
Abstract
Data from a cross-sectional study of gay, bisexual, and other men who have sex with men who were active methamphetamine users were analyzed to assess temporal relations between HIV seroconversion and initiation of methamphetamine use. Of the 100 men, 58 reported being HIV-positive. Most HIV-positive participants (65%) initiated methamphetamine use after seroconverting. Among those who initiated use before seroconversion, 8 years elapsed between onset of use and time of infection. Findings suggest the need to develop nuanced and targeted interventions aimed at disentangling the “meth-sex” link in this population. Findings also suggest use of the drug as a coping mechanism for those living with HIV.
Introduction
Methamphetamine is a highly addictive stimulant that has profound effects on the central nervous system (Homer et al., 2008, 2013). The prevalence of methamphetamine use has been documented on a national level as well as internationally (Lea et al., 2013; Rajasingham et al., 2012; Shrem and Halkitis, 2008; Substance Abuse and Mental Health Services Administration, 2010; Van Griensven et al., 2013). Despite a lack of epidemiological data, behavioral research has indicated particularly elevated levels of use of methamphetamine among gay, bisexual, and other men who have sex with men (MSM) (Halkitis, 2009; Halkitis et al., 2009). While poly-drug and alcohol use is common in this population (Halkitis et al., 2011), methamphetamine has received much attention due to its strong association with unprotected and other risky sexual behaviors that potentially increase the transmission of sexually transmitted diseases such as HIV (Gonzales et al., 2010; Halkitis, 2009).
The use of methamphetamine among gay, bisexual, and other MSM has been consistently linked to the spread of HIV (Centers for Disease Control and Prevention (CDC), 2007; Gonzales et al., 2010; Halkitis, 2009; Halkitis et al., 2001, 2005b; Patterson et al., 2005). For example, numerous studies have found that MSM using methamphetamine and other drugs have a significantly higher rate of HIV seroconversion compared to non-methamphetamine users (Buchacz, et al., 2005; Halkitis et al., 2006; Miller et al., 2006; Plankey et al., 2007).
The association between methamphetamine use and HIV risk in MSM can be understood through a theory of syndemics (Halkitis et al., 2013) that posits the synergy that exists between substance use and unprotected sexual behavior in the population. Although, syndemics theory does provide a conceptual frame for understanding the “meth-sex link” (Halkitis et al., 2001), the academic literature and popular press have conceived use of this illicit drug as causal to the acquisition of HIV (e.g. Jacobs, 2006; Urbina and Jones, 2004), although causation has been inferred and not demonstrated; thus, while these two risk behaviors co-occur, it is unclear if methamphetamine use consistently precedes seroconversion. To date, no study has disentangled the temporal relations that exist between initiation of methamphetamine use and the acquisition of HIV, although studies have documented use of the substance in seropositive MSM (e.g. Pappas and Halkitis, 2011). Thus, the goal of our analyses was to examine patterns of methamphetamine use in HIV-positive MSM, and specifically to delineate on onset of use of the substance in relation to time of seroconversion. In our analyses, we (1) describe our study and analytic sample along key demographic characteristics, including level of clinical diagnosis of methamphetamine use; (2) describe years of methamphetamine use and years living with HIV among the seropositive MSM (analytics sample); and (3) examine through bivariate analyses (independent samples t-tests) differences in duration of methamphetamine use in MSM who initiated use prior to seroconversion versus those who initiate use after seroconversion.
Method
A sample of 100 current methamphetamine-using MSM was recruited from the New York metropolitan area. Non-probability sampling methods for hidden populations were employed at recruitment venues, which included parks, street fairs, pride events, bars/clubs, and the Internet. Participants were screened via telephone and determined eligible if they were (1) biologically male, (2) 18 years of age or older, (3) used methamphetamine during the prior 6 months, and (4) had sex with another man during the prior 6 months. The period of 6 months was set as a criterion as we sought men who were currently sexually active and also current users of methamphetamine. Moreover, the literature supports that recall of risk behaviors should be limited to no more than a 6-month period (McElrath et al., 1994; Samuels et al., 1992). Eligible participants took part in a one-time visit where they completed a computerized survey. Data were collected from June 2010 through October 2010. We report on a subset of the quantitative data in this analysis.
