead, with future research, to a better understanding of the theoretical infrastructure of disordered eating and its measurement.
The current study had a few limitations to bear in mind while interpreting and trying to generalize the results: the correlational design does not allow for causal inference, and the associations found should be interpreted with care. The use of an Israeli sample may also limit the generalizability of the outcomes. Existing evidence, however, show similarities between Israel and most of the Western world in ED occurrence and associated factors (Bene Zion Medical Center, 2011). Imbalance in the representation of male and female participants may be another challenge to generalization of the study results, as males were underrepresented in this study. The use of measures of “disordered eating” rather than measures of EDs was meant to assess behaviors within a normative sample, but it may limit our ability to understand pathology, or generalize the results to clinical populations. An additional study is underway looking more carefully at the potential role of these variables in pathological samples.
Despite the limitations, the study highlights the role of EI in disordered eating and points to a direction seldom addressed in the current literature. To date, only two studies addressed the issue directly, both used self-report measures, with little or no control over personality measures (Markey and Vander Wal, 2007; Zysberg and Rubanov, 2010). The current study offers a more complex model of associations between personality factors and two approaches to EI as correlates of disordered eating. Should future research support the current findings, such models may help in early identification of individuals at risk and facilitate treatment and interventions with persons coping with disordered eating.
Footnotes
Acknowledgements
The author wishes to thank Ms Nitzan Argov and Ms Rotem Einat for their invaluable assistance in conducting this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.