Participants were asked to self-report current age, race/ethnicity, sexual orientation, and highest degree of education completed. The participants were also asked to report their current HIV status (positive, negative, or unknown). If a participant indicated an HIV-positive status at the time of evaluation, he was asked to indicate the year in which he had received a positive test result (e.g. 2003). This date was then subtracted from 2010.5 (year of the study) to determine the number of years that each participant had been HIV-positive. Those participants who indicated an unknown status (n = 2) were excluded from the analysis. Given the goal of analyzing temporal relations between methamphetamine use and seroconversion, only HIV-positive men (n = 58) were included in the analytic sample.
With regard to use of methamphetamine, participants were asked to indicate the first year they had used the drug (e.g. 1990). We then subtracted that date from 2010.5 to determine the amount of time in years that each participant had been using the drug. A second question assessed approximately how long each participant had been using methamphetamine on a categorical scale (less than 6 months, 6 months–1 year, 1–2 years, 2–5 years, 5–10 years, or more than 10 years). These data were cross-checked for consistency (e.g. if onset of use was 2010, it should be accompanied by a response to the categorical question indicating use for only the last 6 months to 1 year). No inconsistencies were detected.
A new variable was created based on the dates of methamphetamine initiation and HIV seroconversion. Specifically, we subtracted the year each participant reported testing positive for HIV from the first year the participant initiated methamphetamine use. Participants were also dichotomized into two groups: those who had initiated methamphetamine use prior to contracting HIV and those who began using methamphetamine after contracting HIV.
Diagnostic impressions for methamphetamine use were determined based on criteria designated by the Mini International Neuropsychiatric Interview (Plankey et al., 2007; Sheehan et al., 1998). The instrument was utilized because it provided a brief yet valid assessment of drug use and dependence, and as a means of establishing diagnostic criteria in addition to measures of frequency of use.
Study sample
The study sample consisted of 100 gay, bisexual, and other MSM who ranged in age from 18 to 67 years. The mean age of the participants was 41.46 years (standard deviation (SD) = 11.99; median (Md) = 43; skewness =−0.36; kurtosis = −0.79). Demographics for the study sample, by known HIV status, are shown in Table 1. Two men of unknown status were excluded. Bivariate analyses were performed to investigate relations between demographic variables and to further characterize the sample. Results indicated that no demographic variables were significantly related. Moreover, self-reported HIV status was not related to race, sexual orientation, educational attainment, or clinical level of addiction to methamphetamine.
Sample characteristics.
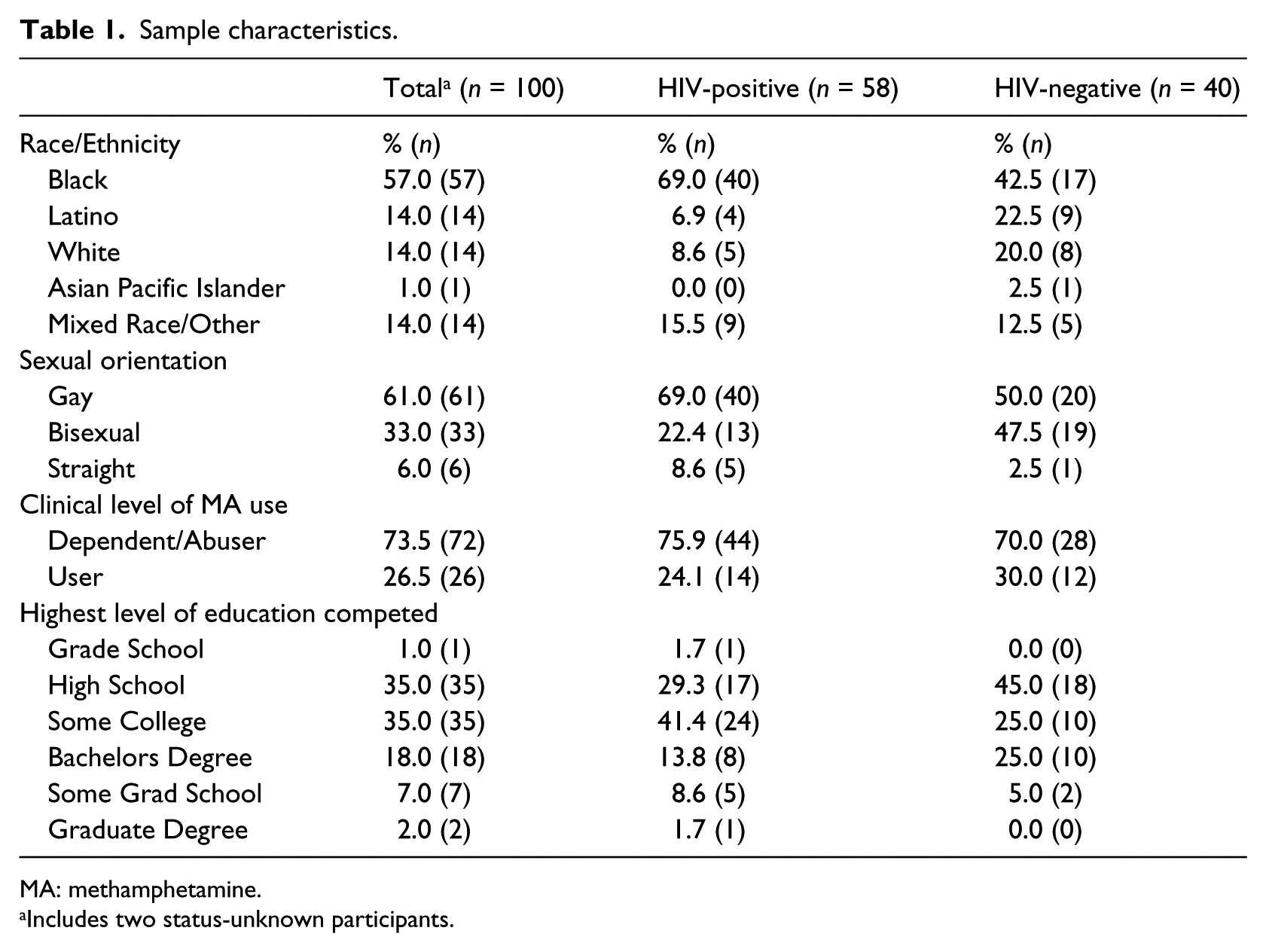
MA: methamphetamine.
Includes two status-unknown participants.
Among all 100 participants, methamphetamine use ranged from less than 1 year to 38 years, on average 8.85 years (SD = 7.96; Md = 7; skewness = 1.16; kurtosis = 2.33). As duration of methamphetamine use was self-reported, we sought to further corroborate the validity of the time at which this drug use was initiated. A strong association (r = .85, n = 100, p < .01) was detected between the number of years in duration they indicated using methamphetamine and the categorical variable which also measured duration of use (i.e. less than 6 months, 6 months–1 year, 1–2 years, 2–5 years, 5–10 years, or more than 10 years).
Analytic sample
The analytic sample consisted of 58 HIV-positive men and their characteristics are also shown in Table 1. Those participants who indicated being HIV-positive (n = 58), reported a mean age of 45.09 years (SD = 10.74; Md = 47; skewness =−0.51; kurtosis =−0.43) and were older than the HIV-negative men (t(96) = 3.63, p < .001) who reported an average age of 36.65 years (SD = 12.11; Md = 39; skewness =−0.12; kurtosis = −1.15). The duration of time since seroconversion ranged from less than 1 year to 25 years, and they had been HIV-positive on average 14.01 years (SD = 7.57; Md = 13.50). Furthermore, there was a significant association between participant’s age and the number of years they had been HIV-positive (r = .49, n = 58, p < .01).
Results
For participants who indicated being HIV-positive (n = 58), we carried out analysis to examine to the relationship between when they seroconverted and when they initiated methamphetamine use. Of the 58 HIV-positive men, 26 percent (n = 15) had used methamphetamine prior to becoming HIV-positive, while the majority, 65 percent (n = 38), used methamphetamine only after seroconversion. The remaining 9 percent (n = 5) indicated that they had initiated methamphetamine use and seroconverted in the same year. These five participants were excluded from the ensuing analyses, as there was no way to determine which event transpired first.
Among those for whom methamphetamine use preceded HIV seroconversion, the average time between onset of use and seroconversion was 9.07 years (SD = 9.00; Md = 6.00; range = 1–35). Those participants who were already HIV-positive initiated use of the drug 10.92 years (SD = 6.10; Md = 11) after infection.
On average, the 58 HIV-positive men had been using the drug for 9.21 years (SD = 8.79; Md = 6.5; skewness = 1.62; kurtosis = 2.09). These participants were then grouped into two categories: those who were HIV-positive (n = 38) at the time of methamphetamine initiation and those who were HIV-negative at the time of methamphetamine initiation (n = 15). Results indicated a significant difference in number of total years of methamphetamine use for participants who seroconverted prior to methamphetamine use versus those who seroconverted after methamphetamine use (t (51adj) = 4.11, p = .001). Specifically, men who were already HIV-positive prior to initiating methamphetamine had been using for an average of 5.61 years (SD = 4.16), and those who were HIV-negative at the time of methamphetamine initiation had been using for an average of 18.43 years (SD = 11.80).
Discussion
The data from this initial exploratory analysis demonstrate two main points: (1) that gay, bisexual, and other MSM can use methamphetamine for years without seroconverting, and (2) that some of these men commence use of methamphetamine only after seroconversion.
The analyses we have undertaken chronologically separate onset of methamphetamine use and HIV seroconversion. This undertaking is particular salient as empirical literature suggest a strong connection between sexual risk behavior associated with methamphetamine use and consequent HIV seroconversion in MSM (Buchacz, et al., 2005; Halkitis, 2009; Halkitis et al., 2001; Thiede et al., 2009). Our findings challenge two longstanding beliefs about use of the drug. First, the temporal association between initiation of methamphetamine use and HIV infection is not always proximate. While this does not mean that methamphetamine is not a significant factor in the ongoing HIV epidemic among gay and bisexual men, it does highlight that other psychological, biological, and social factors may also be interacting, contributing to its continued spread (Halkitis, 2010). Our results suggest that although the use of methamphetamine may indeed promote HIV seroconversion, it does not do so rapidly (Halkitis, 2009; Homer et al., 2008; Jacobs, 2006; Meredith et al., 2005). While HIV-positive methamphetamine users have been implicated in the spread of HIV due to high rates of risky sexual behavior, often with men of negative or unknown status (Halkitis et al., 2006; Patterson et al., 2005; Semple et al., 2008; Wohl et al., 2008), our data suggest that this risky behavior may not lead to contracting HIV for a substantial amount of time.
Our second finding, one with potentially critical clinical implications, demonstrates that for the majority of HIV-positive men in our sample, methamphetamine use was only initiated after several years of living with the virus. In effect, HIV seroconversion precedes use of methamphetamine and not vice versa, the latter being the more commonly held belief. Methamphetamine use has been implicated largely in the acquisition of HIV (e.g. Halkitis, 2009). However, the majority of men in this sample did not use methamphetamine until they had lived with HIV for nearly a decade. This finding highlights the reliance that some HIV-positive men may develop on the substance as a coping with the physical, emotional, and social burdens of the disease, including the stigma associated with HIV that continues to exist, even within a new generation affected by the disease (Dowshen et al., 2009). Studies have demonstrated that the use of substances in the seropositive population is not uncommon (Halkitis et al., 2005b) and this is particularly true of methamphetamine, for which use may be understood as a means of coping with the realities of HIV infection (Halkitis, 2010; Halkitis et al., 2005a, 2005c). This latent connection between seroconversion and methamphetamine use raises critical questions surrounding why many HIV-positive men turn to the sexually liberating, cognitively disengaging, and chemically addictive properties of methamphetamine. Further research is required to clarify if, why, and how methamphetamine is utilized to combat the chronic stress and stigma associated with living with HIV. By extension, as the complex relationships between MSM, HIV, and methamphetamine use are further disentangled, specific interventions can be developed aimed at addressing methamphetamine use in this population in efforts to increase knowledge and reduce new incidences of HIV transmission.
Because of design, this study possesses certain limitations. We acknowledge that our sample size was small and our eligibility criteria were specific, which may limit the generalizability of our findings to other MSM. More importantly, the small sample results in limited power and thus some of the non-significant findings may be due to the sample size itself. Furthermore, given that our sample tended to be older (mean age of 41 years), it is possible that methamphetamine initiation was delayed due to the fact that methamphetamine was not yet elevated in use or widely available in New York City (NYC) until the late 1990’s (Halkitis, 2009). This study’s cross-sectional design limits the authors’ ability to determine causality regarding whether methamphetamine use eventually leads to HIV seroconversion or vice versa, though we are confident our data provide clarified insight into the discourse surrounding the temporal relationship between these two phenomena, with a particular emphasis on the timeline of when and why HIV-positive men initiate methamphetamine use. Finally, data regarding both HIV status and methamphetamine use were self- and retrospectively reported.
Despite these limitations, there is currently no other published study, which has investigated the temporal relations between initiation of methamphetamine use and HIV seroconversion. It is our hope that these findings, despite being a preliminary initial analysis, will help provide a more nuanced understanding of the temporal relationship between the use of methamphetamine and HIV seroconversion among gay, bisexual, and other MSM. Further research is needed to clarify why many HIV-positive men eventually initiate methamphetamine use. The answers to these questions create a richer understanding of the “meth-sex” link and will help better inform clinicians and interventionists of the unique mental health burdens of gay, bisexual, and other MSM who are living with HIV.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.